Dermatology Case Epetia Mar, Erestain Noel, Esguerra Peter Hans, Esmael Krista, Eugenio Clarisse...
21
Dermatology Case Epetia Mar, Erestain Noel, Esguerra Peter Hans, Esmael Krista, Eugenio Clarisse Marie, Evangelista Emman, Evangelista Kristy Elleza, Facton Rosabelle
-
Upload
karl-ketchem -
Category
Documents
-
view
218 -
download
0
Transcript of Dermatology Case Epetia Mar, Erestain Noel, Esguerra Peter Hans, Esmael Krista, Eugenio Clarisse...
Dermatology Case
Epetia Mar, Erestain Noel, Esguerra Peter Hans, Esmael Krista, Eugenio Clarisse Marie,
Evangelista Emman, Evangelista Kristy Elleza, Facton Rosabelle

Patient Profile
• 57 year old• Male• Veterinarian
History
• 4 days PTC complained of pain on his left cheek.
• A day after, he noted numerous vesicles on this left cheek affecting the left periorbital area and nasal region.
• He then consulted the emergency room due to the pain & difficulty of opening his left eye.

Salient features
• 57 years old• Male• Veterinarian• Numerous vesicles on left cheek affecting left
periorbital area and nasal region• Pain and difficulty opening his left eye
Differential Diagnosis
• Miliaria Crystalline (Sudamina)• Impetigo Contagiosa• Steven Johnson Syndrome• Herples Simplex• Herpes Zoster
Miliaria• The retention of sweat as a result of occlusion of
eccrine sweat ducts• Produces an eruption that is common in hot, humid
climates(tropics and hot summer months in temperate climates)
• Staphylococcus epidermidis (Mowad et al)– Produces an extracellular polysaccharide that obstructs
the delivery of sweat to the skin surface– occlusion prevents normal secretion from the sweat
glands, and eventually the backed up pressure causes rupture of the sweat glands
Miliaria Crystalline/ Sudamina
• Small, clear, and very superficial vesicles with no inflammatory reaction
• Lesions are asymptomatic, short lived and self limited
• Appears in bedridden patients – in whom fever produces increased perspiration
• Bundled children – clothing prevents dissipation of heat and moisture
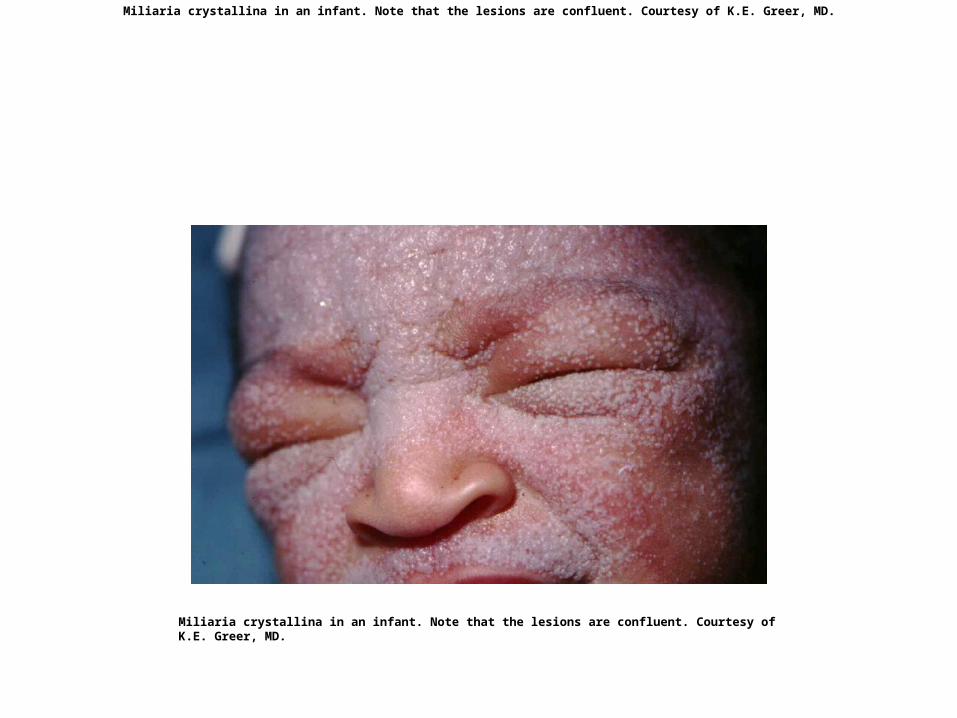
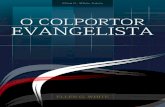
Miliaria crystallina in an infant. Note that the lesions are confluent. Courtesy of K.E. Greer, MD.
