Demographics of HT in HK · 3 Core Document (Table of Content) Chapter 1 Epidemiology 2...
23
1 Hong Kong Reference Hong Kong Reference Framework for Hypertension care for Adults in the Primary Care Settings MANAGEMENT OF MANAGEMENT OF HYPERTENSION USING THE REFERENCE FRAMEWORK 1 Demographics of HT in HK Population Health Survey in 2003-2004 1 O ll l fh t i 27% Overall prevalence of hypertension 27%. Among them, 56% were unaware by patients For those known HT, 73% had taken anti-HT prescribed by doctors while 16% reported to have taken over-the-counter medications. 1. Population Health Survey 2003‐2004. Collaborative project of DN and the Department of Community Medicine of HKU
Transcript of Demographics of HT in HK · 3 Core Document (Table of Content) Chapter 1 Epidemiology 2...

1
Hong Kong ReferenceHong Kong Reference Framework for Hypertension care for Adults in the Primary Care Settings
MANAGEMENT OFMANAGEMENT OF HYPERTENSION USING THE REFERENCE FRAMEWORK
1
Demographics of HT in HK
Population Health Survey in 2003-20041
O ll l f h t i 27% Overall prevalence of hypertension 27%. Among them, 56% were unaware by patients For those known HT, 73% had taken anti-HT
prescribed by doctors while 16% reported to have taken over-the-counter medications.
1. Population Health Survey 2003‐2004. Collaborative project of DN and the Department of Community Medicine of HKU

2
Management of hypertension byprivate doctors in Hong KongHong Kong Med J 2006;12:115-8
Only 24% of the private doctors measured blood pressure in all new patients aged above 18 years.
30% of the hypertensive patients were diagnosed by opportunistic BP screening.
Management of hypertension in Hong Kong
1 A significant proportion of HT patients were1. A significant proportion of HT patients were undiagnosed.
2. A significant proportion of HT patients were not properly managed.
3. Primary care providers have an important role in the management of hypertensionin the management of hypertension.

3
Core Document (Table of Content)Chapter
1 Epidemiology
2 Population based Intervention and Life Course2 Population-based Intervention and Life Course approach
3 Role of Primary Care in the Management of HT
4 Patient Education
5 Aim of the Framework
6 Prevention of Hypertension6 Prevention of Hypertension
7 Early identification of People with Hypertension
8 Clinical Care of Adults with Hypertension
9 Patient Empowerment
10 Future Direction to Promote the Use of the Framework
6

4
ModulesModule
1 Framework for population approach in the prevention and control of hypertension across the life course
2 Blood pressure measurement
3 Secondary hypertension
4 Evaluation for all newly diagnosed hypertensive patientspatients
5 Dietary intervention
6 Exercise recommendations to people with HT
7 Drug treatment for people with HT
8 Annual assessment
Recommendations from Reference Framework
Prevention and early identification of HT
1. Opportunistic blood pressure measurement in all adults from 18 years of age at least every 2 years
2. Advise individuals at increased risk of
8
developing HT and patients with HT to maintain optimal body weight, restrict dietary salt intake, abstain from smoking and practise healthy lifestyles

5
BPclassification
Initial BP(mmHg)
RecommendedMinimum Review Period
Action
SBP DBP
Pre-hypertension
120-139 80-89 Recheck <1 year Lifestyle modificationhypertension
Stage I HT 140-159 90-99 Confirm < 2 months Lifestyle modification
Stage II HT 160-179 100-109 Evaluate < 1 month Treat < 1 monthLifestyle modifications
>180 >110 Evaluate < 1 week Drug treatmentRefer if malignant HT
9
Refer if malignant HT
The classification is based on the average of 3 or more properly measured seated BP readings, at least 1 week apart on office visits
Relationship between Blood Pressure and Cardiovascular Risk
1 The association between BP and CVS risk is1. The association between BP and CVS risk is continuous at all levels, starting as low as 115/70 mmHg, without a threshold.
2. The higher the BP, the greater is the chance of stroke, IHD, heart failure and other vascular causesF i di id l 40 70 f h3. For individuals 40–70 years of age, each increment of 20 mmHg in SBP or 10 mmHg in DBP doubles the risk of CVD across the entire BP range from 115/75 to 185/115 mmHg

