
DESCENDING TRACTS OF SPINAL CORD - WordPress.com · 2019-03-05 · - Posture, Equilibrium & overall...
36
DESCENDING TRACTS OF SPINAL CORD Dr. Ayisha Qureshi Professor MBBS, M Phil
Transcript of DESCENDING TRACTS OF SPINAL CORD - WordPress.com · 2019-03-05 · - Posture, Equilibrium & overall...

DESCENDING TRACTS OF SPINAL CORD
Dr. Ayisha QureshiProfessor
MBBS, M Phil

GRAY MATTER OF SPINAL CORD
Gray matter of spinal cord is a collection of nerve cell bodies, dendrites and parts of axons. It is placed centrally in the form of wings of butterfly and it resembles the letter ‘H’. Exactly in the
center of gray matter is a canal called the Spinal canal.


ANTERIOR GRAY HORN:contains the nuclei of anterior
motor neurons, involved in motor function.
There are 3 types of anterior motor neurons present: 1. ALPHA MOTOR NEURONS: give rise
to large A-alpha fibers (14 micrometeres) that innervate large skeletal muscle “Motor units”.
2. GAMMA MOTOR NEURONS:transmit through A-gamma fibers (5 micrometers) that innervate small special skeletal muscle fibers called “Intrafusal fibers”.
3. RENSHAW CELLS: are inhibitory neurons that carry out “Lateral Inhibition” at the spinal cord.
4. INTERNEURONS: are present in all areas of the cord gray matter. Small and highly excitable neurons. All types of neuronal circuits (diverging, converging & repetitive discharge) are found in the inter-neuronal pool.

What are Descending Tracts or Motor Tracts?

From the various regions of brain to the skeletal
muscles, the information is relayed
through the DESCENDING TRACTS
These are pathways that carry action potentials from multiple regions of the brain to the Lower Motor Neurons in the brainstem or spinal cord, where
they make an NMJ with the motor end plate.

Why do we mention both spinal cord and brainstem when we mention the
termination of the Lower motor neurons?
Skeletal (striated) muscle contraction is initiated by “lower” motor neurons in the spinal cord and brainstem. The cell bodies of the lower motor
neurons are located in the ventral horn of the spinal cord gray matter and in the motor nuclei of the cranial
nerves in the brainstem.

Descending motor pathways innervate alpha motor neurons, gamma motor neurons, and interneurons. The motor neurons are topographically organized in the anterior horn of the spinal cord according to two rules: the flexor-extensor
rule and the proximal-distal rule
Flexor-extensor rule: motor neurons that innervate flexor muscles are located posteriorly to motor neurons that innervate extensor muscles.
Proximal-distal rule: motor neurons that innervate distal muscles (e.g., hand muscles) are located lateral to motor neurons that innervate proximal muscles (e.g., trunk muscles)
Also, if there are lower motor neurons, there should be Upper motor neurons….

What do you understand by the Upper motor neurons and Lower motor neurons?

Upper vs Lower Motor Neurons
UPPER MOTOR NEURONS • Upper motor neurons (UMNs)
are motor neurons that synapse on the lower motor neurons (either directly or via interneurons).
• These neurons arise from the cerebral cortex and the brainstem.
• They usually form the First Order Neurons of the Descending Tracts.
LOWER MOTOR NEURONS • Lower motor neurons (LMNs)
are motor neurons that directly innervate skeletal muscle.
• The cell bodies of these neurons are located within the anterior (ventral) horns of the spinal cord (spinal nerves) and within brainstem motor nuclei (cranial nerves).