Miliaria crystallina in an infant. Note that the lesions are confluent. Courtesy of K.E. Greer, MD.
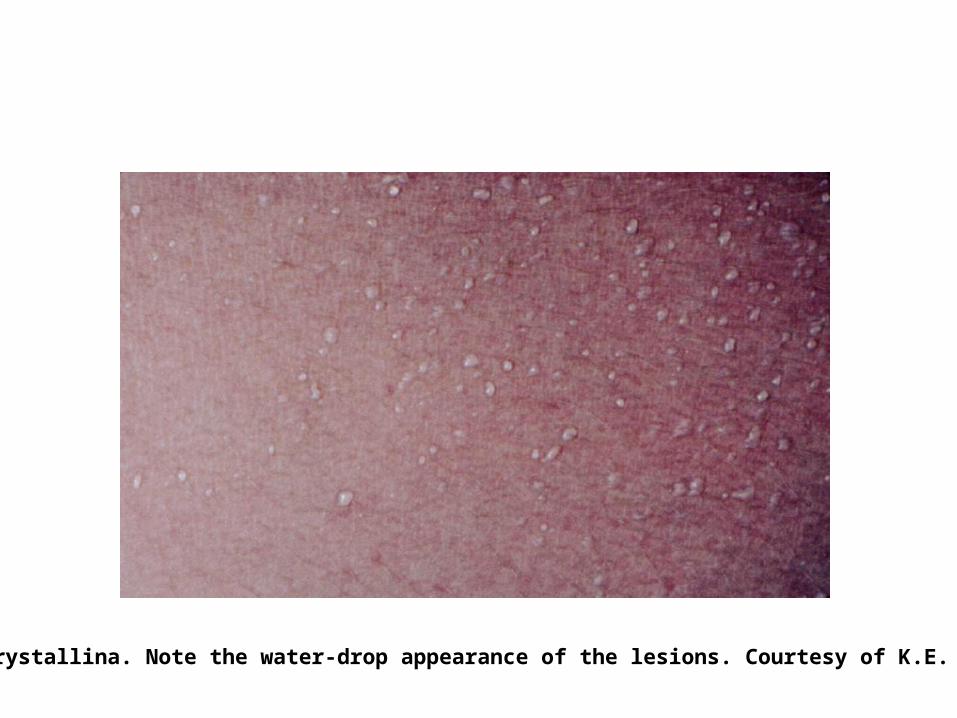
Miliaria crystallina. Note the water-drop appearance of the lesions. Courtesy of K.E. Greer, MD.
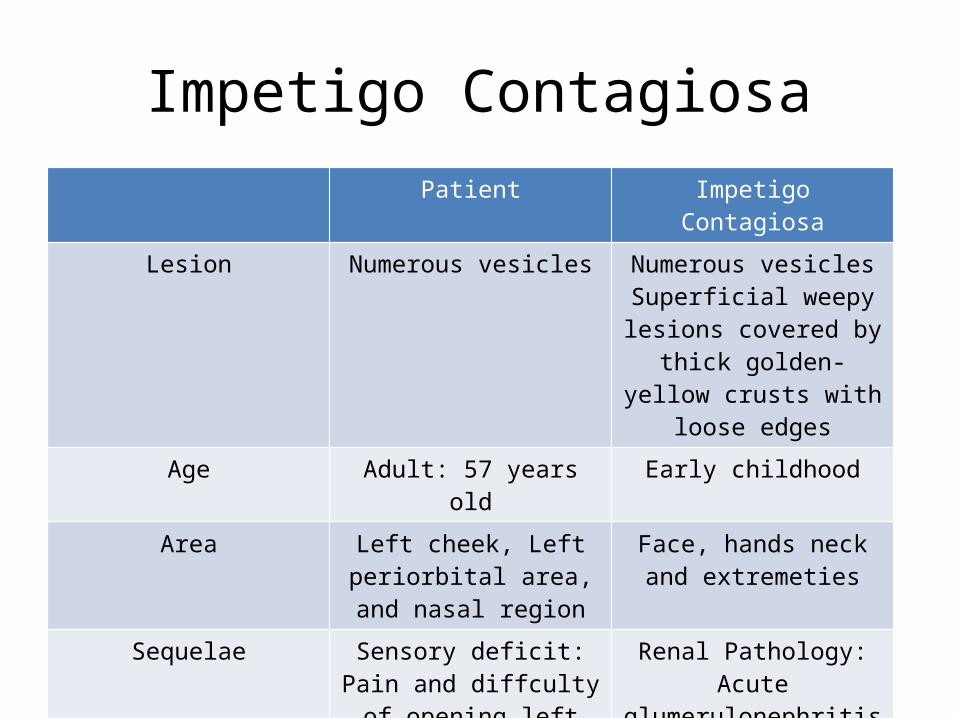
Impetigo ContagiosaPatient Impetigo Contagiosa
Lesion Numerous vesicles Numerous vesiclesSuperficial weepy lesions covered by thick golden-yellow crusts with loose
edgesAge Adult: 57 years old Early childhood
