DEMENTIA NEUROCOGNITIVE DISORDER 2015 37 th Annual Family Medicine Intensive Review Course May 16,...
56
DEMENTIA NEUROCOGNITIVE DISORDER 2015 37 th Annual Family Medicine Intensive Review Course May 16, 2015 Shelia R. Cassidy, Psy.D. Asst. Professor & Clinical Neuropsychologist UAMS College of Medicing Reynolds Institute on Aging
-
Upload
brian-willis -
Category
Documents
-
view
216 -
download
2
Transcript of DEMENTIA NEUROCOGNITIVE DISORDER 2015 37 th Annual Family Medicine Intensive Review Course May 16,...
DEMENTIA NEUROCOGNITIVE DISORDER 2015
37th Annual Family Medicine Intensive Review Course
May 16, 2015
Shelia R. Cassidy, Psy.D.Asst. Professor & Clinical Neuropsychologist
UAMS College of MedicingReynolds Institute on Aging
DISCLOSURES
The following speaker of this CME activity has no relevant financial relationships with commercial interests to disclose:
SHELIA R. CASSIDY, PSYD
OBJECTIVES
1. Differentiate 4 MOST COMMON types of dementia syndromes through functional clinical presentations.
Alzheimer’s diseaseVascular dementia Lewy Body dementia Frontotemporal dementia
2. Discriminate neuropsychiatric conditions associated with dementia syndromes.
Normal AgingSTRUCTURAL BRAIN CHANGES
Thinning of the Cortical Gray MatterAge-Related changes in Neuronal MorphologyOxidative StressDNA DamageLess efficient Neural Circuits and Brain Plasticity
CHEMICAL BRAIN CHANGESDopamineSerotoninGlutamate
GENETIC CHANGESDecline in Gene expression functions
Normal Age-Related Cognitive Changes
SLIGHT DECLINES Attention/ConcentrationProcessing speed slowingWord finding “Tip of the Tongue”Memory “senior moments”Executive abstract reasoning
Compensatory strategies
INTACT FUNCTIONINGSensory MotorVisual SpatialReceptive & Expressive Language Memory for personal history & recent eventsExecutive – Intelligence, fund of information, math skills, judgment, decisional capacityIADLs
RISK FACTORS FOR ABNORMAL COGNITIVE DECLINE
Increasing AgeHypertensionCardiac diseaseDiabetesPoor nutrition Social isolation Family history of dementiaPsychological factors: stress & depression
Stages of AssessmentStage One
1. Medical & psychocial hx with pt & informant
2. Physical & Neuroexam
3. Mood & behavioral screening – SIGECAPS & Anxiety
4. Cognitive Screening- MMSE, MoCA, SLUMS, etc. Make sure vision, hearing, or accents are NOT lowering score
Stage Two
Labs – CBC, Chem 7, Liver fx, Thyroid, Metals, Vit B-12, D-3, serological test as indicated, etc.
