
Developing an Addiction Medicine Consult Service · Developing an Addiction Medicine Consult...
30
Developing an Addiction Medicine Consult Service Alexander Y. Walley, MD, MSc Director, BU/BMC Addiction Medicine Fellowship Medical Director, Opioid Overdose Prevention Pilot Program, MDPH Addiction Medicine Fellowship Director’s Meeting Baltimore Wednesday, April 13, 2016 1pm
Transcript of Developing an Addiction Medicine Consult Service · Developing an Addiction Medicine Consult...

Developing an Addiction Medicine Consult Service
Alexander Y. Walley, MD, MSc Director, BU/BMC Addiction Medicine Fellowship
Medical Director, Opioid Overdose Prevention Pilot Program, MDPH
Addiction Medicine Fellowship Director’s Meeting Baltimore
Wednesday, April 13, 2016 1pm
Presenter
Presentation Notes
Alex

Substance use is pervasive across BMC’s inpatient population
2
5.6% 10.4% 10.7% 10.8% 11.0% 11.5%
12.4% 12.5% 12.8%
13.4% 14.6%
15.5% 17.1%
20.4% 20.6%
29.6% 31.1% 31.6%
33.8% 38.8%
OtherVascular
RenalPlastics
NeurosurgeryGen Cards
GynCT Surg
Heme / OncNeurology
General SurgeryGeriatricsCards CHF
CCUFamily Medicine
Internal Medicine - Hip FractureHospitalist
MICUInternal Medicine
ID
Adult discharges with billed substance use code during visit Percentage of annual discharges
• Across all adult discharges, 17.5% had a substance use code billed during their hospitalization
• Likely undercounts true demand, as substance use is frequently a complicating, but not primary, diagnosis
Source: Internal BMC admission / billing data; May 2014-June 2015.

Patients with underlying substance use issues have higher readmission rates and length of stay, regardless of diagnosis
3
15.7%
11.9%
Active substance useNo active substance use
Readmission rate, by substance use status Percentage
4.82
Active substance useNo active substance use
6.10
Average inpatient LOS, by substance use status Midnights
Source: Internal BMC admission / billing data; May 2014-June 2015.

Outline
• Perceived need among nursing and residents • Description of service
• Curriculum for residents
• Patients seen • Treatment initiated • Linkage and follow-up • Successes and Challenges

Perceived Need: Baseline BMC survey – July - August 2015
33% 27%
87% 93%
33%
11%
88%
73%
Satisfied with SUDcare you provide at
BMC?
BMC approachintegrated?
Need change ourapproach?
Consult serviceuseful?
Percentage rating > 3 on 5-point Likert scale
Medicine Residents N=30 M6 Nurses N=40

Perceived Need: SAAPPQ survey – July-Aug 2015
Short Alcohol and Alcohol Problems Perception Questionnaire generalized to substance users
Role adequacy – feelings of knowledge and skill adequacy
Role legitimacy - the right to work with people who use substances
Motivation - Willingness to work with people who use
Task-specific self-esteem - Feelings of pride vs. failure in work
Work satisfaction - Expectation of satisfaction
The SAAPPQ is a 10 item, 7-point Likert-type pre-training questionnaire measuring attitudes of professionals towards the care of people with substance use disorders
Presenter
Presentation Notes
The SAAPPQ is a 10 item, 7-point Likert-type pre training questionnaire measuring the attitudes of professionals towards the provision of care to those with alcohol use disorders

Perceived Need: SAAPPQ survey – July - August 2015
72% 79%
56% 63%
26%
81%
60% 56% 63%
12%
Role Adequacy Role Legitimacy Motivation Task-specificself-esteem
WorkSatisfaction
Percentage rating > 4 on 7-point Likert scale
Medicine Residents N=36 M6 Nurses N=40
Description of Service: BMC Addiction Consult Service
• ACS started July 17, 2015 • Goals:
• Improve care quality for inpatients, including initiating evidence-based medications
• Link to outpatient chronic care services • Reduce readmission, optimize length of stay • Improve BMC staff satisfaction and trainee knowledge/skills
• Offer consultation Monday-Friday to all inpatient services

