
desmopatia
7
Close this window to return to IVIS www.ivis.org Proceedings of the 54th Annual Convention of the American Association of Equine Practitioners December 6–10, 2008, San Diego, California Program Chair : Harry W. Werner ACKNOWLEDGMENTS Dr. Stephen M. Reed, Educational Programs Committee Chair Carey M. Ross, Scientific Publications Coordinator Published by the American Association of Equine Practitioners www.aaep.org ISSN 0065–7182 © American Association of Equine Practitioners, 2008
-
Upload
tomas-diaz -
Category
Documents
-
view
85 -
download
4
Transcript of desmopatia

Close this window to return to IVIS
www.ivis.org
Proceedings of the 54th Annual Convention of
the American Association of Equine Practitioners
December 6–10, 2008, San Diego, California
Program Chair : Harry W. Werner
ACKNOWLEDGMENTS Dr. Stephen M. Reed, Educational Programs Committee Chair
Carey M. Ross, Scientific Publications Coordinator
Published by the American Association of Equine Practitioners
www.aaep.org
ISSN 0065–7182 © American Association of Equine Practitioners, 2008

Treatment of Suspensory Ligament Desmopathy
Nathaniel A. White II, DVM, MS, Diplomate ACVS; andChristina A. Hewes, DVM, MS, Diplomate ACVS
Suspensory ligament desmopathy is a significant cause of lameness in performance and racehorses.Although injuries to the branches and body can normally be treated successfully with supportive careand rest, injuries at the origin and insertion can become chronic non-healing injuries, which requirestimulation of healing to resolve the lameness. Authors’ addresses: Marion duPont Scott EquineMedical Center, PO Box 1938, Leesburg, VA 20177 (White); and PO Box 620930, Woodside, CA 94062(Hewes); e-mail: [email protected]. © 2008 AAEP.
1. Introduction
Suspensory desmopathy or desmitis has been re-ported to be more common in Thoroughbred race-horses and horses used as hunters, jumpers, or fordressage. Suspensory desmopathy is also observedfrequently in western performance horses.1–4 Thesite of injury in Thoroughbred and Standardbredracehorses is predominantly in the suspensory bodyand branches.5 Recent reports suggest that lesionsat the origin of the suspensory ligament are preva-lent in horses used for performance.6
Suspensory desmopathy causes a mild to moder-ate lameness in the affected limbs. Acute desmitiscan cause localized heat, slight edematous swelling,pain on palpation of the ligament, and rounded bor-ders and enlargement seen on ultrasonograms of thesuspensory ligament. The clinical signs are moreobvious with injuries of the suspensory body andbranches versus injuries at the origin of the liga-ment.7 Front limb lameness caused by proximalsuspensory desmitis is often observed in the outsidelimb when the horse is trotted in a circle on a hardsurface or soft ground. Bilateral lesions are alsocommon and may result in changes in stride rather
than overt lameness. Proximal suspensory injurycan cause mild and intermittent lameness in frontand rear limbs and may be initially missed by riders.Suspensory ligaments affected by chronic desmopa-thy may have no palpable abnormalities.
