Dermatology board review
215
Dermatology Board Review Dr Usama Al Haddabi 2015
-
Upload
ahmed-amer -
Category
Health & Medicine
-
view
899 -
download
4
Transcript of Dermatology board review

Dermatology Board Review
Dr Usama Al Haddabi
2015


Dermatomyositits

.Juvenille DM vs adult DM – list 5 clinical differences
Juvenile Adult
Calcinosis cutis No calcinosis
No malignancy Malignancy (ovarian)
No sex predominance F:M = 2-7:1
10% overlap with other CTD 20% overlap with other CTD
More vasculitis Less vasculitis
what is in adults but not children ?
malignancy (12% vs 0%)
serology in adults not in children ?
anti-synthetase ab (Jo-1)

List myositits specific antibodies and their significant ?


What are the cutaneouse & systemic findings in DM ?


Two medications can induce DM
Statin – type lipid lowering agents.
Hydroxyurea
Two important clinical features differ lesion of DM from LE
Violaceouse hue
Pruritus

List 4 Indications for systemic treatment of hemangiomas
obscure visual axiscompromise airwayulceration & paincosmetically sensitive area like tip of nose or lipulceration and infection

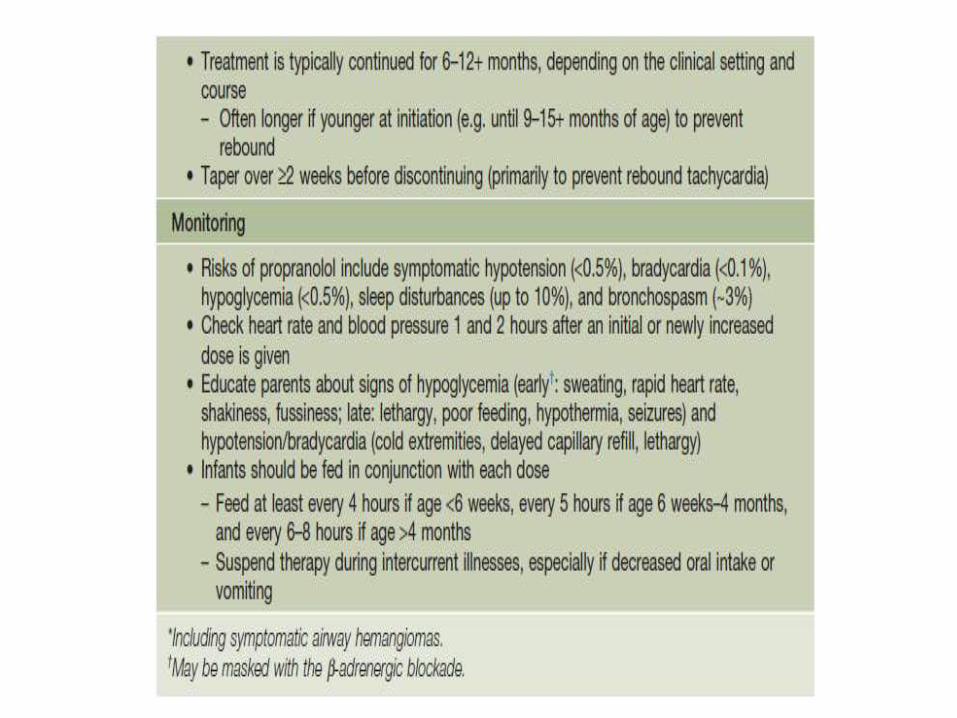
Your approach for starting propranolol for IH

3 clinical differences between Linear IgA disease and drug-induced LAD.
Duration : drug induced is limited, idiopathic is prolonged
Refractory nature: drug induced no, idiopathic yes
Age group: drug induced –adults>kids , idiopathic –kids>adults

Mechanism of action of ACE-induced angioedema
ACE inhibitors lead to an increased level of bradykinin. Bradykinin causes vasodilation increased vascular permeability and hypotension
emedicine: ACEI block action of enzyme kinase II which converts ang I to ang II. Ang ii is a potent vasoconstrictor and inactivates bradykinin.Acei block conv of ang 1 to II, which increases bradykinin levels

Protein C deficiencyProtein S deficiency Obesity Female sex (4x that of men)incorrect or too rapid anticoagulation dosinginstitution of warfarin without concurrent heparininstitution of warfarin with loading doses
Warfarin necrosis – 3 risk factors for this
List the different phases of cell cycle – describe what happens at each stage
Gap1- major period of growth of the cell, protein production
S- Synthesis: DNA duplication in preparation for mitosis
Gap2 – preparation for mitosis, shortest part of cell cycle, checkpoint before mitosis to ensure no errors in replication of DNA during S phase
M - Mitosis
G0 – resting phase, can be entered from either G1 or G2. no replication of DNA

SCORTEN for TEN – list criteria
MABIGUTMalignancy
Age
Bicarbonate
Initial surface detachment
Glucose
Urea
Tachycardia

BCC histologic subtypes: which one looks like a scar clinically, which one likely has positive
margins on local excision.
SuperficialNodularMicronodularInfiltrative- + marginMorpheaform – looks like a scar, + marginBasosquamous – behaves more like an sccLess common subtypes- fibroepithelioma of pinkus

MTX- 4 drugs with interactions of MTX
:-Displace MTX from plasma proteinsTetracyclinessalicylates (also decrease renal excretion)NSAIDs (also decreases renal excretion)Sulfonamide (also decreases renal excretion)PhenytoinChloramphenicolPhenothiazines
-Increased intracellular accumulation:dipyridamoleprobenecid (also decreases renal function)
-Concurrent inhibition of Folic Acid metabolic :pathway
Dapsone (inhibits DHS)Trimethoprim (inhibits DHFR) Sulfonamides (inhibits DHS)
-Synergistic Hepatic toxicity:retinoids, alcohol


MTX …….Absolute and relative contraindications
2 FDA approved dermatology indications of MTX

4 indications of MTX in psoriasis

IP- list four stageswhat is defect what gene is mutated what other organs involved (2 others)
Vesicular, Verrucous, Pigemented, Hypopigmented
Defect is in the gamma subunit of the Inhibitor Kappa Kinase
Gene = NEMO
X-linked dominant
Ophthalmologic – starbismus, cataracts blindness
Dental – anodontia, conical teeth
Neurologic – MR, seizures, spastic paralysis

Imiquimod
FDA approved use/ dose
Dose FDA use
3 times/week maximum 16 weeksExternal genital and perianal warts
5 times/week for 6 weeksSuperficial small (<2 cm) non-facial BCC
2 times/week for 16 weeksActinic keratoses
TLR ? 7New reported side effect of aldara
Eruptive epidermoid cysts

What are Histopathological differences between Ps and PRP
PRPPsfeature
alternating vert and horiz PK
confluent pkparakeratosis
-+intracorneal pustules –Munroes
-+intraspinous pustule –Kojog
-+suprapapillary thinning
-+psoriasiform hyperplasia
-+incr vascularity

Clinical subtypes of Ps
Clinical Subtypes-plaque type psoriasis vulgaris-guttate psoriasis-inverse psoriasis-erythrodermic psoriasis-nail psoriasis-pustular psoriasis impetigo herpetiformisannulargeneralized (von zumbusch)-palmoplantar pustulosis and acrodermatitiscontinua-drug-induced psoriasis

what kind of allergic/adverse reactions can happen with tattoos
-granulomatous reaction-lichenoid-eczematous-photoallergic – inflamed nodules in red or yellow tattoo (cadmium)-migration to local node simulating metastatic melanoma on SNBx-keloid-Koebner phenomenon: psoriasis, lichen planus-Inoculation of disease: HIV, HCV, mTB, esp
prison tattoos
2 nutrients that cause skin discoloration in healthy people
1 nutrient that causes skin discoloration in someone w genetic predisposition
carotenemia (yellow skin discoloration: elevated serum carotenoids, plant pigments-carotene, dietary precursor of Vit A: deeper green or yellow colored vegetables and fruits, red palm cooking oil)
lycopenemia (orange-yellow skin discoloration: lycopene-an inert isomer of -carotene, found chiefly in tomatoes, beets, and rose hips)
bronze diabetes, hemachromatosis, iron overload

3 nutrients that can cause periorificial dermatitis if deficient
2 nutrients that can cause purpura if deficient
biotin deficiency
essential fatty acid deficiency
zinc deficiency
Vit CVit K
What are 3 diseases/syndromes associated with HTLV-1
1.Adult T-cell lymphoma/leukemia (etiological role firmly established), conclusive evidence for a primary etiologic role lacking in MF
2.Chronic progressive myelopathy: tropical spastic paraparesis
3.Infective dermatitis: chronic relapsing eczema + infection[pruritus most common cutaneous symptom, xerosis, acquired icthyosis]

4 clinical types of pustular psoriasis
Explain Auspitz sign
1) generalized pustular psoriasis (von Zumbusch) exanthematous febrile eruption of pustules
2) annular pattern GPP
3) exanthematic type GPP
4) localized patter PP
pustulosis palms and soles
acrodermatitis continua of Hallopeau-pustules
Pinpoint bleeding when psoriatic scale is forcibly removed; occurs because of the severe thinning of the epidermis over the tips of the dermal papillae

