Dento-alveolar Infections2... · Ƀlactum antibiotics Combinations of amoxicillin with clavuonic...
49
Dento-alveolar Infections Ass. Prof. Dr/ Hamed Gad
Transcript of Dento-alveolar Infections2... · Ƀlactum antibiotics Combinations of amoxicillin with clavuonic...
Dento-alveolar
Infections
Ass Prof Dr Hamed Gad
USE OF BACTERICIDAL
RATHER THAN
BACTERIOSTATIC ANTIBIOTIC
Advantages of bactericidal antibiotics are
1 Less reliance on host resistance
2 Killing of bacteria by antibiotic itself
3 Greater flexibility with dosage intervals
4 Faster results than bacteriostatic
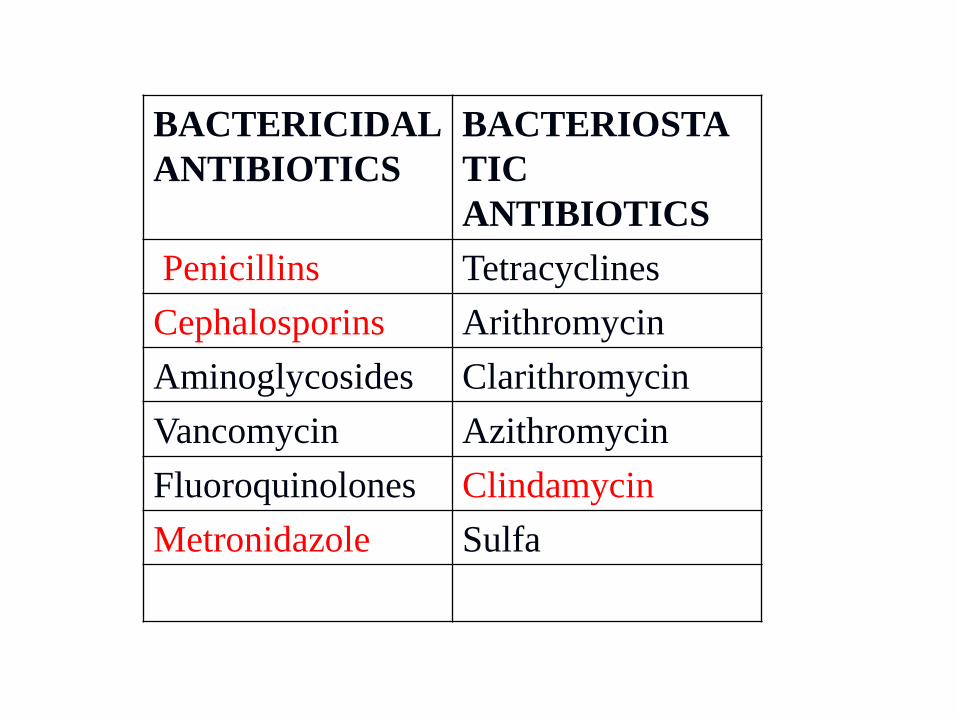
BACTERICIDAL
ANTIBIOTICS
BACTERIOSTA
TIC
ANTIBIOTICS
Penicillins Tetracyclines
Cephalosporins Arithromycin
Aminoglycosides Clarithromycin
Vancomycin Azithromycin
Fluoroquinolones Clindamycin
Metronidazole Sulfa
Ƀ lactum antibiotics
Penicillin
it is considered an antibiotic of choice for the treatment of
odontogenic infections
Penicillin inhibits synthesis of the cell wall
The semisynthetic derivatives(amoxicillin- ampicillen) is
effective against
aerobic Gram-positive rods
Gram negative amp Gram-positive cocci
combinations of semisynthetic penicillins
with various 1048642 -lactamase inhibitors
1Ampicillin with sulbactam
2 Amoxicillin with clavulanic acid
Ƀ lactum antibiotics
Ƀ lactum antibiotics
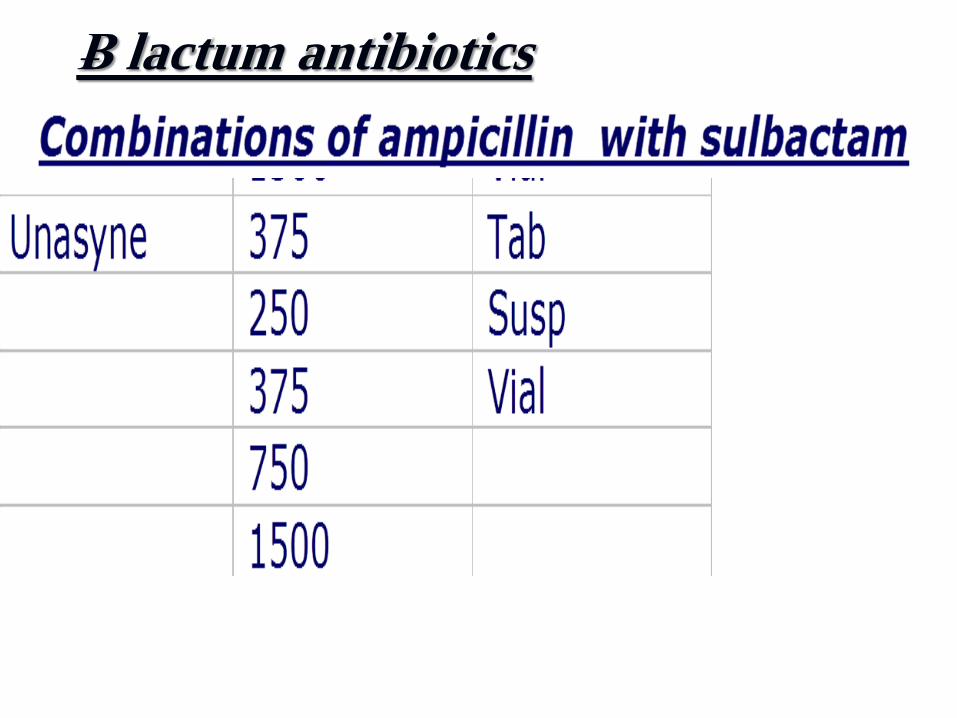
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
USE OF BACTERICIDAL
RATHER THAN
BACTERIOSTATIC ANTIBIOTIC
Advantages of bactericidal antibiotics are
1 Less reliance on host resistance
2 Killing of bacteria by antibiotic itself
