
Develop an E/M level service matrix to capture facility ... · PDF fileTo ensure that your...
12
To ensure that your facility’s doc- umentation supports the level of E/M service coded, develop an accurate matrix. Since E/M codes define the level of care provided, their accuracy drives the level of reimbursement. During an HCPro audio confer- ence in April, Yvonne Hoiland, CCS-P, CPC, CPC-H, RCC, and Charol Spaulding, CCS-P, CPC, CPC-H, PMCC, discussed methods to improve your facility’s — INSIDE— Develop an E/M level service matrix to capture facility-based ED revenue A documentation matrix for ED services can help your facility stay compliant and capture all appro- priate E/M revenue. Hospitals must continue to follow their outpatient E/M level coding until the proposed national guide- lines take effect, most likely in 2006, experts guess. Until then, your facility should focus on tight- ening any loopholes that may exist in your current E/M level system. If you receive denials for reason- able and necessary tests performed in your ED, faulty coding and in- complete documentation may not be to blame. If the practitioner doc- umented that he or she ordered the test based on the patient’s com- plaints and symptoms to meet Emergency Medical Treatment and Active Labor Act (EMTALA) screen- ing and stabilization requirements, you can appeal and probably get paid. The Medicare Prescription Drug Improvement and Modernization Act (MMA) requires reimburse- ment for these tests, but CMS has not yet changed its editing system to allow it, says Valerie Rinkle, MPA. “The problem is that the edits can- not decipher that the admitting diagnosis, not the principle diag- nosis, covers the code, so the claim will be denied,” she says. The MMA section 944 states, In the case of items and services required under EMTALA, deter- minations regarding whether the items and services were “reason- able and necessary” for purposes of Medicare coverage must be made on the basis of information available to the treating practition- er at the time the item or service was furnished. The frequency with which the item or service was pro- vided before or after the patient’s emergency room visit may not be taken into account. Appeal ED diagnosis testing denials Medical necessity tips for reimbursement > p. 2 Vol. 5 No. 6 June 2004 FOR PERMISSION TO REPRODUCE PART OR ALL OF THIS NEWSLETTER FOR EXTERNAL DISTRIBUTION OR USE IN EDUCATIONAL PACKETS, PLEASE CONTACT THE COPYRIGHT CLEARANCE CENTER AT WWW.COPYRIGHT.COM OR 978/750-8400. > p. 5 Do you know? How do you code both a clinic and an emergency visit for the same patient on the same day? You’d know if you read the APC Weekly Monitor on May 21 when it came into your mailbox. This free e-mail newsletter from HCPro answers difficult coding questions like this one every week. Go to the APC Weekly Monitor archives at www.himinfo.com/ apcezine/ezine_arc.cfm. Spotlight on E/M level matrix building BAPCs features a complete matrix-building tool kit in this issue. Experts give direct how-to advice, a sample matrix, and an E/M level coding quiz. It all starts here on the front page, and continues through p. 5. Coding Coach: Capsule endoscopy 7 Learn how to code those pesky “gutcams.” Coding in real life 8 Lolita Jones explains the ins and outs of paracentesis. Ready for ICD-10? 10 An Ohio facility shares its ICD-10 preparation to help you get geared up.
Transcript of Develop an E/M level service matrix to capture facility ... · PDF fileTo ensure that your...

To ensure that your facility’s doc-umentation supports the level ofE/M service coded, develop anaccurate matrix. Since E/M codesdefine the level of care provided,their accuracy drives the level ofreimbursement.
During an HCPro audio confer-ence in April, Yvonne Hoiland,CCS-P, CPC, CPC-H, RCC, andCharol Spaulding, CCS-P, CPC,CPC-H, PMCC, discussed methodsto improve your facility’s
— INSIDE—Develop an E/M level service matrixto capture facility-based ED revenue
A documentation matrix for EDservices can help your facility staycompliant and capture all appro-priate E/M revenue.
Hospitals must continue to followtheir outpatient E/M level codinguntil the proposed national guide-lines take effect, most likely in2006, experts guess. Until then,your facility should focus on tight-ening any loopholes that mayexist in your current E/M levelsystem.
If you receive denials for reason-able and necessary tests performedin your ED, faulty coding and in-complete documentation may notbe to blame. If the practitioner doc-umented that he or she ordered thetest based on the patient’s com-plaints and symptoms to meetEmergency Medical Treatment andActive Labor Act (EMTALA) screen-ing and stabilization requirements,you can appeal and probably getpaid.
The Medicare Prescription DrugImprovement and ModernizationAct (MMA) requires reimburse-ment for these tests, but CMS hasnot yet changed its editing systemto allow it, says Valerie Rinkle,MPA.
“The problem is that the edits can-not decipher that the admittingdiagnosis, not the principle diag-nosis, covers the code, so theclaim will be denied,” she says.
The MMA section 944 states, In the case of items and servicesrequired under EMTALA, deter-minations regarding whether theitems and services were “reason-able and necessary” for purposesof Medicare coverage must bemade on the basis of informationavailable to the treating practition-er at the time the item or servicewas furnished. The frequency withwhich the item or service was pro-vided before or after the patient’semergency room visit may notbe taken into account.
