Obstetric operations: induced abortion, forceps delivery ...
Upload
rombergs-signCategory
view
118download
3
Charmaine G. Abalos ชาร์�เมน

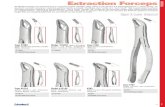
Forceps Two branches4 components
BladeShankLock Handle

Components Blade
- Fits according to the fetal head- Oval, elliptical, fenestrated, solid - Cephalic curve – concavity of the articulated blade
corresponds to the fetal head- Pelvic curve – corresponds more or less the axis of
the birth canal
Shank- Provides the length of the instrument- It connects the blade to the handle

Components Handle
- Applies traction
Lock - Articulation between shanks- English lock – is commonly used; consist of a socket
located on the shank at the junction with the handle, into which it fits a socket similarly located on the opposite shank
- Sliding lock – used in some forceps (Kielland forceps)- French lock – used in Barton forceps

FunctionsTraction
Direction must be along the pelvic curvatureDirection of pull should be perpendicular to the
plane of the level of which it is being applied
Rotation Carried out best in the midpelvisHandles should be swung to a wide arc to reduce
the arc of the bladeEasier and lowers the incidence and extent of
vaginal lacerations

Different Types of Forceps Simpson forceps
- Fenestrated blade- Wide and parallel shanks- Delivered fetus with molded head- Nulliparous women
Tucker-Mclane- Blade is solid- Crossing and narrow shank- Deliver fetus with rounded head- Multiparous women
Barton – for deep transverse arrest and POP


Different Types of Forceps Kielland
- Sliding lock- Allows the shank to move forward and backward
independently- Used in deep transverse arrest, or POP
Piper – for the aftercoming head in breech deliveries
Elliot - cephalic curve is more curved and short- Used for less molded head
Bailey-Williamson – long shanks

Selection of Proper ForcepsSize of the fetal headDegree of moldingStation Position

Definition:Outlet forceps delivery – fetal head must be on
the perineal floor with the sagittal suture no more than 45 degrees from AP diameter
Trial forceps delivery – refers to application with the full knowledge that a certain degree of disproportion existing at the midplane may make delivery difficult, with unacceptable perinatal or maternal morbidity
Failed forceps delivery – unexpected unsuccessful attempts at instrumental delivery

Classification of Forceps DeliveriesProcedure Criteria
Outlet
Low
Midpelvic
High
1. Scalp is visible at the introitus without separating the labia
2. Fetal skull has reached the pelvic floor
3. Sagittal suture is in AP diameter or R or LOA or P position
4. Fetal head is at or on the perineum
5. Rotation does not exceed 45 degrees
Leading point of fetal skull is at station
> +2 cm, and not on pelvic floorRotation is 45 degrees or less (L or
ROA to OA, or L or ROP to OP)Rotation is greater than 45 degrees
Station above +2 cm but head is engaged
Not included in classification

Station above +2 cm but head is
engaged
Leading point of fetal skull is at station
> +2 cm, and not on pelvic floor
Rotation is 45 degrees or less (L or ROA
to OA, or L or ROP to OP)
Rotation is greater than 45 degrees
1. Scalp is visible at the introitus without
separating the labia
2. Fetal skull has reached the pelvic floor
3. Sagittal suture is in AP diameter or R or LOA or
P position
4. Fetal head is at or on the perineum
5. Rotation does not exceed 45 degrees

Forceps Delivery Classification and Instruments Used
Outlet forceps SimpsonsElliot
Low forceps Elliot <45° rotationKielland >45° rotationTucker-Mclane
Midforceps Kielland or MclaneBreech Pipers

Preparation for Forceps Delivery
• Regional analgesia or general anesthesia usually is preferred for low-forceps or midforceps procedures
• Bladder must be emptied• Experienced operator

Prerequisite Head must be engagedVertex presentation or mentum anteriorPosition must be knownCervix should be fully dilatedBOW rupturedNo CPD

