
Dentistry by the Numbers Claims Data Analysis & Risk-Reduction …2015... · Dentistry by the...
47
Dentistry by the Numbers Claims Data Analysis & Risk-Reduction Solutions
-
Upload
nguyendieu -
Category
Documents
-
view
216 -
download
3
Transcript of Dentistry by the Numbers Claims Data Analysis & Risk-Reduction …2015... · Dentistry by the...

Dentistry by the NumbersClaims Data Analysis & Risk-Reduction Solutions

2
Today’s moderator
Rachel is a graduate of Ball State University with a bachelor of science degree innursing, and she earned a master of science degree in nursing administration fromIndiana University. Rachel is a member of the American Society for Healthcare RiskManagement and the Indiana Society for Healthcare Risk Management.
Today’s moderator is Rachel Rosen, RN, MSN, AVP, MedProGroup ([email protected])
Rachel has more than 20 years of experience in patientsafety, quality, and risk management — both as an internalleader and as an external consultant.
Her healthcare industry customers have included multi-hospital systems, large acute care hospitals, long-term acutecare facilities, critical access hospitals, healthcare services,and managed care organizations.
Rachel has extensive experience in standards preparation and compliance, strategicorganizational improvement planning and implementation, quality measurement,patient satisfaction, and medical staff quality and peer review.

3
Are you aware of our vast resources?

4
Join us on Twitter
Join us on Twitter @MedProProtector!
Risk management and patient safety informationdelivered in a convenient, flexible format
Not on Twitter? Give It a Try!
Twitter is an easy, quick way to staycurrent with healthcare news andtrends, receive information andresources, connect with individualsand organizations, and receive riskmanagement info from MedPro!Opening an account is simple —visit www.twitter.com.
Articles Tools
Announcements Case studies
Resources Risk Q&A
Videos And more!

5
Designation of continuing education credit
The Medical Protective Company is designated as anApproved PACE Program Provider by the Academy ofGeneral Dentistry. The formal continuing dental educationprograms of this program provider are accepted by AGDfor Fellowship/Mastership and membership maintenancecredit. Approval does not imply acceptance by a state orprovincial board of dentistry or AGD endorsement. Thecurrent term of approval extends from October 1, 2015,to September 30, 2018. Provider ID 218784.
The Medical Protective Company designates thiscontinuing education activity as meeting the criteria forup to 1 hour of continuing education credit. Doctorsshould claim only those hours actually spent in theactivity.

6
Disclosure
Medical Protective receives no commercial support frompharmaceutical companies, biomedical device manufacturers, orany commercial interest.
It is the policy of Medical Protective to require that all parties ina position to influence the content of this activity disclose theexistence of any relevant financial relationship with anycommercial interest.
When there are relevant financial relationships, the individual(s)will be listed by name, along with the name of the commercialinterest with which the person has a relationship and the natureof the relationship.
Today's faculty, as well as CE planners, content developers,reviewers, editors, and Patient Safety & Risk Solutions staff atMedical Protective have reported that they have no relevantfinancial relationships with any commercial interests.
7
Objectives
At the conclusion of this presentation, participantsshould be able to:
• Review dental claims data to identify the leadingfactors involved in these claims
• Identify the most common reasons dentists callMedPro for risk management advice
• Develop strategies to address issues identified inclaims and telephone consultations
• Discuss how the risk factors identified inclaims and telephone consultations canaffect evolving claim trends and claimsdefense

8
Registration Polling Results
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Have policy toterminate pt
Use "teach-back"
Use CustomerSatisfaction
survey
Incorporatepatient
feedback
Policy &procedure for
refunds
Does ICprocess includediscussion w/pt
Do youdocument ICdiscussion
Seek tounderstand pt's
expectations
Yes No N/A
9
Today’s program
In addition to his academic credentials, Ted has been trained in healthcare mediation andconflict resolution by the Harvard School of Public Health, and clinician–patient communicationby the Institute for Healthcare Communication. His affiliations include Adjunct Professor ofMedical Law at the Thomas M. Cooley Law School, advisory panel member for a physicianlitigation stress website, and former board member of the Tri-County Medical Control Authority.
Today’s speaker is Theodore (Ted) Passineau, JD, HRM,RPLU, CPHRM, FASHRM, Senior Patient Safety & RiskConsultant, MedPro Group([email protected])
Ted provides risk management services for the upper Midwest andNortheast regions. He has worked in the field of medical professionalliability since 1987.
Ted’s professional achievements include experience as a medicalmalpractice defense attorney, risk management consultant, directorof risk management, and director of continuing medical education forboth doctor-owned and commercial professional liability insurers.
In his career, Ted has provided instruction to thousands of physicians, dentists, and hospitalstaffs across the United States and internationally, and he has written extensively on variousprofessional liability-related topics.