Appeal ED diagnosis testing denials Medical necessity tips for reimbursement
> p. 2
Vol. 5 No. 6June 2004
FOR PERMISSION TO REPRODUCE
PART OR ALL OF THIS NEWSLETTER FOR
EXTERNAL DISTRIBUTION OR USE IN
EDUCATIONAL PACKETS, PLEASE CONTACT
THE COPYRIGHT CLEARANCE CENTER
AT WWW.COPYRIGHT.COM OR
978/750-8400.
> p. 5
Do you know?How do you code both a
clinic and an emergency visitfor the same patient on the
same day?
You’d know if you read the APC Weekly Monitor on May
21 when it came into your mailbox. This free e-mailnewsletter from HCProanswers difficult coding
questions like this one everyweek. Go to the APC Weekly
Monitor archives at www.himinfo.com/
apcezine/ezine_arc.cfm.
Spotlight on E/M levelmatrix building BAPCs features a completematrix-building tool kit in thisissue.
Experts give direct how-toadvice, a sample matrix, and anE/M level coding quiz. It allstarts here on the front page,and continues through p. 5.
Coding Coach: Capsuleendoscopy 7Learn how to code those pesky“gutcams.”
Coding in real life 8Lolita Jones explains the insand outs of paracentesis.
Ready for ICD-10? 10An Ohio facility shares its ICD-10 preparation to help youget geared up.

to be put on a matrix. “They know which casesare most often lacking the information they needto code them,” says Hoiland.
• Nursing staff. Nurses know what procedures aremost often encountered in their ED, and are famil-iar with assigning different nursing functions a
point value. “Nurses are invaluable indeveloping your matrix,” saysHoiland. “They are best suit-ed to advise you from the
facility-side on a point system.”• Billing staff. Billersknow which services getbilled through the CDM
and which are coded di-rectly. They will be aware ofquirks in the system. “Prefer-ably, you want someone on
board who is intimately acquainted withthe chargemaster and how it functions,” says Hoiland.
What should be included in the matrix?• Services that do not have a CPT code. Any service
that has a CPT code should be coded separatelyand not listed on your matrix. If your facility doesnot code them as separate procedures, you aremistakenly bundling payment for these into yourlevel of service and leaving money on the table.
• Procedures that the chargemaster will not allowyou to charge from the ED revenue center. YourCDM may not allow specific procedures to be billedfrom the ED revenue center under certain circum-stances. For example, initial respiratory treatmentadministered by a nurse is on the sample matrixunder the 30-point value column because, althoughthere is a CPT code for this procedure, this facilityis not capable of charging respiratory care throughthe ED charging system because of a conflict inthe chargemaster with revenue centers. “If the fa-cility rectifies the conflict so it can code the CPTcode, then it will have to remove the service fromthe matrix and update its guidelines to avoid dou-ble-dipping,” says Hoiland.
E/M coding documentation.
“Your E/M levels have to be very well-documented,”says Hoiland. “How embarrassing if you’ve set yourown guidelines and then an audit finds you are notfollowing them, not to mention opening your facilityup to the risk of noncompliance and lostrevenue.”
Point nursing acuity v.patient classification Use a point system basedon nursing acuity to de-termine the facility E/Mlevels, as opposed to thepatient classification systemused most commonly forinpatient services, Hoilandrecommends. “The patientclassification system is based on levelingthe severity of illness or diagnosis and the intensityof service.”
Hoiland encourages facilities using the patient classi-fication system for determining outpatient E/M levelsto switch to a point nursing acuity system. “There istoo much potential for subjectivity when using thepatient classification system. It’s too complicated andthere is big risk of double-dipping,” she says.
The point nursing acuity system is more defendablefrom an audit standpoint, and there is less risk ofdouble dipping. The drawback is the system’s totalreliance on nursing documentation. If a nurse doesnot document a service, the facility loses reimburse-ment for that service, Spaulding says.
Use the following guidelines to develop a matrixthat will assist you in determining the level of service based on nursing acuity.
Who should help develop the ED matrix?• Coding and compliance staff. Coders review
records every day, and they know what is andisn’t available in medical records and what needs
Page 2 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
E/M matrix < p. 1
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Use a point system based on nursing acuity to
determine the facility E/M levels, as opposed to the
patient classification system used most commonly for inpatient services.

the HIM department. “It is best to have coders whohave been properly trained on the matrix codingfrom the records,” says Hoiland. “Coders are best atmaking objective coding decisions. Where they arelocated is entirely up to your facility.”
Editor’s note: Go to www.hcmarketplace.com/Prod.cfm?id=2435 for information about how to purchasethe tape of this audioconference, “Facility-based E/Mcoding made simple.”
About the sourcesYvonne Hoiland, CCS-P, CPC, CPC-H, RCC, is asenior coding consultant with Coding Continuum,Inc., of Tucson, AZ. Charol Spaulding, CCS-P, CPC, CPC-H, PMCC, isvice president of Coding Continuum, Inc. of Tucson,AZ.