6
CV Mortality Risk Doubles withEach 20/10 mm Hg BP Increment*
7
8
CVmortality
risk
1
2
3
4
5
6
*Individuals aged 40-69 years, starting at BP 115/75 mm Hg.CV, cardiovascular; SBP, systolic blood pressure; DBP, diastolic blood pressureLewington S, et al. Lancet. 2002; 60:1903-1913.JNC VII. JAMA. 2003.
SBP/DBP (mmHg)
115/75 135/85 155/95 175/105
Framework for Population Approach in The Prevention and Control of Diabetes Across the Life Course (MODULE 1)
Age Group Lifestyle advice Risk Screening Disease Monitor g p yassess‐ment
gmanage‐ment
complications
Antenatal •Balanced diet•Physically active
•Monitor wt gain
•Watch out for HT and pre‐eclampsia
•BP control •Monitor fetal growth•Obstetric Cx
Infancy •Breast feeding•Avoid obesity
•Monitor wt gain•Avoid obesity wt gain
Children •Abstain from smoking•Regular exercise•Health eating
•Monitor BMI
12

7
Age Gp Lifestyle advice
Risk assessment
Screening Disease manage‐ment
Monitor compli‐cations
Rehabi‐litation care
Adult & Elderly
•Abstain from smoking•Healthy eating
•monitor BMI•Monitor abdominal circumference
•Measure BP for all individuals aged >=
•BP and lipid control•Monitor
•Malig‐nant HT•TOD
•Help patients to cope with HTeating
•Limit Na intake•Regular exercise•Limit alcohol consumption
circumference•Family history
aged >= 18 every 2 yrs•Measure BP for at risk people every 12 mths or
•Monitor drug adverse effects•Self care•Carer education
with HT and its Cx•Multidis‐ciplinary approach for stroke and renal failure
13
mths orless
Blood Pressure Measurement (MODULE 2)
Mercury sphygmomanometer
most reliable most reliable
checking are needed: e.g. column position, mercury level, blockages and leakages
Electronic devices
can also be used
finger and wrist monitors should be avoided
routine checks and calibration
14

8
Precautions about BP measurement (1)
Seated for at least 5 minutes
Remove constrictive clothing form the arm Remove constrictive clothing form the arm
Use an appropriate sized BP cuff
Support arm with antecubital fossa at heart level
15
Precautions about BP measurement (2)
BP measurement not recommended during exercise or after exerciseexercise or after exercise
Avoid measure BP <1/2hr after eating
Smoking and caffeine should be avoided within 1-2 hours prior to BP recording
Emotional factors may affect BP: consider 24 hr b l t BP it i d lf BPambulatory BP monitoring and self BP
monitoring at home

9
Secondary Hypertension (MODULE 3)
17
Causes of secondary HT Obstructive sleep
apnea Side effects of drugs
Unhealthy dietp
Hyperaldosteronism
Renal parenchymal disease
Renovascular disease
Excess
Unhealthy diet
Erythropoietin side effect
Phaeochromocytoma
Hypothyroidism
H th idi Excess catecholamines
Coarctation of aorta
Cushing's syndrome
Hyperthyroidism
Hyperparathyroidism
Acromegaly18

10
Evaluation of Newly Diagnosed Hypertensive Patients (MODULE 4)
Aims:
to assess lifestyle and identify cardiovascular risk factors that may affect prognosis and guide treatment,
to reveal identifiable causes of high blood pressure, and
to assess the presence or absence of target organ damage (TOD) and cardiovascular diseases
Target organ damages
Heart: LVH, IHD
Renal: Hypertensive nephropathyRenal: Hypertensive nephropathy
Vessel: atherosclerotic plague on big arteries (carotid, iliac,
femoral or aorta)
Angina
Heart failureHeart failure
Brain: stroke, dementia
Peripheral arterial disease
Hypertensive retinopathy, papilloedema