3 systemic disease associated with psoriasis
5 drugs that exacerbate psoriasis
Cardiovascular disease (MI, PE, CVA)Crohn’s disease (+ psoriasis + AnkSpond = HLA-B27)
Diabetes Liver-fatty infiltration, periportal inflammation & focal necrosis
5 clinical features of Reiter’s
Arthritis/seronegative spondyloarthropathy
Conjunctivitis
urethritis/cervicitis
buccal ulcers/stomatitis
circinate balanitis
keratoderma blenhorragica (acral pustules)
Also: fever, weakness, keratitis, optic neuritis
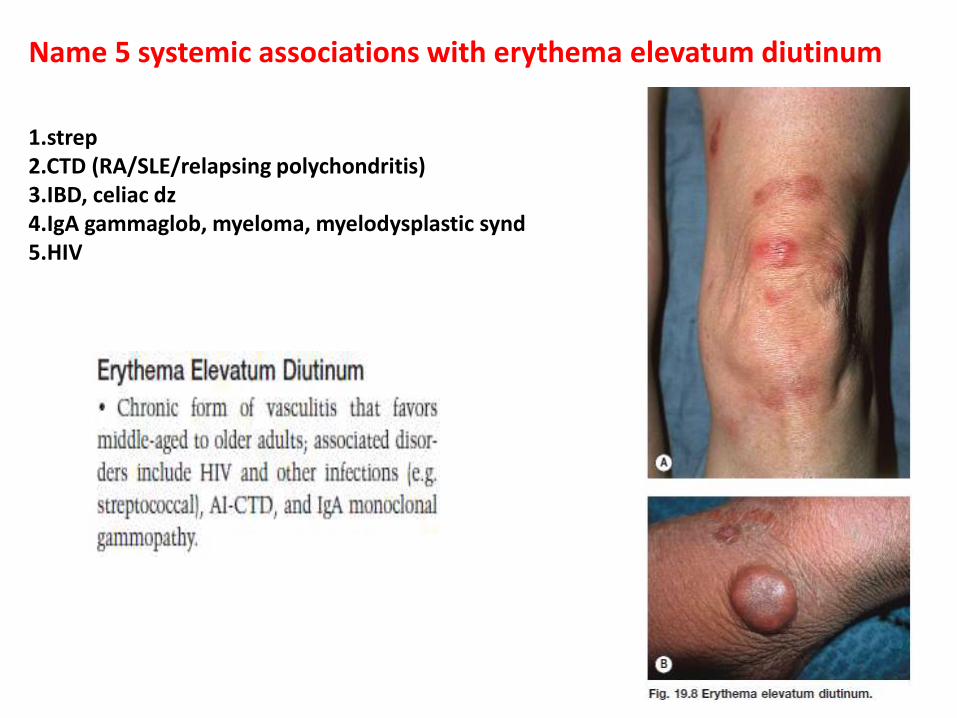
Name 5 systemic associations with erythema elevatum diutinum
1.strep2.CTD (RA/SLE/relapsing polychondritis)3.IBD, celiac dz4.IgA gammaglob, myeloma, myelodysplastic synd5.HIV

Name 3 possible infectious causes of Kawasaki’s disease
1) bacteria (rickettsiae, staphylococci, streptococci)Staph [TSS-toxin-producing staphylococcus, superantigens produced by pathogenic S. aureus] Strep [pyrogenic exotoxin B & C] (toxin secreting bacteria)
2) viruses (EBV, parvovirus, retrovirus)
3) fungi (Candida albicans).

Name an infection thought to predispose an infant to acute hemorrhagic edema
URTIs (adeno, staph, strep)

Name 5 clinical presentations of gold dermatitis

List 5 clinical features that would suggest an allergy to bacitracin
1.Localized to wound area
2.Nonhealing wound
3.Morphology of ACD
4.Anaphylaxis
5.Contact urticaria
List 2 medical diseases where allergy to bacitracin is most common.
1.Venous ulcer
2.Eczema/Atopic dermatitis

What are 3 causes of (lingua villosa nigra)
What anatomic structure on the tongue is responsible
excessive smoking, poor oral hygiene, use of oxidizing mouthwashes, hot beverages
use of oral antibiotics, presence of Candida on surface of tongue
Benign hyperplasia of the filiform papillae of the anterior 2/3 of the tongue resulting in long conical filaments of orthokeratotic and parakeratotic cells

Which tetracycline is safest in renal failure?
Doxycycline (renal failure prolongs the half life of most tetracyclines except doxycycline; doxycycline excreted primarily by the GI tract)

What is the most common anatomic site for white sponge nevus?
What is the inheritance pattern?
What are 2 ways to distinguish white sponge nevus from the leukokeratosis of pachyonychia congenita?
WSN Pachyonychia Congenita1. No extramucosal lesions2. Mostly on buccal mucosa
Progression stops at puberty
Sites: mouth, vagina, rectumHisto: acanthosis, vacuolated prickle layerEM: clumped tonofilaments
1. Multiple assoc findings2. Leukokeratosis of tongue, +/- oral
mucosa, +/- laryngeal involv’twith hoarseness

Diseases associated with cobblestone appearance
Dariers disease
Cowden syndrome
Lipoid protenosis
Crohns disease

Name a skin finding associated with hyperparathyroidism
Calciphylaxis-
metastatic calcinosis
MEN Type 1 – tumours parathyroid, pancreas, pituitary; hypercalcemia. (skin findings: multiple angiofibromas, collagenomas, CALMs, lipomas)
pseudogout – calcium pyrophosphate (CPP) crystals
Describe 5 patterns of parakeratosis and list a disease for each pattern.
1) confluent parakeratosis permeated by neutrophils (Munro’s microabscesses) – psoriasis.
2) alternating para with ortho both vertical & horizontal ‘checkerboard’– pityriasis rubra pilaris
3) (tiers) slanted columns of parakeratosis/stacked porokeratosis – cornoid lamella of porokeratosis/wart
4) shoulder parakeratosis (predilection for the follicular ostia-‘follicular lipping’) – seborrheic dermatitis
5) mound-like (lenticular) parakeratosis ‘staccato parakeratosis’ & ‘skipping scale’ – pityriasis rosea




What is the maximum safe duration of time to have a tourniquet in place?
Max 15 minutes. After that, increased risk of nerve damage.
What is the maximum safe dose of lidocaine with epinephrine?
4.5 mg/kg without EPI, 7 mg/kg WITH EPI
List 3 advantages of using lidocaine with epinephrine.
1.Decreased absorption of lidocaine2.Prolonged anesthesia3.Reduced risk of systemic toxicity4.Reduced bleeding at operative site

Which layer of the skin does HPV infect?
Epidermis
List 2 genes responsible for carcinogenicity .
1. E6 – degrades p53 which normally puts brakes on cell cycling in st. malphigii
2. E7 – binds retinoblastoma (tsg) to liberate E2F from Rbinhibition. This allows synthesis of genes required for DNA replication
List 2 HPV types that cause Heck’s disease
HPV 13, 32

List 7 infectious causes of oral ulcers in the immunocompetent host
1. HSV 1&22. Rare EBV??3. Erosive candida4. primary VZV5. HPV induced SCC6. Hand-foot-mouth – Coxsackie A16 (uvula, tonsillar pillars)7. Herpangina – coxsackie A & B, echoviruses (soft palate)8. HCV-induced erosive lichen planus9. Syphilitic chancre10. Chancroid (H.ducryei)11. TB (TB cutis orificialis)12.Rarely histoplasmosis or cryptococcus (but usually in immunocompromised)

What is a medical way to reverse eyelid ptosis from Botox?
Lid ptosis results from migration of the BTX to the levator palpebraesuperioris muscle.
•It usually lasts 2-6 weeks.
Medical mgmt is with apraclonidine (Iopidine, Alcon), an alpha-
adrenergic agent that stimulates the Meüller muscle and immediately elevates the upper eyelid (use 1-2 drops TID until ptosis resolves). This txusually can raise the eyelid 1-3 mm.
ALTERNATIVE: phenylephrine hydrochloride 2.5% (Neosynephrine) drops

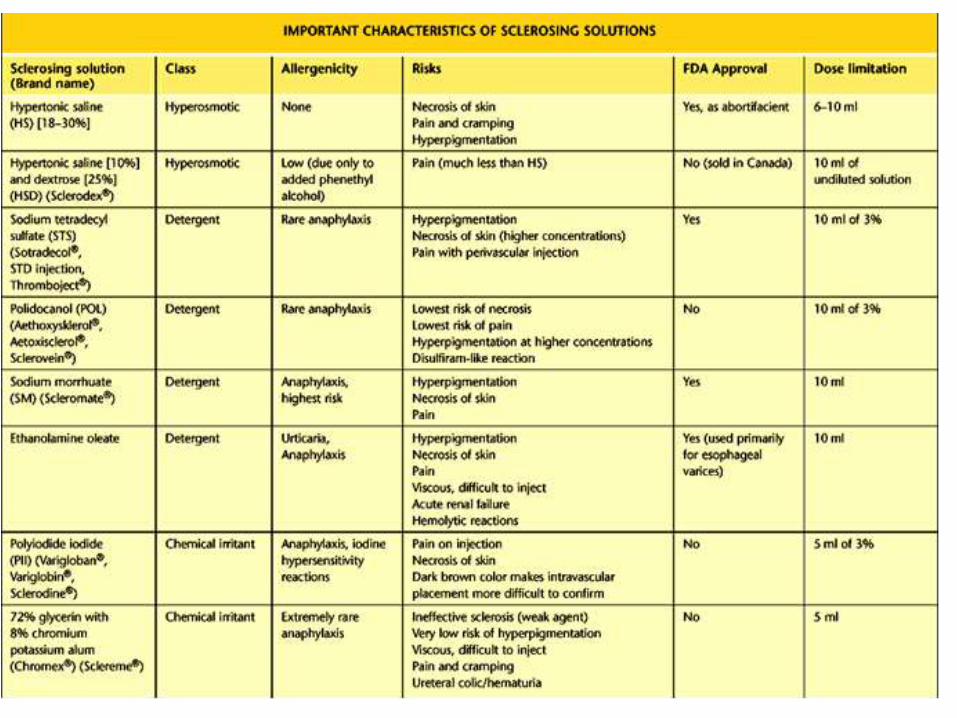
Name 3 broad groupings of agents used in sclerotherapy and give an example of each
Hypertonic- NaCl, NaCl + dextrose
(Sclerodex)
Detergent- sodium tetradecyl sulfate,
polidocanol
Chemical irritant- polyiodide iodide
Eight cutaneous forms of LP.
1. Annular2. Linear3. Generalized4. Actinic5-pemphigoides
6. Atrophic7. Bullous7. Ulcerative (on feet)8. Hypertrophic9. Follicular10. Mucosal11. Lichen planopilaris12. Nail LP13- Drug induced LP14-LP-LE OVERLAP


Four ways to histologically tell apart drug-induced LP from regular LP
1. Focal parakeratosis (vs. compact hyperkeratosis in LP)
2. Colloid bodies higher up, in spinous and granular layers (vs. lower epidermis in LP)
3. Prescence of eosinophils or plasma cells in infiltrate (vs. lymphocytic in LP)
4. Superficial and deep perivascular infiltrate (vs. lichenoid and superficial in LP)

List 5 features of lichen planus seen on pathology.1.Saw tooth acanthosis2.Wedge-shaped hypergranulosis3.Max-Joseph space4.Hyperkeratosis5.lichenoid lymphocytic infiltrate with pigment incontinence6.colloid bodies (dermal)/Civatte bodies (epidermal)

List 4 diseases mediated by staphylococcal exfoliative toxin

List 7 skin infections caused by localized streptococcal infection.
Ecthyma
cellulitis
Erysipelas
necrotizing fasciitis
blistering distal dactylitis
perianal dermatitis
impetigo