Page 3Briefings on APCs—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
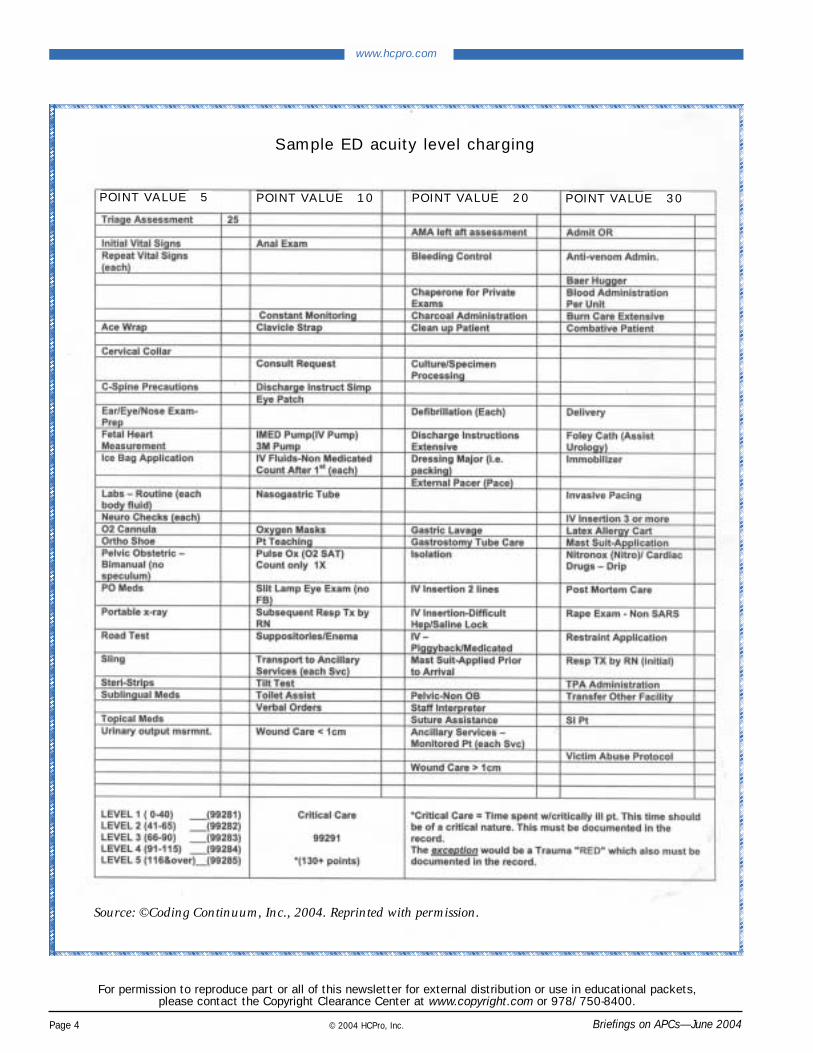
Your matrixA sample matrix for charging services in an EDusing an acuity level point system can be found onp. 4. Your matrix may need to list different proce-dures. Coding and billing staff can help decide whatservices are not captured by other methods. Nursingstaff can help determine the appropriate point acuitysystem for those procedures and services. Each facil-ity’s matrix will be different, says Hoiland. “It alwayssurprises me how every facility has its own separateset of billing issues.”
Coders, not nurses, should code Many facilities ask Hoiland who should code EDencounters and where staff should be located. Somefacilities have nurses post charges linked to CPT codeson the chargemaster. Other facilities place a coder inthe ED department, while others keep their coders in
Matrix sample reviewed
Yvonne Hoiland, CCS-P, CPC, CPC-H, RCC, ofCoding Continuum, Inc., of Tucson, AZ, explainssome services on the sample matrix on p. 4:
Initial triage is worth 25 points• Assign 25 points for triage of an ED patient
because it takes the most time in the beginning ofthe patient visit and is the most resource-intensive.
Don’t forget these five-point assessments• Assign five points every time vital signs are taken,
including the first time. • Assess five points when a nurse applies a sling
and instructs the patient on its use. Do not confusethis charge with coding separately for the supplyof the sling. The five points cover the cost of thenurse’s time and assistance, not the sling itself.
Clarifying 10-point assessments• Add 10 points for a consult request. This includes
the paperwork and time it takes the nursing staffto develop a consult for a patient.
• Document 10 points for each replacement of anonmedicated IV fluid bag. Because the IVcharge includes the initial IV bag, do not include
points for the initial bag. That’s considered doubledipping. Each time you change or replace a bagafter the first one, apply 10 points.
Record these 20-point services • Report 20 points for a chaperone, a person of the
same sex who stays in the room when a physicianof the opposite sex of the patient does an exam.
• Allocate 20 points for ancillary services, moni-tored patient. For example, this occurs when apatient is transported to the radiology departmentfor x-rays and is monitored constantly for vital signson the way. Nursing staff or a technician must staywith the patient the entire time. Do not confusethe description with bundling x-rays into the levelof service.
Use a 30-point value for cases requiring numerous resources• Add 30 points for addressing a combative patient,
because this process usually requires the help ofseveral nurses to make sure no one gets hurt.
• Add 30 points for monitoring a suicidal patient,because the situation requires constant surveillanceand many facility resources.
Page 4 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Source: ©Coding Continuum, Inc., 2004. Reprinted with permission.