11
Evaluation for Newly Diagnosed Hypertensive Patients
HistoryHistory
Physical examination
Laboratory investigationUrine analysis
RFTRFT
FBS
Lipid profile
12-lead ECG
What are the benefits of BP control in reducing complications? Meta-analysis of 61 prospective, observational
studies which involve 1 million adultsstudies which involve 1 million adults
Blood Pressure reduction of 2 mmHg decreases the risk of cardiovascular events by 7–10%
2 mmHg decrease in
7% reduction in risk of ischaemic heart disease mortality
decrease in mean SBP 10% reduction in
risk of stroke mortality
Lewington et al. Lancet 2002;360:1903–13
12
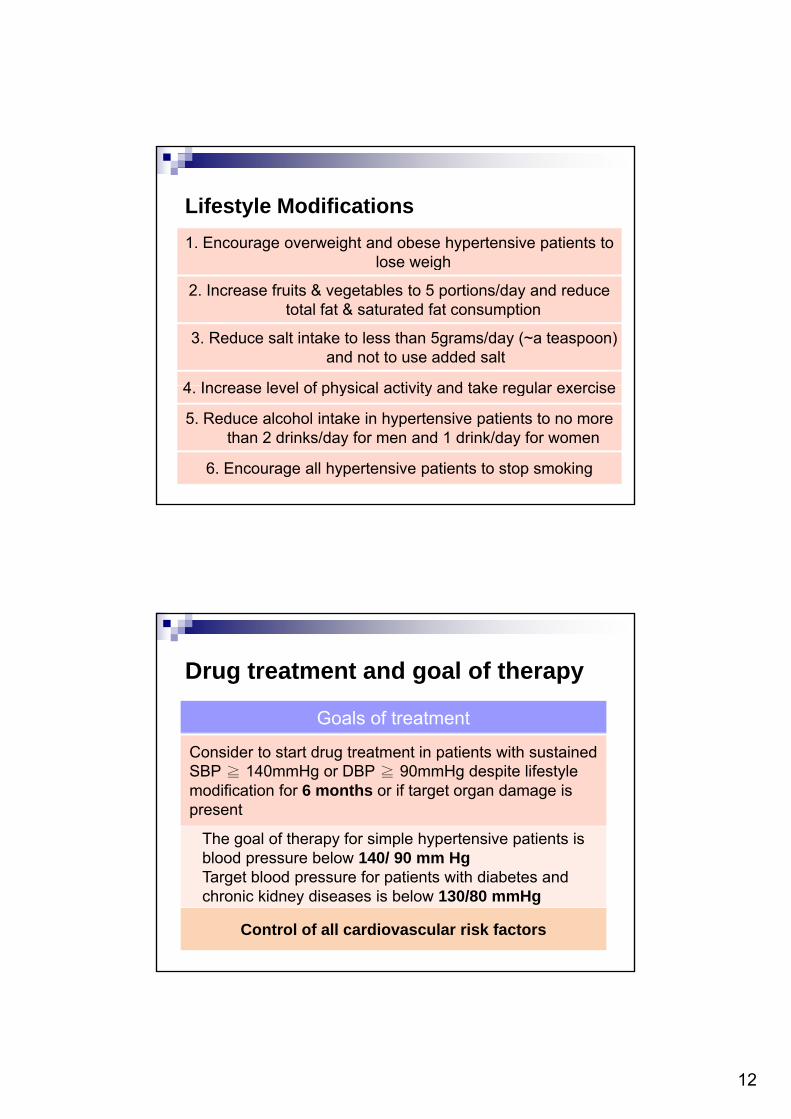
Lifestyle Modifications
1. Encourage overweight and obese hypertensive patients to lose weighlose weigh
2. Increase fruits & vegetables to 5 portions/day and reduce total fat & saturated fat consumption
3. Reduce salt intake to less than 5grams/day (~a teaspoon) and not to use added salt
4 Increase level of physical activity and take regular exercise4. Increase level of physical activity and take regular exercise
5. Reduce alcohol intake in hypertensive patients to no more than 2 drinks/day for men and 1 drink/day for women
6. Encourage all hypertensive patients to stop smoking
Drug treatment and goal of therapy
Goals of treatment
Consider to start drug treatment in patients with sustained SBP ≧ 140mmHg or DBP ≧ 90mmHg despite lifestyle modification for 6 months or if target organ damage is present
The goal of therapy for simple hypertensive patients is bl d b l 140/ 90 Hblood pressure below 140/ 90 mm HgTarget blood pressure for patients with diabetes and chronic kidney diseases is below 130/80 mmHg
Control of all cardiovascular risk factors