3 Greater flexibility with dosage intervals
4 Faster results than bacteriostatic
BACTERICIDAL
ANTIBIOTICS
BACTERIOSTA
TIC
ANTIBIOTICS
Penicillins Tetracyclines
Cephalosporins Arithromycin
Aminoglycosides Clarithromycin
Vancomycin Azithromycin
Fluoroquinolones Clindamycin
Metronidazole Sulfa
Ƀ lactum antibiotics
Penicillin
it is considered an antibiotic of choice for the treatment of
odontogenic infections
Penicillin inhibits synthesis of the cell wall
The semisynthetic derivatives(amoxicillin- ampicillen) is
effective against
aerobic Gram-positive rods
Gram negative amp Gram-positive cocci
combinations of semisynthetic penicillins
with various 1048642 -lactamase inhibitors
1Ampicillin with sulbactam
2 Amoxicillin with clavulanic acid
Ƀ lactum antibiotics
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
BACTERICIDAL
ANTIBIOTICS
BACTERIOSTA
TIC
ANTIBIOTICS
Penicillins Tetracyclines
Cephalosporins Arithromycin
Aminoglycosides Clarithromycin
Vancomycin Azithromycin
Fluoroquinolones Clindamycin
Metronidazole Sulfa
Ƀ lactum antibiotics
Penicillin
it is considered an antibiotic of choice for the treatment of
odontogenic infections
Penicillin inhibits synthesis of the cell wall
The semisynthetic derivatives(amoxicillin- ampicillen) is
effective against
aerobic Gram-positive rods
Gram negative amp Gram-positive cocci
combinations of semisynthetic penicillins
with various 1048642 -lactamase inhibitors
1Ampicillin with sulbactam
2 Amoxicillin with clavulanic acid
Ƀ lactum antibiotics
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Ƀ lactum antibiotics
Penicillin
it is considered an antibiotic of choice for the treatment of
