
Determining the Risk of Stroke in AF
16
1 Determining the Risk of Stroke in AF Lalit Kalra Professor of Stroke Medicine Dept of Basic and Clinical Neurosciences King’s College London PAF, diagnosed opportunistically 2 yrs ago Type 2 Diabetes, Hyperlipidemia, NSTEMI 5 years ago Non-smoker, Drinks half a bottle of wine a day DH: Metformin, Ramipril, Simvastatin, Aspirin Pulse 78 reg, BP= 150/84, no signs of CCF or heart murmurs Bloods: Normal FBC, LFTs, Glu, electrolytes, Cr (eGFR 52ml/min) Normal TFT ECG + 24 h ECG: NSR 7 day event recorder ECG: X3 paroxysmal AF > 30sec, asymptomatic Echo: Preserved LV systolic function – EF 60%, Moderate LA enlargement 4.2cm, no valve abnormalities Mrs W-T 69 yrs F
Transcript of Determining the Risk of Stroke in AF

1
Determining the Risk of Stroke in AF
Lalit Kalra
Professor of Stroke Medicine
Dept of Basic and Clinical Neurosciences
King’s College London
PAF, diagnosed opportunistically 2 yrs ago
Type 2 Diabetes, Hyperlipidemia, NSTEMI 5 years agoNon-smoker, Drinks half a bottle of wine a day
DH: Metformin, Ramipril, Simvastatin, Aspirin
Pulse 78 reg, BP= 150/84, no signs of CCF or heart murmurs
Bloods: Normal FBC, LFTs, Glu, electrolytes, Cr (eGFR 52ml/min)
Normal TFT
ECG + 24 h ECG: NSR7 day event recorder ECG: X3 paroxysmal AF > 30sec, asymptomatic
Echo: Preserved LV systolic function – EF 60%, Moderate LA enlargement 4.2cm, no valve abnormalities
Mrs W-T 69 yrs F

2
Questions:
What are the risks of this patient suffering an ischaemic stroke?
How will you assess the risk?
Is there a difference in risk of an ischaemic stroke between persistent and paroxysmal AF?
Dec 2011
Atrial FibrillationStratification of stroke risk: CHADS2 score
Gage BF et al. JAMA 2001;285:2864–2870
Score
CHF or LV dysfunction 1
Hypertension 1
Age >75 years 1
Diabetes 1
Stroke/TIA 2
CHADS2 score
Adjusted Stroke Rate
(per 100 pt years)
0
4
8
12
16
20
0 1 2 3 4 5 6

3
Stroke risk assessment with CHA2DS2-VASc
CHA2DS2-VASc criteria Score
Congestive heart failure/left ventricular dysfunction
1
Hypertension 1
Age ≥75 yrs 2
Diabetes mellitus 1
Stroke/transient ischaemic attack/TE
2
Vascular disease(prior myocardial infarction, peripheral artery disease or aortic plaque)
1
Age 65–74 yrs 1
Sex category (i.e. female gender)
1
CHA2DS2-VASc total score
Rate of stroke/other TE (%/year)*
0 0.0
1 1.3
2 2.2
3 3.2
4 4.0
5 6.7
6 9.8
7 9.6
8 6.7
9 15.2
* Theoretical rates without therapy: assuming that warfarin provides a 64% relative reduction in TE risk (2.7% ARR), based on Hart et al.
Stroke risk persists even in asymptomatic/paroxysmal AF
The risk of stroke with asymptomatic or paroxysmal AF is comparable to that with permanent AF
Annual risk
of
stro
ke (
%)
Observed rate of ischaemic stroke
Stroke risk category
Low Moderate High0
2
4
6
8
10
12
14 Intermittent AF
Sustained AF

4
Antithrombotic strategy: what are the options?
1. Continue aspirin
2. Stop aspirin and commence oral anticoagulation
3. Others
Limited efficacy of Aspirin in reducing the risk of stroke in patients with AF
Random effects model; Error bars = 95% CI; *P>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic); QOD = every other day
RRR (%)†
100 –10050 0 –50
AFASAK
SPAF
EAFT
ESPS II
Aspirin better Placebo better
LASAF125 mg/d
125 mg QOD
UK-TIA300 mg/d
1200 mg/d
JAST
All trialsRRR = 19%*
(95% CI: –1 to 35%)
8

5
Low dose aspirin in low risk patients
Kaplan-Meier survival curves for primary end points (a) and for primary plus secondary end points (b).
Aspirin associated with an increased risk of major bleeding (7 patients; 1.6%) compared with the control group (2 patients; 0.4%;p= 0.101).
Primary:cardiovascular death, stroke or TIA
Secondary:non-cv death, ICH, major bleeding, and peripheral embolisation.
Warfarin reduces the risk of stroke in NVAF
Random effects model; Error bars = 95% CI; *P>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic)
Warfarin better Placebo better
RRR (%)†100 –10050 0 –50
AFASAK
SPAF
BAATAF
CAFA
SPINAF
EAFT
All trialsRRR 64%*
(95% CI: 49−74%)