List 3 skin diseases that are reactions to streptococcal infection
EN
Sweet’s
guttate ps
scleredema
strep toxic shock like syndrome

List 7 important causes of leukoplakia in an HIV positive individual.
1.Candida – thrush
2.EBV – oral hairy leukoplakia
3.HPV induced SCC
4.Oral florid papillomatosis – HPV 6,11??
5.Syphilitic mucous patches
6.HCV induced oral LP (+/- SCC induced from this)
7-Malignant and premalignant leukoplakia in tobacco users, ETOH, and from chronic irritation
8.Pseudo-hairy leukoplakia (identical clinically and histologically to EBV but no virus identified and etiology is unknown – seen in OTR)

What are the 2 most common HPV types in epidermodysplasiaverruciformis?
5,8

Explain the Rumple-Leeds test
Petechial after application of a BP cuff in those with RMSF
factors that result in chronic, non-healing wounds
1.Poor surgical technique (excessive tension, devitalized tissue)2.Vascular disorders (atherosclerosis, venous insufficiency)3.Tissue ischemia4.Infectious process5.Topically applied medications (C/S, iodine)6.Hemostatic agents (aluminum chloride, ferric subsulfate)7.Foreign body8.Adverse wound environment (dry instead of moist occlusive)9.Pressure10.Neuropathy11.Chronic radiation injury
local
•Malnutrition, protein deprivation, vit A & C deficiency•Systemic meds : c/s, penicillamine, nictoine, NSAID’s, antineoplastic agents•Chronic debilitation dz (hepatic, renal, heme, CVS, AI, oncologic)•Endocrine disorders (DM, Cushing)•Systemic vascular disorders (vasculitis, atherosclerosis)•CTD (Ehlers Danlos)•Advanced age (possibly thru impaired expression of MMP’s)
systemic

Define SPF
UVB only; UV for 1 MED @ 2mg/cm2 divided by UV for 1 MED no sunscreen. Ratio of the duration of UV radiation exposure necessary to produce MED in sunscreen-protected skin compared to the time for unprotected skin.
List the wavelengths of the following
UVA-I
UVA-II
UV-B
UV-C
340-400
320-340
290-320
200-290

what are the different histological types of BCC
1. Nodular 2. Superficial3. Micronodular4. Sclerosing/morpheaform5. Infiltrative6. Metatypical (large pale tumor cells, no pallisading, significant cytological atypia)7. Basosquamous carcinoma (rare with true squamous differentiation)8. Fibroepithelioma of Pinkus
What histological types are more aggressive?
1.Morpheaform2.Micronodular3.Infiltrative4.basosquamous 5.metatypical

How is Mohs performed?
Steps involved Mohs1. Patient prep and local anesthesia2. debulk and delineate extent of tumor with curette3. excise tumor with a 2-3 mm margin of normal tissue – scalpel held at 45 degree angle (undercutting is done parallel for saucerized excision)4. tissue is cut into quadrants and hatch marks are placed for orientation5. map is drawn of the excised pieces relative to the patient and pieces are numbered on the map6. tissue sections are inked – sky blue (up/right); red (down/left)7. tissues are oriented according to map on a petri dish with moist gauze (a mark is made to note specific orientation of the pieces)8. technician embeds tissues upside down (epidermis down) 9. frozen sections are cut and stained with H&E or toluidine blue10. Slides are reviewed microscopically and tumor is marked on map11. further resection and histologic examination is performed12. reconstruction is performed once margins are clear (some cases require permanent sections)


Ten indications for Mohs
“Where tumor recurrence would have an unacceptably low cure rate (or be devastating) and/or where tissue preservation is imperative”
Tumor factors1. Recurrent tumor or positive margin with prior excision2. Large tumor (> 2 cm)3. Poorly defined clinical borders4. High-risk anatomic location (periorbital, perinasal, perioral, periauricular)5. Other cosmetic/functionally important sites (periungual, genital)
Histological factors6. Aggressive histology-Sclerosing, micronodular, metatypical BCC-Poorly differentiated or deeply invasive SCC-Other tumor types with high recurrence with conventional surgery (eg, DFSP, MAC)7. Perineural invasion
Patient factors8. Previously irradiated skin9. Immunosuppressed patient10. Tumor in chronic scar (Marjolin’s ulcer)11. Nevoid basal cell carcinoma syndrome12. Xeroderma pigmentosum13. Basex’s syndrome

1) Papular (or small nodular form/micronodular) – numerous 2-5 mm red-brown papules that turn yellow usually on the upper part of the body.2) Nodular – less frequent 1-2 cm lesions often with surface telangiectasias; although rare to have mucous lesions, they are seen more commonly in the nodular form.-the “Cyrano form” causes disfiguring nasal lesions.3) Giant JXG - >2 cm.4) Mixed form – both small and large nodules present.5) JXG en plaque – lesions tend to coalesce.6) Lichenoid JXG7) Subcutaneous JXG – usually congenital and on the head.8) Erdheim-Chester disease – cutaneous and systemic xanthogranulomasinvolving bone (usually seen with nodular form).9) keratotic JXG10) Pedunculated JXG

Juvenile xanthogranuloma – clinical types, monitoring, complications
Epidemiology: •75% occur before age 1;•20-30% at birth•10% in adults. In adults the peak incidence is 20-30yo
Clinical: •pink-red-brown domed nodule yellows with age due to progressive lipidization•usually H&N and upper trunk•Extracutaneous sites: 1) ocular* *(most common) 2)pulmonary 3) visceral, bone, CNS lesions rare

Monitoring: •Full skin exam for CALM (in 20%) and stigmata of NF1•Ophthalmology assessment if less than 2y.o. (Ocular JXG’s affect the iris and can cause hyphema or glaucoma leading to blindness). Ocular involvement usually occurs before the age of 2 years. (Note 0.5% of those with cutaneous JXG develop ocular involvement, while 40% of patients with ocular JXG’s have cutaneous lesions)
•Monitor for signs and symptoms of juvenile CML (risk increases 20 fold if pt has both JXG’s and NF1)


Sweet’s syndrome – causes, criteria for diagnosis, treatment options.
Causes- Idiopathic, CA (AML, GU, Breast, GI), infection (strep, yrsenia, HIV, Hep C, CMV), pregnancy, meds (GMCSF, OCP, ATRA, lasix,
minocin, septra), CT disease, IBD
Treatment- ILK, pred, KI, dapsone, colchicine, cyclosporine, tetracyclines, clofazamine,
NSAIDs, IFN-a, cyclophosphamide.

Photoeruption – approach to photodermatitis
1-Idiopathic (PMLE, juv spring erup, actinic prurigo, chronic actinic derm. Solar urticaria
2-DNA repair defects (XP, Cockayne, Bloom, Rothmund-Thomson, Hartnup, Trichothiodystrophy…)
3-Photoaggrevation of dermatosis (Rosacea, LE, DM, REM…)
4-Photokoebenerization (vitiligo, ps, acne , LP actinicus…)
3/4 (overlap)- includes viruses like HSV, EM, GA, pemphigus erythematosus
5- Sun damage lesions (BCC, SCC, AKs, lentigines)
6- Medication (topical and systemic phototoxic and photoallergic reactions)
7- Porphyrias (PCT, EPP, pseudoporphyria....)

HSV – how do you do a Tzanck smear?
-Tzanck- Scrape base, (fix in alcohol), stain with Giemsa or Wright, look for multinucleated giant keratinocytes.

what has IgG & C3 along the DEJ (name 4)
1)Bullous pemphigoid2)Herpes gestationis (usually only C3 detected)3)EBA4)Cicatricial pemphigoid5)Bullous SLE6)Paraneoplastic pemphigus
List all diseases with IgA staining:
Dermatitis herpetiformisLinear IgA diseaseChronic bullous dermatosis of childhoodDrug-induced forms of linear IgA diseaseIgA pemphigus – subcorneal pustular dermatosis subtypeIgA pemphigus – intraepidermal neutrophilic IgA dermatosis subtype
IgA can also be a component along with IgG of the immunofluorescence in other autoimmune diseases such as bullous pemphigoid, EBA, CP

5 skin SE of isotretenoin
1) xerosis2) palmoplantar peeling3) photosensitivity4) retinoid dermatitis5) pyogenic-like granulomas6) paronychia7) cheilitis
3 things to avoid while on accutane
8) Pregnancy9) Alcohol10) Vitamin A limited to less than 5000 IU per day.11) Avoid an excessively fatty diet
when post can you have CO2 laser

Name five teratogenic effects of Accutane
1) Cardiovascular-ASD/VSD; abnormal origin of subclavian arteries; hypoplastic/interrupted aortic arch; overriding aorta.
2) Craniofacial-cleft palate; depressed midface; jaw malformation; triangular microcephalic skull.
3) Ocular-microphthalmia; optic nerve atrophy.
4) Auditory-sensorineural hearing loss; absent auditory canals; vestibular dysfunction.
5) Bone-absent thumb; absent clavicle and scapula; aplasia of long bones;
short sternum.
6) CNS-agenesis of cerebellar vermis; hydrocephalus; microcephaly, meningomyelocele; leptomeningeal neuroglial heterotopias.
7) Thymus aplasia or hypoplasia.8) Anal and vaginal atresia.


Lupus erythematosus
a. Name 11 criteria:
Malar rashDiscoid RashPhotosensitivityOral or nasal ulcers (painless)Arthritis (non-erosive in 2 or more peripheral joints)Serositis (pleuritis or pericarditis)Renal disorder (proteinuria >0.5 g/d or 3+ or cellular casts)Neurological (seizures or psychosis)Hematologic (hemolytic anemia, leukopenia (<4), lymphopenia (<1.5),
or thrombocytopenia (<100))Immunologic (LE cell prep +, anti-DNA, anti-Sm, VDRL, anti-cardiolipin Ab)
ANA +



b. Patterns of LE(Gilliam Classification system):
LE-specific skin disease:
1)ACLEi) localized (malar rash)ii) generalized ACLE
2)SCLEi) Annular
ii) Psoriasiform
3)CCLEi) Discoidii) Hypertrophic/verrucous DLEiii) Lupus profundus/lupus panniculitis
iv) Mucosal DLE –oral or conjunctivalv) Lupus tumidus
vi) Chilblain LEvii) Lichenoid DLE (LE/LP overlap)

LE-nonspecific skin disease:
i) Vasculitis – LCV, urticarial vasculitisii) Vasculopathy – degos-like lesions, atrophie blanche, periungual telangiectasia, livedo reticularis, thrombophlebitis, Raynaud’s phenomenon, erythromelalgia.iii) Non-scarring alopecia – lupus hair, telogen effluvium, alopecia areata.iv) Sclerodactyly.v) Rheumatoid nodules.vi) Calcinosis cutisvii) Urticariaviii) Papulonodular mucinosisix) Cutis laxa/anetodermax) Acanthosis nigricansxi) Erythema multiformexii) Leg ulcersxiii) Lichen planus


c. 2 patterns of SCLE
1)Annular (lupus marginatus)
2)Psoriasiform (papulosquamous SCLE)
3)-drug-induced – HCTZ, ACE inhibitors, diltiazem, terbinafine, naproxen, piroxicam, sulfonylureas, sprionolactone, ranitidine, griseofulvin.

d.name pathology features (5 criteria of DLE)
-thickened basement membrane zone.-superficial and deep perivascular and periadnexal lymphocytic infiltrate.-vacuolar alteration of DEJ with lichenoid infiltrate.-eosinophilic colloid bodies.-follicular plugging.-mucin deposition in reticular dermis.-melanophages with pigmentary incontinence.