odontogenic infections
Penicillin inhibits synthesis of the cell wall
The semisynthetic derivatives(amoxicillin- ampicillen) is
effective against
aerobic Gram-positive rods
Gram negative amp Gram-positive cocci
combinations of semisynthetic penicillins
with various 1048642 -lactamase inhibitors
1Ampicillin with sulbactam
2 Amoxicillin with clavulanic acid
Ƀ lactum antibiotics
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
combinations of semisynthetic penicillins
with various 1048642 -lactamase inhibitors
1Ampicillin with sulbactam
2 Amoxicillin with clavulanic acid
Ƀ lactum antibiotics
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Ƀ lactum antibiotics
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
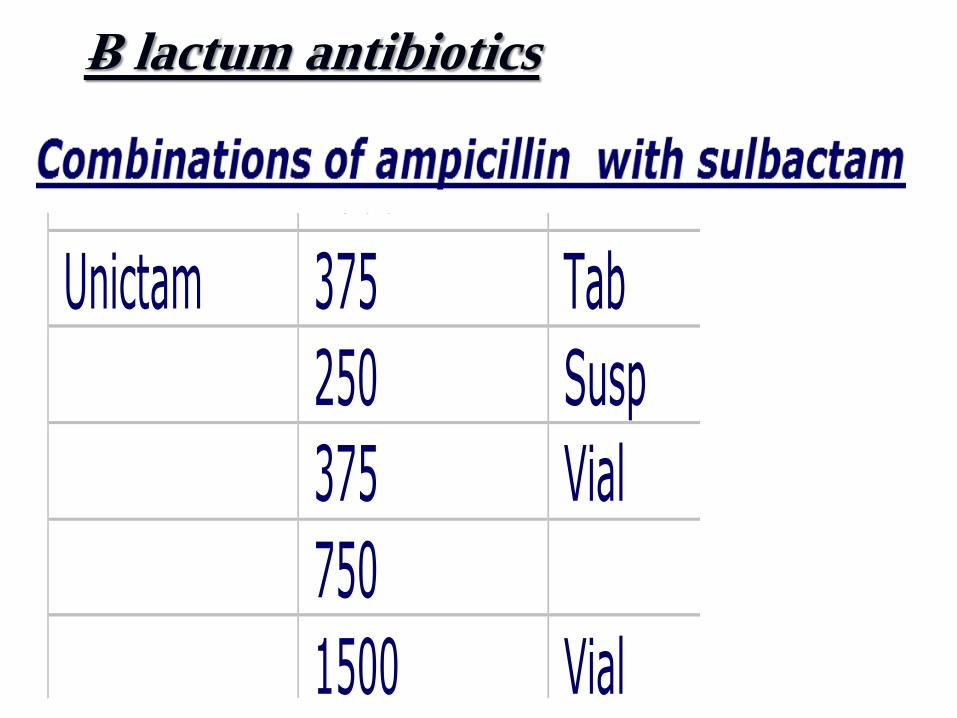
Ƀ lactum antibiotics
Combinations of ampicillin with sulbactam
Sulbin 375 Vial 400
750 650
1500 925
Unictam 375 Tab 30
250 Susp 21
375 Vial 375
750 600
1500 Vial 11
Unasyne 375 Tab 40
250 Susp 33
375 Vial 800
750 1200
1500 1700
3000 Vial 2400
Others ampictam sigmacyn ultracillin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
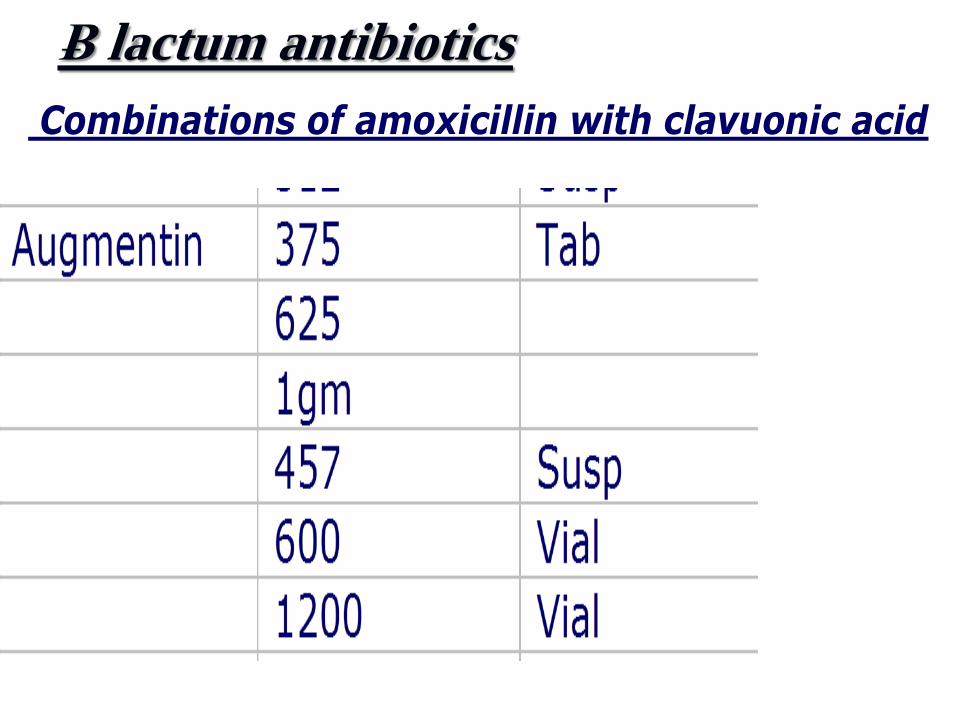
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
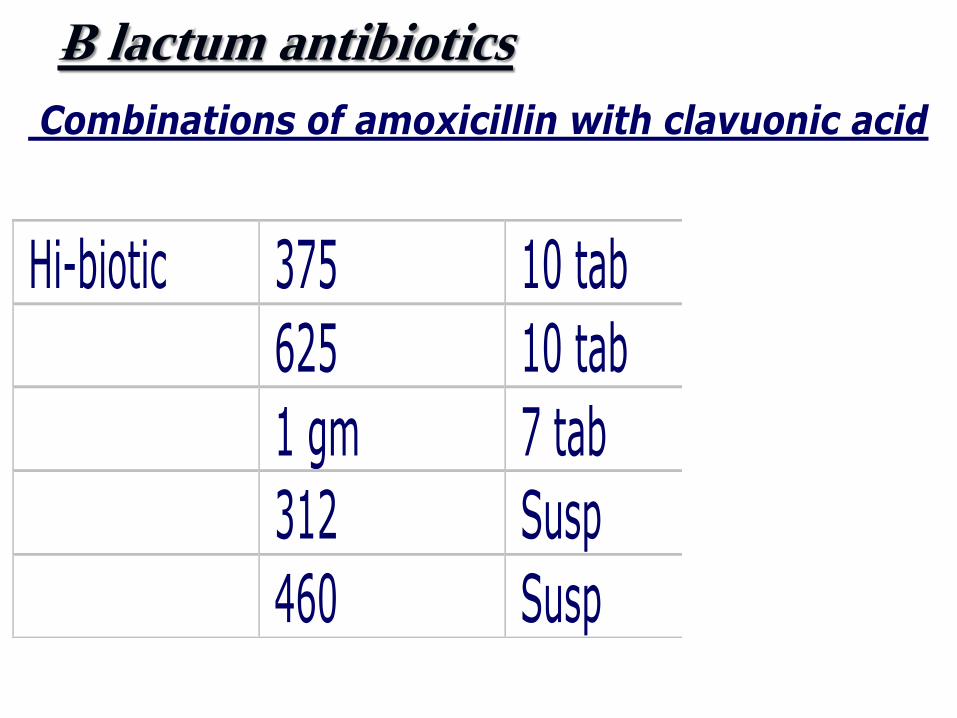
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
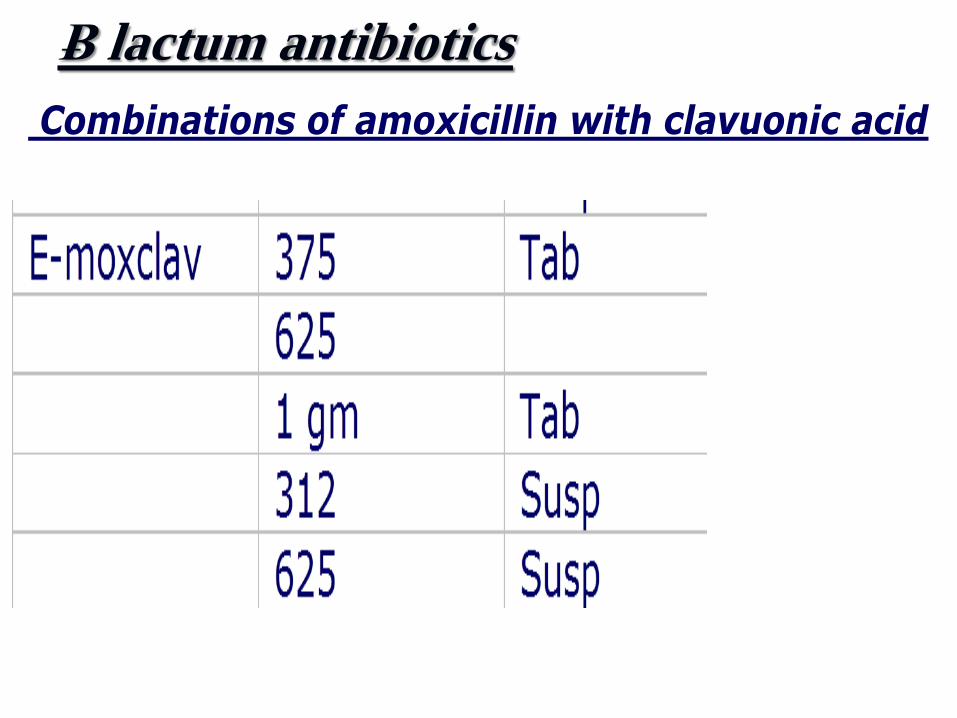
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
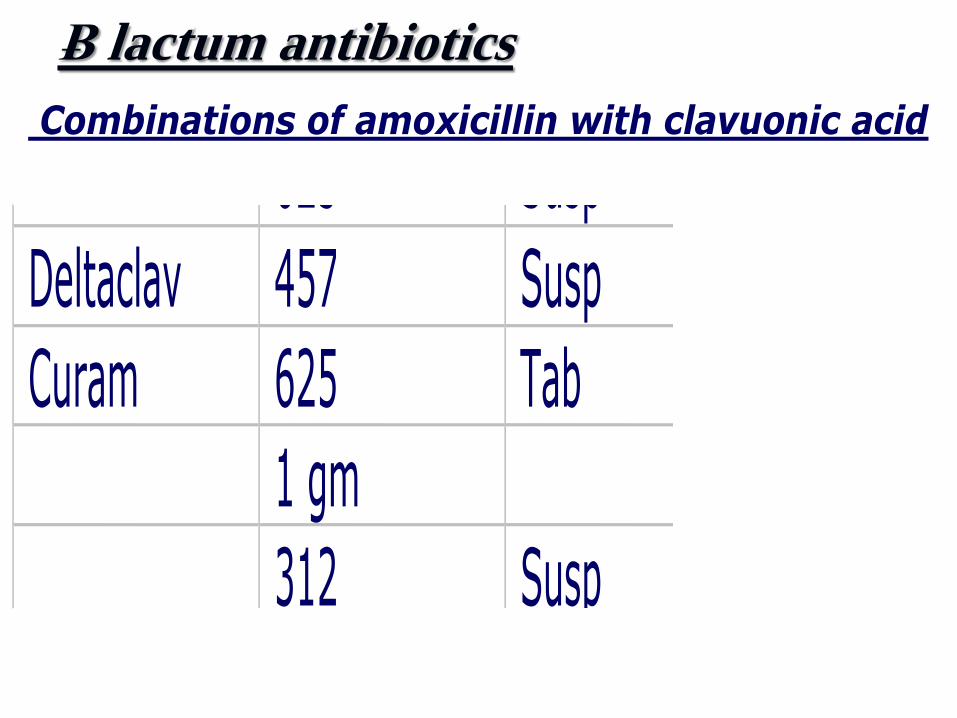
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
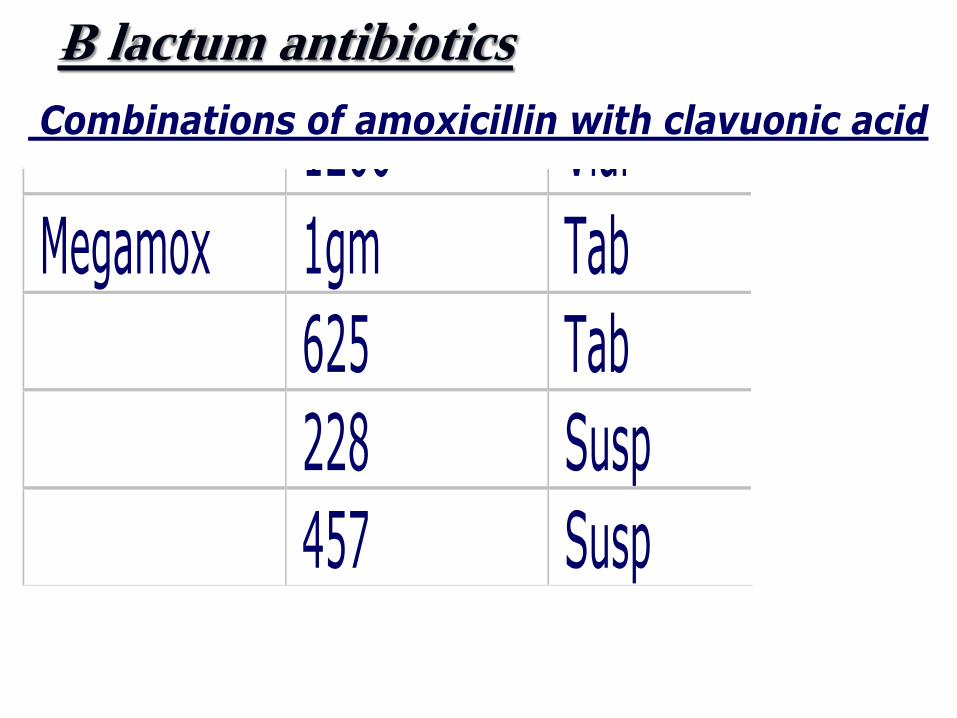
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