6
Warfarin v Aspirin for stroke prevention in NVAF
Random effects model; error bars = 95% CI; *P>0.2 for homogeneity; †Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic)
RRR (%)*
100 –10050 0 –50
AFASAK I
AFASAK II
EAFT
PATAF
Warfarin better Aspirin better
Chinese ATAFS
SPAF IIAge ≤75 yrsAge >75 yrs
All trialsRRR 38%
(95% CI: 18–52%)
OAC v ASPIRIN in patient >75 yrs
973 patients aged 75 years with AF
Warfarin (INR 2–3) or aspirin (75 mg/day)
Follow-up for 2·7 years
Primary endpoint: fatal or disabling stroke (ischaemic or haemorrhagic), intracranial haemorrhage, or clinically significant arterial embolism

7
Dec 2011
HAS-BLED risk criteria Points awarded
Hypertension 1
Abnormal renal and liver function (1 point each) 1 or 2
Stroke 1
Bleeding 1
Labile INRs 1
Elderly (e.g. age >65 years) 1
Drugs or alcohol (1 point each) 1 or 2
Maximum 9 points
INR = international normalised ratio
Assessment of bleeding risk
Dec 2011
ESC Guidelines for AC in AF
Aspirin plus clopidrogel or, less effectively, aspi rin only, should be considered in patients who refuse any OAC or cannot tolerate anticoagulants for reasons unrelated to bleeding

8
Offered Warfarin, risks and benefits explained
Declined:
• “told” risk not high with PAF
• unwilling to have regular blood tests
• anxious regarding risk of bleeding
• Concern about lifestyle changes
“Best” treatment option for Mrs W-T
Presented to ED 4/12 later with acute onset of:
• Left face, arm and leg weakness
• Dysarthria
• L visual and sensory inattention
NIHSS = 9, BP=160/90, BM=5.2 mmols
What happened next to Mrs W-T
9
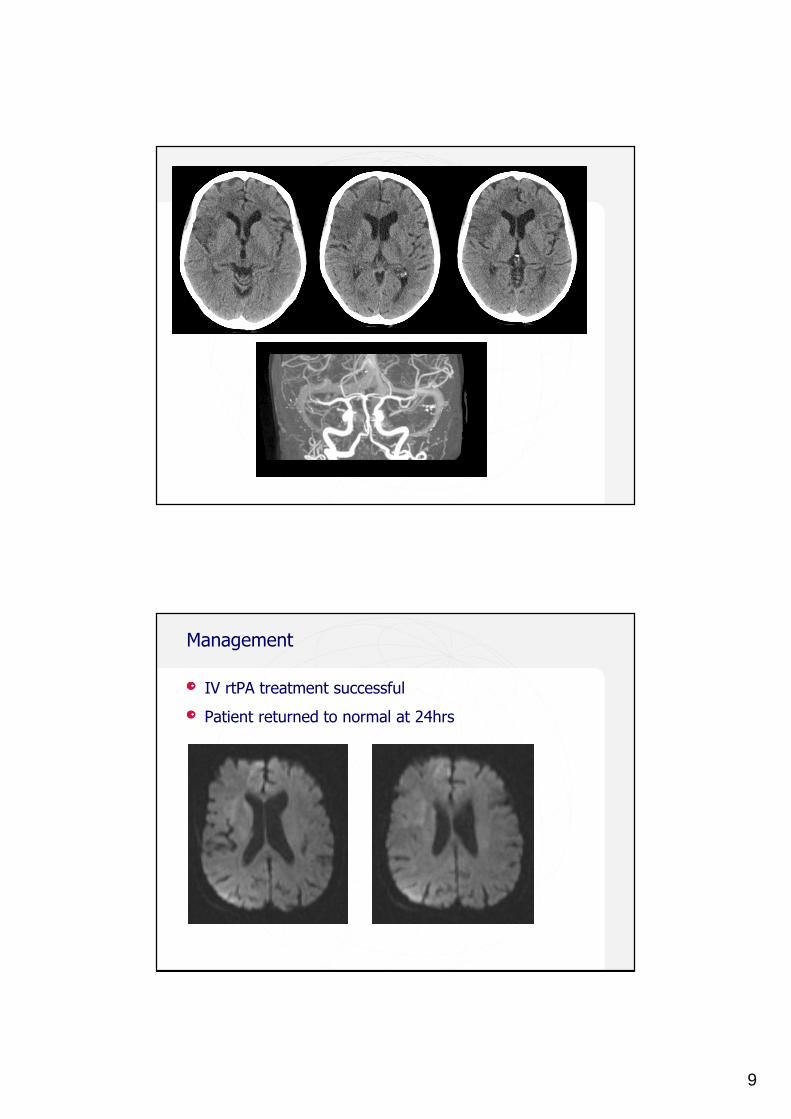
Management
IV rtPA treatment successful
Patient returned to normal at 24hrs

