Detection and management of DILI in NASH/NAFLD … · Detection and management of DILI in...
58
Detection and management of DILI in NASH/NAFLD subjects in drug development Naga Chalasani Indiana University School of Medicine Drug-Induced Liver Injury (DILI) Conference XVII June 2017
Transcript of Detection and management of DILI in NASH/NAFLD … · Detection and management of DILI in...

Detection and management of DILI in NASH/NAFLD subjects in drug
development
Naga ChalasaniIndiana University School of Medicine
Drug-Induced Liver Injury (DILI) Conference XVIIJune 2017
Presenter
Presentation Notes
# 1. As the NAFLD field has heated up, it has come up quite frequently that DILI is more common in patients with NAFLD. How do you monitor for it, given that there are baseline fluctuations in liver chemistries?

Why is this significant?
• Background prevalence of NAFLD is quite high (~ 20-35% of adult population)
• >150 clinical trials for NAFLD are registered at clinicaltrials.gov
• Elevated baseline aminotransferases and fluctuations are common.
Presenter
Presentation Notes
# 2. So why is this significant? I think most of you know NAFLD population prevalence is quite high. If you look with an MRI, it can be as high as 30 to 35 percent, and there are more than 150 clinical trials, various phases, phase one, two, and some three, more than 150 trials registered at clinicaltrials.gov. Elevated baseline aminotransferases are common. Sometimes you may even see increased alkaline phosphatase in the absence of an increase in ALT and NAFLD and the fluctuations are common. A little noisy and also adds to complexities. A sizable proportion of NAFLD, as well as NASH, even advanced fibrosis can exist with totally normal aminotransferases. We are talking on the order of 30 to 35 ALT is not uncommon in somebody with established NASH. So I think the field is interesting and also complex.

Aminotransferases and NAFLD
• Two thirds of adults with NAFLD by MRI will have normal ALT and AST levels
• AST and ALT levels fluctuate, but typically stay under 200 U/L range
• Autoantibodies (e.g., ANA and ASMA) are common and are largely an epiphenomenon
Presenter
Presentation Notes
# 3. I touched on this. The ALT and AST tend to fluctuate, but they tend to stay largely under 200 IU/liter, rarely 250. Once it goes beyond, and I think patients either may be on statins or maybe low-grade autoimmune liver disease, but not more than 250 typically. Autoantibodies are common. A third may have ANA and anti-smooth muscle antibody. Really I don't think that has any clinical significance. It could be a epiphenomenon. Also, increased ferritin is not uncommon in this patient population. Up to 500 and 600 ferritin levels are not uncommon.

