
Dengue case definitions: what is captured and what is missed
23
Dengue case definitions: what is captured and what is missed Kay M. Tomashek Centers for Disease Control and Prevention Dengue Branch, San Juan, Puerto Rico Sabin Vaccine Institute and PAHO Workshop June 11-13, 2014 Washington, D.C.
Transcript of Dengue case definitions: what is captured and what is missed

Dengue case definitions: what is
captured and what is missed
Kay M. Tomashek
Centers for Disease Control and Prevention
Dengue Branch, San Juan, Puerto Rico
Sabin Vaccine Institute and PAHO Workshop
June 11-13, 2014 Washington, D.C.
Overview of Issues
• Most DENV infections are asymptomatic
– Asymptomatic often combined with afebrile cases, undifferentiated fever, or absent <2 days in studies
• Febrile symptomatic cases are difficult to distinguish from other acute febrile illnesses (AFI)
– Mild illness
– Early in clinical course
• Severe cases more identifiable
– Atypical cases
– Cases not meeting all DHF criteria

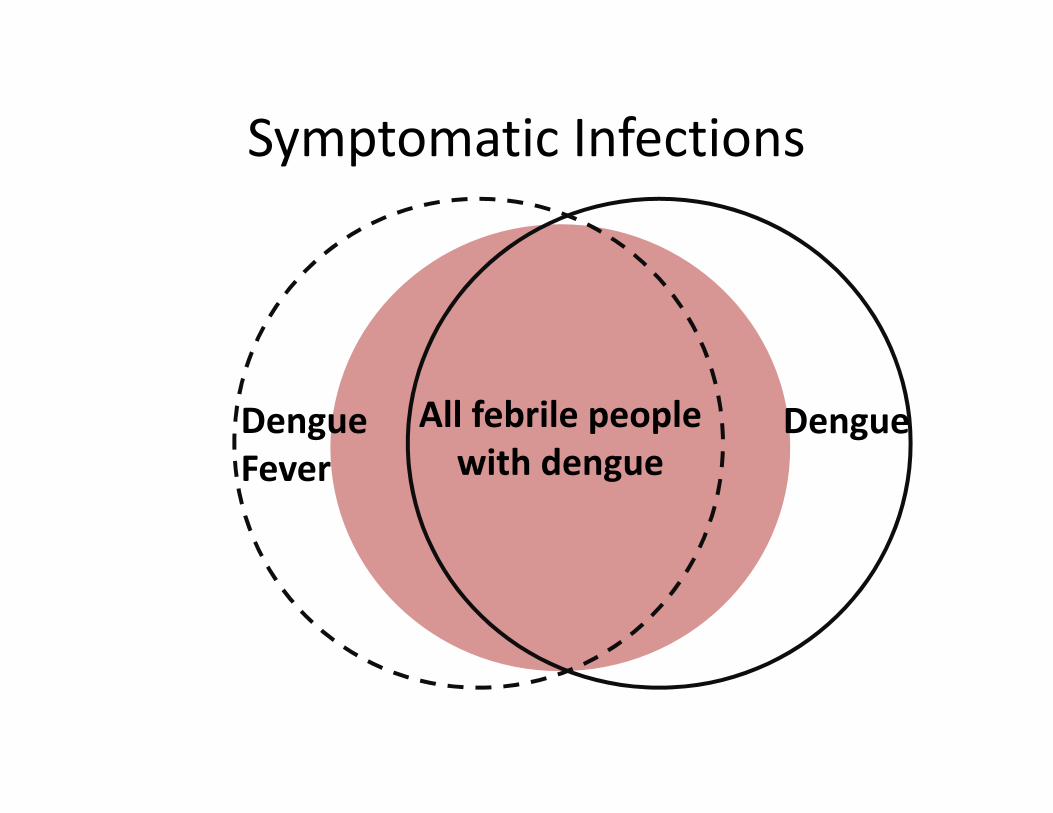
Symptomatic Infections
All symptomatic
people with dengue

Symptomatic Infections
All symptomatic
people with dengue
All febrile people
with dengue
Who are these
afebrile
symptomatic
dengue cases?