10
Today’s program
Today’s speaker is Russ Pride, MA, CPHRM, Healthcare RiskConsultant, MedPro Group ([email protected] )
Patient safety and clinical risk management have been the primary focus ofRuss’ career for the past 25 years. He has worked as a healthcare riskconsultant for Princeton Insurance (part of MedPro Group) for 17 years. Russprovides comprehensive risk management services in New Jersey and New Yorkfor physician practices, hospital systems, and professional healthcareorganizations.
Russ is an approved facilitator of Institute for Healthcare Communication workshops, focusing particularly onprovider-patient communication in the emergency department. He earned a master’s degree in psychologyfrom LaSalle University, has clinical experience as a behavioral therapist, and is a certified hypnotherapist bythe International Medical and Dental Hypnotherapy Association. An advocate for effective communication asthe cornerstone for promoting safer patient care, Russ provides workshops focusing on key issues such asinformed consent, patient compliance, difficult relationships, the impact of social media, patient satisfaction,and more.
Russ is a certified professional in healthcare risk management (CPHRM) through the American HospitalAssociation. He earned his certificate in healthcare risk management through the New England HealthcareAssembly (Boston, MA) and is a chapter member of the Pennsylvania, New York, and New Jersey societiesof healthcare risk managers.
Russ’ previous experience includes serving as a risk manager for an urban acutecare hospital, providing healthcare marketing for hospitals and pharmaceuticalcompanies, and working with a regional health insurer in the areas of qualityassurance, human resources, and corporate administration.

11
General dentistry: claims volume and total paid by allegation type
92%
5% 3%
Treatment-related
Diagnosis-related
Other
Volume of claims by allegation type
• Treatment-related allegations account for the majority of claims and totaldollars incurred.
• Improper performance of treatments/procedures as a specific allegationaccounts for almost three-fourths of the treatment-related dental claims.
Source: MedPro Group claims data, 2003−2012. The “Other” category represents the remainder of the data, in which no onecategory represents a significant individual amount. Total incurred = total dollars paid (indemnity + expense) and reserved on openand closed claims.
86%
14%
Treatment-related
Diagnosis-related
Total dollars incurred by allegation type

12
General dentistry: treatment-related allegations
47%
18%
12%
7%
16%
Dental restoration Root canal
Tooth extraction Fitting of denture
Other
Volume of treatment-related claimsby procedure type
Source: MedPro Group claims data, 2003−2012. The “Other” category represents the remainder of the data, in which no one categoryrepresents a significant individual amount.
Dental restorations and root canals account for two-thirds of all treatment-related claims.Patient dissatisfaction with restoration results tops the complications category. Poorprocedural technique as a risk management issue for treatment-related claims is seen inthe majority of the claims.
Dental restorations and root canals account for two-thirds of all treatment-related claims.Patient dissatisfaction with restoration results tops the complications category. Poorprocedural technique as a risk management issue for treatment-related claims is seen inthe majority of the claims.
52%
18%
15%
6%
5%
4%
Tooth damage Nerve injury
Infection Retained foreign body
Puncture/laceration Other
Injuries in improperly performedtreatments/procedures
13
General dentistry: top risk management issues
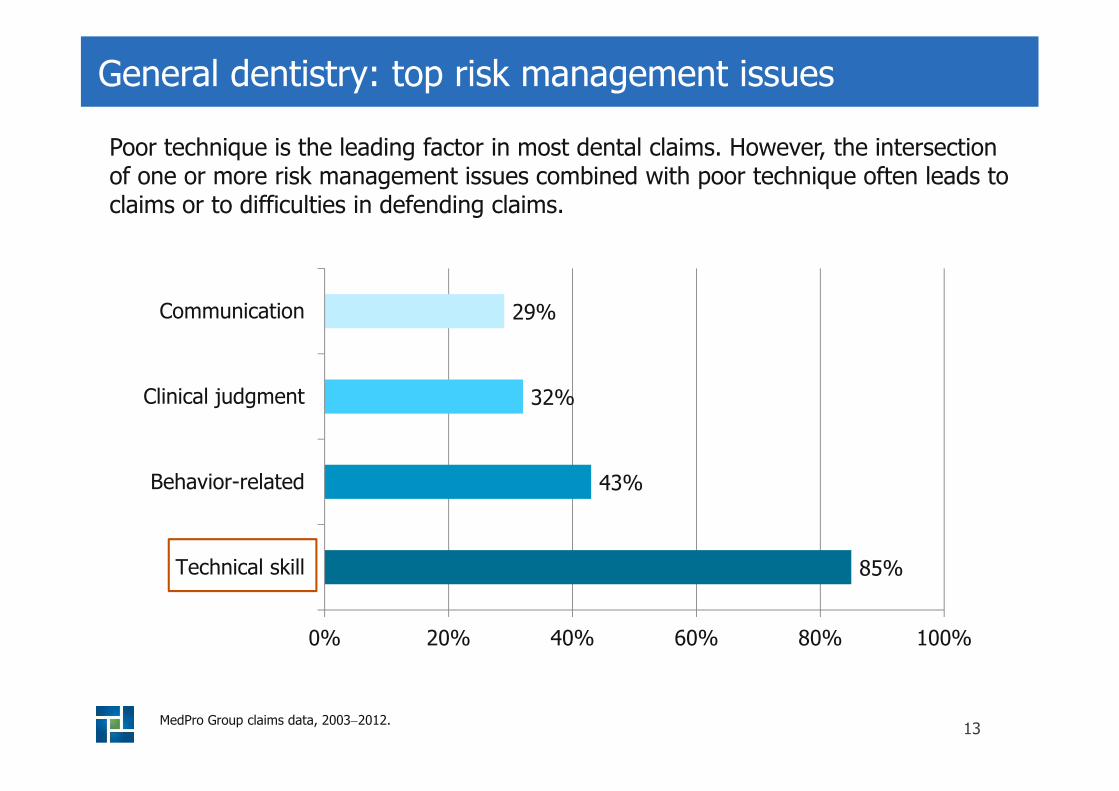
85%
43%
32%
29%
0% 20% 40% 60% 80% 100%
Technical skill
Behavior-related
Clinical judgment
Communication
Poor technique is the leading factor in most dental claims. However, the intersectionof one or more risk management issues combined with poor technique often leads toclaims or to difficulties in defending claims.
MedPro Group claims data, 2003−2012.
14
Technical skill
Three suggestions
Stay currentPay full attention to
each caseIf you want adventure,go climb a mountain