Local anesthesia in the region of the suspensoryinjury or perineural analgesia of the lateral and me-dial palmar/plantar nerves and/or combined withmetacarpal or metatarsal nerves is used to localizepain from the suspensory ligament.5 In the frontlimb, anesthesia of the middle carpal joint will fre-quently anesthetize the origin of the suspensory liga-ment near the palmar joint pouch.8 In the rear limb,local anesthesia of the lateral plantar nerve seems tobe specific for pain from the proximal suspensory lig-ament.6,9 Definitive diagnosis of suspensory desmitisis made with ultrasonography, which is used to eval-uate the size of the affected ligament and the lengthand area with fibers with abnormal echogenicity.Scintigraphy can be used to identify involvement ofthe proximal third metacarpal/metatarsal bone andthe suspensory attachment, but radiographs areneeded to diagnose avulsion fractures, which are sus-pected on ultrasonograms or scintigraphs.10
502 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
NOTES
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008
Ultrasonographic abnormalities associated withsuspensory ligament injury include enlargement ofthe cross-sectional area, poor demarcation of sus-pensory ligament borders, focal or diffuse areas ofdecreased echogenicity, focal anechoic core lesions,reduced regularity in fiber pattern, and focal miner-alization.11 The degree of the ultrasonographic ab-normality often reflects the severity of thelameness.7 Magnetic resonance imaging has evengreater lesion sensitivity with evidence of size andfiber change, which was not evident on ultrasound insome horses.12
2. Suspensory Ligament Pathology
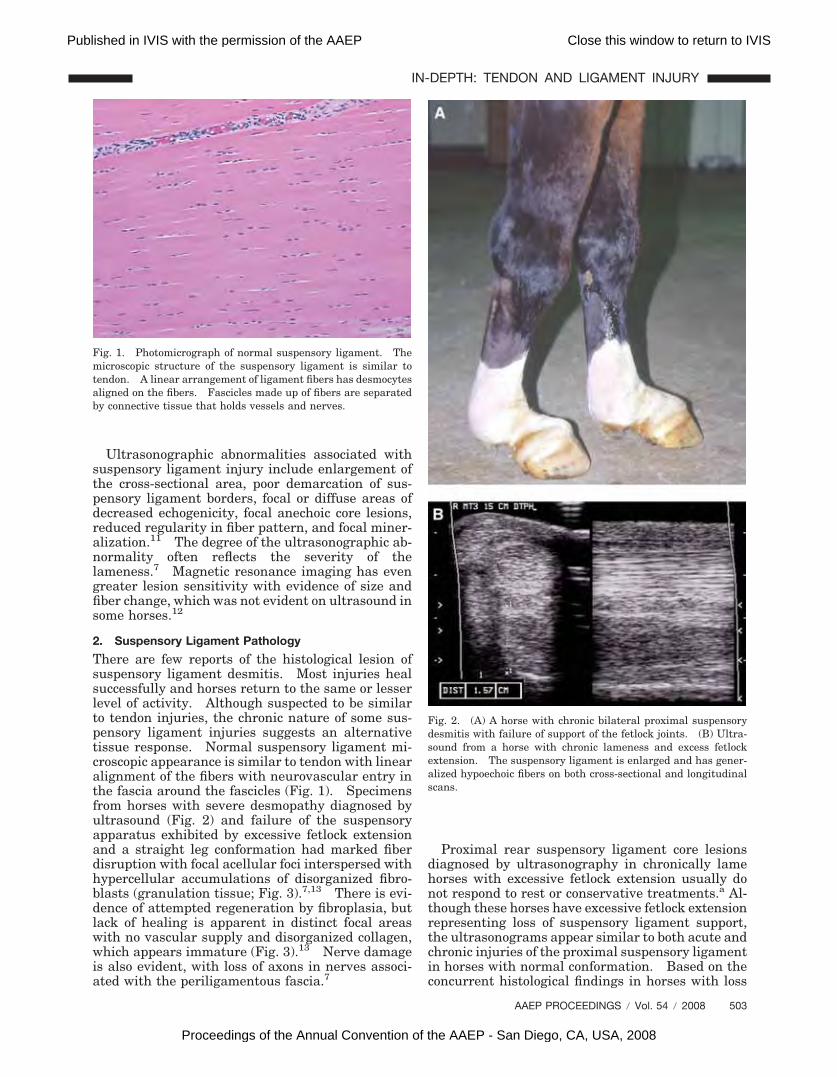
There are few reports of the histological lesion ofsuspensory ligament desmitis. Most injuries healsuccessfully and horses return to the same or lesserlevel of activity. Although suspected to be similarto tendon injuries, the chronic nature of some sus-pensory ligament injuries suggests an alternativetissue response. Normal suspensory ligament mi-croscopic appearance is similar to tendon with linearalignment of the fibers with neurovascular entry inthe fascia around the fascicles (Fig. 1). Specimensfrom horses with severe desmopathy diagnosed byultrasound (Fig. 2) and failure of the suspensoryapparatus exhibited by excessive fetlock extensionand a straight leg conformation had marked fiberdisruption with focal acellular foci interspersed withhypercellular accumulations of disorganized fibro-blasts (granulation tissue; Fig. 3).7,13 There is evi-dence of attempted regeneration by fibroplasia, butlack of healing is apparent in distinct focal areaswith no vascular supply and disorganized collagen,which appears immature (Fig. 3).13 Nerve damageis also evident, with loss of axons in nerves associ-ated with the periligamentous fascia.7
Proximal rear suspensory ligament core lesionsdiagnosed by ultrasonography in chronically lamehorses with excessive fetlock extension usually donot respond to rest or conservative treatments.a Al-though these horses have excessive fetlock extensionrepresenting loss of suspensory ligament support,the ultrasonograms appear similar to both acute andchronic injuries of the proximal suspensory ligamentin horses with normal conformation. Based on theconcurrent histological findings in horses with loss
Fig. 1. Photomicrograph of normal suspensory ligament. Themicroscopic structure of the suspensory ligament is similar totendon. A linear arrangement of ligament fibers has desmocytesaligned on the fibers. Fascicles made up of fibers are separatedby connective tissue that holds vessels and nerves.