THE FINAL COMMON PATHWAY
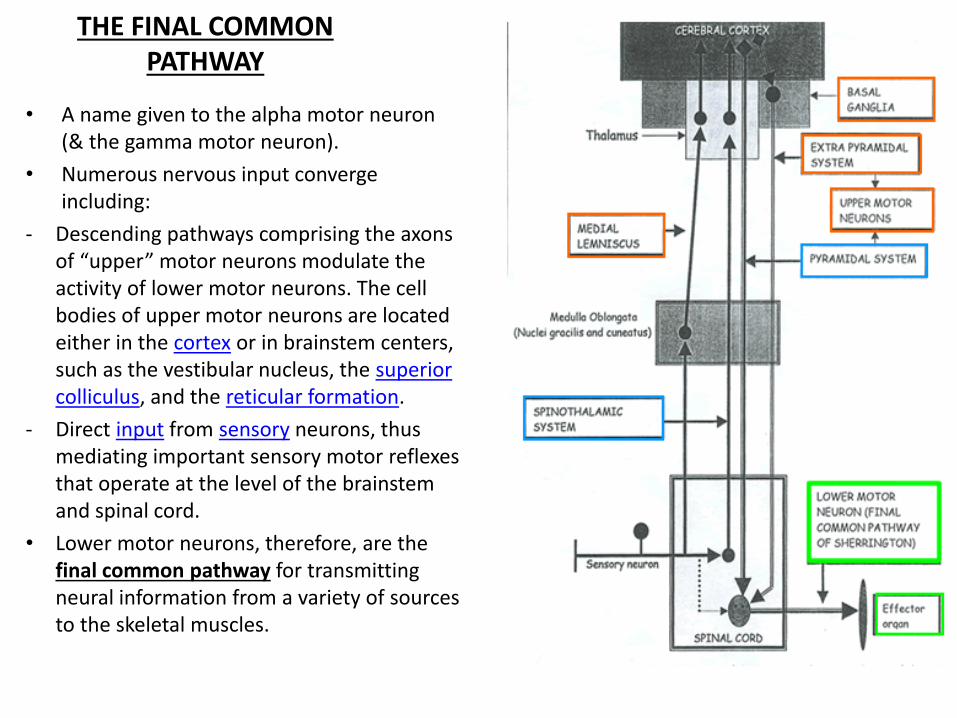
• A name given to the alpha motor neuron (& the gamma motor neuron).
• Numerous nervous input converge including:
- Descending pathways comprising the axons of “upper” motor neurons modulate the activity of lower motor neurons. The cell bodies of upper motor neurons are located either in the cortex or in brainstem centers, such as the vestibular nucleus, the superior colliculus, and the reticular formation.
- Direct input from sensory neurons, thus mediating important sensory motor reflexes that operate at the level of the brainstem and spinal cord.
• Lower motor neurons, therefore, are the final common pathway for transmitting neural information from a variety of sources to the skeletal muscles.

Name the different Descending Tracts?

DESCENDING TRACTS
PYRAMIDAL TRACTS/ DIRECT PATHWAYS
- Muscle Tone - Movements with skill and
precision - Movements of the distal parts
of the limbs
EXTRAPYRAMIDAL TRACTS/ INDIRECT
PATHWAYS
- Posture, Equilibrium & overall body co-ordination.
- Movements of the proximal parts of the limbs and trunk
Divided into:



PYRAMIDAL TRACTS - Also called Direct Pathways.- Aggregations of upper motor neuron fibers that travel from the
cerebral cortex and terminate directly on the Lower motor neurons of either the brainstem (corticobulbar) or spinal cord (corticospinal) and control motor functions of the Face and distal parts of the limbs of the body.
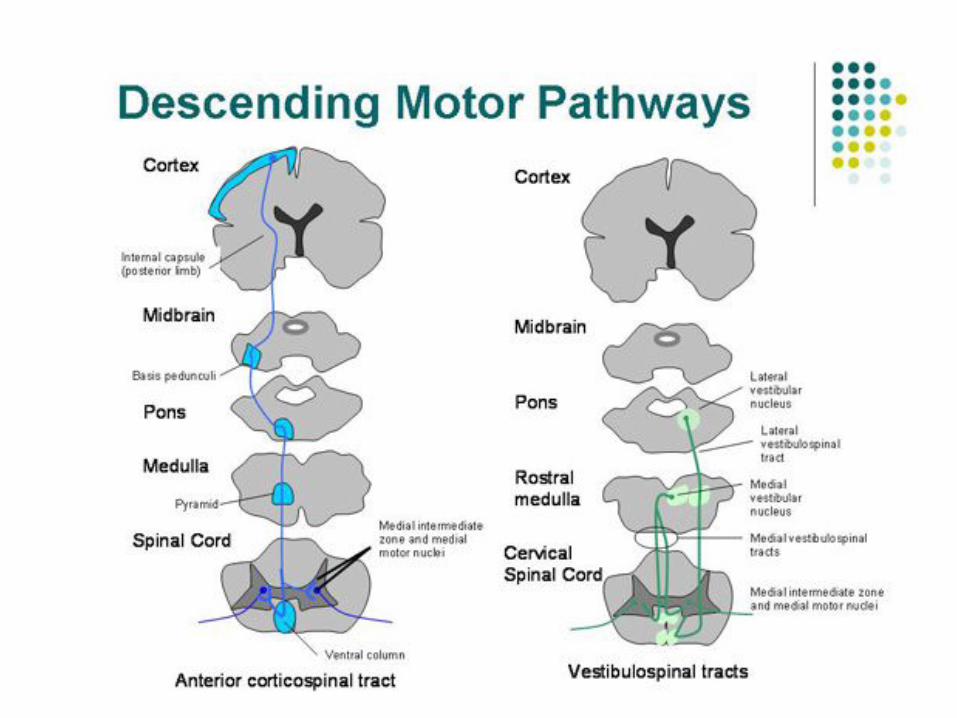
- They include: 1. Corticospinal Tract (Anterior & Lateral): The lateral corticospinal
tract is responsible for the control of the distal musculature and the anterior corticospinal tract is responsible for the control of the
proximal musculature. A particularly important function of the lateral corticospinal tract is the fine control of the digits of the hand.
2. Corticobulbar Tract: Direct cortical control of movements in the head & neck (eye & tongue movements, mastication, facial
expression, & palatine, pharyngeal & laryngeal movements).

