
PP. 957-960. Fights pathogens to prevent infections and disease.
Upload
dana-sinziana-brehar-cioflecCategory
view
262download
2
Dental Healthcare Associated Infections: an overview of pathogens, risks and control
measures
Infection control in dental practice
Purpose: to prevent the transmission of bacteria, viruses and fungi from:
- patient to patient
- patient to dental practitioner
- dental practitioner to patient

Infection in the Dental Practice
• Direct / indirect contact (via contaminated instruments and equipment)
• Germs may enter new host by:– Inhalation
– Ingestion
– Skin discontinuities (contaminated sharps)
– Splashing onto skin or mucosa
Transmission of germs in the dental practice
• Bloodborne:– bleeding/surgical procedures e.g. Hepatitis B virus, Hepatitis C
virus, HIV
• Airborne: – small droplets containing infectious agents eliminated by
infected person who coughs, sneezes, talks e.g. influenza viruses
– large droplets (splash, splatter) generated by specific procedures – involve closer contact: contaminate hands of dental staff, objects, instruments – further transferable to eyes, mouth, other objects, other patients

Infections in the dental practice
• BBP (bloodborne pathogens): HBV, HCV, HIV
• Airborne pathogens: influenza, measles, mumps, rubella, varicella, adenoviruses, respiratory syncytial virus
• Pathogens in the oral cavity i.e. saliva, dental plaque, oral lesions:– herpes simplex virus (HSV), Epstein Barr Virus (EBV), Human
papilloma virus (HPV) – bacterial genera: Streptococcus, Actinomyces, Bacteroides,
Fusobacterium, Lactobacillus, Propionibacterium, Treponema, Veillonella, etc
Infections in the dental practice (continued)
Blood borne pathogens (BBP):Hepatitis B Virus (HBV) – present in blood and saliva of infected
persons; greatest hazard to non-vaccinated dental worker due to:• Effective transmision by percutaneous and transmucosal exposures• Potential transmission through contaminated objects and
instruments:– high survival time outside infected host (over 7 days in dried blood
stains on surfaces, instruments)– resistance to some disinfectants; requires chlorine disinfection (alcohol
is not enough)• disease can become chronic (chronic hepatitis) and complicated
(liver cirrhosis, liver cancer)• Effective vaccination is available and highly recommended /
mandatory for healthcare workers

Infections in the dental practice (continued)
Blood borne pathogens (BBP): (continued)
Hepatitis C Virus (HCV) – similar transmission routes BUT less effective than HBV
• No effective vaccine available yet (researches ongoing)• Infection can lead to chronic hepatitis, liver cirrhosis and liver cancer
Human Immunodefficiency Virus (HIV) – similar transmission routes BUT less effective than HBV due to lower survival time of HIV outside host and to higher vulnerability to disinfectants e.g. alcohol

Infections in the dental practice (continued)
Blood borne pathogens (BBP): (continued)
Estimate Risk of BBP transmission by injury with contaminated sharps (needles, blades, etc):
• 30% for HBV• 3% for HCV• 0.3% for HIV
[McCarthy G.M. – Risk of Transmission of Viruses in the Dental Office, J Can Dent Assoc 2000; 66:554-5, 557]

Infections in the dental practice (continued)
Respiratory viral infections:
• Higher prevalence of influenza, RSV, adenovirus infections in dentists > general population
• immunization against influenza recommended to reduce transmission to patients, co-workers, family members
• Immunization against measles, mumps, rubella (MMR vaccine) and varicella recommended to susceptible workers i.e. not previously vaccinated or who did not get these diseases during childhood (no evidence of natural immunity)

Infections in the dental practice (continued)
Herpes viruses (HSV type 1):• Shed and transmissible via
saliva; Cause persistent infections
• Report on outbreak of gingivostomatitis in 20 of 46 patients treated by dental hygienist with herpetic whitlow (skin HSV lesion acquired from HSV infected patient and further transmitted to other patients due to not wearing gloves!!)
[McCarthy G.M., J.Can.Dent.Assoc., 2000]

Contamination →Infection
• Contamination = presence of infectious agents on various surfaces e.g. objects, instruments, skin, mucous membranes
• Colonization = first stage of infection; pathogen situated at the appropriate entry site e.g. skin (discontinuity!), respiratory, digestive, conjunctiva – not necessarily followed by infection
• Infection = Invasion by and multiplication of a microorganism or infectious agent in a bodily part or tissue ± tissue injury and progress to disease

Factors influencing progress from contamination to infection
Infectivity • Capacity of pathogen to enter, survive and multiply in a
susceptible host
Pathogenicity (+ invasiveness & toxigenesis)• Capacity of pathogen to produce disease in a
susceptible host
Virulence• Degree of pathogenicity: determinants of virulence:
genetic / biochemical / structural features e.g. adhesion factors, toxin production

Factors influencing progress from contamination to infection (continued)
Pathogen Minimal infective dose
S. pyogenes, S. aureus Under 103 CFU
Shigella (virulent strains) As low as 10 CFU
Bacillus anthracis 104 spores !!
Brucella species 10-100 organisms
Francisella tularensis 10-50 organisms