Description of Service: BMC Addiction Consult Service
• Team consists of: • Medicine attending (afternoons) • Addiction Medicine Fellow (when available) • 1-2 Internal medicine or family medicine residents full-time (when
available) • RN 0.5FTE (position to be filled in November) • Daily coordination with Project ASSERT and Social Work • Weekly joint rounds with Psychiatry C/L on Wednesdays

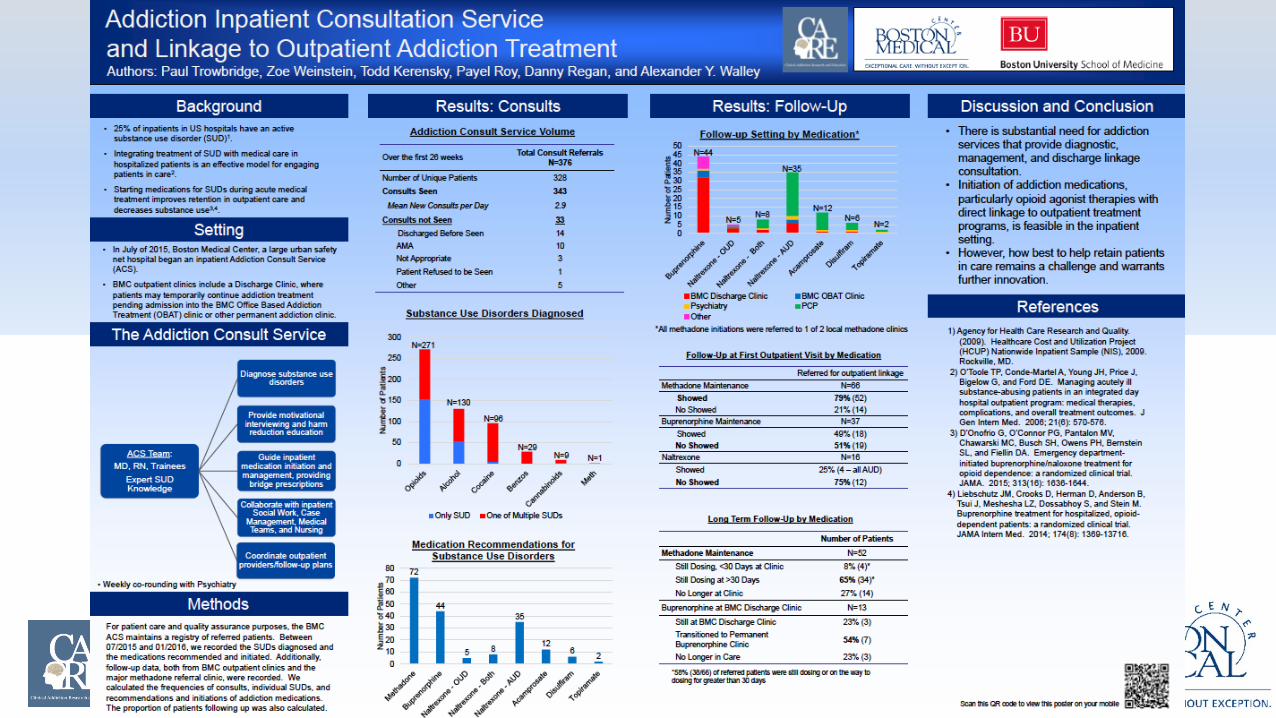
Patients Seen: July 17, 2015 – January 17, 2016
Total Consult Referrals N=376
Number of Patients 328 Consults Seen 339
Mean new consults per day 2.9 Consults not Seen 37
Discharged Before Seen 14 AMA 10 Not appropriate 3 Outpatient 8 Patient Refused to be Seen 1 Not a patient 1
Presenter
Presentation Notes
67% users 33% non-users