Sample ED acuity level charging
POINT VALUE 5 POINT VALUE 10 POINT VALUE 20 POINT VALUE 30

Using the sample acuity level charging matrix provid-ed by Coding Continuum, Inc., on p. 4, add the num-ber of points for this patient visit and determine thecorrect level. The answer is on p. 9.
The details of the visit: A 16-year-old female presents to the ED complainingof nausea, vomiting, and dizziness. The ED staff takeher vitals (blood pressure, respiratory, temperature)and perform pulse oximetry (99%) and a neurologi-cal assessment.
Staff note the patient’s allergies, medications, and her prior medical history of diabetes, post-traumaticstress disorder, bipolar disorder, and depression.
She is triaged at 16:45. According to the nurse’snotes, the patient was given 1,000 cc of IV fluid at17:30 and another 400 CC at 18:30. Her routine fluidtests were sent to the lab at 17:30. Her Glasgow Coma
Score (15) is assessed at 19:00. Her vitals are takenagain at 19:35.
The patient states that she normally takes her insulinin the morning, but she had not had any in 36 hours.The nurse instructs the patient on diabetes and de-hydration care and follow up.
The doctor’s notes show the results of a urine analy-sis, which are not documented in the nursing report.The doctor documented the results of the finger-stick blood sugar—234 the first time, 173 the secondtime. He notes the patient ambulates well and hadpositive urine output.
The doctor diagnoses the patient as hyperglycemicwith uncontrolled diabetes. He recommends shereturn home and follow up if she is not feeling bet-ter within two to three days. Patient is released at21:00.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400
Page 5Briefings on APCs—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
ED case study: How many points of care?
Encourage documentation at time of orderTo ensure documentation at the time of the order, adda box in the order documentation for the ED physi-cian to indicate that he or she ordered the test(s) basedon the presenting condition of the patient, Rinklerecommends. This documentation will be useful ifyou need to appeal to Medicare. Also, other man-aged care plans that usually deny services orderedout of the ED may pay if you present the orderingdocumentation in this manner, she says.
To qualify for payment, the physician’s interpretationmust take place before the EMTALA screening iscomplete and the patient has been stabilized, saysRose T. Dunn, RHIA, CPA, FACHE, FHFMA.
Documenting the time the physician makes the inter-pretation for ordered tests is crucial in reimburse-ment, so educate ED physicians on the importance
of noting it in their dictation, written notes, or wetreads, she adds.
“If you can show the test was ordered for EMTALAand that the order was based on presenting condi-tions, you should get paid for that test,” Rinkle says.“As long as the test was ordered prior to the EMTALAscreening being completed, payers have to pay be-cause it falls under the umbrella of EMTALA.”
Interpretation report formats should include the fol-lowing elements to support medical necessity:
1. A place to document the treating physician/prac-titioner’s ordering indications
2. A space to document the technologist’s indica-tions taken from the patient
3. An area to document the interpreting physician’sfinal impression
Appeal testing denials < p. 1
> p. 6

Page 6 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Appeal testing denials < p. 5
LCDs and LMRPs may trip denials Coding that involves local coverage decisions (LCDs)and local medical review policies (LMRPs) may createunjustified denials. According to Rinkle, payers don’tkeep LCDs and LMRPs current with ICD-9 changes.
“You may be getting inappropriate rejections be-cause payers have not refined their edits out to thefifth digit of the ICD-9codes,” Rinkle says. “Thatis their system’s error.”
Rinkle is lobbying CMS tohold payers to the samedegree of detail it expectsfrom providers with regardto HIPAA transactions sets.“If providers must code tothe greatest specificity, thenpayers need to upgradetheir specificity, especiallysince grace periods havebeen eliminated,” she says.
Coach physicians to stayon top of LMRPs and LCDsto avoid missing ABN op-portunities, says Dunn. “ABNs must be given . . . withenough information so patients can make informeddecisions. It’s too late when they’re in their gownand swabbed,” she says.
Dunn knows facilities whose physicians use person-al digital assistants or palm solutions to keep currentwith LMRPs and LCDs. “At least CMS has moved theLMRPs and LCDs to one Web site (www.cms.hhs.gov/mcd), and when all LMRPs are converted to LCDsby December 2005, it will be easier to keep track ofchanges,” she says.
LCDs and LMRPs differ somewhat, says Dunn. “LCDswere established by the Benefits Improvement Protec-tion Act (BIPA), and fiscal intermediaries and carriersare allowed to explain whether they will cover a serv-ice . . . intermediarywide or carrierwide,” she says.
LCDs include a policy statement describing what is not covered, along with corresponding HCPCScodes. LMRPs describe what Medicare will cover.
“Fortunately LCDs cannot conflict with National CodingDecisions (NCDs). Therefore, it will be important fororganizations to review LCD denials and compare thedenied service to the services specified in the NCD.
If it is a covered service inthe NCD, then the denialshould be appealed,” shesays.
For the most definitiveguidelines for coding serv-ices and requirements ofdocumenting the order,look in the September 26,2001, Program MemorandumAB 01-144, says Rinkle.
“I recommend that facilitiesgo back and compare howtheir policies measure upagainst the guidelines inthis memo. Look at your
coding, ordering, and documentation policies and seeif you are following the rules,” she says. Go towww.cms.hhs.gov/manuals/ pm_trans/AB01144.pdf toreview the program memo.