Afebrile Symptomatic Cases
• Cluster study (Yoon 2013)
• 1599 children 6 months to 15 years old
• Lived 100m from PCR + febrile child or control from cohort
• Visited at day 0, 5, 10, and 15; blood draw days 0 and 15
• 126 infected; 102 symptomatic of which, 19 (18.6%) had no
fever history or history of antipyretic use:
� Symptoms among afebrile: rhinorrhea (47%), cough
(42%), abdominal pain (21%), and headache (16%)
� Used IgM to diagnose so illness may be unrelated
• Prospective study and nested serosurvey (Likosky1973)
• 2865 people (all ages) in households followed for 10 weeks
• 214 of 328 infected; 16 (7.5%) afebrile symptomatic

Symptomatic Infections
All symptomatic
people with dengue
All febrile people
with dengue
All
AFI

Acute Febrile Illness StudiesAuthor Country Inclusion Criteria N Proportion
Diagnosed
Leading Diagnoses
(% of all AFI)Mueller
(2014)
Cambodia;
3 outpatient
health
centers
Outpatients 7-49 years
with fever ≥38.0˚ or
history of fever < 8
days
1193 in 3
years
86% Malaria (57% PCR)
Leptospirosis (9% PCR)
Influenza (9% PCR)
Dengue (6% PCR)
Scrub typhus (4%)
Mayxay
(2013)
Laos;
2 hospitals
Admitted patients 5 -
49 years with fever
≥38.0˚ and no obvious
cause of fever
1938 in 2
years
41% Dengue (8% PCR or NS1)
Scrub typhus (7%)
Influenza (6% PCR)
Leptospirosis (6% PCR, Cx, MAT)
Japanese encephalitis (6% ELISA)
Bacteremia (2%)
Chheng
(2013)
Cambodia;
1 hospital
Admitted children <16
years with fever ≥38.0˚
1,225 in
one year
47% Dengue (11% IgM, 5% NS1)
Scrub typhus (8%)
Japanese encephalitis (6%)
Bacterial infection (11%)*
Other Rickettsioses (3%)
Leptospirosis (1% culture, NAAT)
Kasper
(2012)
Cambodia;
9 clinics
Patients >2 years with
fever >38.0˚ for >24
hours and <10 days;
9.9% admitted
9,997 in
3 years
38% Influenza (20%)
Dengue (9% PCR )
Malaria (7%)

Acute Febrile Illness StudiesAuthor Country Inclusion
Criteria
N Proportion
Diagnosed
Leading Diagnoses
(% of all AFI)Punjabi
(2012)
Indonesia;
1 hospital
Inpatients of all ages
with fever ≥38.0˚
and negative malaria
blood smear
226 in
3 years
35% Leptospirosis (9% PCR)
Rickettsioses (7%)
Typhoid fever (6%)
Dengue (4% seroconversion)
Manock
(2009)
Ecuador;
2 hospitals
Inpatients >5 years
with fever ≥38.0˚ for
<7 days without
focus of infection
304 in
3 years
40% Leptospirosis (13%)
Malaria (13%)
Rickettsioses (6%)
Dengue (5% seroconversion)
Q fever (5%)
* There were 76 (6.3%) bloodstream infections in this group. Staphlococcus aureus, Salmonella enterica serovar Typhi, Streptococcus
pneumoniae, Burkholderia pseudomallei, Escherichia coli lead list

Acute Febrile Illness Studies
• Capture all febrile dengue cases seeking care
– Most studies 35 to 45% of all AFI diagnosed
– Dengue lab confirmed in 4 to 11% of all AFI cases
– Co-infection rate in AFI studies 3 to 11%
• Need system to identify severe dengue cases
not presenting with fever
– Ask history of fever
Symptomatic Infections
All symptomatic
people with dengue
All febrile people
with dengueDengueDengue
Fever