The corticospinal system controls motor neurons and interneurons in the spinal cord.
The corticobulbar system controls brainstem nuclei that innervate cranial muscles.

CORTICOSPINAL TRACT
Thalamus, Basal Ganglia &
Cerebellum
Somato sensory Cortex, Frontal,
Visual & Auditory Cortex
Corpus Callosum (input from the opp. Cerebral
Cortex)
MOTOR CORTEX
INCOMING PATHWAYS TO THE
MOTOR CORTEX

30% Primary Motor Cortex + 30% Premotor Cortex & Supplementary Cortex + 40% Somatosensory Cortex↓
Corticospinal Tract ↓
Posterior Limb of the Internal Capsule ↓
Brainstem(From here the Corticobulbar Tract goes to the muscles of the face & the rest of the tract cont.)
↓Pyramids of the Medulla Oblongata (thus, called Pyramidal tracts)
↓80% fibers cross over in the 20% Fibers stay uncrossed PYRAMIDAL DECUSSATION
↓LATERAL CORTICOSPINAL TRACT ANTERIOR CORTICOSPINAL TRACT
(descends in the lateral white column) (descends in the anterior white column)
↓ ↓
Interneurons Interneurons ↓ ↓
Alpha motor neurons of Alpha motor neurons of neck and upper limbs. all levels of the body.
3% fibers from BETZ Cells, Size: 60µm,
Speed: 70 m/sec
97% fibers, Size: 4µm
Both the lateral and anterior corticospinal tracts are crossed pathways; they cross the midline at different
locations, however.




EXTRAPYRAMIDAL PATHWAYS or INDIRECT PATHWAYS
The Indirect pathways originate in the brainstem & they are concerned with the involuntary movements of the body.
They do not pass through the pyramids, therefore, are also called Extrapyramidal Tracts. 1. Rubrospinal Tract
2. Reticulospinal Tract 3. VestibulospinalTract
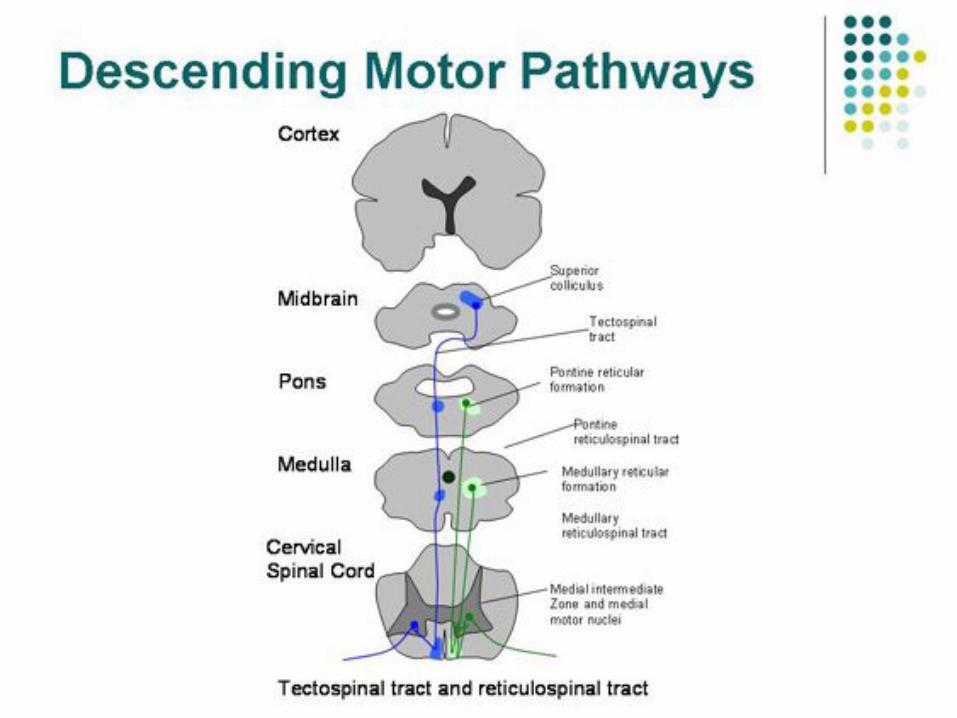
4. Tectospinal Tract
These pathways are also called the Medial Descending Pathways and they innervate the proximal or axial muscles of the body. Thus, this
system is concerned with maintenance of tone, posture and equilibrium (involuntary movements) in the proximal group of muscles.