Factors influencing progress from contamination to infection (continued)
Survival outside host
Variola virus • years - patient exudate, room temperature, dark
Mycobacterium tuberculosis• 90 – 300 days – sputum, room temperature, dark• 10 – 120 days – dust (floor/objects/fabric)
Neisseria meningitidis• 1 day ˂ – glass/plastic/fabric, suspension, dark
Hepatitis B Virus• - at least 7 days !! (dried blood spots on surfaces)

Survival outside host
Spores: reproductive structures adapted
for longtime survival in unfavourable
conditions
(etymology: ancient Greek spora = seed)
Bacterial spores - outer layer of keratin resistant to chemicals, staining and heat → bacterium able to stay dormant for years, protected from temperature differences, absence of air, water and nutrients
Spore forming bacteria: • Clostridium spp (e.g. Clostridium difficile, Clostridium tetani); • Bacillus spp (B. anthracis).

The infectious process
Relationship between PATHOGEN and HOST
• Depends on:– Virulence (pathogen) vs. Resistance/Susceptibility (host)
– Exposure (encounter: pathogen & ”suitable” host)

The ”chain of infection”
New HOSTSusceptible?Age, Gender,
Genetics, Immunity, Prevention
EXITBody fluids: e.g. Blood,
saliva
RESERVOIRInfected host:e.g. Patient
ENTRYRespiratory,Digestive,
Skin injury, Membranes

Infection riskPathogen related
– Transmission route– Survival outside host
The chances of seroconversion following percutaneous exposure to blood infected with blood borne viruses varies significantly from the relatively low chance of infection with HIV (0.3%) to the much higher transmission rates of up to 30% for Hepatitis B. Why? Resistance (survival) outside host.

Infection risk (continued)
Work related = contact with blood, saliva, respiratory secretions and contaminated objects (instruments, equipment)– Techniques: surgical procedures e.g. tooth extraction, periodontal
surgery, implantology; splash generating procedures e.g. air/water flow, tartar removal, dental polishing
– Instruments: sharps e.g. needles, blades, burrs, probes– Additional factors e.g. work load, pressure or interrupted routine
(emergencies, visitors)
___________________________________– PPE: gloves, face protection (mask, goggles, face shields)

Infection risk (continued)
Host (e.g. dental healthcare staff) related:
– Susceptibility (age, gender, genetic factors, immunity, prevention – vaccination!)
– Job proficiency (expertise, experience - being able to recognise potential high risk exposures)
– Knowledge of pathogens; techniques; equipments– Adherence to SOPs (technical & biosafety) – periodic
assessment required
Infection risk (continued)
Exposure of dental patients and dental healthcare providers to microorganisms present in the mouth, blood and respiratory tract
Transmission routes in dental settings:
- Intact or non-intact skin in direct contact with blood, saliva, infectious patient materials (e.g. pus from dental abscess, periodontal pockets)
- Indirect contact with contaminated object (e.g. instruments, operatory equipment, environmental surfaces)
- Contact of mucous membranes of the eyes, nose, or mouth with droplets (e.g. spatter) containing microorganisms from infected person (coughing, sneezing, talking) and propelled a short distance + projection during use of rotative instruments
- Inhalation of airborne microorganisms that can remain suspended in the air for long periods of time (proximity between dentist and patient during treatment)
Risk categorisation for healthcare staffSource: Australian Guidelines for the Prevention and Control of
Infection in Healthcare (2010)
Guidance for vaccination protocols:• Category A = direct contact with blood or body substances e.g. dentists,
surgeons and other medical practitioners, nurses, healthcare students, mortuary technicians, cleaning staff (high exposure to bloodborne pathogens e.g. HBV, HCV, HIV ± airborne pathogens e.g. influenza, rubella, TB)
• Category B = indirect contact with blood or body substances (lower exposure to bloodborne pathogens + exposure to airborne pathogens e.g. influenza, rubella)
• Category C = minimal patient contact (administrative staff, catering staff)
• Laboratory staff = exposure to high concentrations of pathogens generated
by culture procedures + handling human blood and tissues

Infection control
• Reduce the spread of microorganisms:– Reduce contamination of surfaces, objects (cleaning and
disinfection)– Sterilization – disposable instruments– Good personal hygiene practices (hand hygiene!!)– PPE: hand protection (gloves), respiratory protection (mask),
eye protection (goggles, face shield), body (gown, shoes)– Disposable products e.g. paper towels– Risk minimisation techniques e.g. rubber dam, pre-procedural
mouthrinsing with oral antiseptics (e.g. Chlorhexidine)

Universal & Standard Precautions
UNIVERSAL PRECAUTIONS:
• infection control procedures to prevent transmission of bloodborne pathogens (HBV, HCV, HIV)
• blood + certain body fluids should be treated as infectious - impossible to know who may be
carrying a bloodborne virus → should apply to all patients
STANDARD PRECAUTIONS:
• integrate and expand Universal Precautions to include organisms spread by contact with:Blood
+All body fluids, secretions, excretions (regardless of whether they contain blood)
Non-intact skinMucous membranes
Saliva = potentially infectious material in dental infection control → no operational difference in clinical
dental practice between Universal and Standard Precautions