E . treatment of DLE
Sun protectionPotent topical corticosteroids and intralesionalcorticosteroids.Hydroxychloroquine sulphate (<6.5 mg/kg/day) – smoking cessation.-quinacrine may be addedChloroquine (3.5-4 mg/kg/day maximum).Oral retinoidsThalidomideGoldClofazamineSystemic corticosteroids

Give two disease with +ve Auspitz sign not including Ps
Auspitz sign can be positive is Darier's disease and actinic keratosis.
What is Darier's sign and what is pseudo darier sign?Give 3 diseases with +ve darier sign
Rubbing a lesion of mastocytoma causes urtication, flare, swelling and sometimes blister formation due to release of histamine. In contrast, pseudo-Darer's sign is seen in smooth muscle hamartoma where there is increase in induration and piloerection after firm stroking
Other conditions where one could find positive Darier's sign are:- leukemia cutis
- juvenile xanthogranuloma- Langerhans cell histiocytosis

Pyoderma gangrenosum:
a. 4 Major clinical forms:
1) Ulcerative
2) Bullous – AML
3) Pustular – IBD, bowel-associated dermatitis-arthritis syndrome, Behcet’s.
4) Superficial granulomatous

b. Associations:
1)Inflammatory bowel disease – Crohns, ulcerative colitis
2)Lymphoproliferative disorders-hairy cell leukemia, monoclonal gammopathy (IgA), multiple myeloma.
3)Arthritis-rheumatoid arthritis, bowel-associated dermatitis-arthritis syndrome.
4)Myelodysplastic disorders-AML, myelofibrosis, myelodysplasias
5)Vasculitis-Behcet’s, Wegener’s granulomatosis



c. two topical treatments, two systemic treatments:
-potent topical steroids (clobetasol propionate)-topical tacrolimus
-prednisone, dapsone, minocycline, clofazamine, cyclosporine.

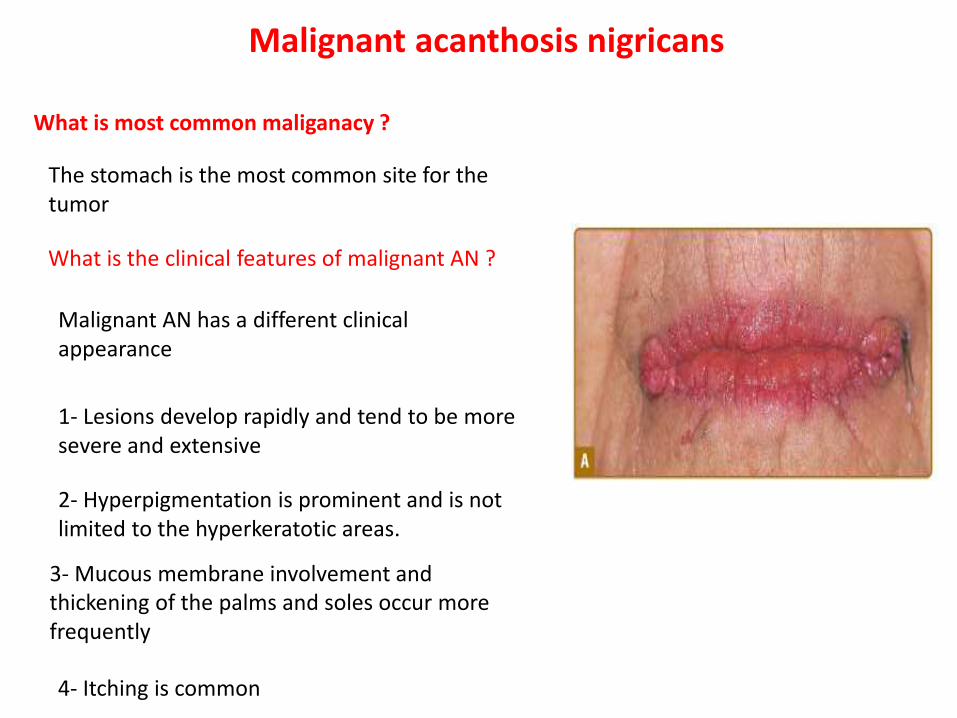
Malignant acanthosis nigricans
What is most common maliganacy ?
What is the clinical features of malignant AN ?
The stomach is the most common site for the tumor
Malignant AN has a different clinical appearance
1- Lesions develop rapidly and tend to be more severe and extensive
2- Hyperpigmentation is prominent and is not limited to the hyperkeratotic areas.
3- Mucous membrane involvement and thickening of the palms and soles occur more frequently
4- Itching is common
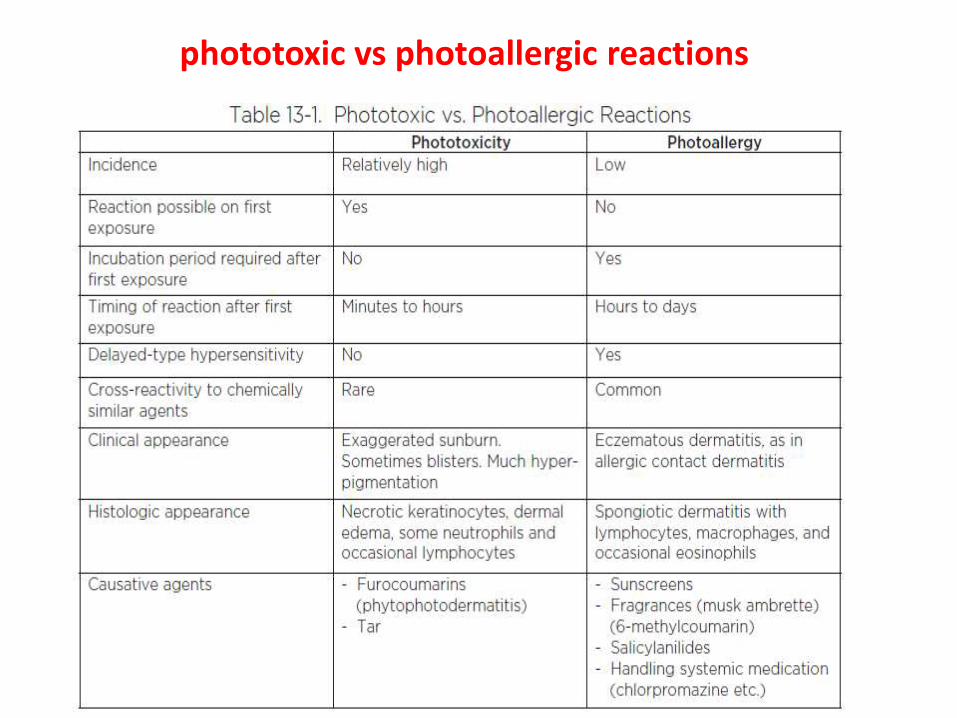
phototoxic vs photoallergic reactions

Name all of the cutaneous forms of sarcoid:
i) Specific (contain granulomas):
1) Maculopapular – most common (acute sarcoid)2) Nodular3) Annular plaque – chronic sarcoid4) Darier-Roussy nodules5) Infiltrative/scar sarcoid6) Lupus pernio – hallmark of chronic fibrotic disease.7) Ichthyotic8) Ulcerative9) Perforating10) Angiolupoid11) Many others – Hypopigmented, verrucous, psoriasiform,
folliculitis, lichenoid, eruptive, erythrodermic, penile, granulomatous cheilitis, morpheaform, umbilicated.
ii) Non-specific/reactive
1) Erythema nodosum2) Prurigo

Alopecia areata:
a) Morphological patterns:
1.Alopecia areata circumscripta (patchy).2.Reticular pattern3.Ophiasis pattern4.Sisapho (ophiasis inverse) – fronto-parieto scalp.5.Diffuse alopecia areata.6.Alopecia totalis.7.Alopecia universalis.

List 4 bad prognostic signs:
1.Atopy (up to 40%).
2.Family history.
3.Comorbid autoimmune disorders (thyroid, vitiligo, IBD).4.Young age of onset (children under age 5
5.Nail dystrophy (pitting, trachyonychia, onychorrhexis, onychomadesis, red-spotted lunulae, koilonychia).
6.Extensive hair loss (totalis/universalis).
7.Duration of hair loss in a given area.
8.Ophiasis pattern.

List 2 local treatments:
1.Topical steroids.
2.Topical immunomodulators.
3.Topical contact sensitizers (diphenylcyclopropenone, anthralin, squaricacid dibutyl esters).
4.Topical Minoxidil.
5.Intralesional corticosteroids.