EXTRAPYRAMIDAL TRACTS
VESTIBULOSPINAL TRACT
- Originates from the Vestibular nuclei.
- Medial and lateral vestibular tracts.
- They are activated during postural
movements, balance and head movements.
RETICULOSPINAL TRACT- Originates from the pontine & medullary reticular formation.
- Regulates posture and muscle tone by
stimulation of the gamma motor neurons.
- Pontine reticulospinaltract is excitatory in
nature & will increase the gamma discharge.
- Medullary reticulospinaltract is inhibitory & will
reduce the gamma discharge.
- If damaged, leads to rigidity as loss of
inhibitory influence.
TECTOSPINAL TRACT- Also called the
Colliculospinal Tract.- Originates in the
superior colliculus of the midbrain.
- Control head & eye movements, in response
to visual & auditory stimuli.
RUBROSPINAL TRACT - Part of the
corticorubrospinal tract. - Fibers arise from the
large meganocellular cells of Red nucleus of the
midbrain. - Synapse on the alpha
motor neurons along with the lateral corticospinal
tract. - Controls movements of
the distal group of muscles, and plays a role in velocity of movements.
- Brings input from cerebellum.

CORTICORUBROSPINALTRACT
• The red nucleus is a structure in the rostral midbrain & is involved in motor coordination.
• Red Nucleus contain large cells called Magnocellular nuclei.
• Has a homunculus. • Accessory route for discrete movements. • They then descend with the Lateral
Corticospinal Tract. • Those fibers that originate in the Red
Nucleus form the Rubrospinal Tract & together with the corticospinal tract are called the Corticorubrospinal Tract.
• The corticospinal and rubrospinal tracts are also called the LATERAL MOTOR SYSTEM of the cord. They control fine motor movements of the distal parts of the limbs. However, the Rubrospinal Tract is an Extrapyramidal Tract.



What is the difference between Upper and Lower Motor Neuron Lesions?
While lower motor neuron lesion is fairly simple, Upper motor neuron lesion means the lesion can occur at any of the 3 locations:
1. Descending tracts 2. Alpha motor neurons
3. Cerebrum
(To understand signs and symptoms of damage to the Upper and Lower motor neurons, it is important to understand that motor
system is not a serial organization but a parallel one!)


UPPER MOTOR NEURON LESION LOWER MOTOR NEURON LESION
1 Muscle groups affected diffusely, NEVER individually.
Individual muscle fibers may be affected.
2 Muscular Atrophy is not seen and if seen, it is very slight.
Marked muscle Atrophy seen due to loss of trophic action of motor nerves. (70-80% wasting).
3 Muscle Tone Increased. Muscle Tone decreased or Absent.
4 Spasticity after an initial flaccidity. Flaccidity.
5Tendon reflexes first lost, later exaggerated.
Tendon reflexes lost.
6 Clonus present. Clonus absent.
7 Babinski’s Positive Babinski’s Absent.
8 Fasciculations not seen. Fasciculations & fibrillations Present.
9 Weakness of muscles/ Paresis. Weakness of the muscle/ Paresis.
10Stroke, Cord section. Poliomyelitis, motor neuron disease,
myasthenia gravis, muscular dystrophy, segmental spinal cord injury.


