Fig. 2. (A) A horse with chronic bilateral proximal suspensorydesmitis with failure of support of the fetlock joints. (B) Ultra-sound from a horse with chronic lameness and excess fetlockextension. The suspensory ligament is enlarged and has gener-alized hypoechoic fibers on both cross-sectional and longitudinalscans.
AAEP PROCEEDINGS � Vol. 54 � 2008 503
IN-DEPTH: TENDON AND LIGAMENT INJURY
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008

of suspensory support evident at its origin, the le-sion is best termed a desmopathy.
Injured ligaments heal by the normal reparativeprocesses including inflammation with removal ofinjured tissue, proliferation and migration of fibro-blasts, which produce collagenous tissue, and liga-ment remodeling.14,15 The collagen fibrils remodelas healing progresses until there is an increase inthe number of cross-links between collagen mole-cules and realignment of the fibrils.14 In horseswith chronic progressive suspensory desmitis withfailure of fetlock support, the reparative process isabnormal, with isolation of collagen bundles fromthe blood supply and death of desmocytes or trans-formation into chondrocytes.13 Cartilage-like tis-sue is produced, resulting in an inelastic ligamentthat is at higher risk for re-injury. Treatment forthe non-healing suspensory injury therefore needsto address chronic inflammation, vascular insuffi-ciency, and ground substance abnormalities.
3. Treatment for Suspensory Ligament Desmopathy
Recommended treatments for acute suspensorydesmitis include rest, support bandages, anti-in-flammatory therapy, and a slow return to controlledexercise. For severe or chronic desmopathy, ancil-lary treatments have been recommended includinglocal and/or systemic administration of glycosamino-glycans,15 administration of systemic corticoste-roids,15 internal blister, injection of bone marrow16
or porcine bladder submucosab17, injection withstem cells, injection with platelet rich plasma,7,18
shock wave of the lesion,21–24 fasciotomy withneurectomy of the deep branch lateral plantarnerve,9,10 and surgical splitting (desmoplasty) ofcore lesions in the injured portion of the ligament.23
The majority of suspensory ligament injuries in-volving the branches or the body will heal with suf-ficient rest.5,7 Similarly, 90% of proximalsuspensory injuries in the front limb respond to restwith rehabilitation, although larger lesions have ahigher rate of re-injury.2,7
Shockwave therapy seems to be beneficial, partic-ularly for lesions at the origin of the suspensoryligament. In two studies, �60% of horses with fore-limb and 40% of hind limb suspensory injuries,which did not heal with rest, returned to full workwithin 6 mo, although a high rate of recurrence wasreported for the rear limb suspensory injuries, andinjuries with a severe grade were less likely to re-solve.20,22 Based on ultrasonographic evaluation,collagenase-induced desmitis healed faster withshockwave treatment.19 Shockwave protocols varywith treatment every 2 wk using 1000–2000 shocksbeing recommended. Weekly treatment by the au-thors has also been used successfully on individualcases.
Injection with a variety of biological devices as astimulus for healing seems to provide improved res-olution of lameness. ACellb is reported to providean �80% success rate for both front and rear sus-pensory injuries.17 Injection of bone marrow aspi-rate or cultured stem cells has been used insuspensory ligaments with an �80% success.16
Hypothetically bone marrow provides both stemcells and growth factors that stimulate ligamenthealing. A commercial company, which offers stemcell extraction and culture, reported a 76% successwith intralesion injection of suspensory injuries.c
Intralesional injection of platelet-rich plasma, whichalso provides growth factors, was reported success-ful in nine of nine horses with severe mid-suspen-sory body lesions with horses returning to racing.18
Bathe6 reported �79% success with horses re-turning to performance using the combination oflateral plantar neurectomy and fasciotomy to treatproximal rear limb suspensory ligaments with corelesions. It is not clear if the fasciotomy or neurec-tomy is the reason for the success, but report ofdesmoplasty (surgical splitting) with fasciotomysuggest that the opening of the fascia is important
Fig. 3. Photomicrographs of the proximal suspensory ligamentfrom a horse with chronic suspensory desmitis (H&E stain) andfailure of fetlock support. Regions of fibroblast proliferation andincreased vascularity (A) are adjacent to areas of metaplasia thatare acellular and avascular with no evidence of healing.