Stage Two (cont.)Neuroimaging – dependent on findings of H & P – if over 75 & consistent with AD may not meet medical necessity
Stage Three
Treat potentially reversible conditions, medications, mood, sleep apnea, B-12 deficiency, etc.
Stage FourRescreen cognition after tx & if still abnormal – refer for Neuropsych eval
Assess effort if secondary monetary gain is present – such as disability or civil suits are present (more likely in younger patients)
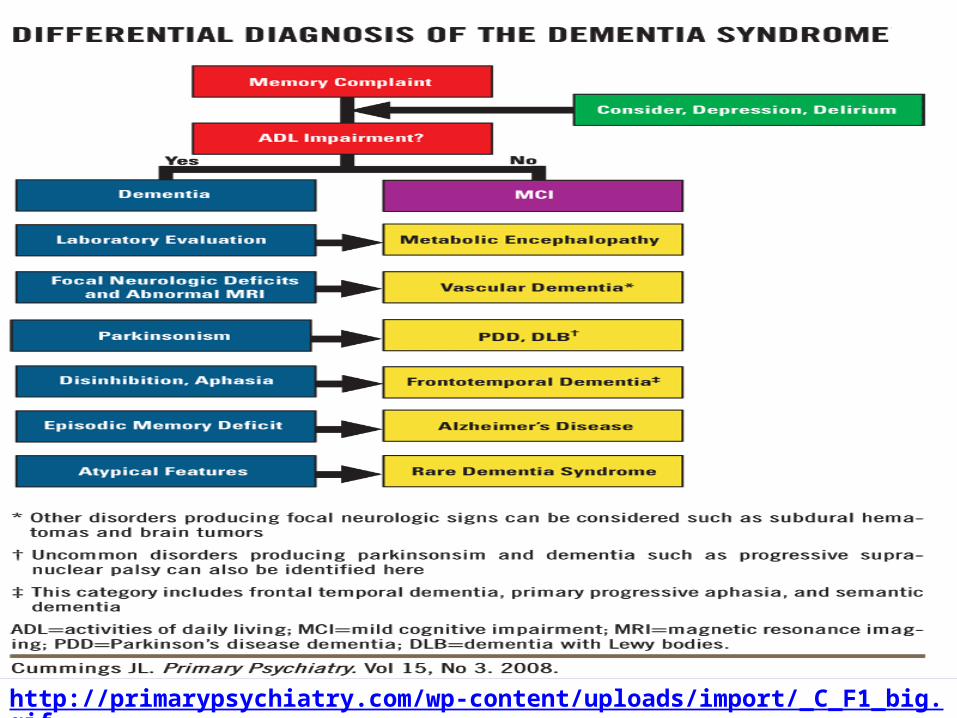
http://primarypsychiatry.com/wp-content/uploads/import/_C_F1_big.gif
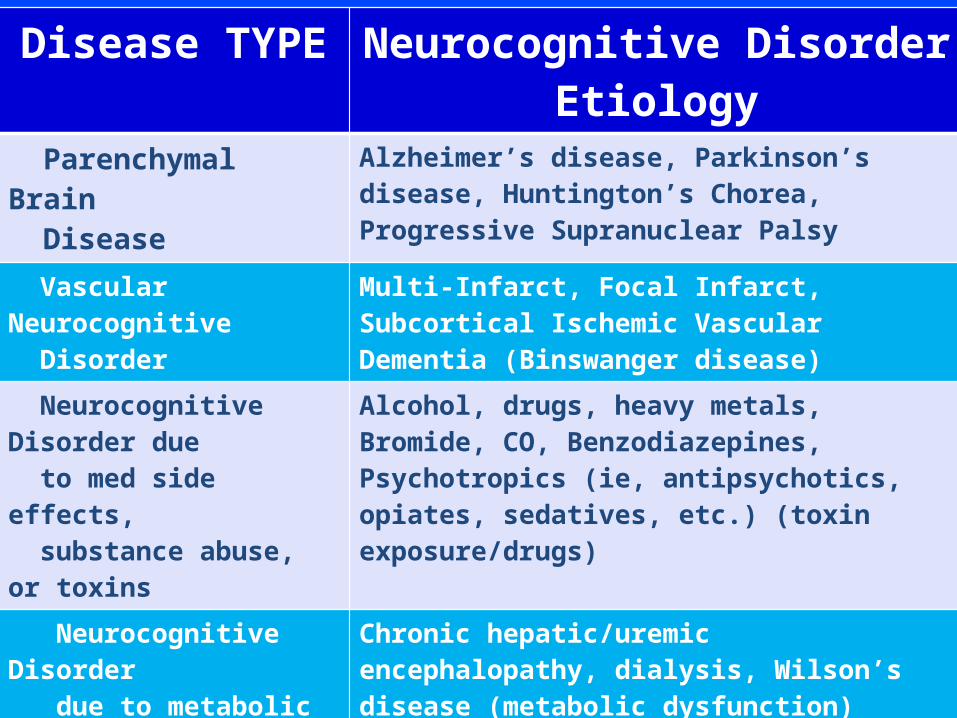
Disease TYPE Neurocognitive Disorder Etiology Parenchymal Brain Disease
Alzheimer’s disease, Parkinson’s disease, Huntington’s Chorea, Progressive Supranuclear Palsy
Vascular Neurocognitive Disorder
Multi-Infarct, Focal Infarct, Subcortical Ischemic Vascular Dementia (Binswanger disease)
Neurocognitive Disorder due to med side effects, substance abuse, or toxins
Alcohol, drugs, heavy metals, Bromide, CO, Benzodiazepines, Psychotropics (ie, antipsychotics, opiates, sedatives, etc.) (toxin exposure/drugs)
Neurocognitive Disorder due to metabolic dysfx
Chronic hepatic/uremic encephalopathy, dialysis, Wilson’s disease (metabolic dysfunction)
Neurocognitive Disorder due to Endocrine disorders
Pituitary, Parathyroisis, Thyroid, Adrenal dysfunction
Neurocognitive Disorder due to nutritional deficiencies
Pernicious anemia, Pellagra, Folic Acid, Thiamine
Neurocognitive Disorder due to Infectious dissease
HIV/AIDS, Neurosyphyllis, Chronic Meningitis, Creudtzfeldt Jacob disease (Infectious disease)
Increased Intracranial Pressure
Brain tumor, Head Trauma, Hematoma, Hydrocephalus

DELIRIUM Mild or Major NCDOnset Acute to Sub-acute InsidiousCourse Fluctuating Stable and ProgressiveDuration Hours to day (rarely weeks) Months to yearsAttention Fluctuates SteadySensorium Often impaired – can
fluctuate rapidlyClear until later stages
Etiology Usually immediate cause identified
Usually no immediate cause
Psychomotor activity
Increased, decreased, or unpredictable
Can be normal
Cognitive function
Globally impaired, poor attn span
Poor short-term memory, attn span less affected
Perception Visual hallucinations, fleeting common delusions
Simple delusions & hallucinations
Sleep/wake cycle
Disrupted, reversed Sun downing
Sun downing
Manepali, et al. Primary Psychiatry. Vol 14, No. 8, 2007http://primarypsychiatry.com/wp-content/uploads/import/0807PP_Manepalli_T1.gif
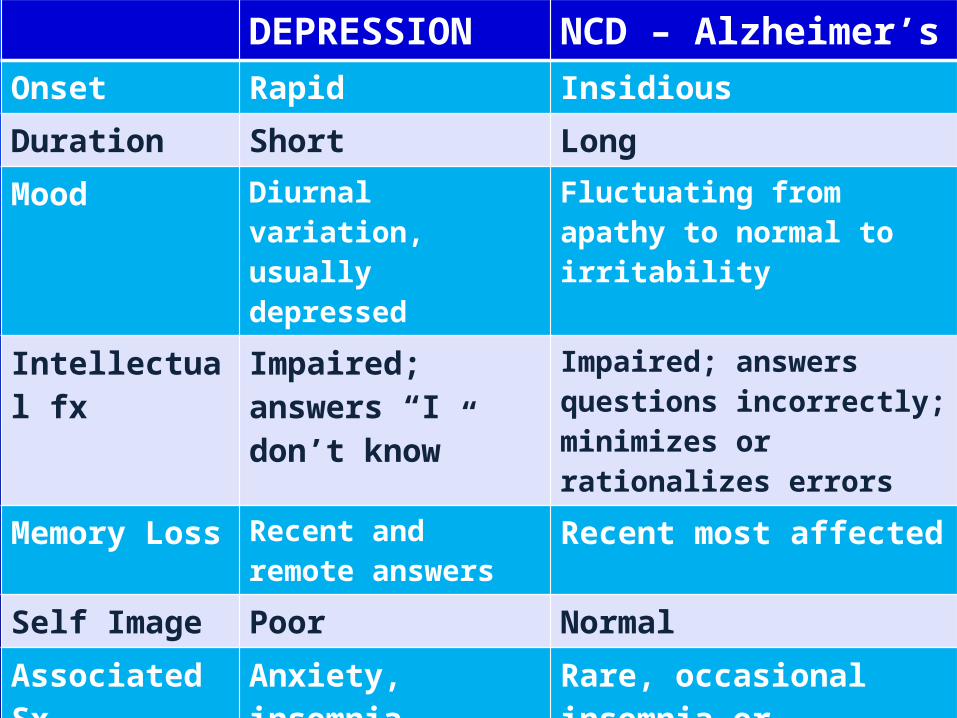