Area Left cheek, Left periorbital area, and nasal region
Face, hands neck and extremeties
Sequelae Sensory deficit: Pain and diffculty of opening left
eye
Renal Pathology: Acute glumerulonephritis
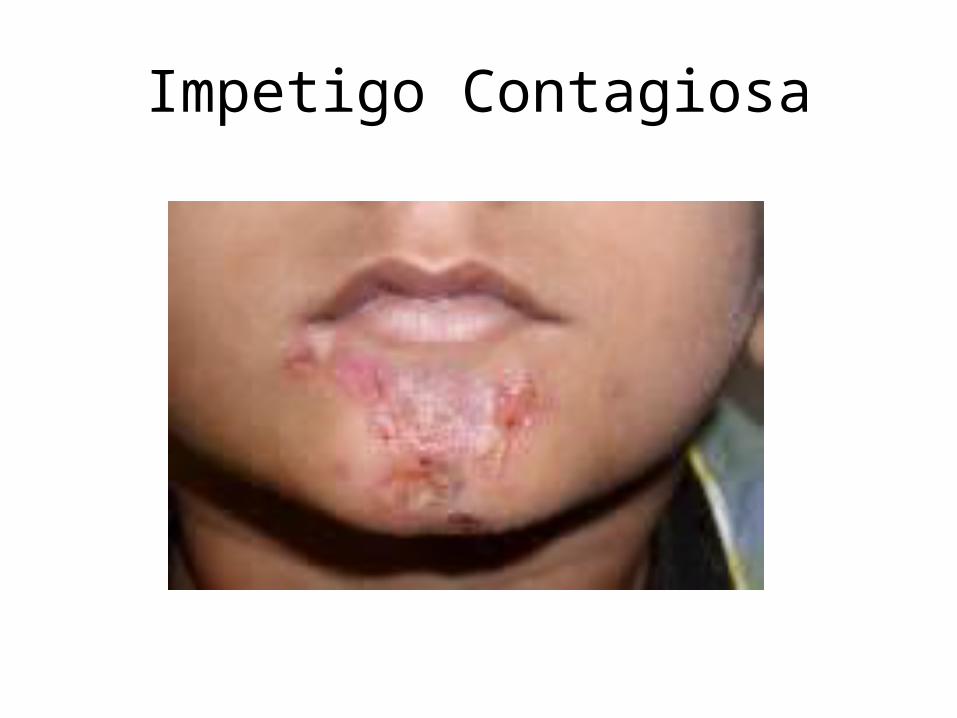
Impetigo Contagiosa
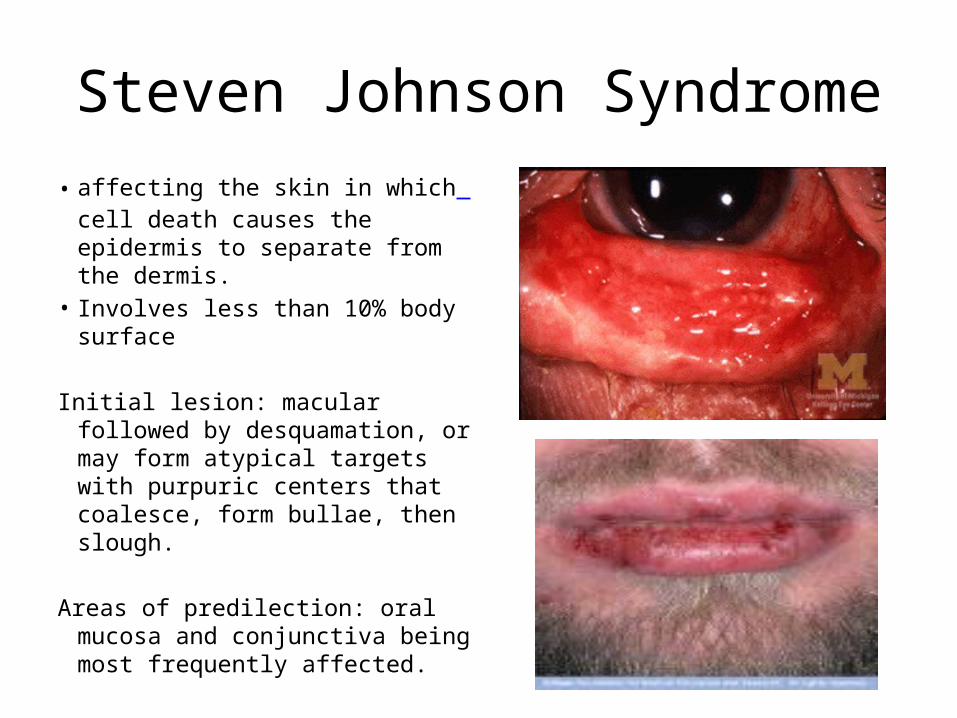
Steven Johnson Syndrome• affecting the skin in which cell
death causes the epidermis to separate from the dermis.
• Involves less than 10% body surface