Case DefinitionsDengue fever, 19971
• AFI with ≥2 of following:
– Headache
– Retro-orbital pain
– Myalgia
– Arthralgia
– Rash
– Leukopenia (WBC <5.0 x 109 /L)
– Hemorrhagic manifestation
• Case must have either supportive
serology or occurred in same
location and time as other lab
confirmed cases
Dengue, 20092
• A febrile illness with ≥2 of following: – Aches and pains
– Rash
– Leukopenia
– A positive tourniquet test
– Nausea, vomiting
• In patients who traveled to or lives in dengue endemic area
Dengue with warning signs• Abdominal pain or tenderness, persistent
vomiting, clinical fluid accumulation, mucosal bleeding, lethargy, restlessness, liver enlargement, and an increase in hematocrit with decrease in platelet count
Aches and
pains
1World Health Organization (1997) Dengue haemorrhagic fever: diagnosis, treatment, prevention and control. 2nd ed. Geneva: World Health Organization.2World Health Organization (2009) Dengue: guidelines for diagnosis, treatment, prevention and control. Geneva, Switzerland: World Health Organization.
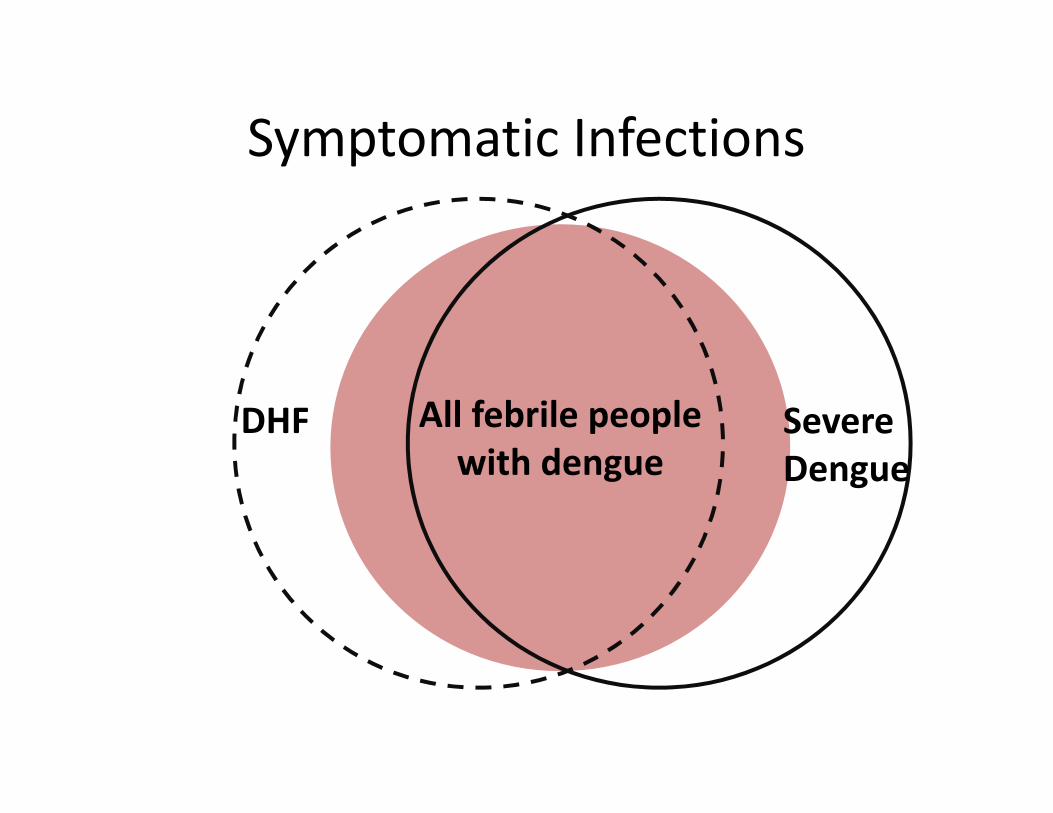
Symptomatic Infections
All symptomatic
people with dengue
All febrile people
with dengueSevere
Dengue
DHF

Case DefinitionsDengue hemorrhagic fever, 19971
• An illness with the following:
– fever or history of fever of 2 to 7 days
duration
– hemorrhagic tendency
– Platelet count <100,000 cells per mm3
– Evidence of plasma leakage
Severe dengue, 20092
• An acute febrile illness of 2 to 7
days duration with any or all of
the following:
– Severe plasma leakage leading to shock
or fluid accumulation with respiratory
distress
– Severe bleeding as evaluated by clinician
– Severe organ involvement as evidenced
by elevated liver transaminases or
impaired consciousness
1World Health Organization (1997) Dengue haemorrhagic fever: diagnosis, treatment, prevention and control. 2nd ed. Geneva: World Health Organization.2World Health Organization (2009) Dengue: guidelines for diagnosis, treatment, prevention and control. Geneva, Switzerland: World Health Organization.