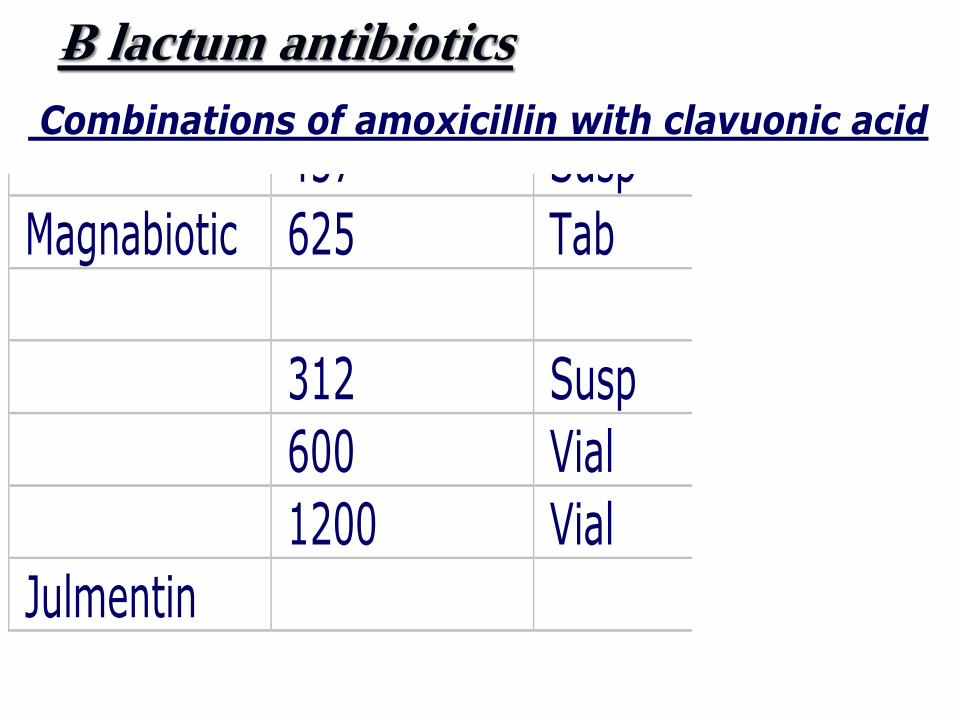
Ƀ lactum antibiotics
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Combinations of amoxicillin with clavuonic acid
Hi-biotic 375 10 tab 2200 amoun
625 10 tab 2600
1 gm 7 tab 2500
312 Susp 1500
460 Susp 2300
E-moxclav 375 Tab 2600 epico
625 3000
1 gm Tab 3300
312 Susp 1800
625 Susp 2400
Deltaclav 457 Susp 1800
Curam 625 Tab 1200
1 gm 1500
312 Susp 2100
Augmentin 375 Tab 3000
625 3500
1gm 5800
457 Susp 3700
600 Vial 115
1200 Vial 2000
Megamox 1gm Tab 50
625 Tab 40
228 Susp 2300
457 Susp 3500
Magnabiotic 625 Tab 200
312 Susp 180
600 Vial 90
1200 Vial 1600
Julmentin
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Cephalosporins
The mechanism of action of cephalosporins regardless of
generation is the same as that of penicillin
Cephalosporins are considered relatively safe drugs during
pregnancy (category B according to FDA categorization) and
their dose needs to be decreased only in case of advanced
renal failure
Ƀ lactum antibiotics
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
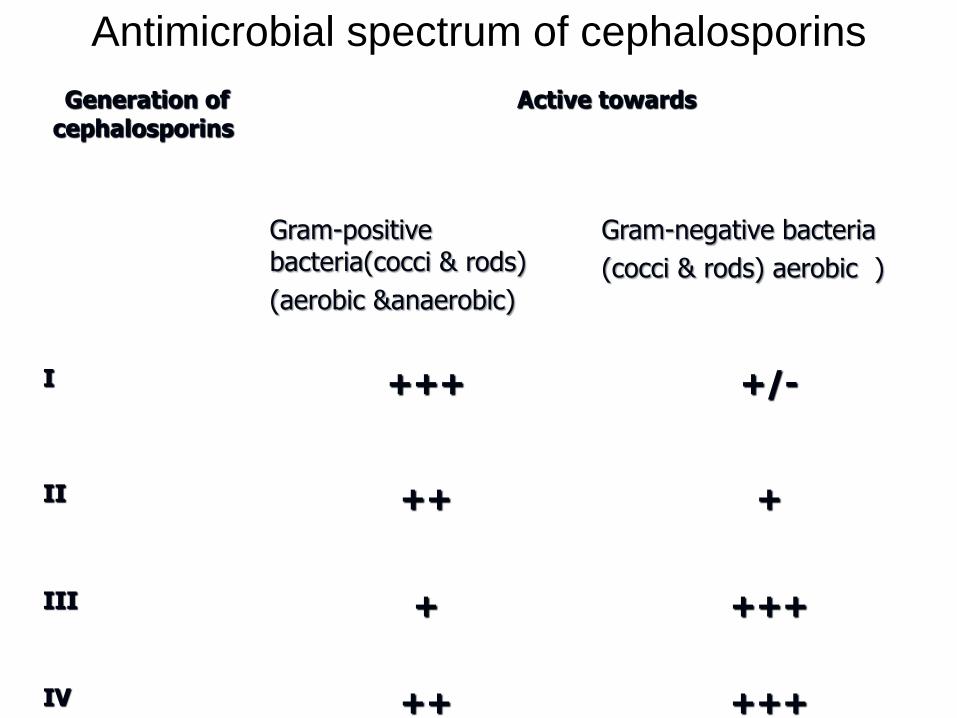
Antimicrobial spectrum of cephalosporins
Generation of cephalosporins
Active towards
Gram-positive bacteria(cocci amp rods)
(aerobic ampanaerobic)
Gram-negative bacteria
(cocci amp rods) aerobic )
І +++ +-
ІІ
++ +
ІІІ
+ +++
ІV ++ +++
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
First generation
Similar to penicillinase-resistant
penicillins with greater gram-
negative coverage
Used for
community-acquired infections
mild to moderate infections
Not penetrate CNS
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Ƀ lactum antibiotics