Initial lesion: macular followed by desquamation, or may form atypical targets with purpuric centers that coalesce, form bullae, then slough.
Areas of predilection: oral mucosa and conjunctiva being most frequently affected.
Steven Johnson SyndromeSigns and Symptoms
• Fever and influenza-like symptoms precede eruption
• Photophobia• Difficulty with swallowing• Cough• Painful on urination• Rectal erosions
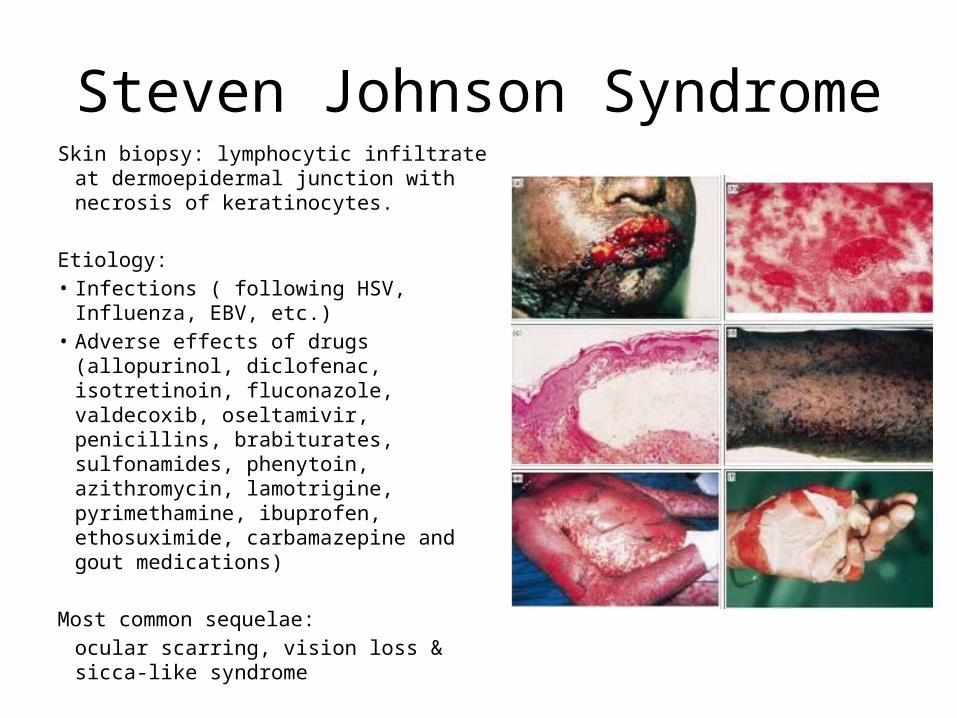
Steven Johnson SyndromeSkin biopsy: lymphocytic infiltrate at
dermoepidermal junction with necrosis of keratinocytes.