13
LifestyleLifestyle
Control Control of blood of blood
Lifestyle Lifestyle modificationsmodifications Drug treatmentDrug treatment
pressurepressure
Lifestyle ModificationsEvidences from studies
Modification Recommendation Approximate SBP
Reduction (range)
W i ht d ti 1 2 M i t i l b d i ht 5 20 H / 10kWeight reduction1,2 Maintain normal body weight 5-20 mmHg/ 10kg
weight reduction
Adopt DASH eating plan
Diet rich in fruits, vegetables, high K and low fat dairy products with a reduced content of saturated and total fat.
8-14 mmHg
Dietary sodium 3,4,5
reduction Reduce dietary sodium intake to no more than 6g per day
2-8 mmHg
Physical activity 6,7 Engage in regular aerobic physical activity 4-9 mmHgPhysical activity , Engage in regular aerobic physical activity such as brisk walking (at least 30 min per day, most days of the week).
4-9 mmHg
Moderation of alcohol
consumption
Limit consumption to no more than 2 drinks per day in most men and to no more than 1 drink per day in women and lighter weight persons.
2-4 mmHg

14
Dietary Intervention (MODULE 5)
DASH – Dietary Advice to Stop Hypertension:
Rich in fruits, vegetables Rich in potassium, magnesium and
calcium Low in cholesterol, saturated and total fatLow in sodiumLow in sweets and added sugars
DASH eating plan based on 2000 calories a day
Food GroupDailyServings Examples of Serving Sizes
Grain and grain products
6‐8 1 slice bread1 cup ready to eat cerealproducts 1 cup ready‐to‐eat cereal1/2 cup cooked rice, pasta, or cereal
Vegetables (dark green vegetables
are good sources of K+ and Mg++)
4‐5 1 cup raw leafy vegetables1/2 cup cooked vegetables1/2 cup vegetable juice
Fruits( d f K )
4‐5 1 medium fruit1/4 d i d f it
1 cup = 240 ml
(good sources of K+) 1/4 cup dried fruit1/2 cup fresh, frozen, or canned fruit1//2 cup fruit juice
Low fat or fat free dairy products
(good sources of Ca++)
2‐3 1 cup milk1 cup yoghurt1 1/2 ounce cheese

15
Food GroupDailyServings Examples of Serving Sizes
Lean meats, poultry, and fish
6 or less 1 ounce (28 grams) cooked lean meat, skinless poultry, or fish
d d k / /Nuts, seeds, and dry beans(good sources of Mg++ & Ca++)
4‐5 per week 1/3 cup or 1 1/2 ounces nuts1 tablespoon or 1/2 ounces seeds
Fats and oils 2‐3 1 teaspoon soft margarine1 tablespoon low‐fat mayonnaise2 tablespoons light salad dressingtab espoo s g t sa ad d ess g1 teaspoon vegetable oil
Sweets 5 or less per week
1 tablespoon sugar1 tablespoon jelly or jam1 cup lemonade
1 cup = 240 ml
Recommending Exercise to People with HT (adopted from Department of Health Exercise Prescription) (MODULE 6)
Physical RecommendationsyActivity Profile
Frequency • Perform aerobic exercise everyday• Perform resistance exercise 2 to 3 times per week
Intensity • Aerobic and resistance exercise should be at
30
Intensity Aerobic and resistance exercise should be at least at moderate intensity
Time • 30 to 60 minutes per day of aerobic exercise

16
Special precautions on prescribing exercise to people with HT Avoid intensive isometric exercise
If HT is poorly controlled should avoid heavy physical If HT is poorly controlled, should avoid heavy physical exercise until appropriate treatment has been given and BP lowered
For patients on β-blockers and diuretics
educate them about sign and symptoms of heat intolerance and hypoglycaemia
For patients on anti-hypertensive medications such as calcium channel blocker &vasodilators
extend and monitor the cool-down period.
Patients should be informed about the cardiac prodromal symptoms
31
Drug Treatment for Patient with Hypertension (MODULE 7)
1. Concluding evidence generated from existing trials1. Concluding evidence generated from existing trials indicate that the main benefits of antihypertensive therapy in CVS outcomes are due to lowering of blood pressure per se, rather than choice of drug class, except patients with compelling indications.
2 ACEI calcium channel blockers and thiazide-2. ACEI, calcium channel blockers and thiazidetype diuretics are largely equivalent in efficacy and safety.