DEPRESSION NCD – Alzheimer’s Onset Rapid InsidiousDuration Short LongMood Diurnal variation,
usually depressedFluctuating from apathy to normal to irritability
Intellectual fx Impaired; answers “I don’t know”
Impaired; answers questions incorrectly; minimizes or rationalizes errors
Memory Loss Recent and remote answers
Recent most affected
Self Image Poor NormalAssociated Sx Anxiety, insomnia,
anorexiaRare, occasional insomnia or uncooperative
Consultation reason
Self-referral Family referral
Previous History Previous depression, social problems
Family hx of dementia

RECENT TERMINOLOGY CHANGES
DSM-IV
Mild Cognitive Impairment
DSM-5
Mild Neurocognitive Disorder
DSM-IV
Dementia due to …
DSM-5ICD-9/1CD-10
+Major Neurocognitive
Disorder
DSM-5 Pertinent Cognitive Domains
COMPLEX ATTENTION
EXECUTIVE FUNCTION
LEARNING AND MEMORY
LANGUAGE
PERCEPTUAL MOTOR
SOCIAL COGNITION
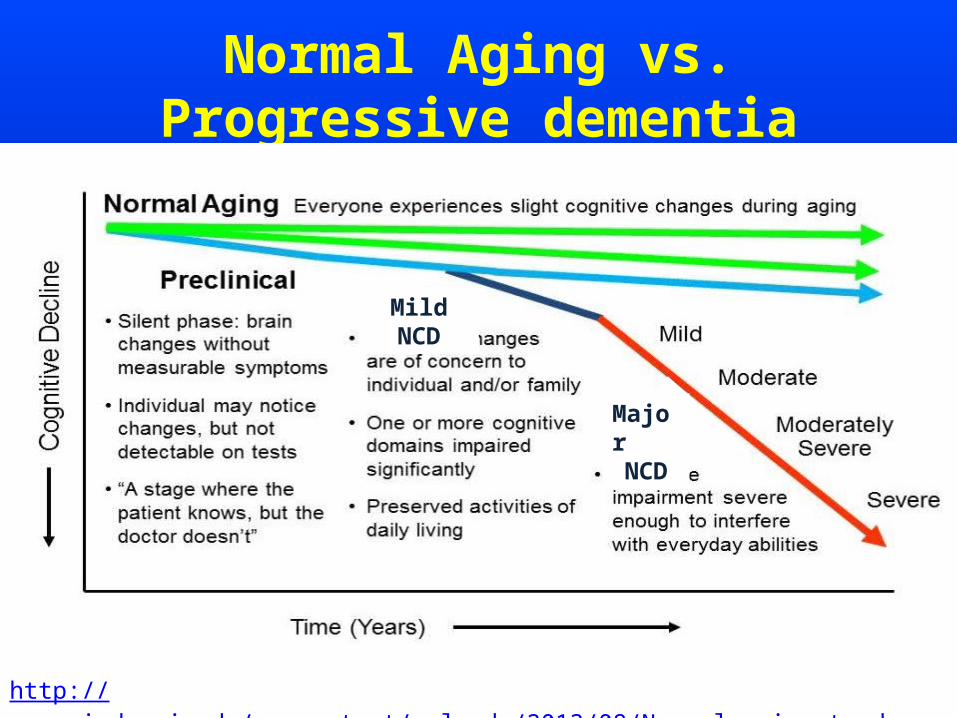
Normal Aging vs. Progressive dementia
http://www.mind.uci.edu/wp-content/uploads/2013/08/Normal-aging-to-dementia.jpg
Mild NCD
MajorNCD
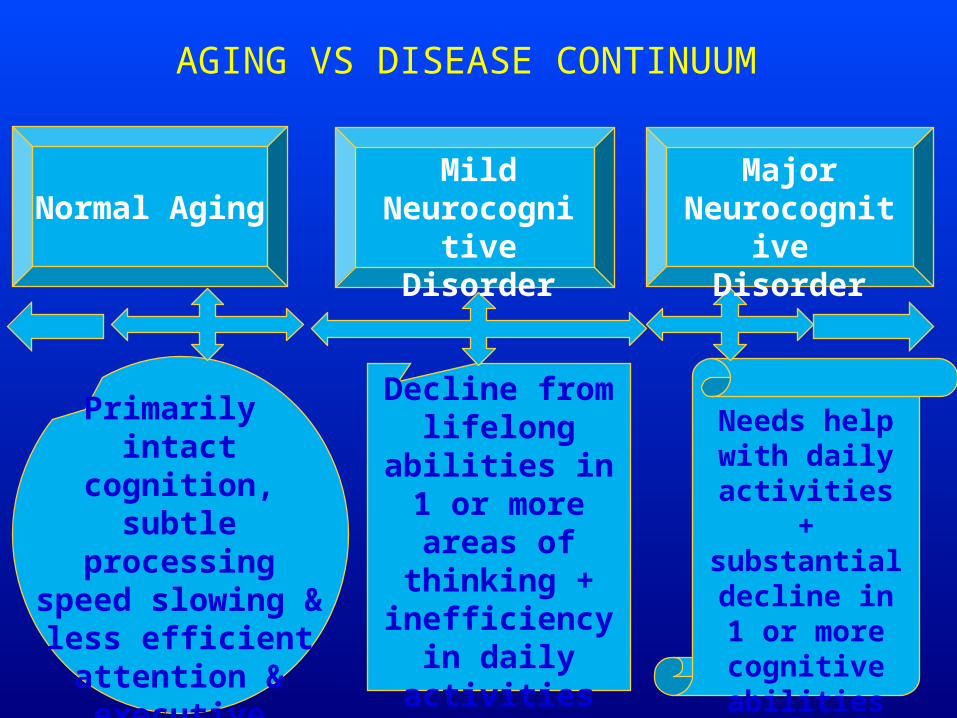
AGING VS DISEASE CONTINUUM
Normal Aging
Decline from lifelong abilities
in 1 or more areas of
thinking + inefficiency in daily activities
Needs help with daily
activities + substantial
decline in 1 or more cognitive
abilities
Major Neurocognitive
Disorder
Mild Neurocognitive
Disorder
Primarily intact cognition,
subtle processing speed slowing &
less efficient attention & executive reasoning
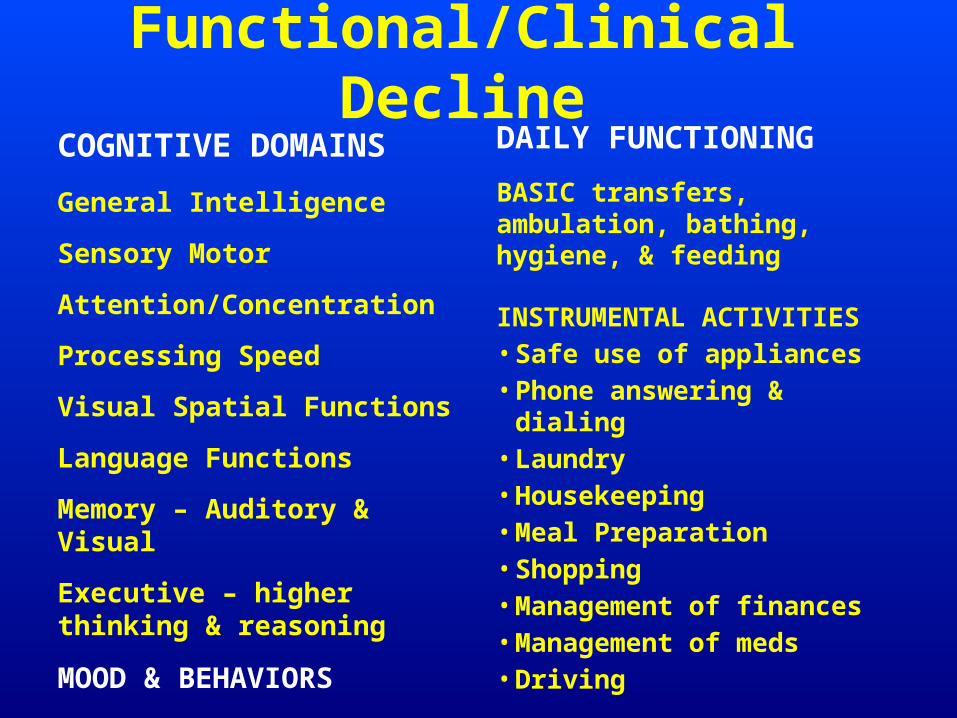
Functional/Clinical DeclineCOGNITIVE DOMAINS
General Intelligence
Sensory Motor
Attention/Concentration
Processing Speed
Visual Spatial Functions
Language Functions
Memory – Auditory & Visual
Executive – higher thinking & reasoning
MOOD & BEHAVIORS
DAILY FUNCTIONING
BASIC transfers, ambulation, bathing, hygiene, & feeding
INSTRUMENTAL ACTIVITIES• Safe use of appliances• Phone answering & dialing• Laundry• Housekeeping• Meal Preparation• Shopping• Management of finances• Management of meds• Driving
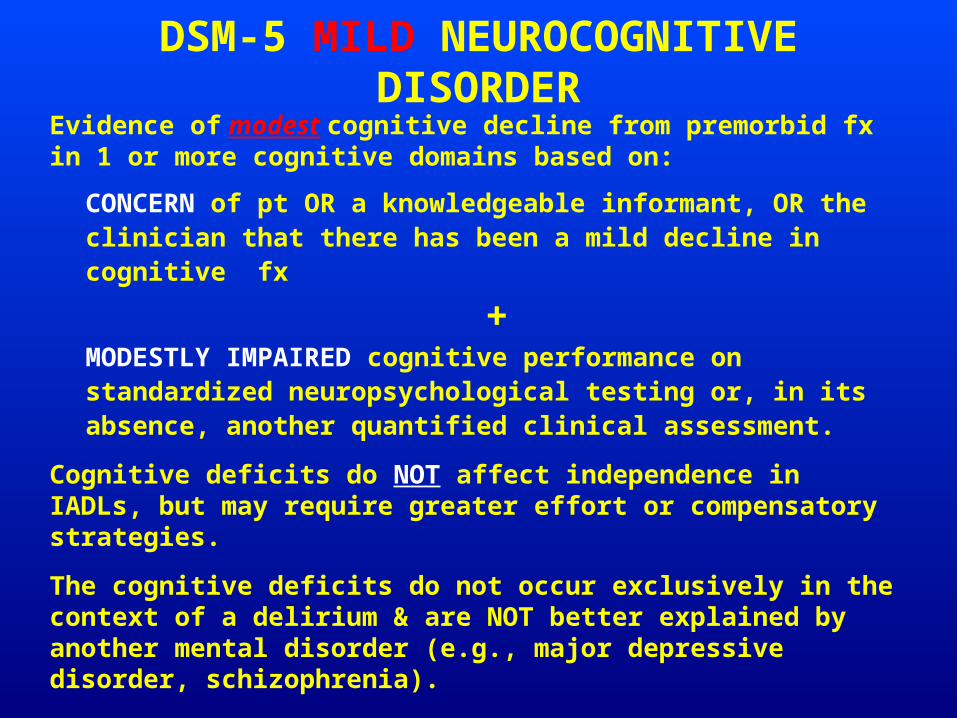
DSM-5 MILD NEUROCOGNITIVE DISORDEREvidence of modest cognitive decline from premorbid fx in 1 or more cognitive domains based on:
CONCERN of pt OR a knowledgeable informant, OR the clinician that there has been a mild decline in cognitive fx
+MODESTLY IMPAIRED cognitive performance on standardized neuropsychological testing or, in its absence, another quantified clinical assessment.