Editor’s note: For more information about Medicaremedical necessity for outpatient services, go to www.hcmarketplace.com/Prod.cfm?id=2441 to purchase thetape of the HCPro audioconference “Medicare medicalnecessity for outpatient services,” in which both Dunnand Rinkle participated.
About the sourcesValerie Rinkle, MPA, is the revenue cycle director at Asante Health System in Medford, OR.Rose T. Dunn, RHIA, CPA, FACHE, FHFMA, ischief operating officer of First Class Solutions, Inc., inSt. Louis.
Diagnostic tests require UPIN numbers
Only the treating physicians or physician ornonphysician practitioners acting under theirscope of practice can order diagnostic tests.
For example, you can accept orders fromnurse practitioners, physician assistants,clinical nurse specialists, and others actingunder the scope of practice as long as youreport the unique physician identificationnumber (UPIN) of the nonphysician practitioner.

Page 7Briefings on APCs—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
BAPCs and its sister publica-tion, APC Answer Letter, havereceived several inquiries aboutcoding the new “gutcam” orcapsule endoscopy. The proce-dure was recently assigned a
new code, but coding for the procedure is not assimple as assigning the code. You must know yourlocal medical review policy (LMRP), says TiffanyNeally, RHIA, CCS, director of quality/remote cod-ing manager for Precyse Solutions in King Prussia,PA.
Review your own LMRP carefully“Don’t forget to check your LMRPto determine coverage conditionsin your state for the capsule en-doscopy procedure,” she says.
For example, Cahaba GovernmentBenefit Administrators, a fiscal in-termediary covering states in theMidwest, allows payment of thegutcam only for beneficiaries whohave one of the following:
• Continuing gastrointestinal (GI)blood loss and anemia second-ary to bleeding and who haveundergone upper GI endoscopy,colonoscopy, and either push enteroscopy orsmall-bowel radiologic study within the same peri-od of illness that failed to reveal a source of bleeding
• A prior small-bowel malignancy or radiologicallyidentified small-bowel pathology suggesting malig-nancy, which requires this study in follow-up.
There are other limitations under this LMRP. The testis
• not reimbursable for colorectal cancer screening
• payable only for services using FDA-approved devices
• not reimbursable for the confirmation of lesions orpathology normally within the reach of upper orlower endoscopes (lesions proximal to the liga-ment of Treitz or distal to the ileocecal valve)
• not payable for patients with hematemesis
• covered when performed by physicians trained inendoscopy or independent diagnostic-testing facili-ties under general supervision of a physiciantrained in endoscopy procedures
Common denial causesInaccurate ICD-9-CM codes, theabsence of the treating physi-cian’s order, or more than oneservice per episode of illnessreported account for the mostcommon denial reasons for thisprocedure under Cahaba Govern-ment Benefit AdministratorsLMRP.
And in some cases, Medicarecoverage does not include screen-ing procedures of the smallbowel.
How the procedure worksCapsule endoscopy is a non-
invasive diagnostic-imaging device for viewing theGI tract, especially the small bowel, which is notaccessible through standard upper endoscopy andcolonoscopy.
The patient swallows a small capsule (approximately11 mm x 26 mm) that contains a disposable mini-camera that transmits video pictures as peristalsispropels the capsule through the GI tract. As the cap-sule passes through the GI tract, the signal calculatesits position.
“The images are viewed on a computer terminal thatcan read the results once they are downloaded fromthe data recorder belt,” Neally explains.
Review your LMRP before coding ‘gutcam’
GI tract capsule endoscopy (interimAPC 1508, $650, national unadjusted“S” status indicator). For dates ofservice prior to January 1, 2004, re-port G0262, small intestinal imaging;intraluminal, from ligament of Tre-itz to the ileo cecal valve, includesphysician interpretation and report.Payers that do not accept HCPCSLevel II codes may prefer 91299,unlisted diagnostic gastroenterolo-gy procedure.
Capsule endoscopy,CPT 91110
> p. 12

Page 8 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Real-life coding: Ultrasound-guided paracentesis and fluid aspiration Test your skills on this actual coding scenario
Editor’s note: BAPCs and Lolita M. Jones, RHIA, CCS, of
Lolita M. Jones Consulting in Fort Washington, MD,bring you this month’s coding quiz on how to codemore than one procedure performed on the samepatient during the same visit.
Use the information provided to code the case, andcheck your answer against the one provided by Joneson p. 12.
What you need to know to code this caseThe following is adapted from the Medicare HospitalManual, Section 442.9, “Use of Modifiers in Report-ing Hospital Outpatient Services.”
Use modifier -59 to identify procedures/services thatare not normally reported together, but may be per-formed during the same visit under certain circum-stances.
This may represent a different session or patientencounter, procedure or surgery, site or organ sys-tem, incision, or injury not ordinarily encountered or
performed on the same day by the same physician.Use this modifier to indicate that a procedure or serv-ice was distinct or independent from other servicesperformed on the same day.
For example, procedures 23030 (incision and drainage,shoulder area: deep abscess or hematoma) and 20103(exploration of penetrating wound [separate proce-dure]; extremity) are performed on the same patienton the same day.