NAFLD and risk for DILI
• No data to suggest that obesity or NAFLD are risk factors for all-cause DILI. May increase risk for liver damage from alcohol, methotrexate, or tamoxifen, but not well studied.
• DILI in patients with underlying liver disease may have worse outcomes
Presenter
Presentation Notes
# 4. Just as NAFLD doesn't increase the risk of all-cause DILI, I have not seen any evidence that the NAFLD increases all-cause DILI across all drugs. Maybe if you have underlying fatty liver disease you may be at a higher risk for methotrexate hepatotoxicity. Some of the data are contaminated with hep C patients. Not quite sure how rigorous those data are. There is some talk about tamoxifen may be more toxic if somebody has underlying NAFLD. Once again, it's written as a possibility but not rigorously tested. And alcohol, I think, pretty logically, but I don't think there are strong data to suggest.
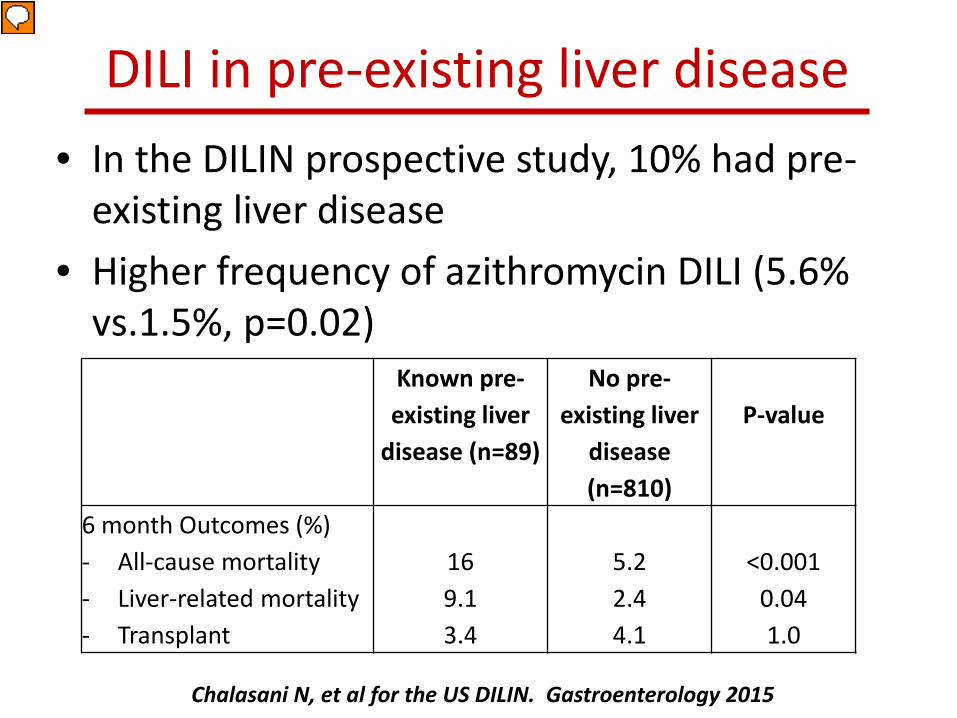
DILI in pre-existing liver disease• In the DILIN prospective study, 10% had pre-
existing liver disease• Higher frequency of azithromycin DILI (5.6%
vs.1.5%, p=0.02)Known pre-existing liver
disease (n=89)
No pre-existing liver
disease (n=810)
P-value
6 month Outcomes (%)- All-cause mortality- Liver-related mortality- Transplant
169.13.4
5.22.44.1
<0.0010.041.0
Chalasani N, et al for the US DILIN. Gastroenterology 2015
Presenter
Presentation Notes
# 5. Maybe we have 10 - 15 well-done clinical trials in NAFLD,. In some other early trials there were occasional DILI cases. Most seem like compound-specific rather than underlying disease. I don't think we have seen any cases of DILI in Piven's or Flynn's trials. You know, early trial with rosiglitazone, there was one case with DILI.,Ben Tetry's (phonetic) study, and I think it was thought to be a prednisolone-related DILI. In a small trial from Australia with high-dose resveratrol, there was an increase in ALT. I don't think we're seeing DILI signals across NASH trials. It has been said before that DILI patients with underlying liver disease may have worse outcomes, first Dr. Zimmerman in his textbook. There are now data to show that it may be the case, from Drug-Induced Liver Injury Network funded by the NIDDK. In a paper that was published in 2015, about 10% of the patients enrolled had underlying liver disease. DILI in patients with underlying liver disease had significantly worse outcomes, about 5.2 % mortality in patients without underlying liver disease, but 16% in patients with pre-existing liver disease. We noted a higher frequency of azithromycin DILI, maybe just a coincidence, or over-represented in patients with underlying liver disease.

Effect of NAFLD onHepatic CYP3A
activity
Vuppalanchi R, et al. Clin Gastro Hepatol 2007; 5: 388-393
Presenter
Presentation Notes
# 6. In earlier data about altered pharmacokinetics with obesity, there is a fair bit of literature in 70s and 80s looking at the drug disposition, but not to the same number of investigations in effect of fatty liver on drug disposition. When Steve Hall was at Indiana University, we showed that with more fat accumulation in the liver there is lower CYP3A activity.