First generation
1- cephalexin
2- cefadroxil
3- cephradine
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
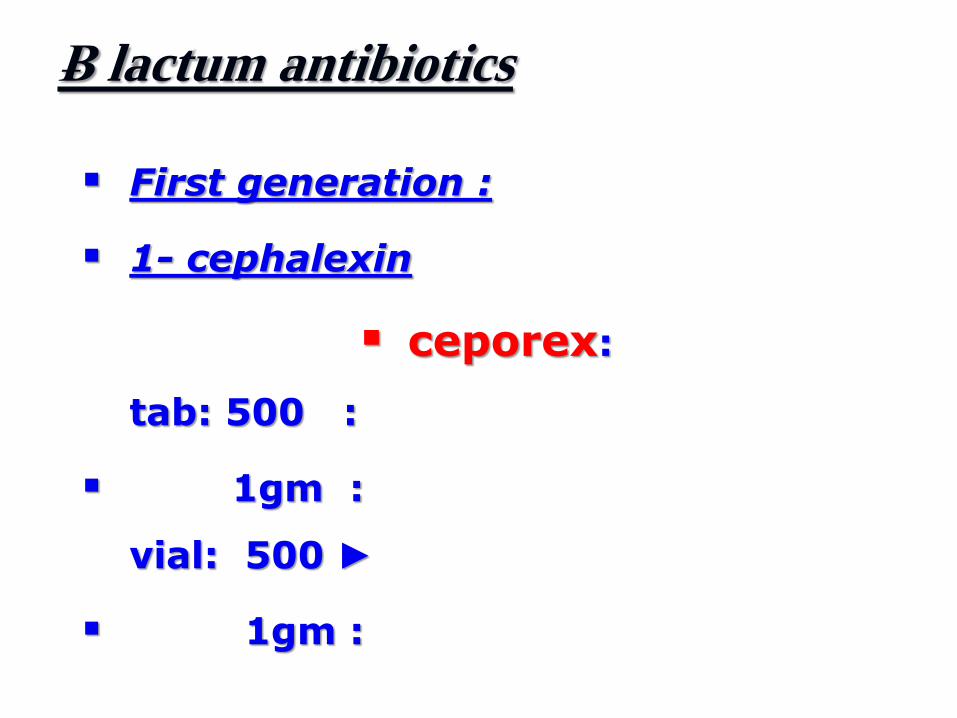
Ƀ lactum antibiotics
First generation
1- cephalexin
ceporex
tab 500
1gm
vial 500
1gm
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
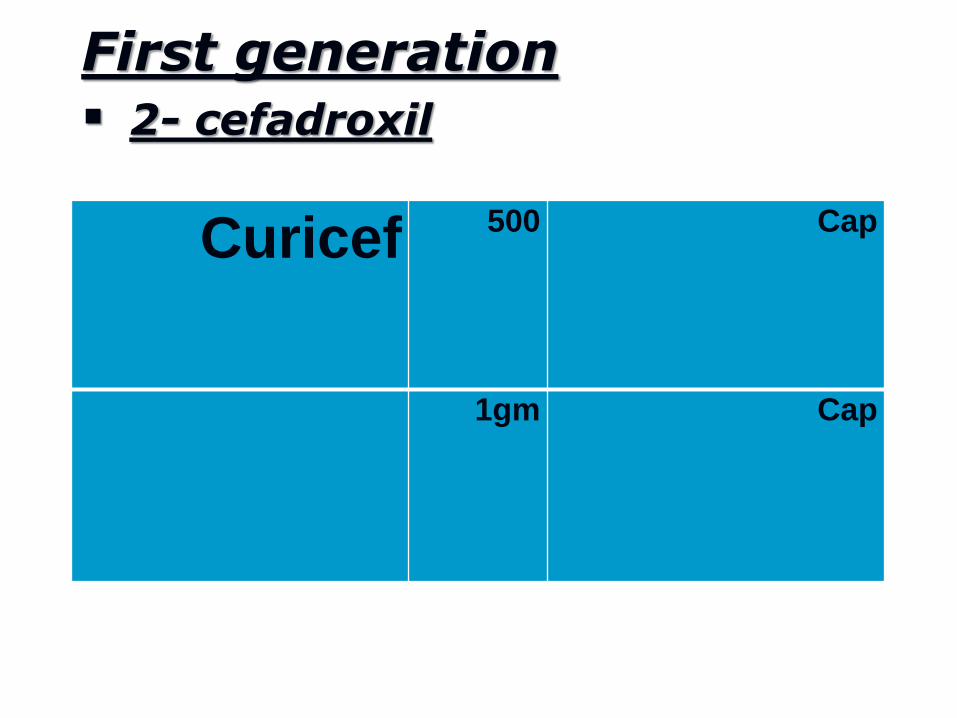
First generation
2- cefadroxil
Curicef 500 Cap
1gm Cap
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
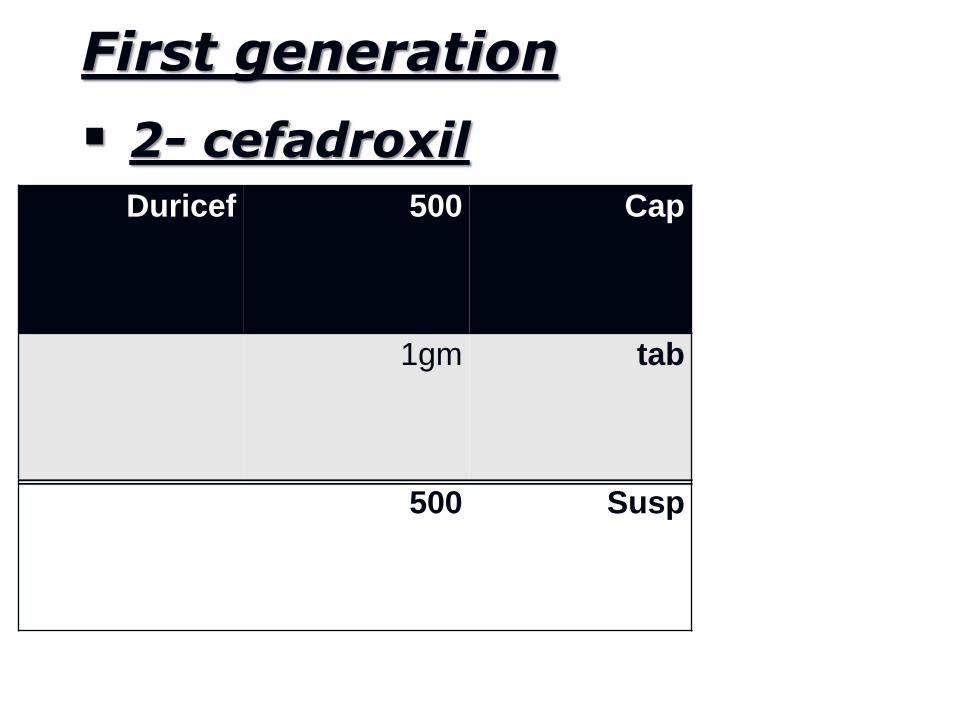
First generation
2- cefadroxil
Duricef 500 Cap
1gm tab
500 Susp
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
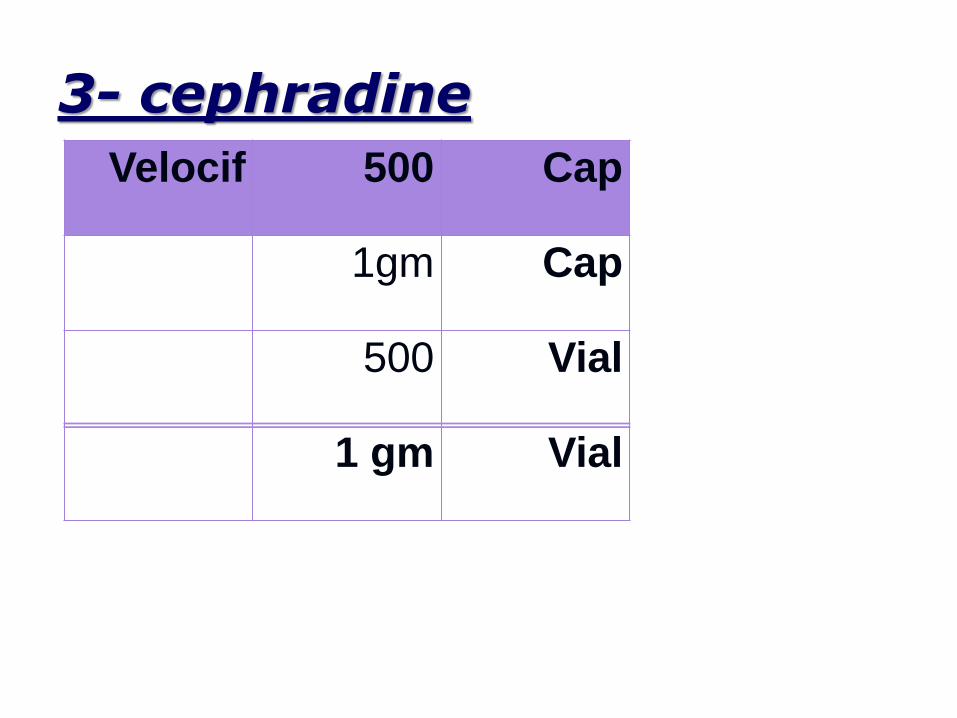
3- cephradine
Velocif 500 Cap
1gm Cap
500 Vial
1 gm Vial
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Third generation HIGLY Active toward aerobic gr ndashve
rods
1-Cefotaxime
2- cefoperazne sodium
3- ceftriaxone
ceftazidime (Fortum)
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
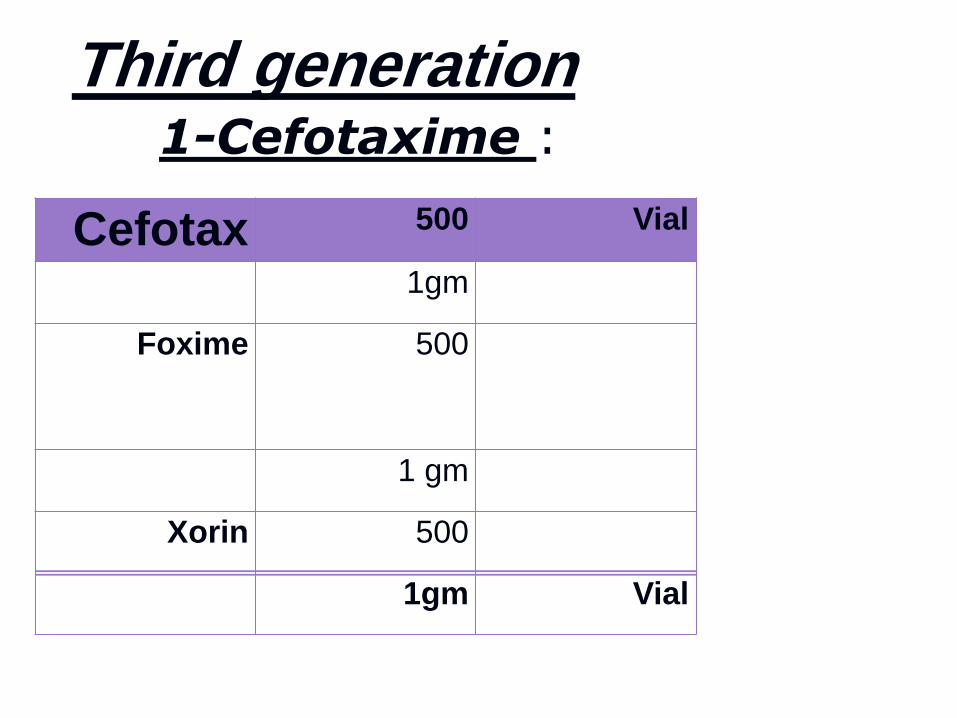
Cefotax 500 Vial
1gm
Foxime 500
1 gm
Xorin 500
1gm Vial
1-Cefotaxime
Third generation
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
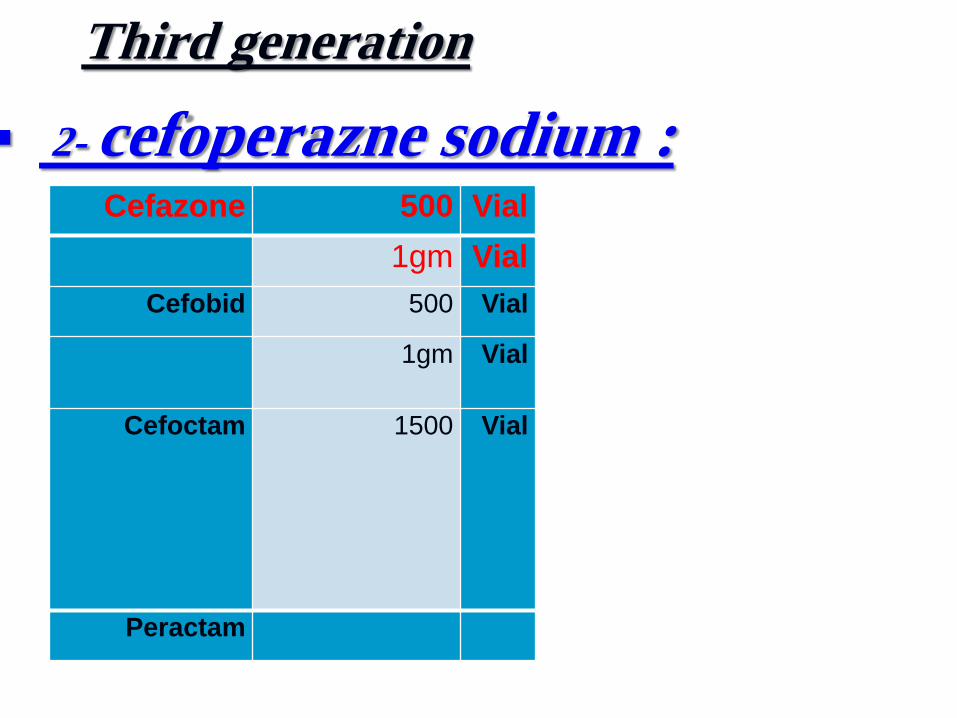
Third generation
2- cefoperazne sodium
Cefazone 500 Vial
1gm Vial
Cefobid 500 Vial
1gm Vial
Cefoctam 1500 Vial
Peractam
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
bull
Third Generation 3- ceftriaxone
IV and IM long half-life once-a-day dosing
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
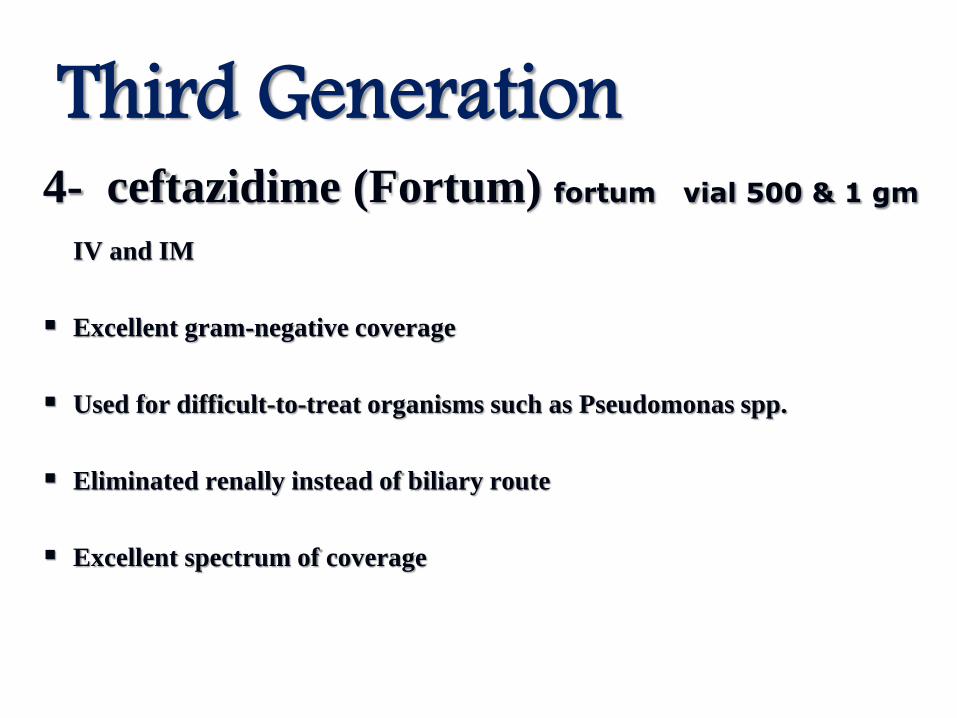
Third Generation 4- ceftazidime (Fortum) fortum vial 500 amp 1 gm
IV and IM