15
Clinical judgment

16
Clinical judgment: critical thinking
• Critical thinking approach in clinical practicehas two goals:
o Accurate problemidentification
o Optimal problemresolution
• Experiencedpractitioners vs.less-experiencedpractitioners
Facione, N., & Facione, P. (2008). Critical thinking and clinical reasoning in the health sciences: A teaching anthology. Insight Assessment/The California Academic Press.

17
Clinical judgment: cognitive errors
Anchoring A snap judgment; diagnose on the first symptom or lababnormality
Availability Using a prior experience — maybe what’s mostavailable in your memory — to diagnose
Attribution To mentally invoke a stereotype and attribute symptoms
Horses vs.zebras
Case may not be typical
Groopman, J. (2008, September/October). Why doctors make mistakes. AARP Magazine, p. 34.

18
Risk strategies
Consult with medical providers asoften as necessary.
Review allergies, medications, andnew medical issues.
Update and review patient’s medicaland dental history on a regular basis.
Perform a complete assessment.

19
Communication

20
Communication: methods
Verbal
Written

21
Communication: pathways
Dentist ↔ Other Providers
Consults with medical providers Referrals to specialists
Dentist ↔ Staff
Organizational culture Education and trainingJob descriptions and
competencies
Staff ↔ Patient
Office procedures Patient education
Dentist ↔ Patient
Health literacy Informed consent

22
Risk strategies
“Teach-back” method
Written materials at appropriate reading level
Team training

23
Communication strategies to enhance the Dr.–Pt. relationship
Explain the recommended procedure.
Start with the diagnosis and educate the patient.
Offer an explanation and rationale for why this is an appropriate treatmentplan.
Go over the treatment plan step by step.
Ask the patient to repeat back proposed treatment plan and/or informedconsent discussion.
Provide written documentation for patient to take home, and document inchart.
Reinforce patient teaching (staff).

24
Teach-back method
“I want to be sure that Idid a good job explainingyour problem. Can youtell me:
• What your problem is?
• What you need to do?
• Why you need to doit?”