10
Antithrombotic strategy: what would you do next?
1. Offer oral anticoagulation
2. Offer NOAC
3. Other
What should we do next for Mrs J-T?
69 yr female with PAF
T2DM (metformin)
Half a bottle of wine/day
Recent stroke on Aspirin
The story continues
Presents to ED 2/12 later
– Not feeling well
– Headache and malaise
– Difficulty in walking, no falls
– Dysarthric and confused
Bilateral weakness, sensation difficult to assess
Upgoing plantars
ITTR < 60%, INR > 5 x2 since discharge
INR 4.4
69 yr female with PAF
T2DM (metformin)
Half a bottle of wine/day
Recent stroke on Aspirin
Now warfarinised

11
Dec 2011
Warfarin utilisation in practice
0 500 1000 1500 2000
Survival to stroke (days)
0.6
0.7
0.8
0.9
1.0
Cu
mu
lati
ve
su
rviv
al
71–100%
Warfarin group
61–70%
51–60%
41–50%
31–40%
<30%
Non warfarin
There are no guidelines for the management of symptomatic chronic SDH
– surgical evacuation if clot thickness ≥10 mm
– Conservative management for 30 to 45 days, may produce complete recovery alone
Managed conservatively, improved

12
Dec 2011
Stroke risk assessment with CHA2DS2-VASc
CHA2DS2-VASc criteria Score
Congestive heart failure/left ventricular dysfunction
1
Hypertension 1
Age ≥75 yrs 2
Diabetes mellitus 1
Stroke/transient ischaemic attack/TE
2
Vascular disease(prior myocardial infarction, peripheral artery disease or aortic plaque)
1
Age 65–74 yrs 1
Sex category (i.e. female gender)
1
CHA2DS2-VASc total score
Rate of stroke/other TE (%/year)*
0 0.0
1 1.3
2 2.2
3 3.2
4 4.0
5 6.7
6 9.8
7 9.6
8 6.7
9 15.2
* Theoretical rates without therapy: assuming that warfarin provides a 64% relative reduction in TE risk (2.7% ARR), based on Hart et al.
HAS-BLED risk criteria Points awarded
Hypertension 1
Abnormal renal and liver function (1 point each) 1 or 2
Stroke 1
Bleeding 1
Labile INRs 1
Elderly (e.g. age >65 years) 1
Drugs or alcohol (1 point each) 1 or 2
Maximum 9 points
INR = international normalised ratio
Assessment of bleeding risk

13
Dec 2011
What would you do for secondary prevention?
Switch back to aspirin
Start aspirin and clopidrogel
Continue anticoagulation
Other
Dec 2011
ACTIVE: Dual antiplatelet therapy is superior to Aspirin alone but inferior to Warfarin
ACTIVE Investigators. N Engl J Med 2009;360:2066–78
Aspirin aloneAspirin (75–100 mg/d)
Dual antiplatelet therapyClopidogrel (75 mg/d) + Aspirin (75–100 mg/d)
HR 0.72(95% CI: 0.62–0.83)
P<0.0001
Stroke
Cum
ula
tive
inci
dence
Years
0.15
00.00
1 2 4
0.10
0.05
3
26
Oral anticoagulationVKA (target INR = 2.0–3.0)
RR 1.72(95% CI: 1.24−2.37)
P=0.001

14
Balancing risk using the CHADS2-VASc and HAS-BLED scores
Anticoagulation for AF in perspective
28
Meta-analysis of ischaemic stroke or systemic embolism
Favourswarfarin
Favoursother treatment
Warfarin vs.:
Placebo
Low-dose warfarin
Aspirin
Aspirin + clopidogrel
0.0Hazard ratio
2.00.5 1.0 1.5
Dabigatran (H), Apixaban
Dabigatran (L) Rivaroxaban

15
ICH: Novel agents v warfarin
Dec 2011
Left atrial ablation (LAAB)
Restoration of NSR
Reduction in stroke risk
Reduced need for anti-arrhythmic drugs
No/reduced need for lifelong anticoagulation
Restoration of mechanical function
Reversal of inflammation and EF (AF begets AF)
Reversal of hypercoagulation disorder

16
Dec 2011
LAAB as treatment for abolishing AF
Freedom for AF: 85% PAF, 72% persistent AF
Number of procedures:
– 1 procedure 46%
– 2 procedures 36%
– 3 procedure 13%
– 4 or more procedures 5%
75% of PAF and 60% of Persistent AF off anti-arrhythmics
OAC may not be required if sustained NSR (low CHADS risk)
Key messages
NVAF incl PAF is associated with high risk of stroke
All patients with AF need risk stratification for AC
Risk stratification needs to be individualised to patients
– Stroke and bleeding risk (CHADS-VASC and HASBLED)
– Lifestyles and concordance with treatment
Lower threshold for OAC, those with ≥1 stroke risk factors are eligible (ESC guidelines)
Suboptimal assessment or prevention INCREASES the risk of stroke or bleeding


