Excellent gram-negative coverage
Used for difficult-to-treat organisms such as Pseudomonas spp
Eliminated renally instead of biliary route
Excellent spectrum of coverage
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Macrolides
Their antimicrobial spectrum includes
Gram-positive aerobic and anaerobic
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
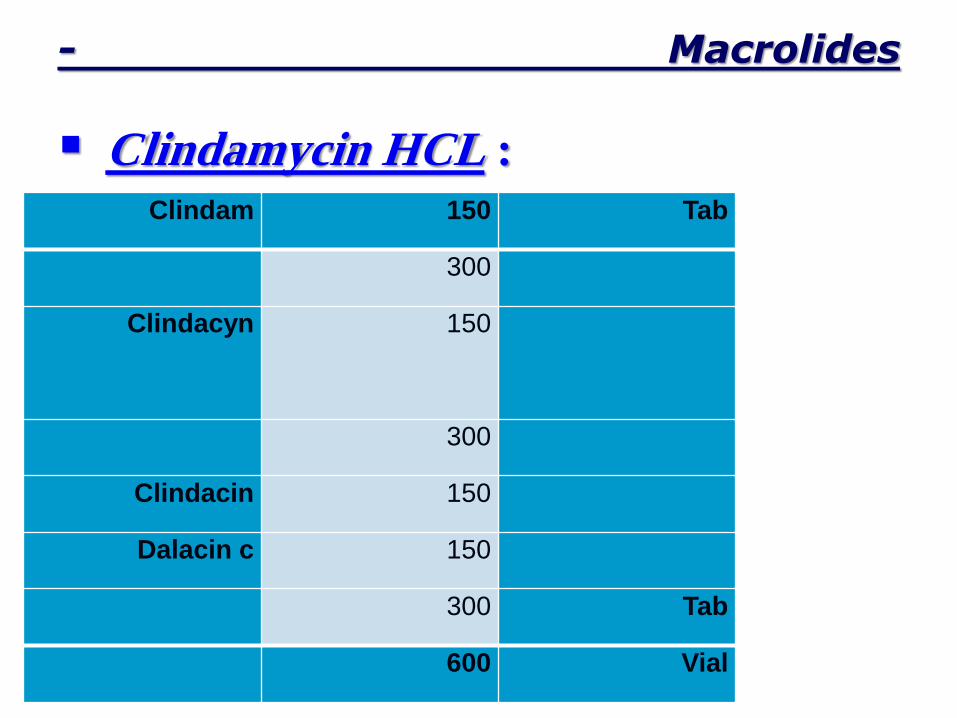
- Macrolides
Clindamycin HCL
Clindam 150 Tab
300
Clindacyn 150
300
Clindacin 150
Dalacin c 150
300 Tab
600 Vial
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
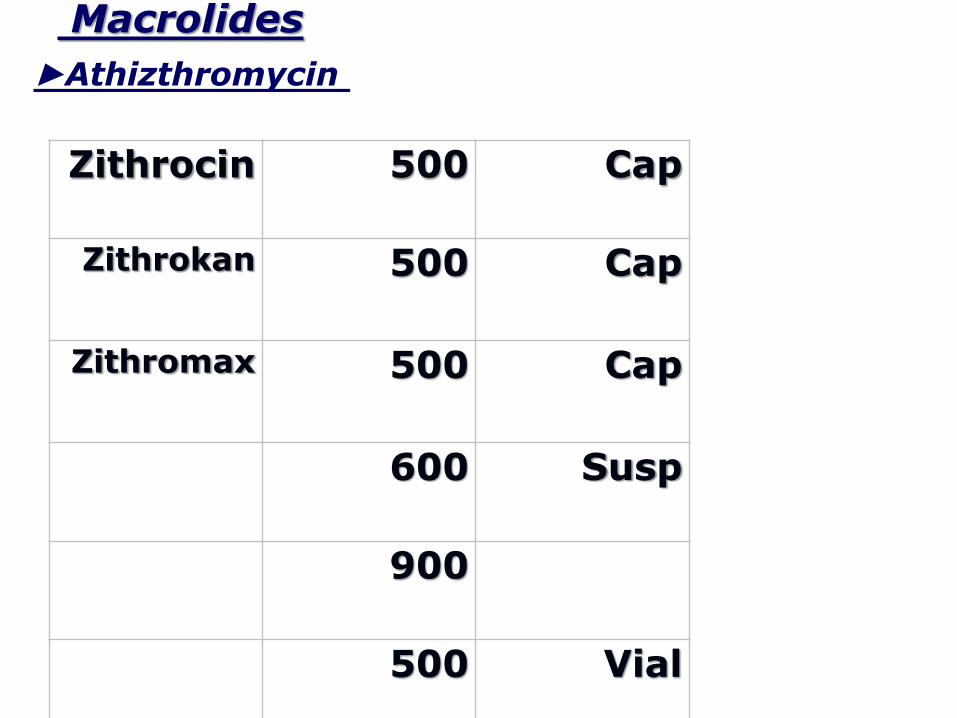
Macrolides
Zithrocin 500 Cap
Zithrokan 500 Cap
Zithromax 500 Cap
600 Susp
900
500 Vial
Athizthromycin
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Metronidazole They are drugs with rapid bactericidal action
principally against
Gram-negative and +ve anaerobes
The usual dose for oral administration is 500 mg
every 8 h
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
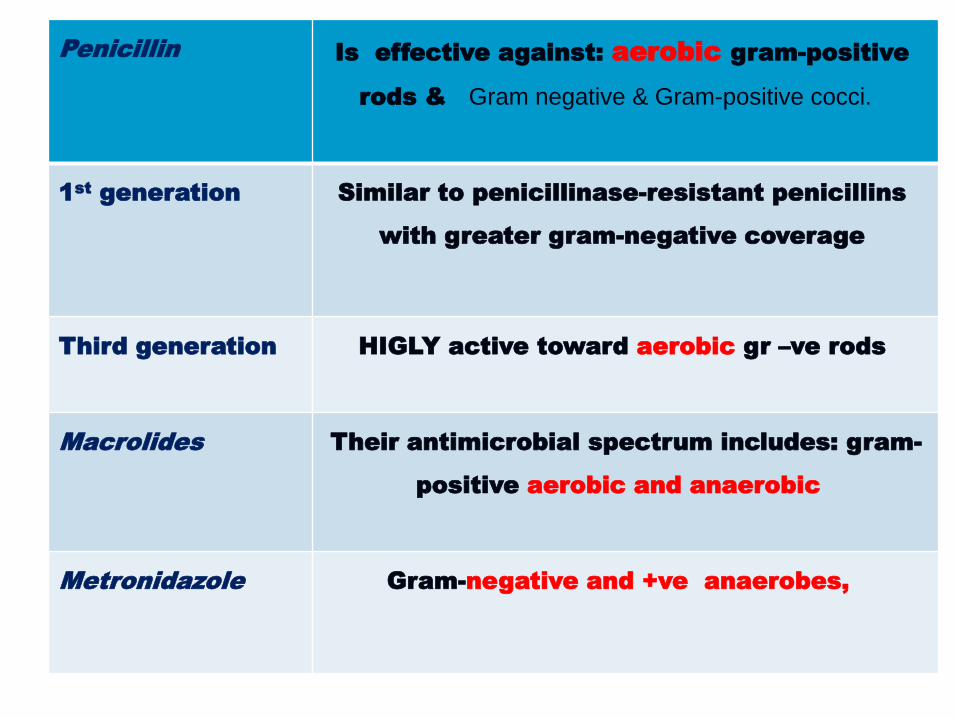
Penicillin Is effective against aerobic gram-positive
rods amp Gram negative amp Gram-positive cocci
1st
generation Similar to penicillinase-resistant penicillins
with greater gram-negative coverage
Third generation HIGLY active toward aerobic gr ndashve rods
Macrolides
Their antimicrobial spectrum includes gram-
positive aerobic and anaerobic
Metronidazole Gram-negative and +ve anaerobes
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Home massage for antibiotic
therapy Removal of the cause drainage and
supportive care more important than
antibiotic therapy
Infections are cured by the patientrsquos