Patients Seen: July 17, 2015 – January 17, 2016
152
52 5 0 0 1
271
130 96
29 4 9
0
50
100
150
200
250
300
Opioids Alcohol Cocaine Benzos Marijuana Meth
Num
ber o
f Pat
ient
s Substance Use Disorders Diagnosed
Only 1 Substance Any Substance
Presenter
Presentation Notes
67% users 33% non-users

Treatments Initiated: July 17, 2015 – January 17, 2016
72
44
5 8
35
12 6 2
01020304050607080
Num
ber o
f Pat
ient
s Medically-Assisted Treatment Recommendations
Presenter
Presentation Notes
67% users 33% non-users

Linkage to Care: July 17, 2015 – January 17, 2016
N=44
N=35
N=5 N=12
N=2
0
5
10
15
20
25
30
35
40
45
50
Suboxone Naltrexone -OUD
Naltrexone -Both
Naltrexone -AUD
Acamprosate Disulfiram Topiramate
Num
ber o
f Pat
ient
s Follow-up by Medication
FAST PATH OBAT Psychiatry PCP Other
N=8 N=6
Presenter
Presentation Notes
67% users 33% non-users

Linkage to Care: July 17, 2015 – January 17, 2016
Referred for outpatient linkage Methadone Maintenance at CSAC N=66
Showed 79% (52) No Showed 21% (14)
Buprenorphine at BMC N=37 Showed 49% (13) No Showed 51%(18)
Naltrexone at BMC N=16 Showed 25.0% (4 – all AUD) No Showed 75.0% (12)
Presenter
Presentation Notes
67% users 33% non-users

Follow-up: July 17, 2015 – January 17, 2016
Referred for outpatient linkage Methadone Maintenance at CSAC N=52
Still Dosing, <30 Days at Clinic 7.7% (4) Still Dosing at >30 Days 65.4% (34) – 52.8% (38/72) No Longer at Clinic 26.9% (14)
Buprenorphine at FAST PATH N=13 Still at FAST PATH 23.1% (3) Transitioned from FAST PATH 53.8% (7) Lost to Follow-up 23.1% (3)
Presenter
Presentation Notes
67% users 33% non-users

Addiction Education Needs Assessment
Lack of adequate education In addiction medicine
Lack of enough experts In addiction medicine

Resident Rotation • Consult service staffed by IM/FM residents, addiction/GIM fellows, and
ABAM-certified attending • M-F 8a-5p with on-call paging • Example consults:
• Initiation of pharmacotherapy for alcohol and opioid use disorder • Complicated benzodiazepine withdrawal • Pain management on opioid agonist therapy
• Interdisciplinary rounds with staff psychiatrists once weekly for difficult patient cases
• Resident rotation: • 1 week elective • Primary consultant of 1-2 new patients per day • Round, develop plan, communicate recommendations, follow-up

Take an appropriate substance use specific history
Counsel patients on use, risks, and benefits of opioid agonist therapy and naltrexone for opioid use disorder
Counsel patients on harm reduction strategies
Rotation-Specific Curriculum • Developed using ACGME Core Competencies • 14-page document with 16 specific learning objectives
Presenter
Presentation Notes
Blow up objectives

Early Reflections on Resident Rotation
• Strengths: • Treat education in addiction like education in any other subspecialty • Train residents to care for an underserved population • Teach residents to manage medications not always used in ambulatory
training, such as opioid agonist therapy
• We hope improving resident ability to identify and treat addiction can improve job satisfaction and patient-provider relationships

Successes and Challenges
• Successes • Starting opioid maintenance medication in the hospital with good linkage and
follow-up rates • Resident enthusiasm and resident rotation • Response from services, nursing, and social work • Collaboration with outpatient programs and psychiatry • Some billing success • Synergy with concurrent hospital efforts to reduce readmissions

Professional Billing
Time period 83-12/25/2015 = 21
weeks Per week
RVUs 1027 49
Professional Charges $131,032 $6240
Charges Paid $37,608 $1791
Reimbursement rate 28.7%
Annualized charges paid (52weeks) $93,132