Indications Prolong 2nd stage of labor
- Nulli – after 2 hours w/o or 3 hours w/ anesthesia- Multi – after 1 hour w/o or 2 hours w/ anesthesia
Maternal - Heart disease- Maternal exhaustion- Previous CS
Fetal - Cord prolapse- Abruptio placenta- Fetal distress

Contraindications Any contraindications to vaginal deliveryRefusal of patient to the procedureCervix not fully dilatedInability to determine station, position, or
inadequate pelvisPossible CPDUnsuccessful trial of vacuum extractionAbsence of adequate anesthesiaInadequate facilities and support staffInexperienced operator

Forceps ApplicationCephalic curve is closely adapted to the sides of
the fetal headThe fetal head is perfectly grasped when the
long axis of the blade corresponds to the OMDThe major portion of the blade is lying over the
faceThe concave margins of the blade directed
toward either the sagittal suture (OA) or the face (OP)
Forceps should not slip and traction may be applied

Types of ApplicationCephalic application – the blade lie against
the side of the head covering space between orbit and eye
Pelvic application – L blade applied to the L side of the mother, and the R blade applied to the R side of the mother regardless of the position of the fetal head
NOTE: Cephalic curve – conforms to the shape of the fetal headPelvic curve – corresponds more or less the axis of the birth canal


Types of GripPencil grip – most
favorable, more easier than
Hand-shaking grip – an alternate to pencil grip
Long forceps – grips the mandible of the fetus
Short forceps – grips the maxilla of the fetus

Insertion of the BladeL blade – held by the L hand of the examiner,
applied to the L side of the mother, and to the L side of the fetus; is guided by the fingers of the R hand
R blade – held by the R hand of the examiner, applied to the R side of the mother, and to the R side of the fetus; is guided by the fingers of the L hand

How to note that the Blade is locked?Sagittal suture is perpendicular to the plane
of the shank
Posterior fontanel is one fingerbreadth distance from the plane
Fenestrations of the planes are equally felt bilaterally

Outlet Forceps DeliveryThe small fontanel (posterior) is directed
toward the symphysis pubisThe forceps are applied as follows:
Two or more fingers of the R hand are introduced inside the L posterior portion of the vulva and into the vagina beside the fetal head
The handle of the left branch is then grasped between the thumb and two fingers of the L hand and the tip of the blade is gently passed into the vagina between the fetal head and the palmar surface of the fingers of the R hand.

Outlet Forceps DeliveryFor application of the R blade, two or more
fingers of the L hand are introduce into the R, posterior portion of the vagina to serve as a guide for the R blade, which is held in the R hand and introduce into the vagina.

Outlet Forceps Delivery: TractionGentle, intermittent, horizontal tractionThe handles are gradually elevated, and
eventually pointing almost directly upward as the parietal bones emerge.
As the handles are raised the head is extended
Upward traction: four fingers should grasp the upper surface of the handle and shanks, the thumb exerts force on their lower surface


Outlet Forceps Delivery: TractionSpontaneous delivery: intermittent, head is
allowed to recede in intervalsSevere fetal bradycardia: delivery is
sufficiently slow, deliberate, and gentle to prevent undue head compression
Traction is applied only with each uterine contraction

Outlet Forceps DeliveryDelivery is completed:
1. forceps in place to control the advance of the head2. forceps is removed and delivery is completed by
the Modified Ritgens Maneuver
Modified-Ritgens Maneuver – head distends the vulva and perineum enough to open the vaginal introitus to a diameter of 5 cm or more, a towel draped, gloved hand is used to exert forward pressure on the chin of the fetus through the perineum just in front of the coccyx, the other hand exerts pressure superiorly against the occiput

Low and Midforceps OperationHead lies above the perineumSagittal suture usually occupies an oblique or
transverse diameter of the pelvisForceps should always be applied to the sides
of the head

Low and Midforceps Operation: LOA positionR hand is introduced into the LP segment of
the vagina (L ear posteriorly)R hand guides the introduction of the L branch
of the forceps (held by the L hand and applied over the L ear)
L hand guides the R branch of the forcepThen applied over the anterior ear of the fetus
by gently sweeping the blade anteriorly until it lies opposite the blade that was introduce first.