defenses not antibiotics
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
What is the antibiotic of choice for
treatment of odontogenic infection
1 penicillin or cephalosporine plus metronidazole
2 clindamycin is an excellent alternative plus
metronidazole
3 Erythromycin
---------------------------------------------------
1 Definitive antibiotic therapy should be based on
culture and sensitivity
2 Antibiotics should be prescribed for at least one
week
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
III
H- EVALUATE THE PATIENT
FREQUENTLY
1 Subjective sense of feeling better
2 Objective signs of improvement
3 Review culture amp sensitivity reports
4 Re-evaluate host responses if
necessary
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Lower premolars
Sublingual space Submandibular
space Lateral pharyngeal
space Retropharyngeal space
Superior mediastinum
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
Complications of odontogenic
infections
Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU

Orbital cellulitis and blindness
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
- Ludwigs angina
Ludwigs angina is bilateral
brawny induration of the
submandibular sublingual
and submental spaces
The term angina is used because
of the respiratory distress
caused by the airway
obstruction
The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU

The incisions must be bilateral
extraoral parallel and
medial to the inferior border
of the mandible at the
premolar and molar region
and intraoral parallel to the
ducts of the submandibular
glands
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
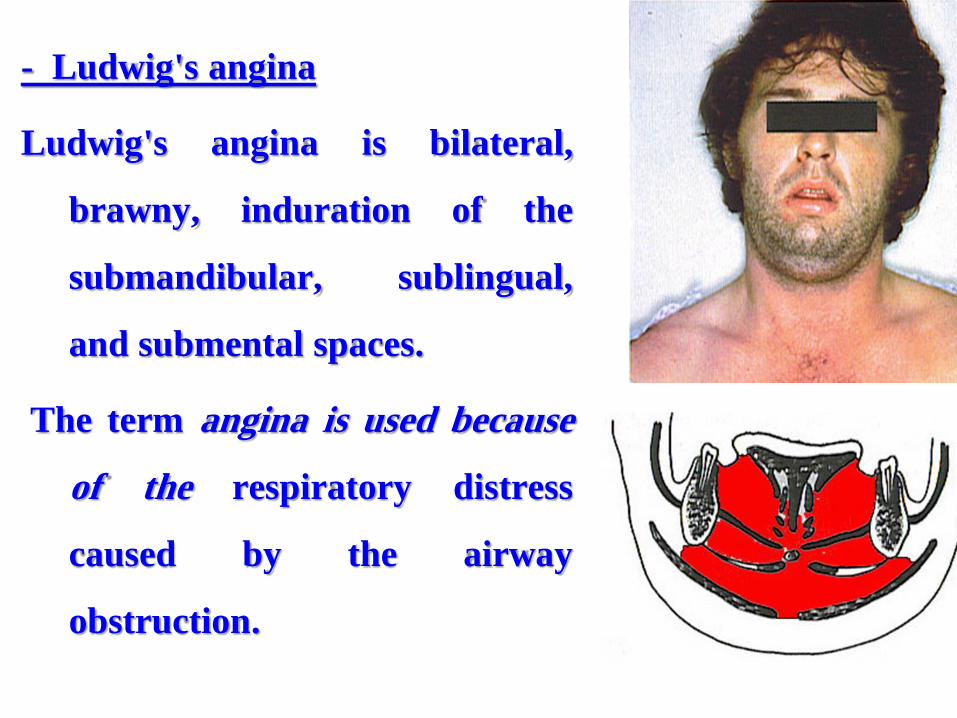
It is an uncommon but potentially
lethal extension of odontogenic
infection
An orofacial infection can reach the
cavernous sinus through two
routes
1 an anterior route via the angular
and inferior ophthalmic veins and
2 posterior route via the transverse
facial vein and the pterygoid
plexus of veins
- Cavernous sinus thrombosis
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
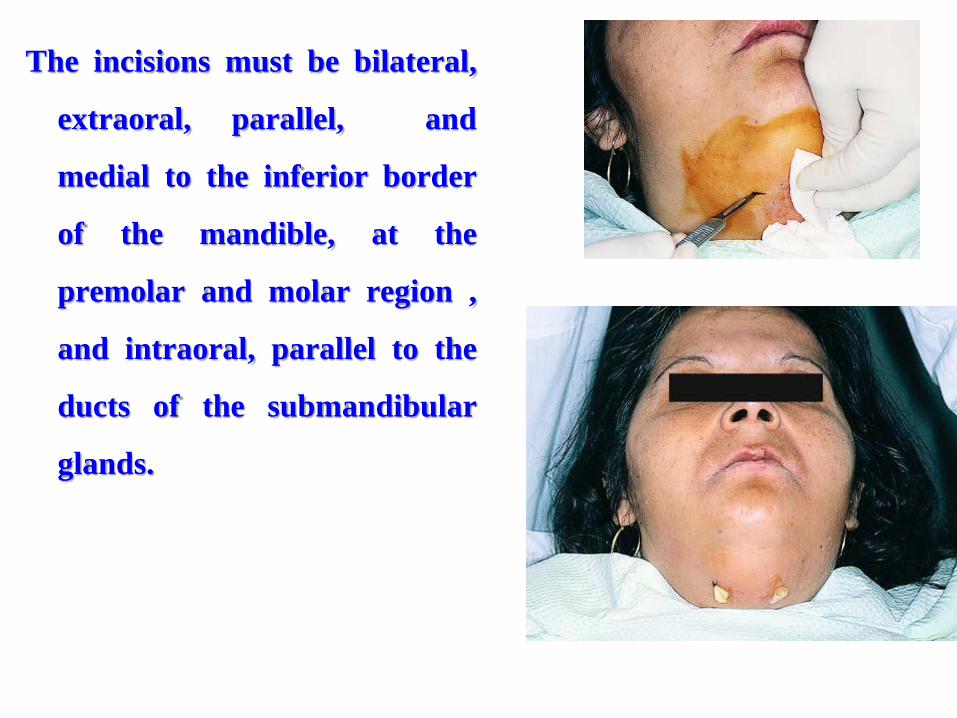
Cavernous sinus thrombosis
The first clinical signs of cavernous sinus
thrombosis include vascular congestion in
periorbital scleral and retinal veins
Other clinical signs include periorbital edema
proptosis thrombosis of the retinal vein dilated
pupils absent corneal reflex and supraorbital
sensory deficits
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
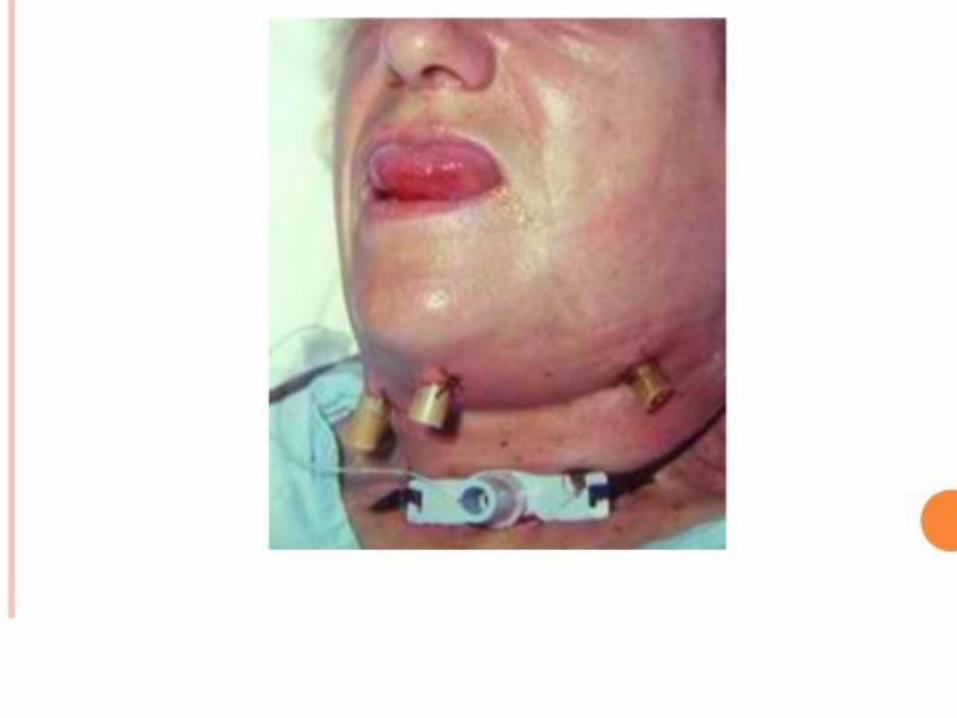
3- Cervicofacial
necrotizing fasciitis
Cervicofacial necrotizing fasciitis is a
very aggressive infection of the skin and
superficial fascia of the head and neck
and is commonly seen in diabetic and
immunocompromised patients
It carries a mortality rate of 30-50
from sepsis of the dead tissue in the
affected area
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
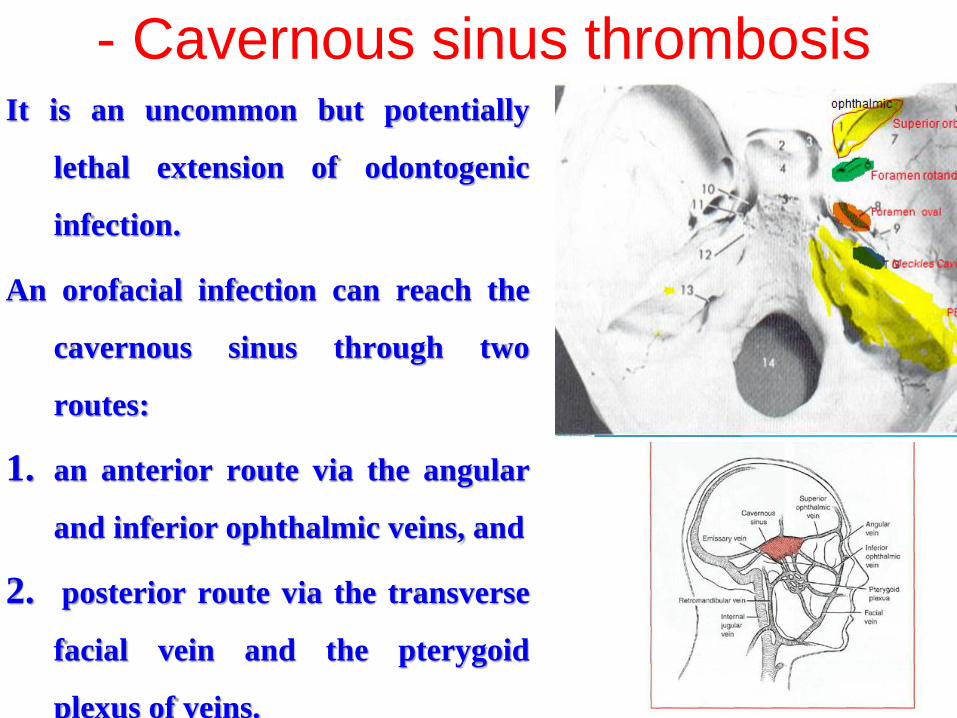
Necrotizing fasciitis Large granulating skin defect extending from the inferior border of the mandible to the clavicle 2 weeks After deacutebridement
4- pulmonary
abscess
THANK YOU
THANK YOU
4- pulmonary
abscess
THANK YOU
THANK YOU
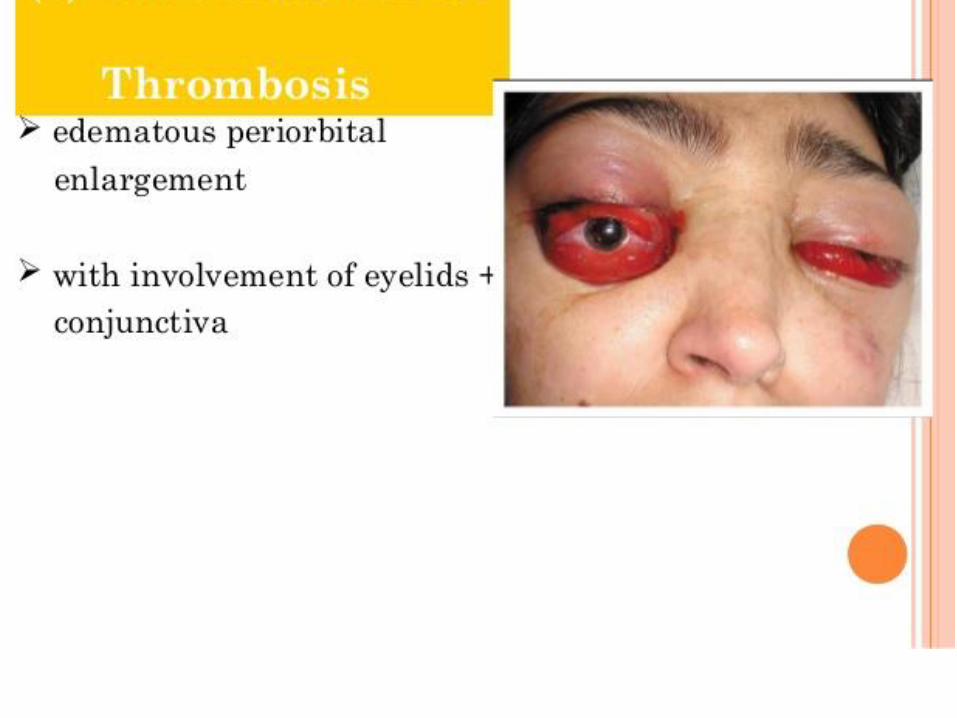
THANK YOU
THANK YOU