Cognitive deficits do NOT affect independence in IADLs, but may require greater effort or compensatory strategies.
The cognitive deficits do not occur exclusively in the context of a delirium & are NOT better explained by another mental disorder (e.g., major depressive disorder, schizophrenia).
DSM-5 MAJOR NEUROCOGNITIVE DISORDER A. Evidence of significant cognitive decline from previous abilities in one or more cognitive domains based on:
1. Concern of pt OR a knowledgeable informant OR clinician that there has been a significant decline in cognitive function; AND2. SUBSTANTIALLY IMPAIRED cognitive performance on standardized neuropsychological testing or, in its absence , another quantified clinical assessment.
B. Cognitive deficits INTERFERE with independence in activities. C. Cognitive deficits not due exclusively to a delirium.
D. Cognitive deficits not better explained by another mental disorder (e.g., major depressive disorder, schizophrenia).
Major NCD
SPECIFY: 1. Without behavioral disturbances 2. With behavioral disturbances: if cognitive disturbance plus a clinically significant behavioral disturbance psychosis, mood disturbance, agitation, or apathy.
SPECIFY:1. Mild: difficulties limited to IADLs2. Moderate: difficulties with basic activities of daily living3. Severe: fully dependent

Neuro-CognitiveDisorder due to
Alzheimer’sdisease
Vascular Neuro-
cognitiveDisorder
Neuro-cognitive disorder
with Lewy
Bodies
OTHERS:Parkinson’sDepressionSeizuresNPHTraumaInfectionMetabolicDrugs/ToxinsNeoplasmsAnoxia
Fronto-Temporal Neuro-Cognitive
Disorder
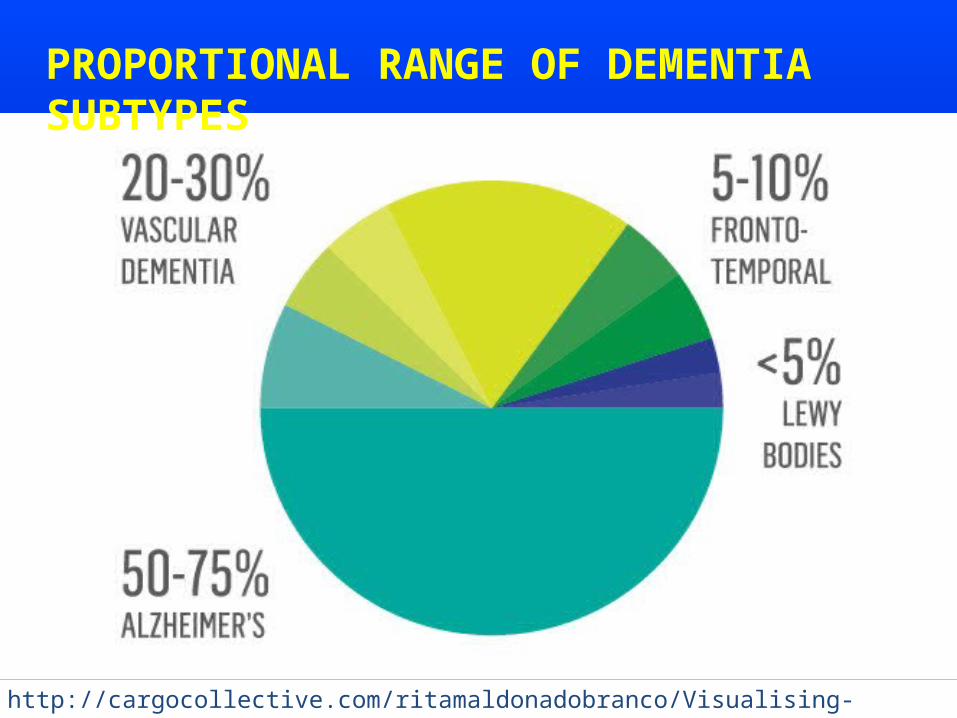
http://cargocollective.com/ritamaldonadobranco/Visualising-dementia
PROPORTIONAL RANGE OF DEMENTIA SUBTYPES

“Alzheimer’s disease is bankrupting America”
AD – 6th-leading cause of death in US.
AD - only disease in top 10 causes of death in America without a way to prevent it, cure it or significantly slow its progression.
Currently $172 billion is spent caring for people with AD & other dementias.
By 2050, the costs may reach over $1 trillion without adjusting for inflation.
Almost 1/2 of all AD costs are paid by Medicare & more than one in every six Medicare dollars is spent on a pt with AD
Between 2010 & 2050, Medicare costs Medicare of caring for a pt with AD will increase over 600 % & out of pocket costs to families will grow more than 400 %.
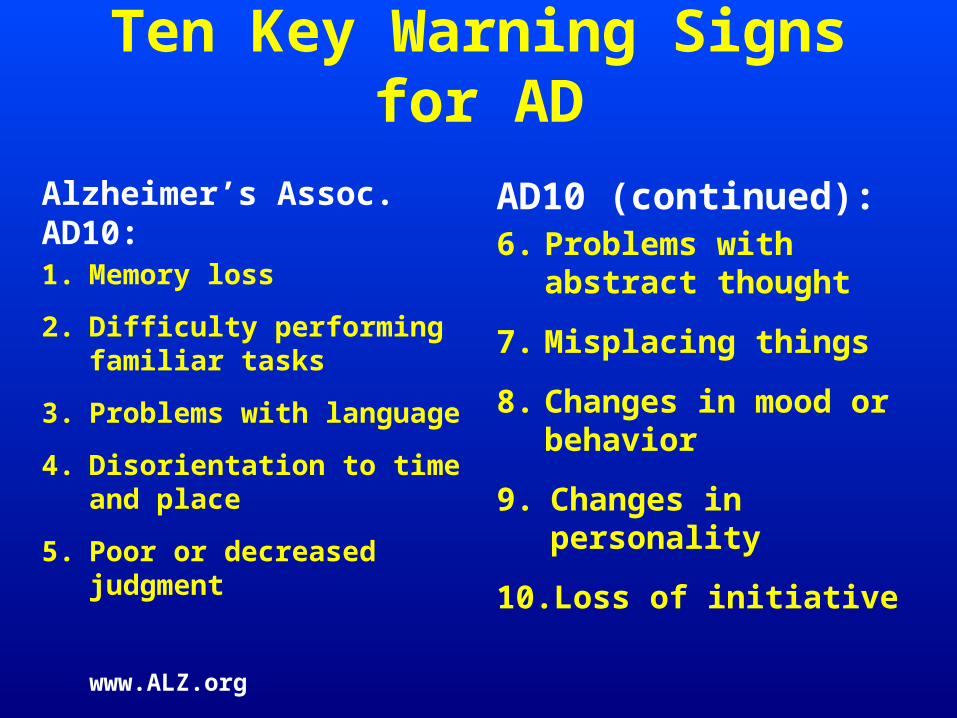
Ten Key Warning Signs for AD
Alzheimer’s Assoc. AD10:1. Memory loss
2. Difficulty performing familiar tasks
3. Problems with language
4. Disorientation to time and place
5. Poor or decreased judgment
AD10 (continued):6. Problems with abstract
thought
7. Misplacing things
8. Changes in mood or behavior
9. Changes in personality
10. Loss of initiative
www.ALZ.org
Alzheimer’s disease facts and figures
5.3 million Americans have AD - 5.1 million are aged 65 and over (1 in 8).
By 2050, 13.5 to 16 million in US will have AD
Nearly 1 in 2 aged 85 and over has the disease.
Every 70 seconds, someone in US develops Alzheimer’s.
In 2050, every 33 secs an American will develop AD
Survival is an average of 4 to 8 years after diagnosis with AD, but many live for as long as 20 years with the disease.
On average, 40 % of person’s years with AD are in the most severe stage of the disease.