17
3. Beta-blockers is NOTrecommended as first line therapy:
h d t h d t i l h d th t th head-to head trials showed that they were less effective than the comparator drug at reducing major CVS events, in particular stroke
increased risk of developing diabetes, particular with the combination of thiazide-type diuretic.
4. Aldomet, alpha blockers No convincing evidence in reducing CVS
morbidity and mortality
Points to consider when prescribing anti-hypertensives (1)
1 Previous favourable or unfavourable1. Previous, favourable or unfavourable, experience of the individual patient with a given class of drugs.
2. Cost of drugs
3. Presence of TOD
l di DM th f th renal disease, DM or the presence of other coexisting CVD may either favour or limit the use of particular classes of antihypertensive drugs

18
Points to consider when prescribing anti-hypertensives (2)
4 A significant number of patients require two or4. A significant number of patients require two or more anti-hypertensive drugs in order to achieve blood pressure control. The possibility of interactions with drugs used for other conditions present in the patient.
5. There is substantial inter-individual variation in5. There is substantial inter individual variation in response to single drugs
Class of Drug Compelling Indications Compelling Contraindications
ACE Inhibitors (ACEI) Heart failure,Left ventricular dysfunction,Post myocardial infarction,Diabetic nephropathy
Pregnancy,Bilateral renal artery stenosis,Hyperkalaemia
Angiotensin II ACE inhibitor intolerance PregnancyAngiotensin IIReceptor Blockers (ARB)
ACE inhibitor intolerance Pregnancy,Bilateral renal artery stenosis,Hyperkalaemia
Alpha-Blockers Benign prostatic hypertrophy
Beta-Blockers Angina,Post myocardial infarctionTachyarrhythmias
Asthma, chronic obstructive pulmonary disease,Heart block
Calcium Elderly patients,Channel Blockers(dihydropyridine)
y p ,Isolated systolic hypertension
CalciumChannel Blockers(rate limiting, e.g. verapamil, diltiazem)
Angina Heart block
Thiazide/thiazide-likeDiuretics
Heart failure,Elderly patients,Isolated systolic hypertension
Gout

19
Annual Assessment (MODULE 8)
Aim:
to detect complications
to assess patient’s knowledge, attitude and compliance of HT and drug treatment
to advise on healthy lifestyle and cardiovascular risk factors
to ensure satisfactory BP control
38

20
Annual assessment (1)
History •Angina, neurological symptomsS ki t t•Smoking status
•Alcohol intake•Exercise•Family history of premature coronary heart disease•Patients’ concerns
Physical •Measure BP
39
Physical examination
•Measure BP•Check body mass index•Cardiovascular examination
Annual assessment (2)Laboratory investigation
General: urine for protein/albuminuric acid if on diuretic
R l f ti t t S di P t i URenal function test: Sodium, Potassium, Urea, Creatinine
Lipid Profiles: Total cholesterolTriglycerideHDL-CholesterolLDL-Cholesterol
Management •Review the risk factors and blood results
40
•Assess side effects•Encourage lifestyle modification•Explore reasons for non-compliance•Ensure patients understand HT and benefits of follow up

21
41
Summary
1. Early intervention and blood pressure control d di l bidit d t litreduce cardiovascular morbidity and mortality.
2. Lifestyle modifications and drug treatment are both important and should be individualized to maintain an optimal control of all clinical parameters.
3. Multidisciplinary team approach is needed to provide ongoing education to reduce risks, assess patients’ needs, monitor treatment responses and adherence.
Initiatives
Service gaps are being identified in the d ti f th f f kadoption of the reference frameworks
Patient education and empowerment are crucial. The patient’s version of the Reference Frameworks and other education materials are available at the website of the PCO.
42
22
One page summary on HT and DM reference frameworkOne page summary on HT and DM reference framework

23
Your support will be crucial crucial
in the promotion of reference frameworks!
THANK YOU!45