
Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October...
25
Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October 2009 Most recently updated: September 2013
-
Upload
abner-bennett -
Category
Documents
-
view
224 -
download
0
Transcript of Developed by Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed : October...

Developed by Kathy Wonderly RN, BSPA, CPHQPerformance Improvement Coordinator
Developed : October 2009Most recently updated: September 2013

To identify the patients who should receive a Beta blocker during the perioperative period.
To recognize the approved venous thromboembolism (VTE) prophylaxis for surgical patients.
To recognize the importance of the VTE prophylaxis being started with 24 hours before to 24 hours after surgery
Changes for January- September 2014 will be in italics.

This is the only cardiac measure in the current SCIP program.
Research has shown that mortality increases when patients who are on beta-blocker therapy prior to admission do not receive a beta-blocker during the perioperative period

For this measure the perioperative period is defined as the day prior to surgery through postoperative day two with day of surgery being day zero. It is expected that the patient will receive a dose the day before or the day of surgery, a dose on P.O. days 1 and 2.
If the patient’s length of stay is less that 2 days the administration of the beta blocker the day prior to or day of surgery only are assessed.
Nursing role
While ordering a medication is a physician responsibility, nurses should remind the physician that the patient was taking a beta blocker prior to admission.
Nursing or often anesthesia will administer the medication as ordered. Be sure to document the date and time of the administration.

As with the other indicators if the practitioner does not order a beta blocker for patients who are on one prior to admission. He/she must document the reason for not ordering this medication. This documentation must occur each day the medication is not ordered. Acceptable reasons include having a ventricular assist device or heart transplantation.
.

Acebutolol Atenolol Atenolol/chlorthalidone Betapace Betapace AF Betaxolol Bisoprolol Bisoprolol/fumarate Bisoprolol/hydrochlorothiazide Brevibloc Bystolic Carvedilol Coreg Corgard Corzide 40/5 Corzide 80/5 c Esmolol

Inderal Inderal LA Inderide Inderide LA InnoPran XL Labetalol Levatol Lopressor Lopressor HCT Lopressor/hydrochlorothiazide Metoprolol Metoprolol/hydrochlorothiazide Metoprolol Tartrate/hydrochlorothiazide Nadolol Nadolol/bendroflumethiazide Nebivolol Nebivolol HCL Nebivolol Hydrochloride

Penbutolol Toprol-XL Pindolol Trandate Propranolol Trandale HCL Propranolol HCL Visken Propranolol Hydrochloride Zebeta Propranolol/hydrochlorothiazide Ziac Sectral Sorine Sotalol Sotalol HCL Tenoretic Tenormin Tenormin I.V. Timolol Toprol
Specifications Manual for National Hospital Inpatient Quality
Measures Discharges 01-01-14(1Q14) through 09-30-14- (3Q14) Appendix C

The VTE measure requires that the ordered VTE prophylaxis is initiated within 24 hours prior to the anesthesia start time to 24 hours after the anesthesia end time. This is a nursing driven measure.

There are several groups of patients who are excluded from this indicator.
These include: Burn patients Patients whose total surgical time is less than 60 minutesPatients who stay less than two nights.Patients who are on oral anticoagulation
therapy prior to admission.

There are two types of prophylaxis. Pharmacological which include: Heparin
Low molecular weight heparin such as Lovonox
Factor Xa inhibitor fondaparinux –Arixtra
or Xarelto Warfarin (Coumadin)

2. Mechanical prophylaxis which include : Graduated Compression Stockings (GCS)
Intermittent Pneumatic Compression Devices (IPC)
Venous Foot Pump (VFP)

Years of research have identified that the type of procedure done drives the choice of VTE prophylaxis.
The following slides show the recommendations for each category of surgery.
While ordering prophylaxis is the responsibility of the practitioner, the nurses caring for post-op patients should look for some type of order or documentation as to why nothing was ordered.