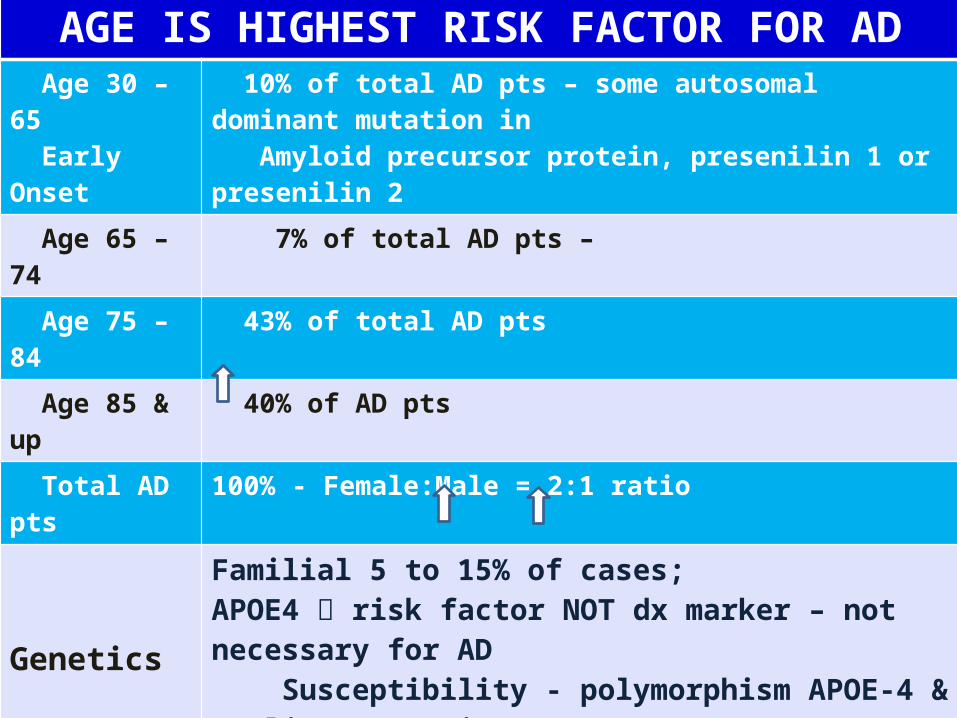
ALZHEIMER’S DISEASEAGE IS HIGHEST RISK FACTOR FOR AD
Age 30 – 65 Early Onset
10% of total AD pts – some autosomal dominant mutation in Amyloid precursor protein, presenilin 1 or presenilin 2
Age 65 – 74 7% of total AD pts – Age 75 – 84 43% of total AD pts
Age 85 & up 40% of AD pts
Total AD pts 100% - Female:Male = 2:1 ratio Genetics
Familial 5 to 15% of cases; APOE4 risk factor NOT dx marker – not necessary for AD Susceptibility - polymorphism APOE-4 & earlier onset in homozygous individuals. Down’s syndrome (trisomy 21 gene) AD if survive to midlife
Risk Factor / Disease Course
Vascular risk factors AD by cerebrovascular pathology or thru direct effects on AD pathologyTypical course 8 to 10 yrs after dx, but some live 20 yearsLate stage AD become mute and bed boundEarly onset more likely to survive full courseLate onset dx more complex multiple comorbiditiesDeath commonly due to aspiration
(Weuve et al 2012
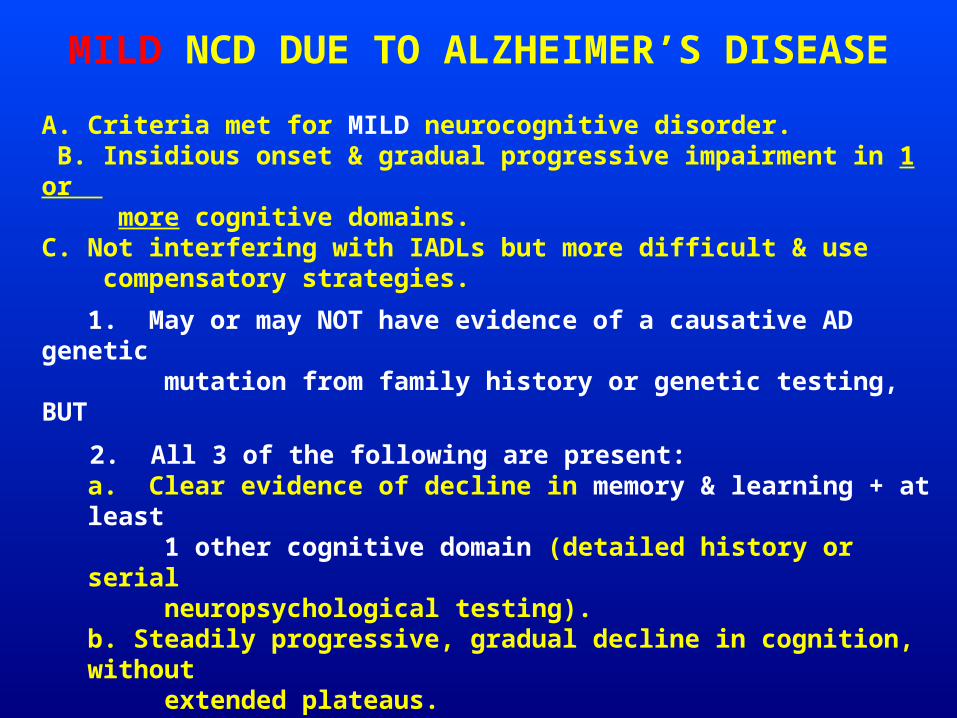
MILD NCD DUE TO ALZHEIMER’S DISEASE
A. Criteria met for MILD neurocognitive disorder. B. Insidious onset & gradual progressive impairment in 1 or more cognitive domains. C. Not interfering with IADLs but more difficult & use compensatory strategies.
1. May or may NOT have evidence of a causative AD genetic mutation from family history or genetic testing, BUT
2. All 3 of the following are present: a. Clear evidence of decline in memory & learning + at least 1 other cognitive domain (detailed history or serial neuropsychological testing). b. Steadily progressive, gradual decline in cognition, without extended plateaus. c. No evidence of mixed etiology
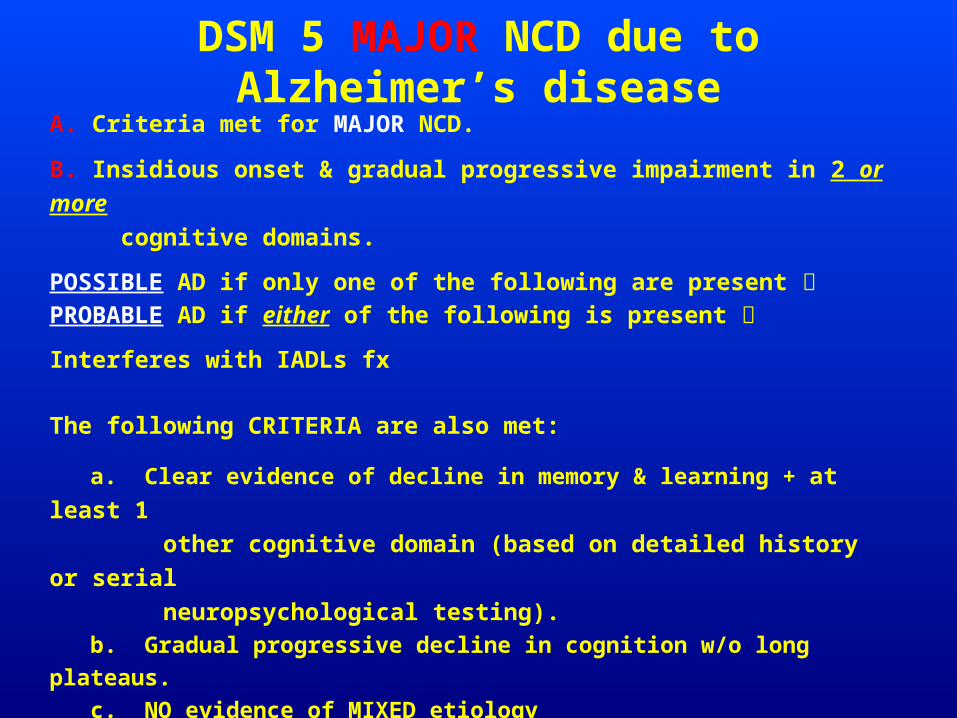
DSM 5 MAJOR NCD due to Alzheimer’s diseaseA. Criteria met for MAJOR NCD.