Etiology:• Infections ( following HSV, Influenza, EBV,
etc.)• Adverse effects of drugs (allopurinol,
diclofenac, isotretinoin, fluconazole, valdecoxib, oseltamivir, penicillins, brabiturates, sulfonamides, phenytoin, azithromycin, lamotrigine, pyrimethamine, ibuprofen, ethosuximide, carbamazepine and gout medications)
Most common sequelae: ocular scarring, vision loss & sicca-like syndrome

Differential DiagnosesHerpes Simplex
• Lesion– Vesicles are
intraepidermal– Dermis and epidermis
containing infiltrates of leukocytes and serous exudates
• Area of Predilection– Oral herpes: Face and
mouth (cold sores)
Herpes SimplexSigns and Symptoms
• Common infection of the skin or mucosa may affect the face and mouth (orofacial herpes), genitalia (genital herpes), or hands (herpes whitlow).
• More serious disorders occur when the virus infects and damages the eye (herpes keratitis), or invades the central nervous system, damaging the brain (herpes encephalitis).
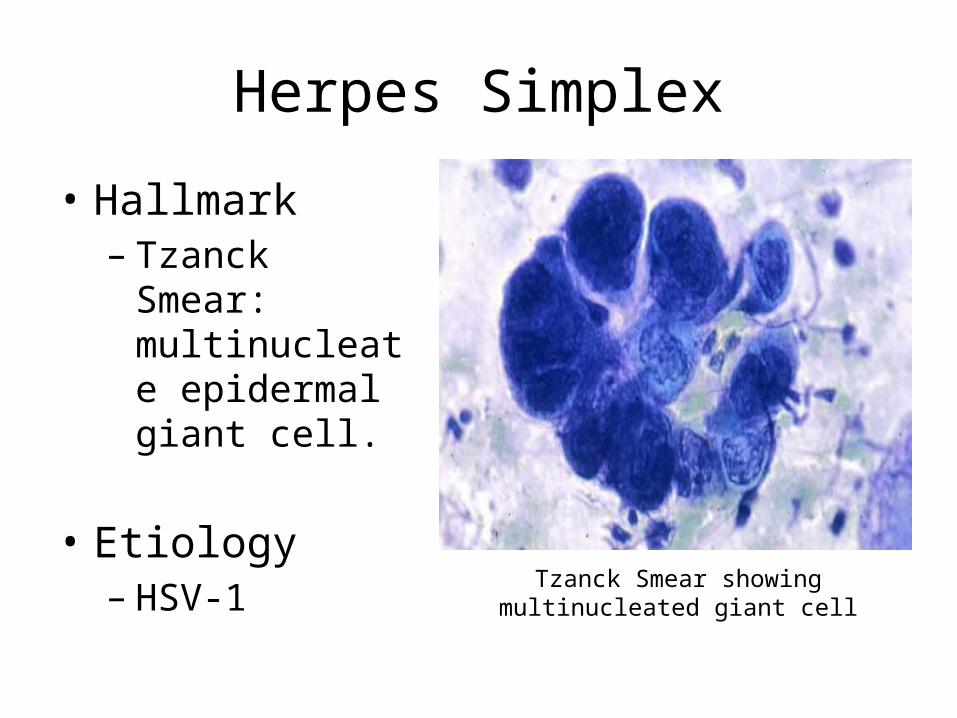
Herpes Simplex
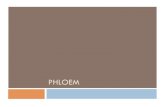
• Hallmark– Tzanck Smear:
multinucleate epidermal giant cell.