Subsequent readmissions, admissions, and ED use decrease after Addiction Medicine consult, but LOS increases slightly
23
2.92
2.12
Pre-consult After consult
Admission rate Average admissions per year
44.3%
12.2%
26.8%
Pre-consultIndex visitAfter consult
30d readmission rate Average admissions per year
10.0
6.6
Pre-consult After consult
ED utilization rate Average ED visits per year
4.6 5.9 5.5
Pre-consultIndex visitAfter consult
Inpatient length of stay Average length of stay, excluding outliers
Source: Internal BMC data; January 2015-December 2015

Although many teams are making use of the Addiction Medicine consult service, demand is multiple times current capacity
24
Penetration of Addiction Medicine consult service, July 2015-March 2016
Team Current penetration of c/s service
Total potential consults / day
General Internal Medicine 62% 3.1 Family Medicine 30% 1.1
Gen Surg + Trauma 4% 0.9 Hospitalist 58% 0.9
ID 69% 0.7 OB 11% 0.4
Geriatrics 7% 0.3 ICU 92% 0.3
Neurology 20% 0.3 Cards CHF 33% 0.2
CCU 13% 0.2 Heme/Onc 42% 0.2
Renal 31% 0.2 General Cards 50% 0.2
Ortho 25% 0.2 GYN 7% 0.2
Neurosurgery 41% 0.1 CT Surgery 42% 0.1
OMFS 0% 0.1 Vascular Surgery 0% 0.1
Hip Fracture 0% 0.1 ENT 18% 0.1
Other 0.1
• If all patients with active substance use were to be seen by the c/s service, there would be 10 new patient consults per day
• Major opportunities to increase penetration outside of Medicine include General Surgery / Trauma Surgery, Family Medicine, and OB/Gyn
• Addiction Medicine service is already seeking to increase penetration by participating on Readmission Risk Assessment BPA for High Risk and Super Utilizer patients
Source: Internal BMC data; May 2014-June 2015.

Successes and Challenges
• Challenges • Staffing
• Consistency • Capacity
• Post-hospital dispositions • Lack of a clear “owner” dedicated to bed search process Tracking outcomes
• Proving to the hospital that this is worth sustaining

Based on our initial experience, an ideal Addiction Medicine consult service would consist of:
26
Attending
Mid-level provider(s) /
trainee(s)
Transitions-focused RN
Bed finder (LPA, BSW)
Staffs all new consults and sees active follow-up patients daily (with efficient team, could be ~ 8 encounters per half-day)
• Performs all new consults and active / relevant follow-up patients daily
• Writes notes and bills for low-acuity follow-ups not requiring attending oversight (experienced mid-level provider only)
Communicates with outpatient treatment programs and provides necessary patient information to ensure successful enrollment
Dials for beds
Main activities AY2017 AY2018
0.5 FTE 1.0 FTE
1.0 FTE NP1 • 1.0 FTE NP • 0.8 FTE Fellow2
0.5 FTE 0.5 FTE
0.5 FTE 0.5 FTE
• ~8 encounters • 2-3 new consults
• ~10-12 encounters • 4-5 new consults
Daily work:
1 – No Addiction Medicine Fellows hired for AY2017 2 – Two potential Addiction Medicine Fellows hired for AY2018. Potential for GME funding, but remains uncertain

Outline
• Perceived need among nursing and residents • Description of service
• Curriculum for residents
• Patients seen • Treatment initiated • Linkage and follow-up • Successes and Challenges
Acknowledgements Paul Trowbridge, Payel Roy, and Alexandra Yurkovic
• Addiction Medicine Fellows • Zoe Weinstein, Todd Kerensky, Phoebe Cushman
• David Yuh • Linda Neville • Project ASSERT - John Cromwell • Psychiatry Consult and Liason Service • CSAC Bradston • OBAT Team • Jeffrey Samet and David Coleman • ACS attendings
• Amy Fitzpatrick, Zoe Weinstein, Theresa Kim, Jason Worcester, Christine Pace, Jeffrey Samet, Rich Saitz, Sarah Bagley, Sandra Gordon, Sheila Chapman, Jane Liebschutz, Dan Alford, Sarah Kimball
• ACS residents

Thank You! [email protected]


