B. Insidious onset & gradual progressive impairment in 2 or more cognitive domains.
POSSIBLE AD if only one of the following are present PROBABLE AD if either of the following is present
Interferes with IADLs fx
The following CRITERIA are also met:
a. Clear evidence of decline in memory & learning + at least 1 other cognitive domain (based on detailed history or serial neuropsychological testing). b. Gradual progressive decline in cognition w/o long plateaus. c. NO evidence of MIXED etiology
NEUROPSYCHIATRIC FEATURES AD~ 80% of pt with MAJOR NCD due to Alzheimer’s disease behavioral & psychological SX – that are also frequent at the MILD stage.
Behavioral symptoms = or more distressing than cognitive SX & are frequently the reason health care is sought.
MILD STAGE NCD due to AD depression & apathy
MODERATE STAGE NCD due to AD psychotic features, irritability, agitation, combativeness, sundowning & wanderingRummaging, hiding, & hoardingDelusions: Paranoia & persecutory themesLATE STAGE NCD due to AD gait disturbance, dysphagia, incontinence, myoclonus, and seizures
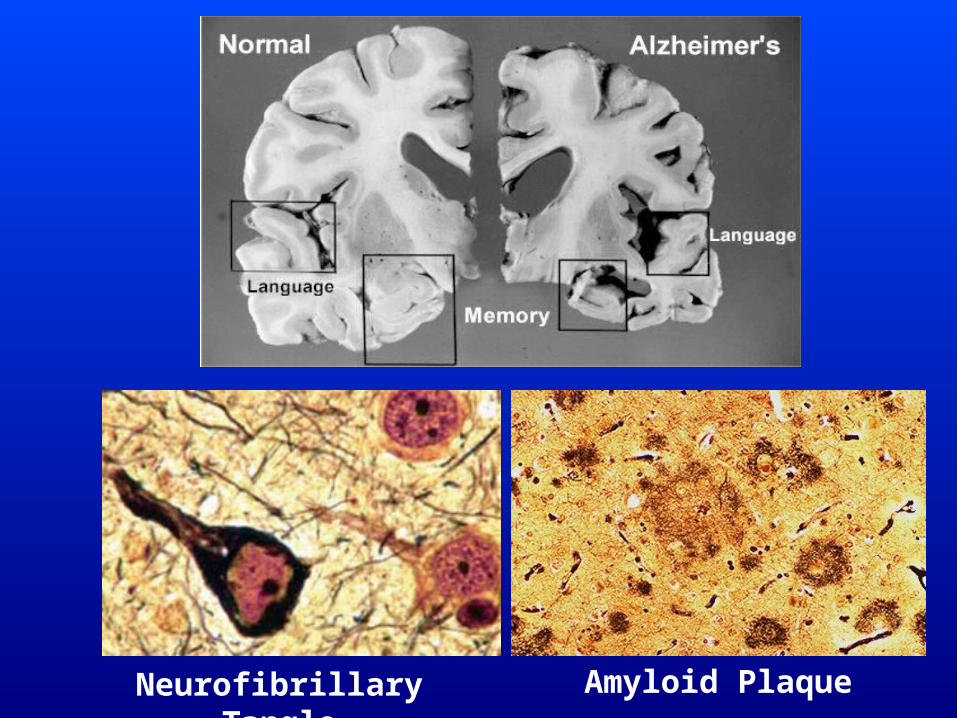
Neurofibrillary Tangle Amyloid Plaque
http://www.drugdevelopment-technology.com/projects/caprosinol/images/2-graph.jpg
Biomarkers in the GameInvasive, time consuming, & expensive• Structural & functional magnetic resonance imaging• Cerebrospinal fluid tau and amyloid-β levels• Pittsburg compound amyloid imaging or “inflammaging”
Blood based biomarkers will likely become more pragmatic
Mark Mapstone, Howard Federoff et al @ Georgetown University 525 people aged 70 & over for 5 years.74 developed aMCI or mild AD46 of the 74 were incidental cases28 of 74 (the "converters") converted from nonimpaired memory status at entry to aMCI or AD, over an average time of 2.1 years.Validated set of 10 peripheral blood lipids that predicted phenoconversion to either amnestic MCI or AD within a 2–3 year timeframe with a sensitivity and specificity of 90% accuracy

NCD pharmacological treatment for AD
Acetylcholinesterase Inhibitorsdonepezil (Aricept)rivastigmine (Exelon)galantamine (Razadyne)tacrine (Cognex) – less used due to side effects
memantine (Namenda) – NMDA antagonist
Vascular Neurocognitive Disorder
2nd most common cause of dementia in elders
Potentially preventable condition/slow progression tight BP & BG control (90 – 150 mg/dL) + cholesterol lowering therapyHighest 5-year mortality rate (61%) of all dementias
TYPES:1. CADASIL (Cerebral autosomal dominant arteriopathy with
leukoencephyalopathy) gene mutation Notch 3
2. Multi-Infarct Dementia
3. Subcortical Ischemic Vascular Dementia (SIVD)Beers MH, Porter RS, Jones TV, et al. The Merck Manual of Diagnosis and Therapy. 18th ed. Whitehouse Station, NJ: Merck Research Laboratories; 2006:1635,1727,1808-1822,2541-2545.
What is Dementia? National Institute of Neurological Disorders and Stroke. National Institutes of Health. Available at: http://www.ninds.nih.gov/disorders/dementias/dementia.htm. Accessed March 31, 2015
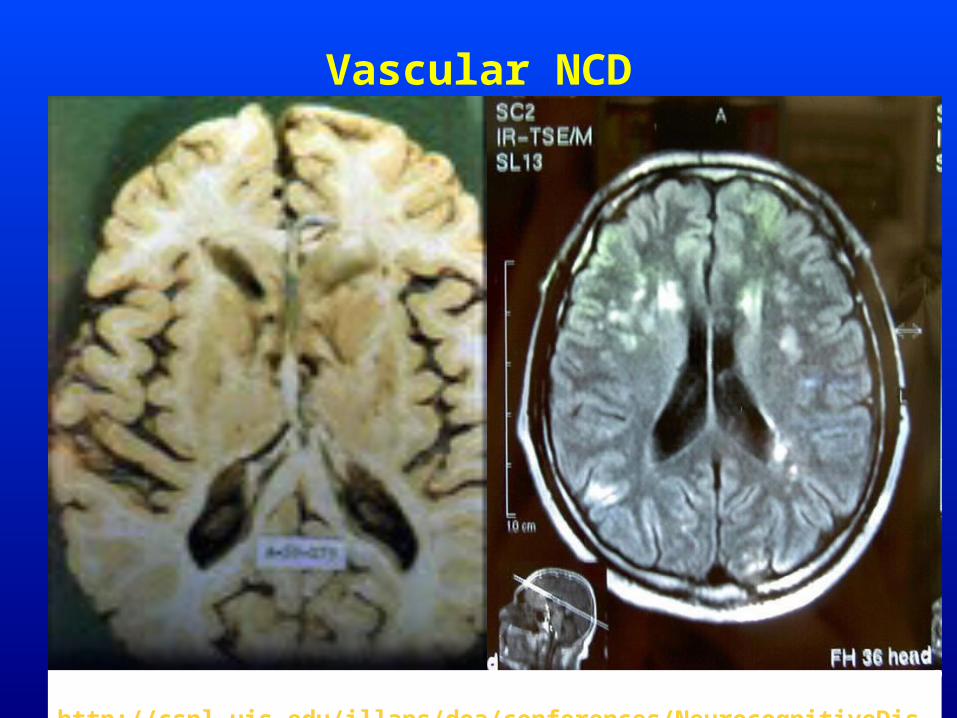
Vascular NCD
http://cspl.uis.edu/illaps/doa/conferences/NeurocognitiveDisorders.Chicago.2014.pptx.