504 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008

for healing and the reason for the success of thesecombined techniques.23
Suspensory desmoplasty (ligament splitting) hasbeen used for several decades and is similar to ten-don splitting. Tendon splitting was first developedin the 1960s and was reported in the 1970s to helpwith local regeneration of injured tendon tis-sue.24–26 One previous report of suspensorybranch splitting describes a percutaneous incisionwith a tendon-splitting knife to produce a fan-likesplit in the ligament to open the ligament in Stan-dardbred trotters. Fifty-nine percent of cases raced�10 races and 29% raced 1–10 races. Most horsesraced 6–7 mo post-operatively. Because only 59%of horses raced �10 races, co-existent involvementof the proximal sesamoid bone was thought to havelimited performance.25
The desmoplasty with fasciotomy completed usingultrasound guidance opens both the core lesion andthe palmar/plantar fascia. The technique is similarto tendon splitting and likely stimulates healing bydecompression, neovascularization, and fibroplasiasin areas lacking collagen replacement.26 The sur-gery is completed with horses under general anes-thesia in lateral recumbency with the affected leguppermost or in dorsal recumbency if bilateral le-sions are present. The procedure is completed us-ing ultrasound to guide a no. 11 scalpel blade or aligament knifed through stab incisions just lateral tothe superficial flexor tendon.8 At the origin of thesuspensory, the blade is advanced through the sus-pensory ligament lesion to the bone surface, whichwas scored with the blade at the suspensory origin(Fig. 4). Stab incisions are spaced at 2-cm divisionsfor decompression of the entire core lesion, whichsimultaneously opens the deep metatarsal fascia.The skin incisions (4–5 mm) are left open. A sim-ilar procedure can be performed on the forelimbproximal suspensory ligaments that do not heal withinitial rest or shockwave treatment.
Recommended post-operative care for ultrasoundguided desmoplasty consists of treatment with phe-nylbutazone (2.2 mg/kg, PO, q 12 h) for 5–7 dayspost-operatively and 30 days of absolute stall restfollowed by 30 days of stall rest with 5–10 min ofhand walking daily. After 60 days, an ultrasoundexamination is completed to make sure the corelesion has increased density from growth of newfibers. If improvement is detected on ultrasono-grams and no lameness is detected, exercise is grad-ually increased (Table 1).23 The increase inexercise is dependent on improved fiber density onultrasound at each subsequent ultrasound examina-tion and stabilization or decrease in the cross-sec-tional area. Turn out is not recommended untilhorses are ridden at the walk, trot, and canter, in-dicating adequate ligament strength.
Ultrasound-guided desmoplasty can also be suc-cessful in stimulating healing in non-healing inju-ries at the insertion of the suspensory branches on
the sesamoid bones and in the straight and obliquedistal sesamoidean ligaments.i
The technique has resulted in resolution of lame-ness with return to work in �85% of horses that hadlong-term follow-up.23 The suspensory ligamentultrasonographic structure does not always returnto normal, with some ligaments retaining hypo-echoic areas or an increased cross-sectional area in
Fig. 4. Cross-section of a cadaver limb with a desmoplasty knife(arrow) guided by ultrasound through the metatarsal fascia andinto the suspensory ligament. The blade is rotated longitudi-nally to open core lesions and the deep fascia. (Reprinted withpermission from Hewes CA, White NA. Outcome of desmoplastyand fasciotomy for desmitis involving the origin of the suspensoryligament in horses: 27 cases (1995–2004). J Am Vet Med Assoc2006;229:407–412.)