•What’s a flame figure? Three diseases it’s found in
Flame figure:
- poorly circumscribed focus of eosinophilic collagen
- from eosinophilic granules (major basic protein) adhering to dermalcollagen bundles
-sometimes see basophilic fibrillar material at periphery
Found in:
1. Eosinophilic cellulitis (Well’s syndrome)2. Arthropod reactions3. Parasitic infections (Splendore-Hoeppli deposits around parasites in tissues)Also in: -BP
-Herpes gestationis-diffuse erythemasdermatophyte infections

Two new topical treatment for Rosacea

•List 5 cutaneous manifestations of Crohn’s disease
1. Oral Crohn’s disease
2. Cutaneous Crohn’s disease (metastatic Crohn’s)
3. Contiguous perianal Crohn’s disease (1/3 of all patients)
4. Reactive skin findings-Cutaneous PAN-LCV-Pyoderma gangrenosum-EN-EM-Clubbing-Palmar erythema
-EBA
5. Nutritional deficiency-Zinc-deficiency mimicking acrodermatitis enteropathica



Four causes of hirsutism
1. Idiopathic hirsuitism
2. PCOS
3. Androgen-secreting tumor (ovarian or adrenal)
4. Late-onset congenital adrenal hyperplasia (21-hydroxylase deficiency)
5. Prolactinoma/Hyperprolactinemia
6. Severe insulin resistance syndromes
7. Drug (androgenic progestins, anabolic steroids)

Four drugs to treat hirsutism and the MOA1. Oral contraceptive Suppress ovarian androgen production,
increase SHBG
2. Spironolactone ↓ Ovarian testosterone production, androgen receptor blockade
3. Flutamide Androgen receptor blockade
4. Cyproterone acetate Androgen receptor blockade


Ten cutaneous associations with renal failure
1. Skin colour changes-Pallor-Sallow yellowish cast
-Hyperpigmentation2. Solar elastosis3. Ecchymoses (due to platelet dysfunction)4. Xerosis5. Acquired ichthyosis6. Decreased skin turgor7. Uremic frost8. Half-and-half nails9. Pruritus (most common)10. Acquired perforating dermatoses11.Metastatic calcification
-Calcinosis cutis-Calciphylaxis
12. Bullous dermatoses-PCT-Pseudoporphyria

Five vascular changes with alcoholic liver disease
1. Spider angioma2. Palmar eythema3. Corkscrew scleral vessels4. Caput medusae5. Plethoric facies6. Transient flushing6. Unilateral nevoid telangectasia

Photodynamic therapy:
Describe the pathophysiology of cellular damage
-In PDT, a photosensitizing chemical is given either topically (ALA or mALA; hydrophilic)or systemically (porfimer sodium, temoporfin; hydrophobic). This is taken up by the cells
and is converted to protoporphyrin IX (PpIX) in the mitochondria. It leaks from the mitochondria to other cellular structures and then to the blood vessels. The target tissue is then irradiated with photo-activating light(blue light – 417 nm for epidermal lesions; red light – 630 nm for deeperlesions). Porphyrins are able to convert from a ground state to a singletand finally to a triplet state possessing a longer lifetime. If tissue oxygenis present, an interaction occurs and singlet oxygen is created. This singlet oxygenoxidizes amino acids, DNA and lipids causing molecular cross-linking.Preferential inactivation of bcl-2 occurs; cytochrome c leaks from the Mitochondrial membrane and activates caspase-3 and get apoptosis.


Name 5 diseases that respond to PDT
Actinic keratosis (FDA indication)
Actinic cheilitisBowen’s diseasePsoriasisCTCLSuperficial BCCAcneCondylomata

Draw IgA Molecule
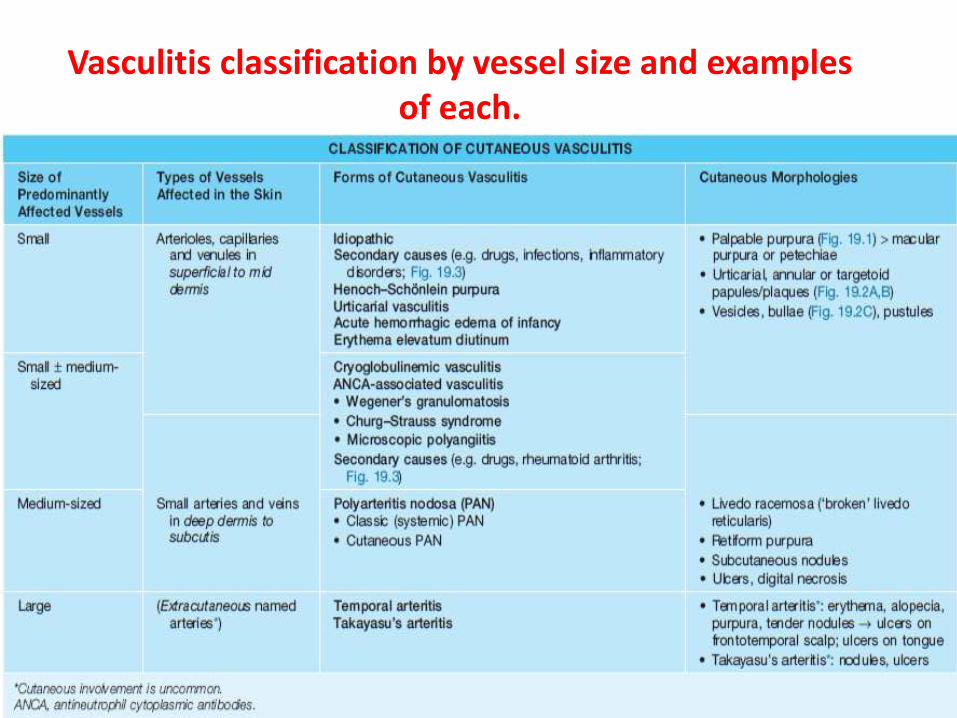
Vasculitis classification by vessel size and examples of each.

List advantages to using nb-UVB (311-313 nm)
1. nbUVB is less erythemogenic than broad-band UVB (BB)2. More effective for treatment of psoriasis than BB-higher clearance rates and duration of remission; though lower than PUVA3. As effective as PUVA for vitiligo4. More convenient than PUVA (no oral medication or bath required)5. Possibly less long-term risk of photocarcinogenesis than PUVA (but long-term data lacking)

EBM

Sensitivity: Proportion of people who actually have disease that test positiveNegative result of a sensitive test rules out disease “SnOut”Test with high sensitivity: won’t miss anyone who has disease (but will also
have false positives)eg, negative ANA helps rule out SLE
Specificity: Proportion of patients without the disease that test negativeSpecific test will rarely misdiagnose people who don’t have disease as
diseasedPositive result on specific test rules in disease “SpPin”eg, positive anti-Sm makes you pretty confident that someone has SLE
PPV: Proportion of people with positive test who actually have the diseasePPV increases with disease prevalence
NPV: Proportion of people with negative test who truly do not have diseaseNPV decreases with increasing disease prevalence
Odds ratio: Ratio of odds of exposure among those with and without outcome of interest
Measure of risk in a case-control study“the equivalent of relative risk in a case-control study” – R. Hayes

p-value: the likelihood that an observed association has arisen by chance alone
-(whereas, in fact, no such association exists)
low p-value (eg, < 0.05) is statistically significant (but may not be clinically significant)
-difference observed in study would be expected to occur by random chance alone in less than 5% of repetitions of study
CI: range of plausible valuesa measure of precision; width
corresponds to most likely range of values to contain the true value

clinical difference between SCLE and DLE (list 5):
SCLE vs DLE
1. SCLE no scarring vs DLE scarring2. SCLE despite the name, at least 50% of patients meet the criteria for a diagnosis of SLE (75% have arthralgia or arthritis, 20% have leucopenia, 80% have +ANA) vs DLE no associated systemic involvement and rare to progress to SLE ~5% patients3. drug-induced SCLE vs no drug induced DLE4. SCLE +ANA ~80% vs <5% +ANA (if positive, may progress to SLE)5. SCLE: scaly papules, which evolve into either psoriasiform, more commonly, or polycyclic annular lesions (scale is thin, easily detached, telangiectasis and dyspigmentation are nearly always present – follicles are not involved and there is no scarring) vs DLE: dull red macules with adherent scales extending into patulous follicles (remove scale, undersurface has carpet tack scale – horny plugs that fill the follicles), patches heal centrally first, with atrophy, scaring, dyspigmentation and telangiectasia.

DLESCLEDifference
+-Scaring
-+Drug induce
5%50%Symptoms of SLE
5%80%ANA +VE
dull red macules with adherent scales extending into
patulous follicles (remove scale,
undersurface has carpet tack scale –
horny plugs that fill the follicles), patches heal
centrally first, with atrophy, scaring,
dyspigmentation and telangiectasia.
scaly papules, which evolve into either
psoriasiform, more commonly, or polycyclic annular lesions (scale is thin, easily detached,
telangiectasis and dyspigmentation are
nearly always present –follicles are not involved and there is no scarring
Lesions

List 6 clinical features that may suggest a subungual melanoma in a patient with melanonychia
1. melanonychia which begins in a single digit of a person during 4th-6th decade of life or later (however, subungual melanoma has been seen in children)2. melanonychia develops abruptly in a previousl normal nail plate3. it becomes suddenly darker or wider4. occurs in either thumb, index finger or great toe5. occurs singly in the digit of a dark-skinned patient, particularly if the thumb or great toe is affected6. demonstrates blurred, rather than sharp, lateral borders7. occurs in a person who gives a history of malignant melanoma8. occurs in a person in who the risk of melanoma is increased (dysplastic nevus syndrome)9. is accompanied by nail dystrophy, such as partial nail destruction or disappearance10. occurs in a person who gives a history of digital trauma (several authors have implicated trauma in the pathogenesis of subungual melanoma)11. Hutchinson’s sign: periungual spread of pigmentation to the proximal and lateral nail folds as well as to the tip of a single digit (corresponds to the radial growth phase of subungual melanoma)
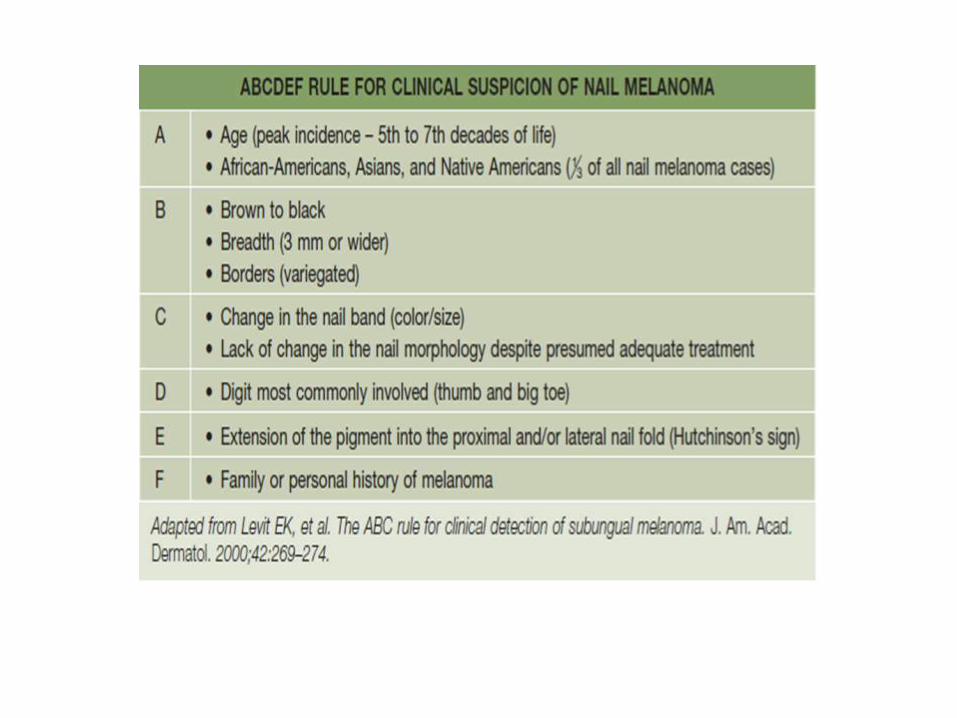

Hutchinson’s sign
single nail vs multiple nails
blurred margin
proximal portion of band is wider than distal
history of change (size, color)
accompanying nail dystrophy
Red Flag

List 3 nail signs seen in liver disease
- Terry’s nails
- Muehrcke lines (from hypoalbuminemia)
- clubbing.