MAJOR OR MILD VASCULAR NEUROCOGNITIVE DISORDER
Criteria are met for major or mild NCD
Clinical features are consistent with a vascular etiology, as suggested by the following:
Onset of cognitive deficits is temporally related to 1 or more cerebrovascular eventsEvidence for decline is prominent in complex attention (including processing speed) and frontal-executive function.
There is evidence of the presence of cerebrovascular disease from history, physical examination, and/or neuroimaging considered sufficient to account for the neurocognitive deficits.
The symptoms are not better explained by another brain disease or systemic disorder.
Possible vs. Probable Vascular NCDPOSSIBLE vascular NCD symptoms meet clinical criteria but NO neuroimaging +TEMPORAL relationship of the neurocognitive syndrome with 1 or more cerebrovascular events is not established.
PROBABLE vascular NCD is diagnosed if 1 of the following is present
Clinical criteria supported by neuroimaging evidence of significant parenchymal injury attributed to cerebrovascular disease (neuroimaging-supported).
The neurocognitive syndrome is temporally related to one or more documented cerebrovascular events.
Both clinical & genetic (CADASIL) evidence of cerebrovascular disease is present.
Neuropsychiatric features of Vascular Neurocognitive Impairment
• Personality change• Apathy / Dependent behaviors / lack of insight• Impaired social communication with family and friends• Mistrust• Repetitive fixated behaviors• Neglect of hygiene & appearance• Guilt or shame• Generalized Anxiety• Frequently Depressed• Agitation /Anger /Disrespectful • Increased risk of self harm – impulsivity, dangerous risk-taking• When severe, may have delusions, hallucinations, delirium
Neurocognitive Disorder due to Lewy BodiesCriteria are met for major or mild NCD.Insidious onset & gradual progression.Combination of CORE dx features & suggestive dx features for either PROBABLE or POSSIBLE NCD with Lewy bodies.PROBABLE major or mild NCD with Lewy bodies, the individual has 2 core features, or 1 suggestive feature with 1 or more core features. POSSIBLE major or mild NCD with Lewy bodies, the individual has only 1 core feature, or 1 or more suggestive features.
CORE diagnostic features:FLUCTUATING cognition with pronounced variations in attention & alertness.RECURRENT visual hallucinations that are well formed and detailed.SPONTANEOUS features of parkinsonism, with onset subsequent to the development of cognitive decline.SUGGESTIVE diagnostic features:
• Meets criteria for rapid eye movement sleep behavior disorder• Severe neuroleptic sensitivity
Disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder.
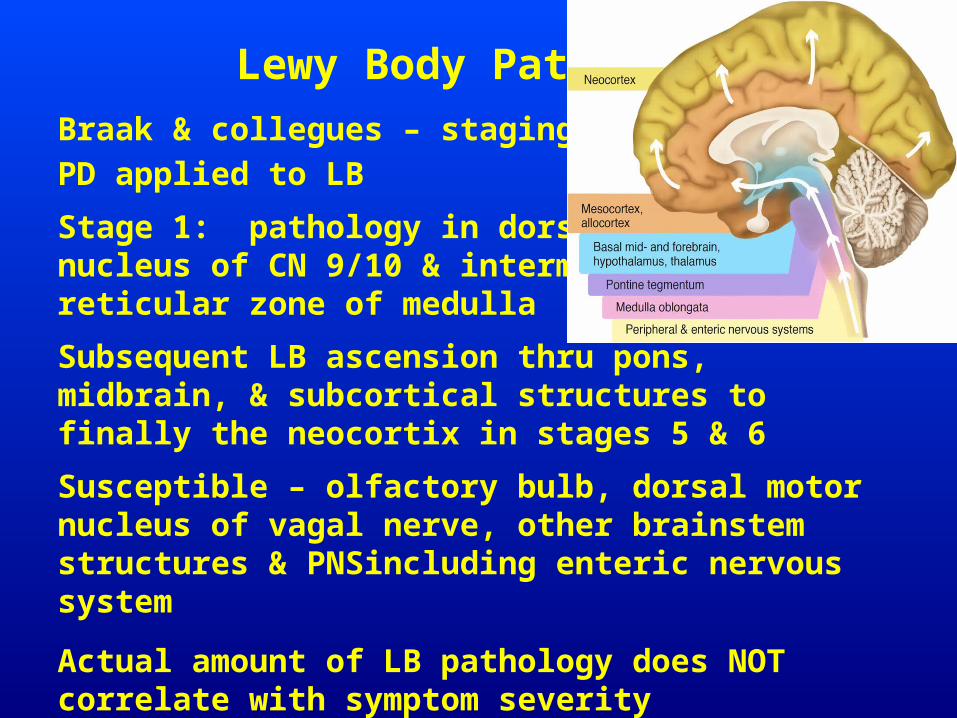
Lewy Body PathologyBraak & collegues – staging system in PD applied to LB
Stage 1: pathology in dorsal motor nucleus of CN 9/10 & intermediate reticular zone of medulla
Subsequent LB ascension thru pons, midbrain, & subcortical structures to finally the neocortix in stages 5 & 6
Susceptible – olfactory bulb, dorsal motor nucleus of vagal nerve, other brainstem structures & PNSincluding enteric nervous system
Actual amount of LB pathology does NOT correlate with symptom severityDonaghy and McKeith The Clinical characteristics of dementia with Lewy bodies and a consideration of prodromal diagnosis Alzheimer's Research & Therapy 2014, 6:46 http://alzres.com/content/6/4/46
Lewy Body Pathology (cont.)
DLB & PDD pathological differences - DLB - higher amyloid plaque deposition in the striatum
More αSyn deposition in CA2/3 area of hippocampus & higher frontal cortical 5-HT1A receptor density
DLB less cell loss - substantia nigra & minimal D2 receptor up-regulation in striatum
Coexisting LB & AD pathology (amyloid-beta (Aβ) and tau) postmortem
DLB < structural brain changes compared with AD
MILD OR MAJOR NEUROCOGNITIVE DISORDER WITH LEWY BODIES
Affects 2ce as many men
Fluctuations in alertness, attention, & cognition
Decline in smell (hyposmia)
Postural Dizziness
Constipation
Parkinsonian symptoms - muscles that go abnormally rigid or tremble uncontrollably
Relative preservation of short-term memory unlike AD
Later in course - memory loss, poor judgment, and confusion
Supportive features of NCD due to Lewy Bodies
Repeated Falls & Syncope
Transient unexplained loss of consciousness
Severe autonomic dysfunction (orthostatic hypotension, incontinence)
Relative preservation of medial temporal structures on CT or MRI
Generalized low uptake on PET / SPECT perfusion scan with reduced occipital activity
Abnormal low uptake on MIBG myocardial scintigraphy
Prominent slow wave activity on EEG with transient temporal lobe sharp waves
Neuropsychiatric features of NCD due to Lewy Bodies
Rapid Eye Movement (REM) sleep d/o – parasomnia characterized by enactment of dreams (kicking, punching) that often results in injury
Systematized Delusional thinking
Ego Syntonic well formed visual hallucinations
Hallucinations in other modalities
Depression – ¼ pts
Anxiety – ¼ pts
Frontotemporal Neurocognitive Disorder (FTNCD)
Criteria met for major or mild neurocognitive disorder
Disturbance - insidious onset and gradual progressionEither (1) or (2):
BEHAVIORAL VARIANT:3 or more of the following behavioral symptoms:
Behavioral disinhibitionApathy or inertiaLoss of sympathy or empathyPerseverative, stereotyped or compulsive/ritualistic behaviorHyperorality and dietary changes
Prominent decline in social cognition and/or executive abilities.
LANGUAGE VARIANT:PROMINENT DECLINE in language ability, speech production, word finding, object naming, grammar, or word comprehension
Relative sparing of learning and memory & perceptual-motor function.
Frontotemporal NCD (cont.)