25
Printed Material
Simply Put CDC:
• Use a font size of at least 12–14 points.
• Remember:
o Italic font is difficult to read.
o ALL CAPS ARE DIFFICULT TO READ.
• Limit information to three to four messages.
• Put the most important information at thebeginning and repeat it at the end.
• Eliminate technical jargon.
Developing your own patient education materials
http://www.cdc.gov/healthliteracy/pdf/simply_put.pdf

26
Issues with documentation
Content
Complete, timely,factual, consistent
Appropriateness
Nothing other thanwhat’s pertinent to
the care of thepatient
Mechanics
Legibility, correctmethod for making
addendums orcorrections,alterations

27
Issues with documentation
• Patient compliance, including missed/cancelledappointments
• Treatment plan changes
o Receipt of diagnostic results
o Follow-up
o Patient response
• Telephone conversations
• After-hours contact
• Consults

28
Contributing factors to patient behavior
• Complex medical/dental history
• Psychiatric disorders
• Drug/alcohol use/abuse
• Social/personal issues
• Cultural factors
• Language barriers
• Health literacy

29
Factoring in provider/staff behaviors
• Fatigued
• Frustrated
• Angry or defensive
• Dogmatic
• Inexperienced
• Distracted
• Condescending
• Unprofessional

30
Factoring in provider/staff behaviors
• Likely to make clerical mistakes (billing,appointments, etc.)
• Impatient
• Lack of empathy
• Apathetic
• Uses language tootechnical for patients tounderstand
• Gives advice that is toogeneral

31
Risk strategies
Patient behavior Dentist/staff behavior
Policies and procedures Policies and procedures
Behavioral contracts Supervision & evaluation
Termination from practice Training and education

32
Top 5 risk management dental consultations
Refunds and waivers
Terminating the provider−patient relationship
Demands or claims from patients
Complaints
Adverse events

33
Refunds and waivers
Businessdecision vs.true liability
Options
Release fromliability
34
Proactive steps: screening process
Have you carefully reviewed the patient’smedical history? (Obtain records inadvance, if possible.)
Do gaps exist in the patient’shistory/information?
Does the patient have realisticexpectations?
Why did the patient choose your practice?

35
Terminating the doctor–patient relationship
Should comply with practice policies stated in the officebrochure.
Requires sufficient and objective documentation that supportsthe decision.
Time termination to avoid abandonment (e.g., patients instaged phases of treatment.)
For nonpayment of bills, be cautious of timing.

36
Terminating the doctor–patient relationship
• Rationale based onlong-term benefits tothe patient
• Letter is business-likeand nonconfrontational
• Reason for discharge isnot required
• Offer emergency carefor stated period, e.g.,30 days, specifyingwhen offer expires

37
Termination can be challenging
Make sure the process is well thought out and the rightchoice for each situation.
Once the decision is made, stick to it.
Second chances often lead to the patient believinghis/her negative behaviors can continue withoutconsequence.

38
Demands or claims from a patient
• Definition of aclaim
• Contacting yourmalpracticecarrier
• Release ofliability
39
Complaints: sources
Phone In person Email or letter
Social mediaState attorney
general’soffice
State licensingboards
Office of CivilRights
Federal TradeCommission

40
Complaint–litigation cycle
Complaint
Noresolution
ClaimLitigation
Public &staff effect

41
Complaints are opportunities
Basic risk-reduction tool:
• Quality of care
• Policies and procedures
• Communication issues

42
Complaints are opportunities

43
Risk strategy: performance improvement program
Informalprogram
• Every complaint is an opportunity for improvement.
• Other triggers: refunds, terminations, multiple visitsfor same complaint, etc.
Formalprogram
• Respond to board complaints in a timely manner.
• May need assistance from MedPro Group.
• Before implementing a formal program, consult withlegal counsel.
Kalenderian, E., Walji, M. F., Tavares, A., & Ramoni, R. (2013). An adverse event trigger tool in dentistry: A new methodologyfor measuring harm in the dental office. Journal of the American Dental Association, 144(7):808−814.

44
Adverse events
In emergentsituations,
patient safetycomes first
Assistance asneeded
Contactmalpractice
carrier

45
Summary
Technical skill is the leading factor in most dentalclaims.
Other key risk issues identified in dental claimsinclude clinical judgment, communication, andbehavior-related factors.
Documenting a complete, timely, and factual recordis critical to your defense — should a claim be madeagainst you.
Implementing risk-reduction strategies can help youdecrease the potential for claims and complaints, aswell as save you time and frustration.

46
What questions doyou have?
Thank You!

47
Disclaimer
The information contained herein and presented by thespeaker is based on sources believed to be accurate at thetime they were referenced. The speaker has made areasonable effort to ensure the accuracy of the informationpresented; however no warranty or representation is madeas to such accuracy. The speaker is not engaged inrendering legal or other professional services. If legaladvice or other expert legal assistance is required, theservices of an attorney or other competent legalprofessional should be sought.


