Low and Midforceps Operation: ROA positionBlades are introduced similarly but in
opposite directionBlades are applied at the sides of the head,
the left handle and shank lie above the right Forceps do not immediately articulateLocking the branches is affected, however,
rotating the left around the right branch brings the lock into its proper position

Low and Midforceps Operation: OT positionFirst blade applied over the posterior ear The second blade is rotated anteriorly to a
position opposite to the firstOne blade lies in front of the sacrumAnd the other behind the symphysisSimpson, Mclane, Keilland forceps

Low and Midforceps Operation: Anterior and Transverse position
Occiput is obliquely anterior, it gradually rotate spontaneously to the symphysis as traction is exerted
When it is in transverse, a rotary motion is requiredRotation CCW from the left side towards the midline
is required when the occiput is directed towards the left, and the reverse if directed towards the right side of the pelvis
Flattened pelvis , rotation is not attempted until the head has reached or approached the pelvic floor
Traction is exerted downward until the occiput appears at the vulva

OP Position: Manual RotationA hand with the palm upward is inserted into the
vagina and the fingers are brought in contact with the side of the fetal head that is to be rotated toward the anterior position, while the thumb is placed over the opposite side of the head
Occiput in the RP position, the left hand is used to rotate the occiput anteriorly in a CW direction
The right hand is used for the LOP positionThe head must not be disengaged during the
procedureOcciput has reached the anterior position – labor is
allowed to continue or assisted by forceps

OP Position: Forceps deliveryIf manual rotation is not accomplishedBlade is applied to the head in the posterior position
and is delivered in the OP positionMC of POP position is anthropoid pelvisOcciput is directly posterior, horizontal traction is
applied until the base of the nose is under the symphysis
Handles are slowly elevated until the occiput gradually emerges over the anterior margin of the perineum
Forcep is directed in a downward motion and the nose, face and chin , emerges out from the vulva

Large episiotomy Severe perineal
lacerationsSevere vaginal
lacerationsErb and Facial nerve
palsies

OP Position: Forceps rotation on Occiput Oblique Posterior
Tucker-Mclane, Keilland, and Simpson forcepsRotated 45 degrees to posterior position or 135
degrees to anterior positionWith Simpson and Mclane forceps head must be
flexedPelvic curvature which is originally directed
upward, is inverted and directed posteriorly Causes vaginal sulcus tears and sidewall
lacerationsKeilland forceps – flexed head is not necessary
for they have a more straightened pelvic curve


Forceps Rotation of OTDifficult operative vaginal deliverySpecial skills and training are important Either Simpson or Keilland forceps The station of the fetal head must be
accurately at or below or below the level of the ischial spines

Forceps Rotation of OT: KeillandWandering or gliding method
Anterior blade is introduced over the side of the pelvis over the brow or face
Blade is arched to an anterior position with the handle held close to the opposite maternal buttock
The second blade is introduced posteriorly and the branches are locked
Direct or classical applicationAnterior blade is introduced with the cephalic curved
directed upward curving under the symphysisAfter it has entered far into the uterine cavity, it is
turned on its axis into 180 degrees to adapt the cephalic curvature to the head




Forceps Delivery of Face PresentationWith the chin directed toward the symphysis –
mentum anterior – forceps are occasionally used to effect vaginal delivery
Blades are applied to the sides of the head along the OM diameter, with the pelvic curve directed toward the neck
Downward traction is exerted until the chin appears under the symphysis
By an upward movement, face is slowly extracted with the nose, eyes, brow, and occiput appearing in succession over the anterior margin of the perineum


Morbidity from Forceps OperationsElective outlet forceps with rotations not
exceeding 45 degrees are associated with little, if any, increase in maternal morbidity
Maternal injury increases significantly with rotations greater than 45 degrees and at higher stations
The need for blood transfusions is increased with operative vaginal delivery
Vacuum extraction – 6.1 % Forceps – 4.2 % CS – 1.4 %