Case Definition Evaluation
• Sensitivity = probability that LP cases are identified by test (case
definition) as having dengue; high sensitivity � few FN
• Specificity = probability that LN cases are identified by test as
not having dengue; high specificity � few FP
• Positive predictive value =
probability clinically diagnosed
case is a LP dengue case
• Negative predictive value =
probability that clinically diagnosed
non-dengue case is LN dengue case

Diagnostic Value of Case DefinitionsComparison of Outpatient and Inpatient Settings
• Pre-selected population that already met some of the criteria for
DF so increased sensitivity. Also, improved in inpatient setting,
which may be due to a difference in patient populations.
• Lower sensitivity in children < 4years old (values in parentheses)
• Higher PPV with increased incidence of disease (inpatient setting)
Author Study population Sensitivity Specificity PPV NPV
1997 2009 1997 2009 1997 2009 1997 2009Gutierrez
(2013)
Nicaragua
Prospective cohort of children 2 -
15 years; 3407 sought care and
suspected dengue and FUO cases
presenting in first 6 days of illness
are tested; 476 PCR positive cases
89%
(37%)
87%
(46%)
43% 55% 20% 24% 96% 96%
Gutierrez
(2013)
Nicaragua
Prospective inpatient study of 0.5-
14 years old; enrolled those with
fever <7 days and one or more
criteria for DF and no focus; 1160
cases and 723 PCR positive cases
97%
(87%)
99%
(97%)
22% 8.5% 67% 64% 80% 88%

Positive Predictive Value (PPV)
• What proportion of clinically diagnosed cases actually have
the disease?
From Assoc. of Faculties of Medicine of Canada. Accessed at http://phprimer.afmc.ca/Part2-MethodsStudyingHealth/Chapter6MethodsMeasuringHealth

Use of Case Definition to Identify CasesAmong Hospital Inpatients
Author Study population 1997 2009
DF DHF DSS UC D DWS SD UCMacedo
(2014)
Brazil
Retrospective review of
suspected dengue
inpatients 0 - 18 years old
from 3 hospitals during
outbreaks; 267 of 450
laboratory positive.
26 119 46 76 (29%)
• 7 D
• 50 DWS
• 19 SD
18 142 107 0
Gan
(2013)
Singapore
Retrospective review of
1278 PCR+ adult inpatients
at 1 hospital. All classified.
1061 183 34 0 617 457 204 0
* DF Dengue Fever; DHF Dengue Hemorrhagic Fever; DSS Dengue Shock Syndrome; UC Unclassified; D Dengue; DWS Dengue with
Warning Signs; SD Severe Dengue
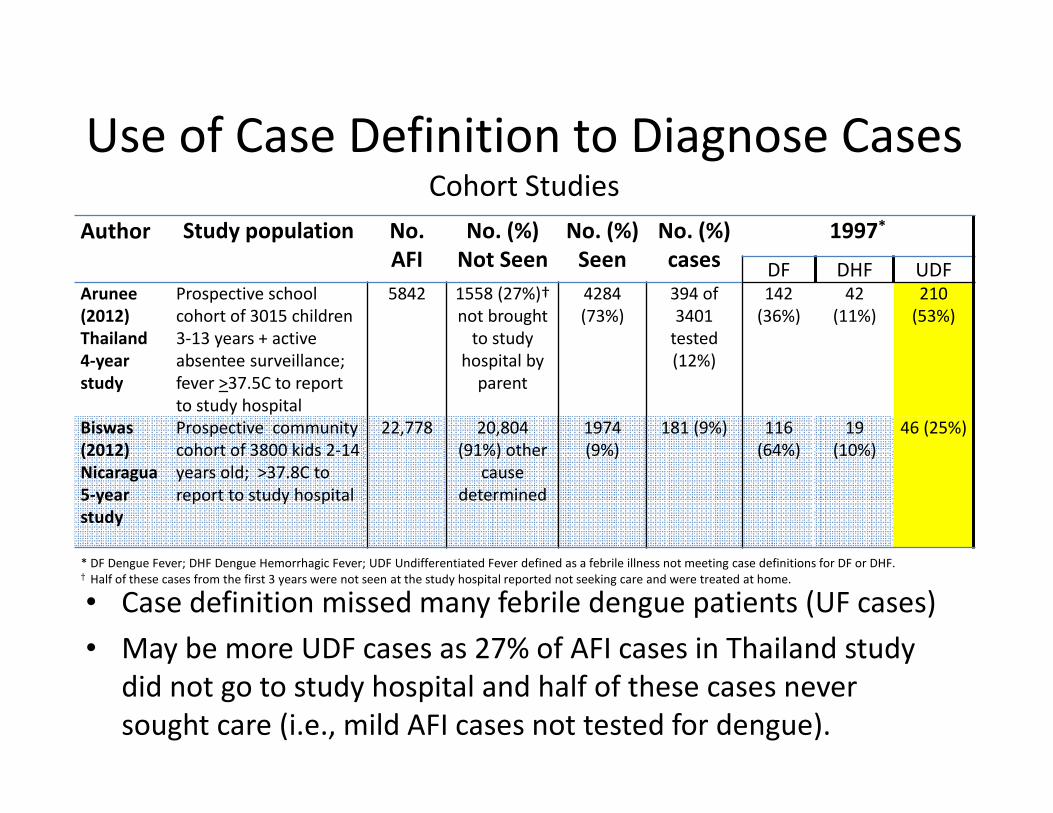
Use of Case Definition to Diagnose CasesCohort Studies
Author Study population No.
AFI
No. (%)
Not Seen
No. (%)
Seen
No. (%)
cases
1997*
DF DHF UDFArunee
(2012)
Thailand
4-year
study
Prospective school
cohort of 3015 children
3-13 years + active
absentee surveillance;
fever >37.5C to report
to study hospital
5842 1558 (27%)†
not brought
to study
hospital by
parent
4284
(73%)
394 of
3401
tested
(12%)
142
(36%)
42
(11%)
210
(53%)
Biswas
(2012)
Nicaragua
5-year
study
Prospective community
cohort of 3800 kids 2-14
years old; >37.8C to
report to study hospital
22,778 20,804
(91%) other
cause
determined
1974
(9%)
181 (9%) 116
(64%)
19
(10%)
46 (25%)
* DF Dengue Fever; DHF Dengue Hemorrhagic Fever; UDF Undifferentiated Fever defined as a febrile illness not meeting case definitions for DF or DHF.† Half of these cases from the first 3 years were not seen at the study hospital reported not seeking care and were treated at home.
• Case definition missed many febrile dengue patients (UF cases)
• May be more UDF cases as 27% of AFI cases in Thailand study
did not go to study hospital and half of these cases never
sought care (i.e., mild AFI cases not tested for dengue).