Hepatic CYP2E1 activity in patients with NASH
• Hepatic CYP2E1 activity, as assessed by oral clearance of chlorzoxazone, was significantly higher in patients with NASH, compared to obese controls (41±12 vs. 33±16 L/h, p=0.03)
• Are patients with NAFLD more sensitive to acetaminophen?
Chalasani N, et al. Hepatology 2003; 37:544-550
Presenter
Presentation Notes
# 7. In NAFLD, clearly there is an upregulation of hepatic 2E1, in one of the papers that we published. Jeff Farrell has done nice work in this area, as well. Increased 2E1 could be a bad actor predisposing to at least certain compounds. There is one paper on children with fatty liver, looking at acetaminophen at a standard dose, and I think there was a higher production of NAPQI. Whether that translates into hepatotoxicity I don't think there are any data. Although there is a lot of talk about altered pharmacokinetics as a risk for drug hepatotoxicity, when you carefully look in the literature, very rare well-documented cases. You know, so you can see an increase there you see in higher drug levels when drug dosing is doubled, you know, for example 6-mercaptopurine, you see DILI but not necessarily a convincing relationship between, you know, altered pharmacokinetics, or drug interactions for that matter, and instances of well-documented DILI.

Baseline ALT• Since patients with NAFLD/NASH may have
normal or elevated ALT, strategies to detect and manage DILI in NASH clinical trials should consider both patient’s baseline (in case of elevated ALT) or ULN (in case of normal ALT)
• May need more than one ALT reading during the screening phase to establish a baseline for DILI monitoring
Presenter
Presentation Notes
# 8. Baseline ALT fluctuations occur in NAFLD. You cannot really take upper limit of normal in monitoring for DILI. You may need multiples of baseline. Establishing baseline in NAFLD can be tricky, and agencies now are asking multiple readings during screening phase to establish a baseline. That's sort of becoming standard in NASH trials.

Chalasani N & Regev A. Gastroenterology 2016;151: 1046-1051
Presenter
Presentation Notes
# 9. This is a commentary that Arie and I wrote for Gastro, published maybe six months ago, on how to identify DILI in patients with chronic liver disease in early-phase clinical trials and how to manage them. This was a starting point, and some of you have challenged some of what we said. But I think, generally, there is a consensus in fatty liver or other underlying liver disease. If there is a baseline, it’s high, There is a general acceptance you now look for multiples of baseline rather than upper limit of normal. there isn't a lot of controversy. So here we stratified. For example, if somebody has ALT 5x of upper limit of normal,, then we recommended repeat liver tests in two to five days and just follow for symptoms.. And for those with,ALT,300, whichever comes first, as long as there isn't an increase in bilirubin and there are no symptoms, could continue treatment and just follow the serial liver biochemistries, whereas if the ALT goes above 8x upper limit of normal in those with normal baseline or if it touches 500, even if the bilirubin is normal and if there are no symptoms, we recommended interrupting the study drug, a work-up for competing etiologies, and only restart the investigational drug product if other etiologies identified.