• Etiology– HSV-1
Tzanck Smear showing multinucleated giant cell
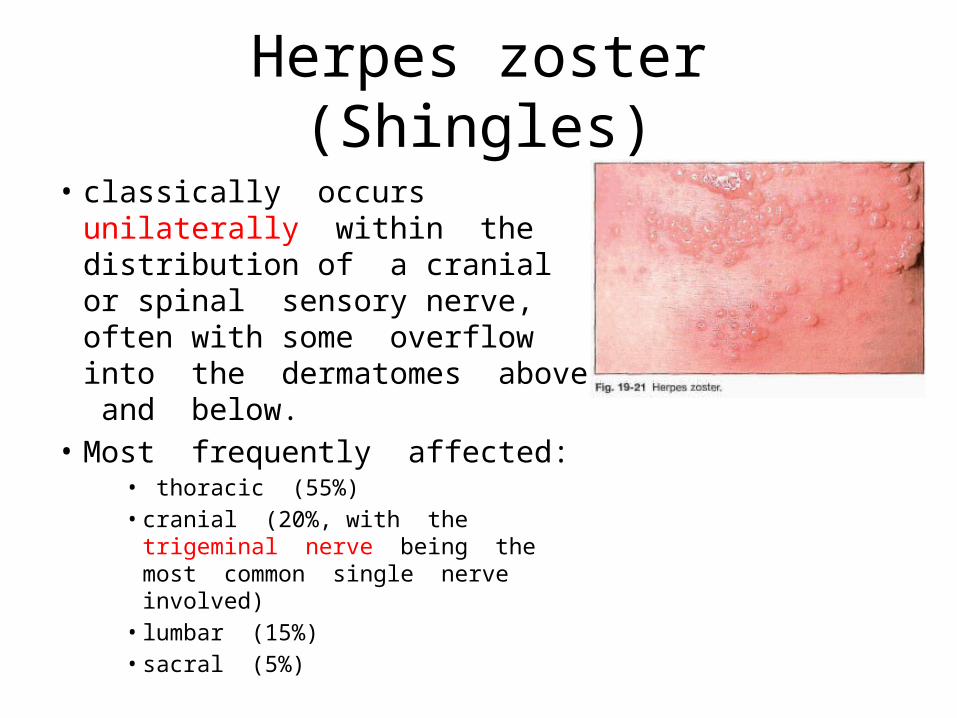
Herpes zoster (Shingles)
• classically occurs unilaterally within the distribution of a cranial or spinal sensory nerve, often with some overflow into the dermatomes above and below.
• Most frequently affected:• thoracic (55%) • cranial (20%, with the trigeminal
nerve being the most common single nerve involved)
• lumbar (15%)• sacral (5%)
Herpes zoster (Shingles)
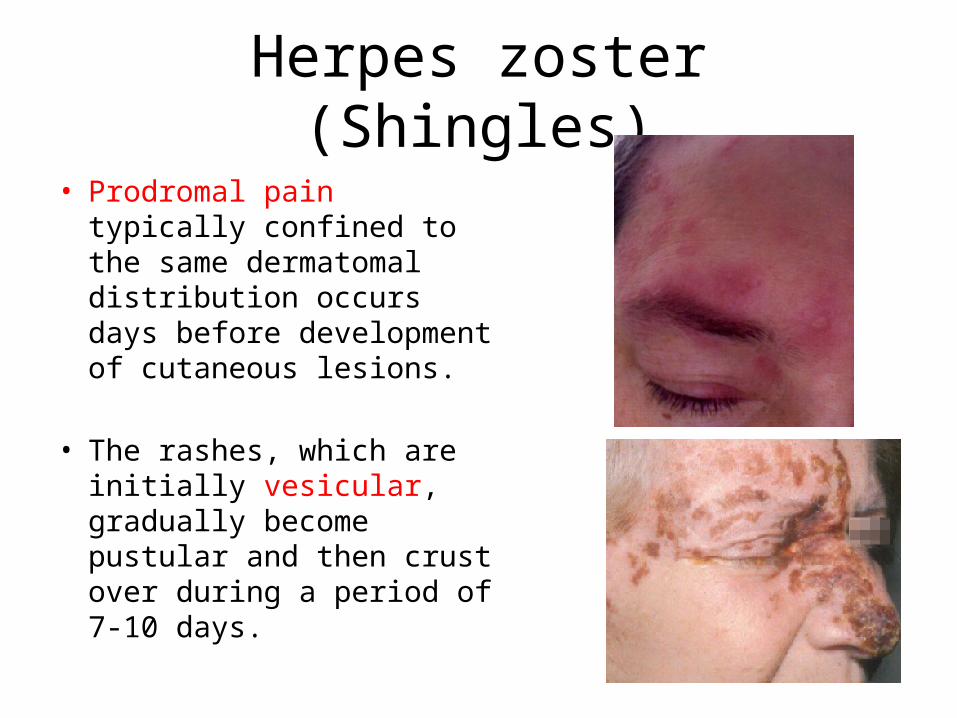
• Prodromal pain typically confined to the same dermatomal distribution occurs days before development of cutaneous lesions.
• The rashes, which are initially vesicular, gradually become pustular and then crust over during a period of 7-10 days.

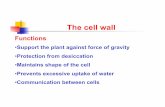
Herpes zoster ophthalmicus
• The ophthalmic division of the CN V is
involved.
• If the external division of the nasociliary branch is affected, with vesicles on the side and tip of the nose (Hutchinson's sign), and the eye is involved 76% of the time.
• Etiology: Varicella-zoster virus (reactivation)