If these two codes were billed together withoutmodifier -59, code 20103 would be denied as dupli-cate billing.
Because the incision and drainage of the shoulder(code 23030) is the definitive procedure, any explora-tion of the area (20103) preceding this is consideredpart of the procedure. However, if the explorationprocedure (code 20103) was conducted on a dif-ferent part of the same limb or on a different limb,adding the -59 modifier to either code 20103 orcode 23030 would explain the circumstance andprevent a denial.
An elderly male with end-stage liver and heart failurepresents for drainage of recurrent ascites, or accumu-lation of fluid in the abdomen. A needle is insertedthrough the abdominal wall into the peritoneal cavityto obtain a sample of fluid. This test may be donein an office setting, a treatment room, or hospital.
After a local anesthetic is applied, the needle isinserted 1 in–2 in into the abdomen. Sometimes asmall incision is made to help insert the needle. Asample of fluid is then withdrawn into a syringe.
The needle is removed and a dressing is applied to
Case study: Paracentesis, fluid aspiration in the ED
the puncture site. If an incision was made, one ortwo stitches may be used to close it.
The operative report says ultrasound-guided para-centesis and ultrasound-guided fluid aspiration start-ed at 10:20 a.m. and ended at 12:17 p.m.
Ultrasound was used to identify free ascites in theleft-upper quadrant and a loculated pocket ofascites in the left-lower quadrant of the abdomenjust lateral to the ostomy site.
The patient gave verbal consent after the risks and

Page 9Briefings on APCs—June 2004 © 2004 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
www.hcpro.com
Answer to E/M leveling case study
The correct answer is 80 points, level 3, code99283.
You should have checked 25 points for triage,five points for each time vitals were taken (10),five points for each neuro check (10), five pointsfor routine lab tests, and 10 points for the sec-ond IV fluid bag, 10 points for the pulse oxime-try, and 10 points for the simple dischargeinstructions given by the nurse.
The total could have been 85 if the nurse haddocumented the physician’s interpretations ofthe urine analysis test, but in this case the extrafive points does not change the level.
However, because most coders rely on the nurs-ing flow sheet for their information, YvonneHoiland, CCS-P, CPC, CPC-H, RCC, suggestsif you see this type of documentation happen-ing in your facility, it is a good opportunity touse it as a learning tool for your staff.
benefits were explained. Patient’s left abdomen wasprepped and draped in a standard sterile fashion.
Results of the ultrasound-guided paracentesis: Pre-liminary ultrasound revealed a moderate-sized areaof ascites in the left-upper quadrant. A suitable entrysite was chosen and the area was anesthetized with1% lidocaine.
Under direct ultrasound visualization, a micropunc-ture needle was advanced into the peritoneal space.
A straw-colored ascetic fluid was immediately re-moved via the needle. Using standard guide wireand catheter technique, a 6 French APD was placedin the left-upper quadrant for drainage of the fluid.
This was followed by aspiration of 5600 cc of straw-colored, slightly cloudy peritoneal fluid. The catheter
was then removed and hemostasis was obtained.
Results of the ultrasound-guided fluid aspiration:Preliminary ultrasound of the left-lower quadrantrevealed a loculated fluid collection just lateral tothe patient’s ostomy. A suitable entry site was cho-sen and the area was anesthetized with 1% lidocaine.Under direct ultrasound visualization, a micropunc-ture needle was then advanced into the fluid collection.
There was immediate return of clear ascetic fluid. Using standard guide wire and catheter technique, a6 French APD was then placed into the left-lowerquadrant for drainage of fluid.
This was followed by aspiration of 350 cc of clearascetic fluid with multiple small mucous shreds.
Additional drainage was unsuccessful due to themucous shreds. The APD catheter was removed.Ascetic fluid continued to drain from the access sitefor approximately five minutes. The site was thencovered with a dressing.
The patient tolerated the procedure well withoutany immediate complications. The patient was thenmonitored for approximately 30 minutes, duringwhich vital signs remained stable. He was transport-ed back to hospice care.
He will return in one week for a repeat paracente-sis. Written documentation of the procedure wassent with the patient back to hospice care.
Findings: Ultrasound revealed a moderate amountof free ascites in the left-upper quadrant and a small-sized loculated pocket of ascitic fluid in the left-lowerquadrant just lateral to the patient’s ostomy site.
Impression: Technically successful drainage of theleft-upper quadrant ascitic fluid by ultrasound guid-ance with 5600 cc of ascetic fluid removed andof left-lower quadrant loculated fluid pocket by ultra-sound guidance with 350 cc of clear ascitic fluidwith multiple mucous shreds removed.
Turn to p. 12 for the correct coding for this case.

Page 10 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
By Randy Wagner BSN, RN, CCS
The ICD-10-CM coding system could take effect assoon as 2007. When the data is announced in theFederal Register, providers will have only 24 monthsto prepare for implementation. With much to do,only good planning will make it happen.
Our facility has invested in researching best practicesfor the inevitable change to ICD-10. After attendingseveral seminars and studying articles on the subject,we are now planning. The first order of business:deciding who in our facility needs to involved. Weplan to use lessons learned during APC implementa-tion to avoid some of the same pitfalls. Because pit-falls will vary from one organization to the next, eachfacility should review its challenges during the APCtransition.