Skin diseases/syndromes with cardiac involvmetCardiac involvmentDisease
tetralogy, Ao aneurysm, ASD, pulm artery stenosis, spont large vessel rupture, mitral
regurg, valvular prolapse
EDS( 1,2,4,5)
dissecting Ao aneurysms, mitral and Ao regurgitation, MVP
Marfans
Ao aneurysm, cor pulmonale, peripheral pulmonic stenosis, MVP
Cutis laxa
rhabdomyosarcoma (TS rhabdomyoma), renovasc HTN, pulm stenosis
NF-1
AV fistula esp pulm, pulmonary HTNOsler-weber-rendu
accelerated atherosclerosis, HTNProgeria
atrial myxomasCarney complex
pulmonary stenosisWatson synd
atherosclerosisHomocysteinuria
arrythmias with heart block, cardiac failure
Refsum disease

The 2013 Contact Allergen of the Year ??
methylisothiazolinone
Methylisothiazolinones are biocidal preservatives added to bubble solutions, bubble baths, soaps and cosmetic productsdiaper wipes
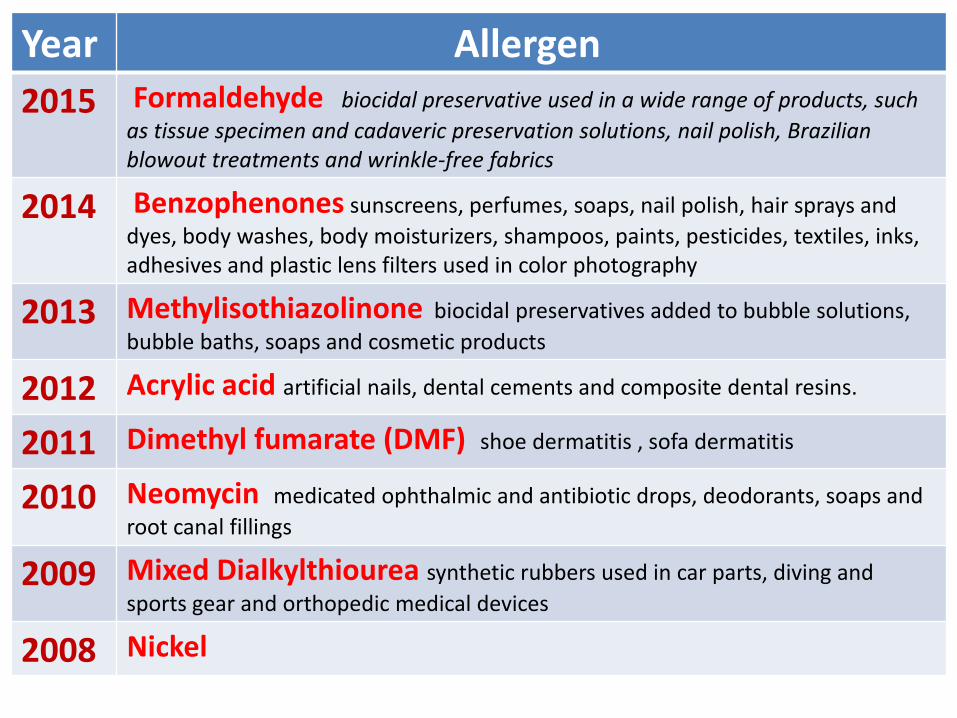
Allergen Year Formaldehyde biocidal preservative used in a wide range of products, such
as tissue specimen and cadaveric preservation solutions, nail polish, Brazilian blowout treatments and wrinkle-free fabrics
2015
Benzophenones sunscreens, perfumes, soaps, nail polish, hair sprays and
dyes, body washes, body moisturizers, shampoos, paints, pesticides, textiles, inks, adhesives and plastic lens filters used in color photography
2014
Methylisothiazolinone biocidal preservatives added to bubble solutions,
bubble baths, soaps and cosmetic products 2013
Acrylic acid artificial nails, dental cements and composite dental resins.2012
Dimethyl fumarate (DMF) shoe dermatitis , sofa dermatitis2011
Neomycin medicated ophthalmic and antibiotic drops, deodorants, soaps and
root canal fillings2010
Mixed Dialkylthiourea synthetic rubbers used in car parts, diving and
sports gear and orthopedic medical devices2009
Nickel2008

Relationship of h.pylori to skin diseases
Chronic urticaria
Rosacea
Psoriasis
Sjogren syndrome
Others : sweet, henoch schonlein purpura,lichen planus

What is R.E.M Disease
Reticular erythematous mucinosis
Midline mucinosis
It most often affects middle-aged women

What are systemic photoprotective agents
b. Caroten
Antimalaria
Ascorbic acid
Retinol
Green tea
Antihistamines
Aspirin
Indomethacin
corticosteroids
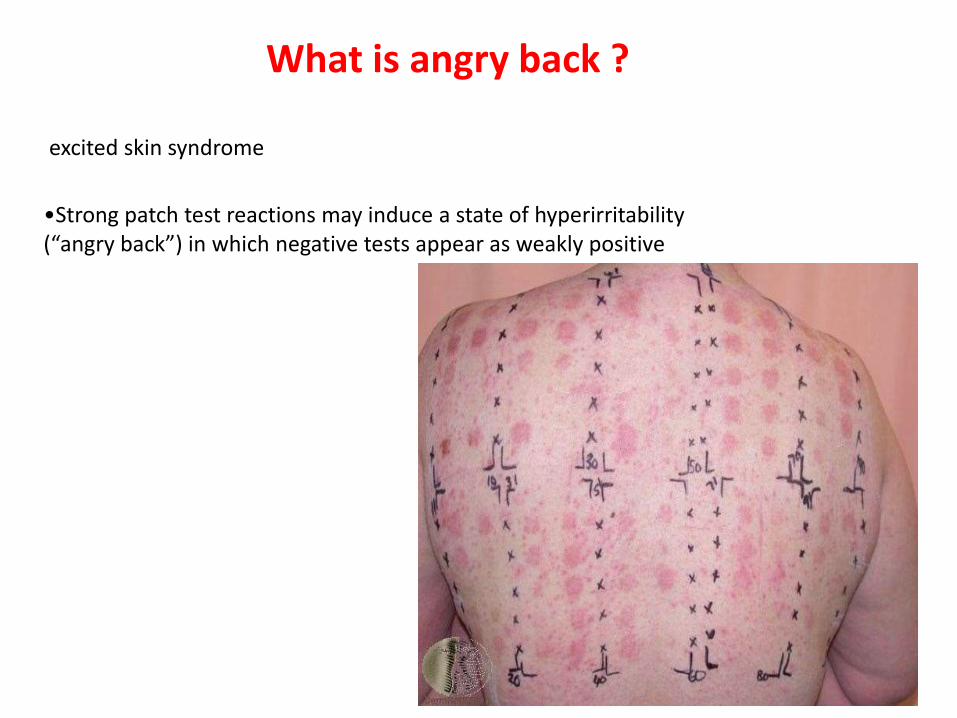
What is angry back ?
excited skin syndrome
•Strong patch test reactions may induce a state of hyperirritability (“angry back”) in which negative tests appear as weakly positive

Give one MOA of why neutrophils are seen in psoriasis plaques
•In psoriasis TNF-is a major cytokine which induces the expression of IL-8, which enhances accumulation of neutrophils and T-lymphocytes.
•IL-8 is chemotactic for neutrophils and T-lymphocytes. It also activates neutrophils.

Give 8 skin types of TB : a) exogenous exposure/direct inoculation:
1. primary TB chancre2. TB verrucosa cutis (warty tuberculosis,
prosector’s wart)
b) endogenous infection :
3. scrofuloderma4. acute miliary TB5. lupus vulgaris6. tuberculous gumma (metastatic
tuberculous ulcer)7. orificial tuberculosis (autoinoculation)
c) Tuberculids:
8. papulonecrotic eruption,9. lichen scrofulosorum10. erythema induratum of Bazin

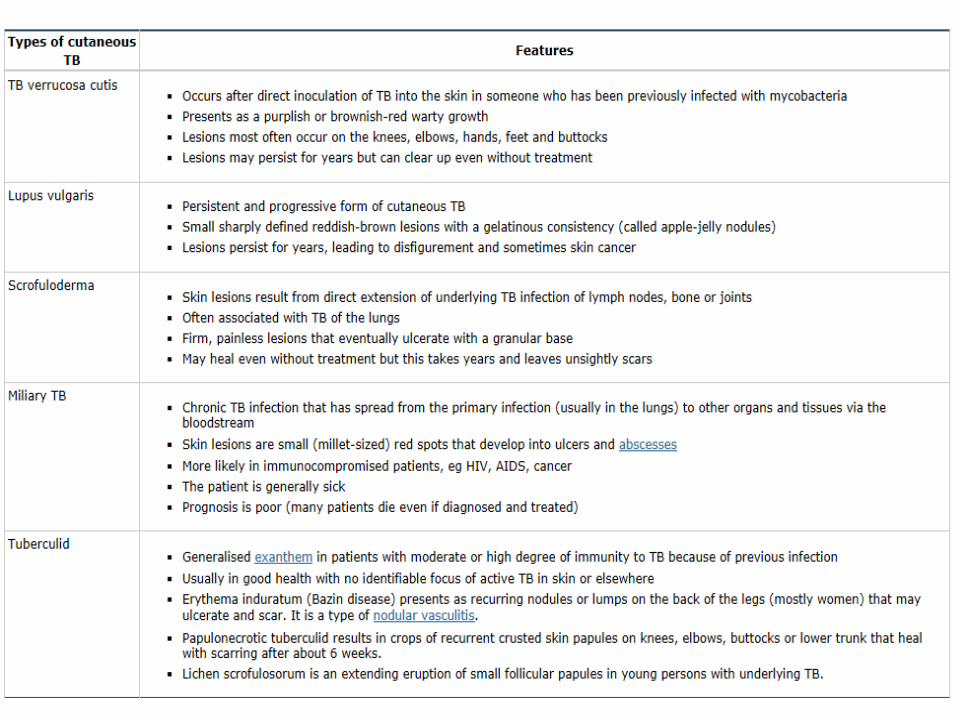

primary TB chancreTB verrucosa cutis

lupus vulgaris scrofuloderma

orificial tuberculosis

papulonecrotic eruption erythema induratum of Bazin

Pregnant and chickenpox
Common complication of chickenpox in pregnant women ?
Pneumonia ------10 – 20%
What are the Risk factors for varicella pneumonia during pregnancy?
- Smoking - Number of lesions more than 100