Standard Precautions
- Handwashing- PPE: gloves, masks, eye protection, and gowns,
intended to prevent exposure of skin and mucous membranes to blood and other potentially infectious materials
- Proper cleaning, disinfection/sterilization of patient care equipment
- Cleaning and disinfection of environmental surfaces
- Injury prevention through engineering controls or safer work practices

Disinfectant solution used for immersion of instruments prior to sterilization

Autoclave – moist heat sterilization

Autoclave chamber with trays for instruments; control panel with predefined programmes

Autoclave: control panel and sterilization report

Preparing the instruments for autoclavation: packaging in heat-sealed plastic (PP) bags
Dental instruments packaged for autoclavation

Autoclaved sealed plastic bags (PP) with instruments prepared for use
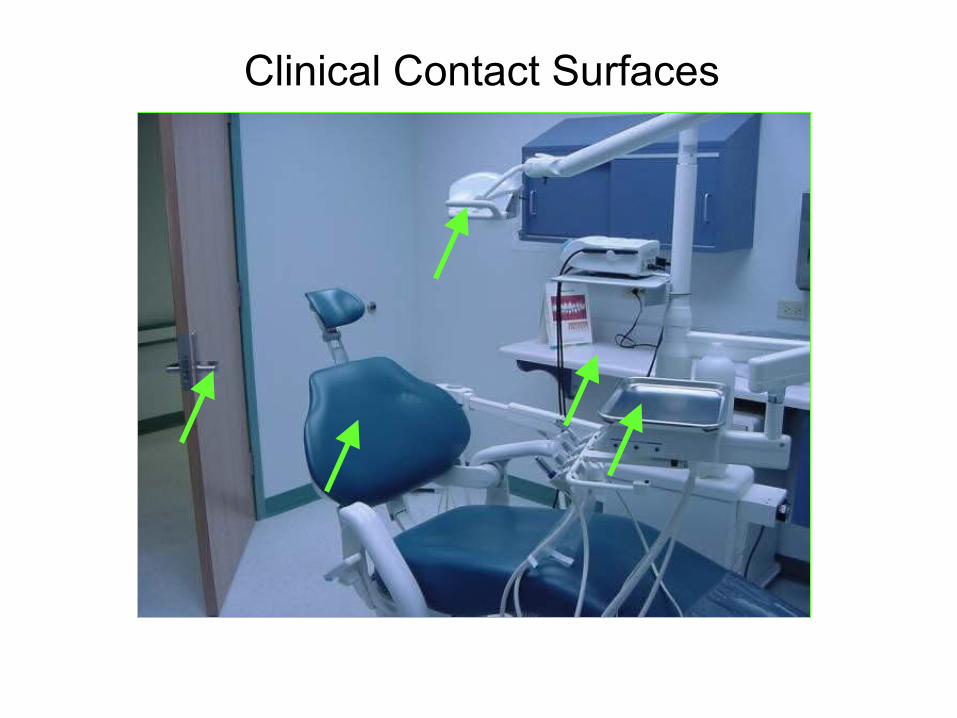
Clinical Contact Surfaces

Housekeeping Surfaces

Disinfectant solution used for surfaces; hand washing station

Dental unit waterlines, biofilm and water quality
• Biofilms = colonies of microorganisms on surfaces e.g. inside plastic tubing that transports water within the dental unit to handpieces and air-water syringes = reservoir of microorganisms in water used for dental treatment
• Most microorganisms isolated from dental water systems originate from the public water supply (low risk of disease for healthy persons)
• + pathogenic organisms (e.g. Legionella spp. and Pseudomonas sp.) BUT no documented infections

Disinfectant solution for the aspiration system of dental unit

Use of sterile water/irrigating solutions
• Purpose: to prevent entry of oral microorganisms into the bloodstream or oral sterile sites (e.g. bone or subcutaneous tissue) during oral surgery
• Dental units cannot deliver sterile water/irrigating solutions (tubing cannot be reliably sterilized)
• Sterile water delivery devices:– sterile irrigating syringes– physiodispensers (sterile water
bypasses the dental unit and passes through sterile disposable or autoclavable tubing)

Waste management (1): containers for disposal of sharps (left) and other contaminated materials
(right) - (final elimination by incineration)

Waste management (2): contaminated materials packed in yellow plastic bags and deep frozen prior to collection by
specialized company (final elimination by incineration)

References
• http://www.cdc.gov/oralhealth/infectioncontrol/guidelines/index.htm

References (continued)
• http://www.ada.org.au/app_cmslib/media/lib/1203/m356702_v1_infection%20control%20guidelines%202012.pdf
• http://www.dentistrytoday.com/infection-control/1329-new-cdc-infection-control-guidelines-for-dentistry
•


