The disturbance is not better explained by cerebrovascular disease, another neurodegenerative disease, the effects of a substance, or another mental, neurological, or systemic disorder.PROBABLE frontotemporal neurocognitive disorder is diagnosed if either of the following is present:
Evidence of a causative Frontotemporal neurocognitive disorder genetic mutation, from family history or genetic testing.Evidence of disproportionate frontal and/or temporal lobe involvement on neuroimaging.
POSSIBLE frontotemporal neurocognitive disorder is dx’d if: NO evidence of a genetic mutation NO neuroimaging has not been performed.
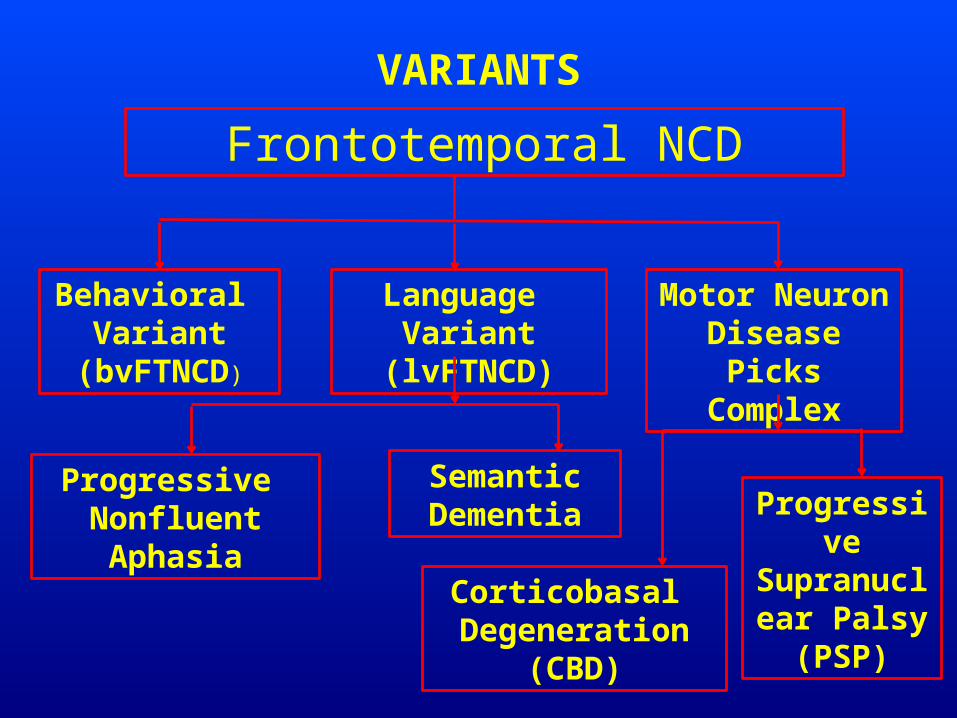
VARIANTS
Frontotemporal NCD
Behavioral Variant
(bvFTNCD)
Language Variant (lvFTNCD)
Motor Neuron Disease
Picks Complex
Progressive Nonfluent Aphasia
Semantic Dementia
Corticobasal Degeneration (CBD)
Progressive Supranuclear
Palsy (PSP)
BEHAVIORAL VARIANT Frontotemporal Neurocognitive Disorder
60 % of FTNCD pts have (bvFTNCD)
Dysfunction in frontal & temporal lobes
Diminished social skills, emotional regulation, personal conduct, & self awareness
Mood changes – stubbornness, emotinal coldness or distance, apathy, & selfishness
Initially limited confusion about place or time
FTNCD (cont.)
Inability to control impulsive urges /impulsive behavior
Poor decision-making
Loss of the ability to empathize with others
Decrease in personal motivationChanges in grooming or eating habits
Language- or speech difficulties – aphasia or dysarthria
Loss of the ability to use words that make sense for a given conversational context
Less frequently FTNCD – impaired body movement Rigid or trembling & weak muscles Loss of the ability to coordinate the activity of different muscles Swallowing problems.

Frontotemporal Neurocognitive Disorder Language Variant PROGRESSIVE NONFLUENT APHASIA (PNFA)
20% of FT NCD cases – temporal lobe dysfunction
Receptive language deficits – difficulty understanding complex sentences.
Expressive language deficits - difficulty producing language fluently though they still know the meaning of the words they are trying to say; talk slowly, have trouble saying words, difficulty talking in groups of people or on the telephone
Eventually, many pts with PNFA develop severe Parkinsonian symptoms overlapping with Progressive Supranuclear Palsy (PSP) & Corticobasal degeneration (CBD) – inability to move eyes side-to-side, muscle rigidity in arms & legs, falls, & weakness of muscles around the throat.
FT NCD SEMANTIC DEMENTIA (SD)
20 % of FTD cases – Temporal lobe dysfunction
Left Hemispheric onset – loss of meaning for words, decline in reading & spelling, decline in people’s names; Memory not affected until later; intact orientation to place & time, intact muscle control
Right Hemispheric onset – trouble recalling faces of friends & familiar people; deficits understanding emotions of others; loss of empathy
Eventually both hemispheres will become dysfunctional
SD patients eventually develop behavioral problems – disinhibition, apathy, diminished insight
FT NCD with Motor Neuron Disease
15 % of pts with FTNCD also develop motor neuron disease (FTNCD-MND)
MND affects motor nerve cells in spinal cord, brain stem, and cerebral cortexMotor sx = tremors, jerks (chorea or myoclonus), excessive startle response, seizures
More frequently found in pts with bvFTNCD
Rare in SD or PNFA
Most common MND is amyotrophic lateral sclerosis (ALS). Often pts with ALS have behavioral or cognitive problems similar to those seen in FTNCD.
MND Symptoms: slurring of speech, difficulty swallowing, choking, limb weakness, or muscle wasting.
Often a family history of the disease
Neuropsychiatric features of FTNCD
Inattention
Low Motivation, Apathy or inertia
Poor Insight
Behavioral disinhibition
Aggression
Impulsivity
Sexual Impropriety
Loss of sympathy or empathy
Perseverative, stereotyped or compulsive behavior
Hyperorality and dietary changes

http://openi.nlm.nih.gov/imgs/512/143/3104685/3104685_jmdh-4-125f3.png
Mild or Major Neurocognitive Disorder
Mild Neurocognitive DisorderSubjective cognitive complaint corroborated by informant Objective cognitive impairment, preserved general cognition INTACT IADLs
Potentially Reversible Causes
Depression, drug side effects, metabolic d/os, vitamin deficiency, infectious disease, neoplams NPH, subdural hematoma
Gradual onset, progressive decline, ADL deficits, memory loss, aphasia, apraxia, agnosia, executive dysfunction
Acute onset, stepwise decline, vascular risks, frontal deficits, neurological signs, neuroimaging findings
Hallucinations, parkinsonism, attn / arousal fluctuations, executive dysfx, visuospatial deficits
Early onset, family history, executive dysfx, disinhibition, personality change, aphasia (fluent / non-fluent
mNCD AD
Vascular NCD
NCD LB or PD
bvFTNCDlvFTNCD
PREVENTION & NONPHARMACOLOGICAL TREATMENT
Controlling risk factors for chronic disease, such as heart disease and diabetes (e.g., tight control of blood cholesterol and blood pressure at healthy levels & maintaining a healthy weight)
Enjoying Consistent exercise regimen and physical activity
Reduce stress – limit caffeine, meditation routine &/or MINDFULNESS
Eating a healthy lifestyle diet - including plenty of vegetables & fruits, such as the Mediterranean diet
Engage in intellectually stimulating activities and maintaining close social ties with family, friends, and community
Don’t smoke & Limit alcohol intake
Get 7 to 9 hours of sleep each night
Do activities that require quick responses – ping pong, tennis, board games, computer games
Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE)
2,802 healthy adults ages 65 & up living independently – 4 Groups @ 10 computer sessions
1. Memory 26% improved2. Reasoning 74% improved3. Processing Speed 87% improved4. Control group
11 mos later 60% 75-minute “booster” sessions
5 years later Groups 1 - 3 > controls
REASONING & PROCESSING SPEED groups
Any Questions?
Thank you!