Table 1. Typical Protocol for Exercise After Suspensory Ligament Des-moplasty
Weeks 1–4 Absolute stall rest
Weeks 5–8 Walking in hand for 10 min twice daily
Weeks 9–12Walking in hand for 15 min twice daily or
under saddle for 15 min once daily
Weeks 13–16
Walking under saddle for 30 min andtrotting if allowed by healing of thesuspensory ligament
Weeks 17–20Walking and trotting under saddle with
increasing trotting time weekly
Weeks 21–24
Walking, trotting, cantering and possibleturn out dependent on ultrasonogramand absence of lameness
After 24 moGradually increasing exercise progressing
to regular work
AAEP PROCEEDINGS � Vol. 54 � 2008 505
IN-DEPTH: TENDON AND LIGAMENT INJURY
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008

sound horses. Failure seems to be related to thehorse conformation. Horses with excess extension(dorsiflexion) of the fetlock are anecdotally slower toheal or never completely heal. These horses aremore likely to be re-injured or never heal sufficientlyto resolve the lameness.25 This may be related tothe excess suspensory ligament tension likelypresent with this conformation. In two cases, afetlock support shoe allowed for healing of the sus-pensory ligament with resolution of lameness albeitfor light exercise and effective in decreasing thefetlock extension after the support shoe wasremoved.
Horses with forelimb injuries are usually able toreturn to full work 6–12 mo after surgery dependingon the rate of healing. Horses with hind limb prox-imal suspensory injuries can take up to 18 mo beforebeing in full work. In the authors’ experience, sus-pensory ligament injuries that are resistant to heal-ing or that cause continued lameness may respondto repeat shockwave therapy after the surgery.Shockwave treatment is applied after the inflamma-tion from the surgery has decreased (after 60 days),and to date, this has only been used for horses thatstay lame after the surgery.
4. Discussion
New treatments have resulted in improved out-comes for suspensory ligament desmopathy. Allthe invasive techniques likely stimulate healing byphysical stimulation and improved circulation andmobilization of local mesenchymal cells. Monitor-ing the rehabilitation with serial ultrasound exam-ination is just as important as treatment used tostimulate healing. Experience suggests that exer-cise, applied to healing suspensory ligaments wherehealing has become static, can help stimulate newfiber growth or maturity resulting in increased echo-genicity. The improved ultrasonographic characterof the lesion normally corresponded with resolutionof the lameness.
Fasciotomy combined with lateral plantar neurec-tomy for rear limb proximal suspensory desmitisresolved lameness in �80% of horses.6 These re-sults suggest that relief of the compartment pres-sure is a key to the success in healing this type ofinjury. This was also supported by the results ofintralesional injection of porcine bladder submuco-sab (urinary bladder matrix powder) for suspensorydesmitis, in which 36 of 38 of the hind limb suspen-sory ligament desmopathies were also treated with afasciotomy in addition to the porcine bladder sub-mucosab injection.17
The prognosis after desmoplasty is improved com-pared with a rest and rehabilitation program orshockwave therapy and should be considered as analternative or in combination with other treatments.Careful monitoring of healing with a gradually in-creasing exercise program seems to be important inthe rehabilitation program.
References and Footnotes1. Dyson SJ, Arthur RM, Palmer SE, et al. Suspensory liga-
ment desmitis. Vet Clin North Am [Equine Pract] 1995;11:177–215.
2. Cowles R. Proximal suspensory desmitis—a qualitativestudy, in Proceedings. 50th Annual Meeting of the Ameri-can Association of Equine Practitioners. 2002;142–143.
3. Dabareiner RM, Cohen ND, Carter GK, et al. Musculoskel-etal problems associated with lameness and poor perfor-mance among horses used for barrel racing: 118 cases(2000–2003). J Am Vet Med Assoc 2005;227:1646–1650.
4. Kasashima Y, Takahashi T, Smith RK, et al. Prevalence ofsuperficial digital flexor tendonitis and suspensory desmitisin Japanese Thoroughbred flat racehorses in 1999. EquineVet J 2004;36:346–350.
5. Dyson S, Genovese R. The suspensory apparatus. In:Ross MW, Dyson S, eds. Diagnosis and management oflameness in the horse. St. Louis: Saunders, 2003;645–666.
6. Bathe AP. Plantar metatarsal neurectomy and fasciotomyfor the treatment of hindlimb proximal suspensory desmitis,in Proceedings. ACVS Vet Symposium 2007:116–117.
7. Dyson S. Proximal suspensory desmitis in the forelimb andthe hindlimb, in Proceedings. 46th Annual Meeting of theAmerican Association of Equine Practitioners 2000;137–142.
8. Ford TS, Ross MW, Orsini PG. A comparison of methods forproximal palmar metacarpal analgesia in horses. Vet Surg1989;18:146–150.