Febrile MorbidityPostpartum metritis is more frequent and
severe in CS deliveries compared to operative vaginal deliveries
In midpelvic level – increases neonatal morbidity
Higher incidence of intracranial hemorrhageIncrease the risk for brachial plexus injury
Perinatal Morbidity

Complications Maternal
- Pulmonary embolism- Increase blood loss- Febrile morbidity- Cervical and vaginal lacerations
Fetal - Facial and abducens nerve palsies – resolve by 6
weeks- Increase risk of brachial nerve injury- Cephalhematoma – midforceps- Transient forceps marks

Trial of Forceps and Failed ForcepsAttempt for operative vaginal delivery is
anticipated to be difficultOR and the staff are equipped for immediate
cesarean deliveryIf unsatisfactory - abandoned and proceeds to
vacuum or CS deliveryIf satisfactory – gentle downward pulls are
made on the forceps; if no descent abandonedFails to effect vaginal delivery – CS delivery

Vacuum Delivery
First used in 1829 by Seemann and Arnott1957 Malmston developed the modified
instrument using a metal cup

Metal cupSoft cup
Low incidence of scalp injuryHigher failure rate
Silastic cup Reusable deviceSoft65mm diameterCMI tender touch uses 62mm cup

Advantage Avoidance of insertion of space occupying
steel blades within the vagina Avoidance of the requirement for precise
positioning over the fetal head Ability to rotate the fetal head without
impinging on maternal tissuesDecreased ICP during traction

Recommendations 1. The classification of vacuum deliveries should be the same
as that utilized for forceps deliveries (including station)2. The same indications and contraindications utilized for
forceps deliveries should be applied to vacuum-assisted deliveries
3. The vacuum should not be applied to an unengaged vertex, that is, above O station
4. The individual performing or supervising the procedure should an experienced operator
5. The operator should be willing to abandon the procedure if it does not proceed easily or if the cup pops off more than 3 times

Indications Cervix must be completely dilatedMembranes must be rupturedFetal head must be engagedCapability of quick CS is available

Maternal IndicationsInadequate voluntary effortSoft tissue obstructionElective avoidance of valsalva effort in the
second stageMalpresentation of the vertex
Anticipated or evident fetal intolerance of continued labor
Fetal Indications

ContraindicationsInexperienced operatorApplication to the aftercoming head, brow or face
presentation
Fetal prematurityPrior fetal scalp traumaActive bleeding or suspected fetal coagulation
defectsMacrosomiaNonvertex presentations
Relative Contraindications


Procedure Note:
Proper cup placement is the most important determinant of success
Center of cup should be over the sagittal suture about 3 cm in front of posterior fontanelle towards the face
Full circumference of the cup should be palpated before and after vacuum has been created and prior to traction
Rigid cup – gradually increases suction by o.2 kg/cm² every 2 min until a negative pressure of o.8 kg/cm² is reached

Procedure Soft cup – negative pressure can be increased to
0.8 kg/cm² over as little as 1 minTraction is intermittent and coordinated with
maternal expulsive efforts2 handed technique – fingers of 1 hand are placed
against the suction cup, while the other hand grasp the handle of the instrument
Progress of descent should accompany each traction attempt
Willingness to abandon attempts if satisfactory progress is not made

Guidelines for AbandonmentRepeated detachmentsProlonged vacuum and traction efforts w/o
significant progress of deliveryTotal extraction time takes up to 15 minutes
or5-10 tractions during uterine contractions

ComplicationsMaternal
Fewer vaginal and perineal lacerations
Fetal Large caput Cephalhematoma Subaponeurotic hemorrhage Retinal hemorrhage Occasional intracranial hemorrhage

Comparison of Vacuum Extraction with Forceps
Forceps Vacuum Higher frequency of maternal trauma and blood lossMore 3rd and 4th degree lacerationInfants delivered have more marks and bruising
Increase in the incidence of neonatal jaundiceIncidence of shoulder dystocia and cephalhematoma is doubledIncreased fetal traumaDecreased maternal trauma and neonatal morbidity

Thank you