If you haven’t already, form a steering committee toprovide guidance and support for the implementa-tion. Take the following steps: • Begin budget provision and information services
(IS) analysis • Organize an action plan for implementation • Start education for documentation within six months
to a year, and train coders not more than six monthsbefore the go-live date
Include staff from the following on the committee:
• ISDue to the increased specificity of ICD-10, the ISdepartment will need to implement a system thatallows up to seven alphanumeric characters insteadof the five currently used for ICD-9, replace ICD-9software with new ICD-10 software, and develop asystem for conversion or a crosswalk to interfacecode entry and electronic billing.
• Financial servicesThe financial department will have to rework the bud-get to include the expenses of implementation, conver-sion, and education needed to transition to ICD-10.
The practice of billing quickly to get money backdeveloped in the fee-for-service days will no longerproduce a desirable outcome. You’ll have to create anew definition of accounts receivable (A/R). A/Rshould no longer be all records for billing, but onlythose with complete content. Allow time for all diag-nostic reports to become available or clarificationqueries to the physician to be made.
Restructuring a system with the foresight to makedocumentation available for coding could reap greatrewards for the organization. If necessary, considercreating a way to facilitate accurate and timely docu-mentation from physicians or other medical profes-sionals, such as electronic charting. If you rush cod-ing without specific documentation, the inaccurate
Form steering committee for smooth transition to ICD-10
BAPCS Subscriber Services Coupon Your source code: N0001
Name
Title
Organization
Address
City State ZIP
Phone Fax
E-mail address(Required for electronic subscriptions)
❑ Payment enclosed. ❑ Please bill me.❑ Please bill my organization using PO # ❑ Charge my: ❑ AmEx ❑ MasterCard ❑ VISA
Signature(Required for authorization)
Card # Expires(Your credit card bill will reflect a charge to HCPro, the publisher of BAPCS.)
❑ Start my subscription to BAPCS immediately.
Options: No. of issues Cost Shipping Total
❑ Print 12 issues $229 (BAPCSP) $18.00
❑ Electronic 12 issues $229 (BAPCSE) N/A
❑ Print & Electronic 12 issues of each $286 (BAPCSPE) $18.00
Sales tax(see tax information below)*
Grand total
Order online atwww.hcmarketplace.com and save 10%
Be sure to enter source code N0001 at checkout!
*Tax Information Please include applicable sales tax. Electronic subscriptions are exempt.States that tax products and shipping and handling: CA, IL, MA, MD, NJ,VA, VT, FL, CT, GA, IN, MI, NC, NY, OH, PA, SC, TX, WI. States that tax prod-ucts only: AZ, TN. Please include $21.95 for shipping to AK, HI, or PR.
Mail to: HCPro, P.O. Box 1168, Marblehead, MA 01945 Tel: 800/650-6787 Fax: 800/639-8511 E-mail: [email protected] Web: www.hcmarketplace.com

Page 11Briefings on APCs—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
billing that will result will severely affect strategicplanning, resource utilization, facility and physicianprofiling, and contract negotiations.
• Billing and coding personnelTrain each coder and biller in how to code a healthrecord using ICD-10. Plan on some staff membersleaving the organization as a result of this transition,particularly those nearing retirement, because theydon’t want to learn a new coding system. By remain-ing positive and assuring them that the transition willnot be difficult, you can keep your loss to a minimum.Go to www.aha.org for a report on field testing or goto www.ahima.org and click on the site’s “Body ofKnowledge” for the complete ICD-10 field test report.
You will need to review and collect more clinical datafrom the health record for accurate coding. Manage-ment will have to allow more time for coders to re-ceive those reports. Develop a system for prioritizingthe charts for coding based on your most commonpayer (commercial or Medicare/Medicaid), as well asthe priority of the facility and office manager.
Consider the need for staff coverage while coders
train for ICD-10. Depending on the style of trainingthat the organization selects, the coder will be in aclassroom for 16–32 hours. You may also want toallow a grace period to ease coders into the newsystem.
In the American Health Associaion field test report,participants reported that although coding with ICD-10initially took longer, ease of coding rapidly increased.Some reported the ICD-10 system was easier and lessfrustrating than ICD-9 and took equal or less time tocode the chart.
• Medical servicesThe coding system change will affect physicians, nurs-ing, and other allied medical personnel documenta-tion and diagnostic reports. Physicians must knowthe standardization of terminology of ICD-10 so theyprovide the right information in their documentationfor accurate code selection. Train by department orspecialty to address the terminology relevant to spe-cific physicians, especially surgeons.
Assist physicians through this transition with tools totransform lists of symptoms, lab findings, and diag-nostic reports into an accurate portrayal of their pa-tients’ illnesses. It is important that they understandthat all their documentation in every setting—inpa-tient, outpatient, or their own office—must be spe-cific and expanded.
Once each department understands what it mustaccomplish, the steering committee must determinethe best way to accomplish these goals. Try the following: • Educate staff on coding system changes• Develop capital and multi-year budgets• Assist departments in determining their educational
needs • Develop an action plan and monitor progress• Commit to achieving a smooth, successful
transition
About the sourceRandy Wagner, BSN, RN, CCS, is the education co-ordinator in the documentation department for Ohio-Health, a Columbus-based, not-for-profit, charitableorganization serving and supported by the community.