Treatment emergent ALT
Treatment emergent Total Bilirubin
Liver symptoms Action
Normal baseline:
ALT>5x ULN
Elevated baseline:
ALT> 3 x baseline or >300 U/L (whichever occurs first)
Normal
Patients with Gilbert’s syndrome:
No change in baseline TBL
None Repeat ALT, AST, ALP, TBL, in 2-5 days
Follow-up for symptoms.
Normal baseline:
ALT>8x ULN
Elevated baseline:
ALT> 8x baseline or >500 U/L (whichever occurs first)
Normal
Patients with Gilbert’s syndrome:
No change in baseline TBL
None Interrupt study drug.
Initiate close monitoring and workup for competing etiologies.
Study drug can be restarted only if another etiology is identified and liver enzymes return to baseline.
Suggested algorithm for monitoring and management of DILI in Phase 2-3 NASH studies in patients with normal or elevated baseline ALT
Continued next slide
Presenter
Presentation Notes
#10. An area that requires discussion here is whether to un-blind and continue the subject in the trial requires further discussion. It may be that you take the patient off the study and then you realize he was never exposed to an experimental compound. Regardless of what happens to AST or ALT, if the bilirubin doubles or in those with Guillain-Barre, if the direct fraction doubles, I think that indicates more severe liver injury because we have to interrupt and you have to be very cautious about re-challenging subjects. Liver symptoms feature heavily, but very rarely have I seen a case of DILI just from symptoms. When you suspect DILI just based on symptoms, it turns out to be something else, gallbladder disease or mitochondrial toxicity. I would you may see a signal with, INR or prothrombin time. For monitoring and assessment of DILI in patients with decompensated liver disease, it may be hard to come up with a general guidance that applies to all compounds and a very tricky patient population.
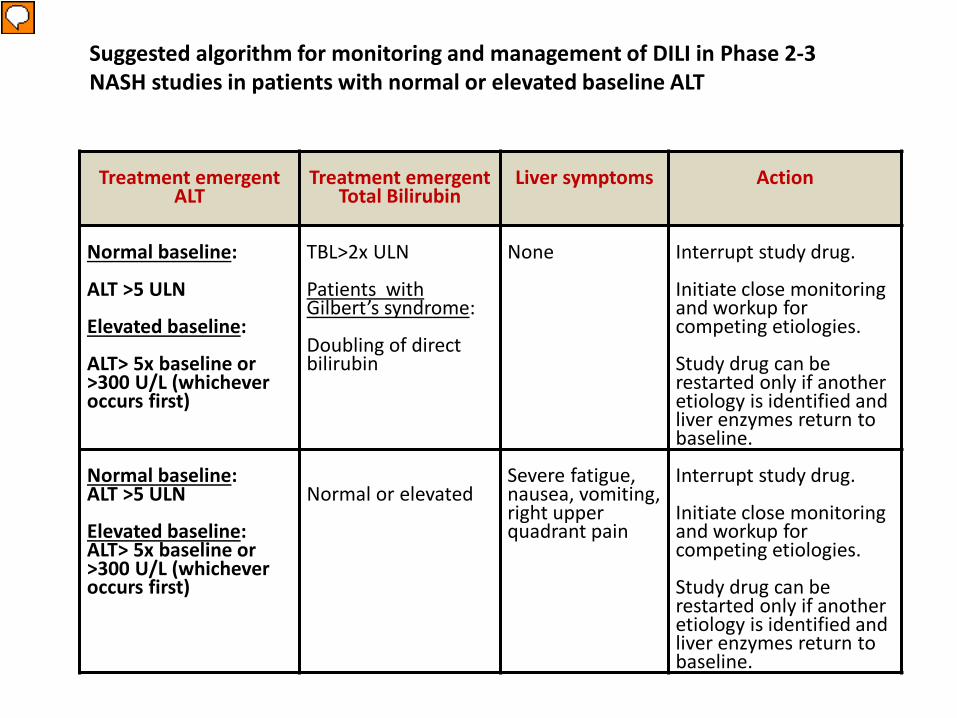
Treatment emergent ALT
Treatment emergent Total Bilirubin
Liver symptoms Action
Normal baseline:
ALT >5 ULN
Elevated baseline:
ALT> 5x baseline or >300 U/L (whichever occurs first)
TBL>2x ULN
Patients with Gilbert’s syndrome:
Doubling of direct bilirubin
None Interrupt study drug.
Initiate close monitoring and workup for competing etiologies.
Study drug can be restarted only if another etiology is identified and liver enzymes return to baseline.
Normal baseline: ALT >5 ULN
Elevated baseline: ALT> 5x baseline or >300 U/L (whichever occurs first)
Normal or elevatedSevere fatigue, nausea, vomiting, right upper quadrant pain
Interrupt study drug.
Initiate close monitoring and workup for competing etiologies.
Study drug can be restarted only if another etiology is identified and liver enzymes return to baseline.
Suggested algorithm for monitoring and management of DILI in Phase 2-3 NASH studies in patients with normal or elevated baseline ALT
Presenter
Presentation Notes
#11. So I'd like to highlight this paper. It was published last year by Dr. Hoofnagle and Dr. Bjornsson who is also in the audience. Really interesting, grading hepatotoxic potential of compounds that are available. I encourage you to look at this paper. Where I'm heading with this is should we be recommending patients with chronic liver disease when they are in clinical trials maybe avoid some hepatotoxic compounds. It seems like aood practice to me.. �I was really surprised to learn there is a study ongoing in France studying Augmentin to treat alcoholic hepatitis. I'm like thinking it's the most common cause of DILI and yet. And ASLD guidelines for treating spontaneous bacterial peritonitis, one of the choices to treat is amoxicillin-clavulanate acid, and I'm like here this is the most common cause of DILI and, yet, that is recommended. So this also is open for discussion. You know, should we be cautious and list these compounds, Dr. Hoofnagles', the top hits from hepatotoxic potential? Should we make a recommendation that these be avoided in clinical trials? There isn't any data, but it just seems sensible to me.











