Procedure Recommended prophylaxis
Elective Total Knee or Total Hip Replacement
Any of the followingLow molecular weight heparinFactor Xa inhibitor including oral route (Xarelto)WarfarinICPVFPLow molecular weight heparinAspirin
Hip Fracture surgery Low molecular weight heparinLow dose unfractionated heparinFactor Xa InhibitorWarfarinICPAspirin

General Surgery Low molecular weight inhibitorLow dose unfractionated heparinFactor Xa InhibitorIPC
Urologic Surgery Low molecular weight inhibitorLow dose unfractionated heparinFactor Xa InhibitorIPCPharmacological combined with IPC or GCS
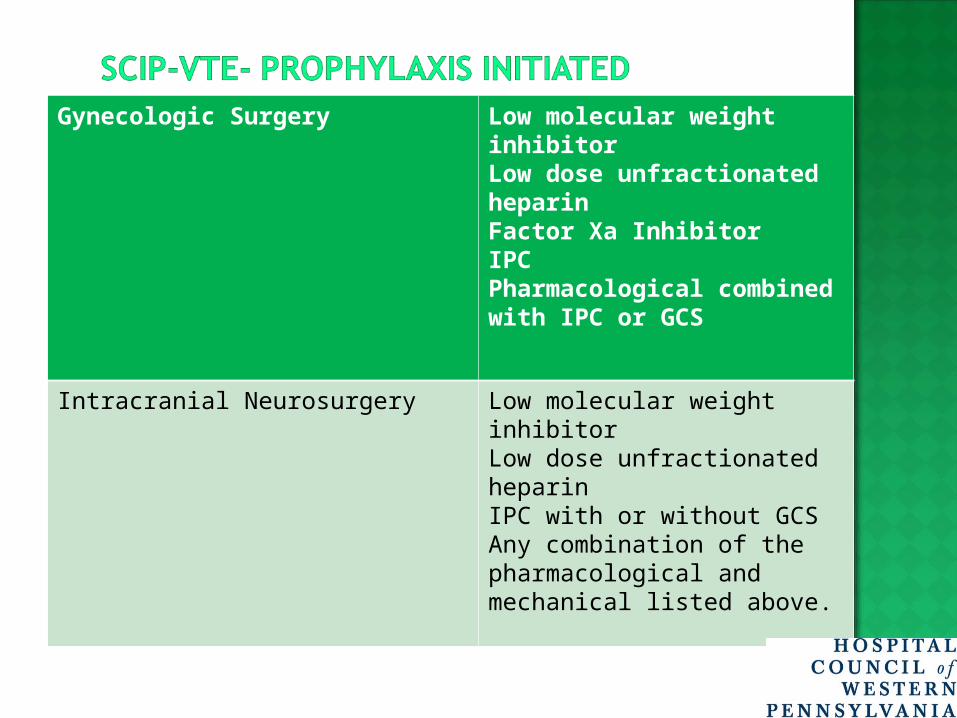
Gynecologic Surgery Low molecular weight inhibitorLow dose unfractionated heparinFactor Xa InhibitorIPCPharmacological combined with IPC or GCS
Intracranial Neurosurgery Low molecular weight inhibitorLow dose unfractionated heparinIPC with or without GCSAny combination of the pharmacological and mechanical listed above.

As you see in the previous charts the first choice of prophylaxis for VTE prevention is medication with or without any mechanical device use.
When the patient has a documented contraindication such as recent GI bleed , the mechanical device prophylaxis can be used alone.

Regardless of the treatment ordered it must be initiated in the time frame of 24 hours prior to anesthesia start time to 24 hours after the anesthesia end time.
Nursing and Pharmacy need to work together to assure the medications are available, administered and the start time documented within this window.

The SCIP core measure set is the most complicated of all. Not only are there the most measures but there are specific time limits designated for six of these indicators.
The role of nursing is huge. Not only do you need to know the recommendations but you must be sure that each measure is addressed within the designated timeframe.
As with the other CMS core measures each indicator requires an action and concise documentation.

Reducing the complications of surgery continues to be one of the National Patient Safety Goals and a goal of the health care reform movement.

1. Patients who are taking a beta blocker prior to arrival for surgery and receiving general anesthesia should have a dose given during the perioperative period which ends at discharge from PACU.
A. TrueB. False

2. The SCIP VTE measures will be met as long as you get that patient out of bed on post-op day 1.
A. True
B. False

3. Heparin or Lovonox can be given up to ____ hour(s) before anesthesia start time and still be considered appropriate treatment according to the SCIP guidelines.
A. 4 B. 16 C. 24 D. 48

4. The first choice for VTE prophylaxis is pharmacological with or without a mechanical device.
A. True
B. False


