Sources to prepare for ICD-10
• U.S. prerelease drafts posted on National Center for Health Statistics Web sitewww.cdc.gov/nchs/icd9.htm
• Copy of article from For the Record, Preparingfor ICD-10, www.3m.com/us/healthcare/his/icd-10.jhtml
HIPAA glossary
• www.3m.com/us/healthcare/his/HIPAA/resources.jhtml
• www.wedi.org/public/articles/HIPAA_GLOSSARY.pdf
• http://aspe.os.dhhs.gov/admnsimp/index.shtml
Source: Randy Wagner of OhioHealth. Reprintedwith permission.

Page 12 Briefings on APCs—June 2004© 2004 HCPro, Inc.
www.hcpro.com
Briefings on APCsEditorial Advisory Board
Publisher/Vice President: Suzanne PerneyGroup Publisher: Lauren McLeodManaging Editor: Robin Robinson [email protected]
Dave FeeProduct manager3M Health Information SystemsMurray, UT
Frank J. Freeze, LPN, CCS, CPC-HPrincipal, The Wellington GroupValley View, OH
Carole L. Gammarino, RHIT, CPURRecruiting management, HIM servicesPrecyse SolutionsKing of Prussia, PA
Briefings on APCs (ISSN: 1530-6607) is published monthly by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. Subscription rate: $229/year. • Periodicals postage paid, Marblehead, MA01945 and other mailing offices. Postmaster: Send address changes to BAPCs, P.O. Box 1168, Marblehead, MA 01945. • Copyright 2004 HCPro, Inc. All rights reserved. Printed in theUSA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, Inc., or the Copyright ClearanceCenter at 978/750-8400. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For renewal or subscription information, call customer service at 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/ven-dors. If you do not wish to be on this list, please write to the Marketing Department at the address above. • Opinions expressed are not necessarily those of BAPCs. Mention of productsand services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions. CPT codes, descrip-tions, and material only are Copyright 2001 American Medical Association. CPT is a trademark of the American Medical Association. All Rights Reserved. No fee schedules, basic units,relative values, or related listings are included in CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS restrictions apply to government use.
Susan Garrison, CPC, CCS-P, CPC-H, CPARSenior manager, 3M HIS Consulting ServicesAtlanta, GA
Diane R. Jepsky, RN,MHA, LNCExecutive vice president, Coding and ComplianceCodeCorrect, Inc.Yakima, WA
Lolita M. Jones, RHIA, CCSLolita M. Jones Consulting ServicesFort Washington, MD
Jugna Shah, MPHPresident, Nimitt ConsultingSt. Paul, MN
Rita Scichilone, MHSA, RHIA, CCS, CCS-P, CHCPractice manager, Coding Products and ServicesAmerican Health Information Management AssociationChicago, IL
Lois Yoder, RHIT, CCSThe enVision GroupNaples, FL
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
www.hcpro.com
Answer to real-life coding quiz
Use codes 49081 and 49081-59 to code the case on p. 8.
Per the operative report, the patient presents fordrainage of recurrent ascites. Since this was notthe first drainage procedure performed on thispatient, assign code 49081 (subsequent peritoneo-centesis, abdominal paracentesis or peritoneallavage).
The second paracentesis was performed on a dif-ferent site, making it a separate and distinct pro-cedure from the first one, requiring modifier -59.“Modifier -59 signals the payer that your documen-tation will show why both procedures are legiti-mate and deserve reimbursement,” says Jones.
Coding Coach < p. 7
The capsule passes naturally from the body with thestool, and because it is disposable, is not recovered.
This test is used for the diagnosis of obscure GI
bleeding when the site has not previously beenidentified by upper GI endoscopy, colonoscopy,push enteroscopy, or radiologic procedure. It maybe especially helpful in the diagnosis of angioec-tasias of the GI tract.
Use code 91110The new CPT-4 code assignment for this procedure,91110, “Gastrointestinal tract imaging, intraluminal(e.g. capsule endoscopy) esophagus through ileum,with physician interpretation and report” took effectJanuary 1, 2004, Neally says.
Check the index of the CPT-4 coding book underGastrointestinal Tract. “You will find a subtitle of‘Imaging, Intraluminal,’ and the code 91110. If youlook up code 91110 in the tabular section of theCPT coding book, you will find two notationsbeneath the code description,” she says.
The notations state, “Visualization of the colon is anintegral part of the procedure and is not reportedseparately; and because of this, if the physician doesnot perform the visualization of the ileum, he mustreport 91110 with modifier -52 appended to indicatethat the procedure was reduced.”
















![INTEGRATED TRUSTED SYSTEMS DEVELOPMENT …systems outlined in "Developing Trusted Systems Using DOD-STD-2167A" by T. Benzel [Ben89] and to elaborate the corresponding doc-umentation](https://static.fdocuments.in/doc/165x107/5ec95a75e92aff32af2fdde3/integrated-trusted-systems-development-systems-outlined-in-developing-trusted.jpg)