Undifferentiated Fever Cases
• No age or sex difference between UDF vs. DF/DHF
• Had lower median peak temperature and shorter duration of fever than DF or DHF
• Most common symptoms among UDF: headache (89%), anorexia (81%), nausea/vomiting (68%), and myalgia (48%)
– Less likely to have petechiae and convalescent rash than DF or DHF cases
– More likely than to have lethargy and drowsiness more than 3 days
* Sirivichayakul, et. al. PLoS Neglected Trop Dis 2012; 6 (2):1-10

Final Thoughts
• There are some challenges in capturing all
dengue cases
– A lot of dengue may be mild and may not present
to hospital
• Clinic and hospital cases needed
– Many cases occur in children but not all
– Some cases have symptoms but no fever but may
contribute to transmission and burden of disease
• Even if they present they may not be captured
• These represent a small proportion of all dengue
Final Thoughts
• If we want to determine if dengue cases still
occurring post vaccine release, we would need
the most sensitive case definition
– Mild cases missed: 1997 case definition did not
capture 25 to 53% of all cases in cohorts in
Thailand and Nicaragua
– Cases among young children missed: 1997 and
2009 case definitions did not perform well among
children <4 years old in Nicaragua
Final Thoughts
• Existing surveillance systems could be adapted to detect acute febrile illnesses (AFI) and cases with recent fever history
– Would allow us to detect mild cases of undifferentiated fever
– Would capture cases in pre-verbal children
– Will enable us to detect atypical cases
• As case counts drop, sentinel AFI sites would augment existing passive surveillance including participatory surveillance systems
Final Thoughts
• As the clinical endpoint for a dengue vaccine is
dengue and not severe dengue, more work is
needed to better classify and distinguish DF
and some lesser degree of severe dengue as
not well defined












![A Peek At What You Missed[1]](https://static.fdocuments.in/doc/165x107/54b57fbb4a795940268b4597/a-peek-at-what-you-missed1.jpg)