What is risk of developing congenital varicella syndrome?
congenital varicella syndrome is uncommon
The risk is greatest when infection occurs during the first 20 weeks of pregnancy
The absolute risk of embryopathy after maternal varicella infection in the first 20 weeks of pregnancy is approximately 2%.
Features of congenital varicella syndrome

Clinical features of congenital varicella syndrome — Congenital varicella syndrome, first described in 1947, is characterized by the following findings :
- Cutaneous scars in a dermatomal pattern
- Neurological abnormalities (eg, mental retardation, microcephaly, hydrocephalus, seizures, Horner’s syndrome)
- Ocular abnormalities (eg, optic nerve atrophy, cataracts, chorioretinitis, microphthalmos, nystagmus)
- Limb abnormalities (hypoplasia, atrophy, paresis)
- Gastrointestinal abnormalities (gastroesophageal reflux, atretic or stenoticbowel)
- Low birth weight
Congenital varicella syndrome is associated with a mortality rate of 30 percent in the first few months of life and a 15 percent risk of developing herpes zoster in the first four years of life


maternal antibody can develop and transfer via the placenta
Maternal infection that develops more than 2 days after delivery is associated with onset of disease in a newborn approximately 2 weeks later, at which point the immune system is better able to respond to the infection.

Where are the hyphae in the most common form of onychomycosis
Distal/lateral subungual- close to the nail bed at the lowest portion of the nail plate

AGEP (Acute generalized exanthematous pustulosis)
1. List the 2 most common antibiotic causes
B-lactams, macrolides (Bolognia)
2. Describe the histology
Spongiform pustules within and just under the stratum corneum. Some papillary dermal edema, and perivascular infiltrate with eosinophils
3. List 2 clinical dDx
Pustular psoriasis,Sneddon-Wilkinson

4. Most common lab finding
1- Hi WBC (with increased neuts). Can also get some eosinophilia2- transient renal dysfunction 3- hypocalcemia.
5. Treatment
Drug withdrawaltopical corticosteroids
supportive measures (including antipyretics)
6. Any way to confirm the diagnosis with a diagnostic test?
Patch testing


How can you differentiate etween AGEP and Pustular Ps ?
- The pustules seen in both diseases are clinically indistinguishable
- Additional skin lesions, including petechiae, purpura, atypical target-like lesions and vesicles, are more frequently observed in AGEP.
- the acuteness of the disease and the drug history in AGEP (( 1-2 Days))
- The histologic findings can be helpful. Massive edema in the superficial dermis, vasculitis, exocytosis of eosinophils, and necrosis of keratinocytes are all suggestive of AGEP, whereas acanthosis is more characteristic of pustular psoriasis
AGEP seems to be seen more frequently in patients with a history of psoriasis, thus making the differential diagnosis even more difficult in some patients.

Histo: differentiate by 2 H +E methods the following:
Steatocystoma from epidermoid cyst
Sebaceous gland in wall, thin keratinized cuticle lining cyst without granular layer.


Pagets from bowens
No intercellular bridges, mucin is +ve
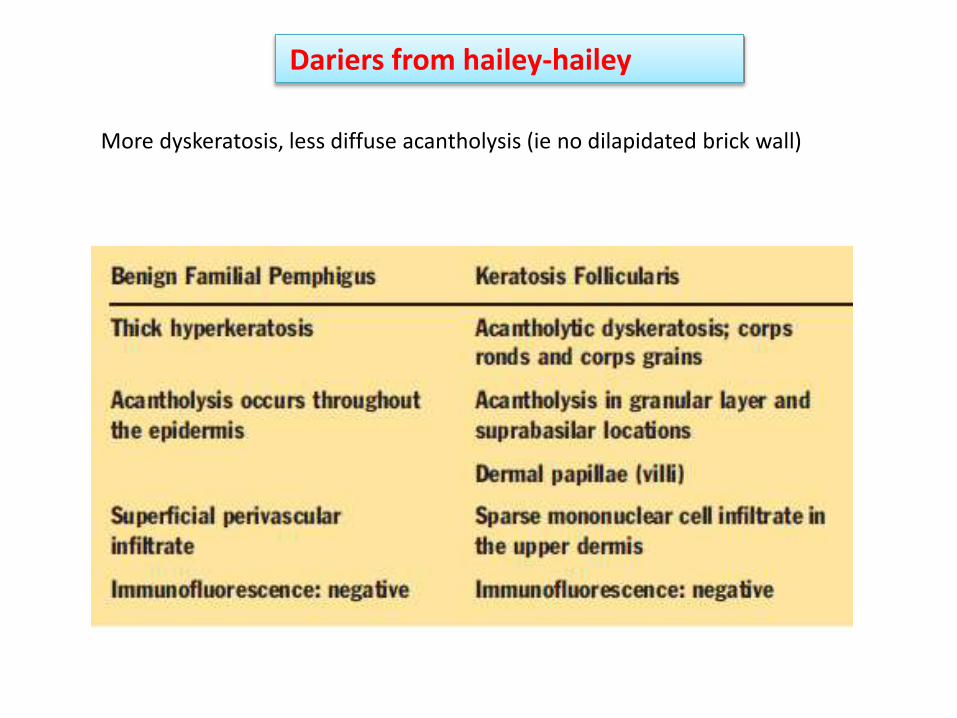
Dariers from hailey-hailey
More dyskeratosis, less diffuse acantholysis (ie no dilapidated brick wall)


GA from NLD
Central mucin (as opposed to central necrobiosis), much fewer plasma cells

Name the immunostain the distinguishes the two (positive for the 1st, negative for the 2nd)
1. merkel vs bowens
paranuclear dot CK20 or “pankeratin”
2. extramamm pagets vs bowens
LMWK (CAM 5.2 = cytokeratins 8, 18)
3. melanoma vs langerhans histiocytosis
HMB-45, Melan-A/MART-1
4. angiosarcoma vs atypical fibroxanthoma
CD31
5. DFSP vs DF
CD34

DFSPangiosarcoma
extramammpagets
melanoma merkel
CD34DF
LMWK (CAM 5.2 = cytokeratins 8, 18)
paranuclear dot CK20
bowens
HMB-45, Melan-A/MART-1
langerhanshistiocytosis
CD31atypical fibroxanthoma
+VE
-VE

Describe the 2 mechanisms for drug-induced pemphigus and describe what happens to the eruption once the drug is discontinued
1) direct interference with or non-immune destruction of adhesion molecules (DG1, DG3) resulting in acantholysis. This tends to be linked to thiol (-SH) containing drugs (penicillamine, ACEi, gold).
2) Induction of antibody reaction against DGs, possibly through modification of the DGs to make them more antigenic. This mechanism tends to be linked to drugs without thiol groups (antibiotics, nifedipine, propanolol, piroxicam, phenobarb). The active component in this group may be an amide.
Generally, patients remit when drug is d/ced. Some may progress to PV. Non-thiol drugs have a worse prognosis than thiol drugs because of the non-thiols’ association with antibody generation. (E-Medicine)

name 2 tumours which can be acantholytic and have an impact on the prognosis of the tumour
1- Acantholytic SCC – poorer px (3-10x increased risk of mets)
2- Acantholytic AK – less responsive to cryotx

•AKs: what are 3 clinical variants?
hypertrophic, pigmented, actinic cheilitis, atrophic
What are 5 histological variants?
Hypertrophic (lichenoid is variant of this), atrophic, pigmented, bowenoid, acantholytic
•What are 8 ways to treat AKs?
1. LN22. 5FU topically (2.5%, 5%, 0.5% Carac)3. topical diclofenac (Solaraze gel) 4. Imiqimod cream5. Chemical peel – Jessner’s/TCA6. ALA-PDT7. Shave excision or curettage8. Systemic retinoid (acitretin)9. CO2 for actinic chelitis

•What are 5 clinical variants of MF (besides patch, plaque or tumour)
1- clinical variants such as bullous and hyper- or hypopigmentedMF have a clinical behaviour similar to that of classical MF and are therefore
NOT CONSIDERED separately – Bolognia
2- Follicular MF (MF-associated follicular mucinosis)
3- Pagetoid reticulosis (Woringer-Kolopp disease-localized type)
4- Granulomatous slack skin

How do you differentiate clinically b/w Vitiligo and Leprosy?
Leprosy is more hypopigmented than depigmented, it can have raised lesions (plaques, nodules), it can have overlying sensory change, it can have associated nerve enlargment

Different types of Miliaria and their microscopic locations?
1- Crystallina (stratum corneum aspect of acrosyringium),
2- rubra (stratum spinosum)
3- pustulosa (is a type of miliara rubra)
4- profunda (upper dermis/DEJ).