9. Hughes TK, Eliashar E, Smith RK. In vitro evaluation of asingle injection technique for diagnostic analgesia of the prox-imal suspensory ligament of the equine pelvic limb. VetSurg 2007;36:760–764.
10. Dyson SJ, Weekes JS, Murray RC. Scintigraphic evaluationof the proximal metacarpal and metatarsal regions of horseswith proximal suspensory desmitis. Vet Radiol Ultrasound2007;48:78–85.
11. Dyson S. Proximal suspensory desmitis: clinical, ultra-sonographic and radiographic features. Equine Vet J 1991;23:25–31.
12. Brokken MT, Schneider RK, Sampson SN, et al. Magneticresonance imaging features of proximal metacarpal andmetatarsal injuries in the horse. Vet Radiol Ultrasound2007;48:507–517.
13. Hewes CA. Characterization of apoptotic cells in equineproximal suspensory desmitis. Leesburg, VA: Virginia Tech,Marion DuPont Scott Equine Medical Center, 2006.
14. Frank CB. Ligament injuries: pathophysiology and heal-ing. In: Zackazewski JE, Quillen WS, eds. Athletic inju-ries and rehabilitation. Philadelphia: W. B. Saunders,1996;9–25.
15. Smith KW, Goodship AE. Tendon and ligament physiology.In: Hinchcliff KW, Kaneps AJ, Geor RJ, eds. Equine sportsmedicine and surgery. Philadelphia: Saunders, 2004;130–151.
16. Herthel D. Enhanced suspensory ligament healing in 100horses by stem cell and other bone marrow components, inProceedings. 47th Annual Meeting of the American Associ-ation of Equine Practitioners 2001;319–321.
17. Mitchell R. Treatment of tendon and ligament injuries withUBM powder (ACell-Vet), in Proceedings. ACVS VeterinarySymposium Annual Meeting of the College of VeterinarySurgery 2004;190–193.
18. Waselau M, Sutter WW, Genovese R, et al. Intralesionalinjection of platelet-rich plasma followed by controlled exer-cise for treatment of midbody suspensory ligament desmitisin Standardbred racehorses. J Am Vet Med Assoc 2008;232:1515–1520.
19. McClure SR, VanSickle D, Evans R, et al. The effects ofextracorporeal shock-wave therapy on the ultrasonographicand histologic appearance of collagenase-induced equine fore-limb suspensory ligament desmitis. Ultrasound Med Biol2004;30:461–467.
20. Lischer CJ, Ringer SK, Schnewlin M, et al. Treatment ofchronic proximal suspensory desmitis in horses using focused
506 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008

electrohydraulic shockwave therapy. Schweiz Arch Tierhei-lkd 2006;148:561–568.
21. Caminoto EH, Alves AL, Amorim RL, et al. Ultrastructuraland immunocytochemical evaluation of the effects of extra-corporeal shock wave treatment in the hind limbs of horseswith experimentally induced suspensory ligament desmitis.Am J Vet Res 2005;66:892–896.
22. Crowe OM, Dyson SJ, Wright IM, et al. Treatment ofchronic or recurrent proximal suspensory desmitis using ra-dial pressure wave therapy in the horse. Equine Vet J 2004;36:313–316.
23. Hewes CA, White NA. Outcome of desmoplasty and fas-ciotomy for desmitis involving the origin of the suspensoryligament in horses: 27 cases (1995–2004). J Am Vet MedAssoc 2006;229:407–412.
24. Maxwell JA. Treatment of tendosynovitis in the horse bythe tendon splitting operation. Aust Vet J 1971;47:192–193.
25. Knudsen O. Percutaneous tendon splitting–method and re-sults. Equine Vet J 1976;8:101–103.
26. Stromberg B, Tufvesson G, Nilsson G. Effect of surgicalsplitting on vascular reactions in the superficial flexor tendonof the horse. J Am Vet Med Assoc 1974;164:57–60.
aN. A. White, II, and C. A. Hewes. Unpublished cases. 2008.bACell Vet Urinary Bladder Matrix Powder, ACell, Jessup, MD
20794.cVet Stem, Poway, CA 92064.dSontec, Englewood, CO 80112.
AAEP PROCEEDINGS � Vol. 54 � 2008 507
IN-DEPTH: TENDON AND LIGAMENT INJURY
Published in IVIS with the permission of the AAEP Close this window to return to IVIS
Proceedings of the Annual Convention of the AAEP - San Diego, CA, USA, 2008


