Monitoring and Assessment of DILI in Patients with Advanced Liver Disease and Decompensated Cirrhosis
• Very close monitoring may be needed in early stage development
• Discontinuation criteria may have to be established for each clinical trial individually
• Unblinding of cases suspected to have DILI may be necessary in selected instances
• Concomitant administration of medications with high hepatotoxic potential may need to be avoided
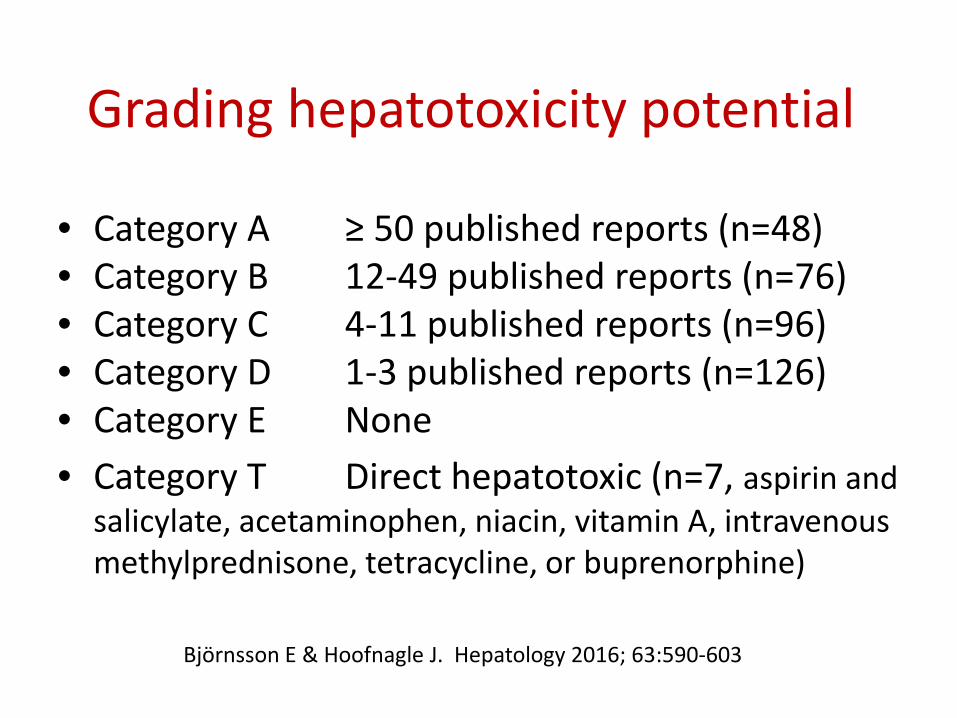
Grading hepatotoxicity potential
• Category A ≥ 50 published reports (n=48)• Category B 12-49 published reports (n=76)• Category C 4-11 published reports (n=96)• Category D 1-3 published reports (n=126)• Category E None• Category T Direct hepatotoxic (n=7, aspirin and
salicylate, acetaminophen, niacin, vitamin A, intravenous methylprednisone, tetracycline, or buprenorphine)
Björnsson E & Hoofnagle J. Hepatology 2016; 63:590-603

Final thought: Should we mandate that certain medications be avoided in patients with CLD participating in
clinical trials?Top 10 therapeutic classes and individual agents to cause DILI in the USA
Therapeutic Class n
1 Antimicrobials 408
2 Herbal and dietary 145
3 CVS agent 88
4 CNS agents 82
5 Anti-neoplastics 49
6 Analgesics 33
7 Immunomodulatory 27
8 Endocrine 20
9 Rheumatologic 13
10 Gastrointestinal 12
Individual agent n
1 Amox-Clavulanate 91
2 INH 48
3 Nitrofurantoin 42
4 TMP/SMX (Bactrim) 31
5 Minocycline 28
6 Cefazolin 20
7 Azithromycin 18
8 Ciprofloxacin 16
9 Levofloxacin 13
10 Diclofenac 12
Chalasani N, et al for the US DILIN. Gastroenterology June 2015