Tinea Pedis
4 types
1- moccasin - T. ruburm/E. floccosum - Difficult to clear b/c low immunogenicity limits host response
2- Interdigital - T. mentag/rubrum, E. floccosum -Usually last 2 webs. Assoc with dermatophytosis complex
3- Inflam/vesicular - T. mentag - Assoc with dermatophytid on hands
4- Ulcerative - T. rubrum, menta, E. floccosum - Erosive changes in webs seen with immunosupp, diabetes

4 complications
1- dermatophytosis complex – bacterial superinfection
2- dermatophytid rxn
3- cellulitis (those with venous HTN)
4- osteomyelitis (diabetics)

List 5 side effects of PUVA
Short-term:
1. Nausea and vomiting (oral PUVA)2. Redness/swelling/blistering3. Hyperpigmentation4. Persistent pruritis
Long-term:
5. Cataract formation (oral PUVA; although no clinical evidence of risk)6. Dermatoheliosis7. PUVA lentigines8. Increased risk of SCC (> 200 treatments means 30x ↑ risk of SCC)

What are painfull skin tumors
"LEND AN EGG".
- Leiomyoma
- Eccrine spiradenoma
- Neuroma
- Dermatofibroma
- Angiolipoma
- Neurilemmoma
- Endometrioma
- Glomus tumor
- Granular cell tumor

Dermatosis on the shin of tibia
Itchy :
1.Lichen simlex chronicus
2.Hyperk. LP
3.Lichen amyloidosus
4.Prurigo nodularis
1.Erythema nodosum
2.NBLD
3.Ecthyma
4.Pretibial myxedema
Non itchy :

Dermatoses with island of normal skin
PRP
MF
BB

Dermatoses on the posterior aspect of the leg
Nodular vasculitis (erythema induratum of Basin)

List causes of genital ulcers
Sexually transmitted diseases
1- Herpes simplex2- Syphilis 3- LGV 4- Chancroid5- Granuloma injuinale6- Scabies 7- HIV
Non sexually transmitted diseases
1- fixed drug eruption2- malignant ulcer3-bollouse diseases4- traumatic ulcer5-herpes zoster6-erosive balanitis7- tuberculosis ulcer

Thank you

2014 Year in Review

Infectious Disease
FDA Approves Two Topical Treatments for Onychomycosis
Currently, oral terbinafine provides the best reported cure rates
dermatologists are in need of safer and more efficacious treatment options
1- Topical efinaconazole 10% solution
the first topical triazole to receive FDA approval for the treatment of toenail onychomycosis.
2- tavaborole 5% solution
While efinaconazole and tavaborole do not appear more efficacious than systemic antifungals, they provide safe treatment alterantives



New Antibiotics Approved for Treatment of Skin Infections
Several new agents have efficacy and safety profiles similar to vancomycin or linezolid in the treatment of acute cellulitis, wound infections and abscesses, including infections caused by methicillin-resistant Staphylococcus aureus (MRSA).
Dalbavancin
was FDA approved on May 23, 2014 for the treatment of acute bacterial skin and skin structure infections (ABSSSI) caused by S aureus and Streptococcus pyogenes.4 Two doses of intravenous (IV) dalbavancin (1 g IV on day 1 and 500 mg IV on day 8) were as effective as a 3-day dose of IV vancomycin (1 g every 12 hours) with or without extension of therapy 10 to 14 days with oral linezolid (600 mg every 12 hours). Clinical success was observed in 91% of patients treated with dalbavancin and 94% of patients treated with vancomycin with or without linezolid. Adverse events of nausea, diarrhea and pruritus were reported less in the dalbavancin group than the vancomycin group with or without linezolid.

Tedizolid phosphate
was also approved by the FDA on June 20, 2014, for the treatment of ABSSSI.
This second-generation oxazolidinone was evaluated in 2 Phase III trials (ESTABLISH-1 and ESTABLISH-2), which demonstrated non-inferiority in the group receiving tedizolidphosphate 200 mg once daily for 6 days compared to linezolid 600 mg twice daily for 10 days.5 The most common adverse events, such as nausea and diarrhea, were reported less in the tedizolid phosphate groups in both studies


Oritavancin
received FDA approval in August 2014
Two Phase III studies (SOLO I and SOLO II) demonstrated that a single 1,200 mg IV dose of oritavancin yielded similar efficacy to a 7- to 10-day IV dose of vancomycin.7,8 The incidence of adverse events was also slightly less in the oritavancin group. The more desirable safety profiles, as well as the likelihood for greater patient adherence with shorter and more convenient dosing, make these new antibacterial agents a promising option, particularly in the treatment of MRSA infections.
Innovative Treatment for Recurrent Herpes Labialis
Once daily, high dose, oral antiviral drugs have long been the mainstay of herpes labialis treatment. Acyclovir Lauriad (Sitavig, Innocutis), is a novel mucoadhesive buccal tablet (MBT) that delivers a high concentration of acyclovir directly to the affected site through the mucous membrane.9 It is recommended to apply the 50 mg MBT at the onset of prodromal symptoms to the upper gum. Phase III trials using a single application of the 50 mg acyclovir Lauriad MBT yielded greater improvement in symptoms, reduced outbreak duration and reduced recurrence compared with placebo.10 This is exciting news for dermatologists and patients alike, as this innovative treatment serves to combat the often debilitating and stigmatizing symptoms of herpes labialis


Topical Ivermectin for Papulopustular Rosacea
Papulopustular rosacea (PPR) is a chronic inflammatory disorder that has limited treatment options; however, a new topical therapy may be on the horizon. The results of 2 randomized, double-blind, vehicle-controlled studies published in March 2014 found once-daily ivermectin1% cream (Galderma Laboratories) to be more effective than vehicle in treatment of moderate-to-severe PPR. About 40% of subjects using ivermectin 1% cream achieved Investigator’s Global Assessment (IGA) of clear or almost clear at 12 weeks, compared to about 12% to 18% with vehicle (P<.001 in both studies).14 A Phase III, investigator-blinded, randomized, parallel group study published in September 2014 found once-daily ivermectin1% cream to be superior to twice-daily metronidazole 0.75% cream (84.9% vs 75.4%, respectively, of subjects achieving IGA of clear or almost clear; P<.001).15 Adverse events were comparable between groups, and local tolerability was superior with ivermectin



Psoriasis and Related Biologics
Apremilast Approved for Plaque Psoriasis
On March 21, 2014, apremilast (Otezla, Celgene Corporation) was approved by the FDA for the treatment of adults with active psoriatic arthritis.17 On September 23, 2014, the treatment received an expanded indication for patients with moderate-to-severe plaque psoriasis who are candidates for phototherapy or systemic therapy.
Apremilast is an oral inhibitor of phosphodiesterase 4, which results in increased intracellular cyclic adenosine monophosphate, which indirectly modulates the production of inflammatory mediators
Most common side effects reported include diarrhea, nausea, upper respiratory tract infection and headache
Cutaneous Malignancy
Programmed Death Inhibitor for Refractory Melanoma
On September 4, 2014, pembrolizumab (Keytruda, Merck & Co.,
Inc.) received accelerated FDA approval and is the first programmed death-1 (PD-1) inhibitor in the United States for the treatment of advanced melanoma
The most commonly reported averse events werefatigue, arthralgia, pruritus and rash;immune-mediated adverse events with pembrolizumab
included hyperthyroidism and hypothyroidism (9.4%), pneumonitis (2.9%), colitis (1%), nephritis (0.7%), hepatitis (0.5%) and hypophysitis (0.5%).
Smoothened Inhibitors for Treatment of Advanced Basal Cell Carcinoma

FDA Mandates Black Box Warning for Sunlamp Products
On May 29, 2014, the FDA reclassified sunlamp products (including tanning beds and booths) and ultraviolet (UV) lamps from low-risk (Class I) to moderate-risk (Class II) devices

Systemic Propranolol for Infantile Hemangiomas
The FDA approved propranolol hydrochloride (Hemangiol, Pierre Fabre Dermatologie) in March 2014
Based on the trial, the most effective dose was 3 mg/kg/day using twice-daily dosing.49 Previous consensus reports recommended treatment with propranolol 1 to 3 mg/kg/day divided into 3 times a day dosing with a minimum of 6 hours between doses.


Anti-Depressant Effects of OnabotulinumtoxinA
A study published in the Journal of Clinical Psychiatry in August 2014 suggested that there may be more benefit to botulinum toxin treatment than meets the eye.58 A randomized, double-blind, placebo-controlled trial demonstrated that patients receiving onabotulinumtoxinA (Botox, Allergan) in the glabellar region had statistically significant improvement in depressive symptoms compared to placebo, based on the 21-item Hamilton Depression Rating Scale (HDRS-21). HDRS-21 scores decreased by 46% and 35% in the first and second treatment groups, respectively, versus a 2% drop in the placebo group (P< .0001). The improvement in major depressive disorder symptoms was sustained over 24 weeks, even after the cosmetics effects had worn off around 12 to 16 weeks

Topical Botulinum Toxin Type A in Phase III Trials
A topical gel formulation of botulinum toxin (RT001, Revance Therapeutics) is undergoing Phase III trials in the United States for the treatment of lateral canthal lines (commonly referred to as crow’s feet). RT001 has the potential to be the first approved non-injectable botulinum toxin product. This topical formulation will be used to treat wrinkles caused by superficial muscle groups.59 Deeper muscles, like those in the glabellar area, will likely continue to require injectable botulinum toxin for best outcomes. The topical botulinum toxin will also be aimed at treatment of hyperhidrosis. A second product formulated by the same company, RTOO2, is a novel injectable formulation of botulinum toxin type A targeted toward longer lasting effects when compared with currently available toxins

Omalizumab for Treatment of Urticaria
an anti-IgE receptor antibody, was approved earlier this year for treatment of chronic idiopathic urticaria
Omalizumab 300 mg administered subcutaneously every 4 weeks


JAK Inhibitors for Treatment of Alopecia Areata
In a letter to the editor in the Journal of Investigative Dermatology in June 2014, a team of researchers reported a case of reversal of hair loss in a patient with alopecia universalis taking toficitinib citrate (Xeljanz, Pfizer, Inc.), a Janus kinase (JAK) inhibitor, for treatment of plaque psoriasis.63 Researchers at Columbia University Medical Center later published data related to the identification of key immune mediators related to the JAK pathway that are thought to be involved in the destruction of hair follicles by T cells in patients with alopecia areata.64 They additionally reported a small study of 3 patients with alopecia areata treated with the JAK inhibitor ruxolitinib (Jakafi, Incyte Corporation) who had significant regrowth of hair over 5 months. This is an exciting discovery in the field of hair loss, and further studies are underway to delineate the clinical and pathophysiologic role JAK inhibitors play in alopecia areata.

Sirolimus, also known as rapamycin (SRL, Rapamune®)
potent immunosuppressant, anti-angiogenic and anti-proliferative properties
Skin Cancer in Solid Organ Transplantation
Kaposi’s Sarcoma
Cutaneous T-Cell Lymphomas
Tuberous Sclerosis
Pachyonychia Congenita Psoriasis
Graft Versus Host Disease (GVHD)
Anti-Aging






Thank you Good luck