
Delivering Treatment for Depression into the Patient’s Home: Telephone & Internet David C. Mohr,...
34
Delivering Treatment for Delivering Treatment for Depression into the Depression into the Patient’s Home: Telephone Patient’s Home: Telephone & Internet & Internet David C. Mohr, Ph.D. David C. Mohr, Ph.D. Northwestern University Northwestern University & & Center for the Management of Complex Center for the Management of Complex Chronic Care Chronic Care Hines VA Hines VA
-
Upload
scott-harrison -
Category
Documents
-
view
216 -
download
0
Transcript of Delivering Treatment for Depression into the Patient’s Home: Telephone & Internet David C. Mohr,...

Delivering Treatment for Delivering Treatment for Depression into the Patient’s Depression into the Patient’s Home: Telephone & InternetHome: Telephone & Internet
David C. Mohr, Ph.D.David C. Mohr, Ph.D.Northwestern UniversityNorthwestern University
&&Center for the Management of Complex Chronic Center for the Management of Complex Chronic
CareCareHines VAHines VA

What I will talk about todayWhat I will talk about today
Describe our telephone psychotherapy Describe our telephone psychotherapy research program in depression.research program in depression. We began in 1995, when the telephone was We began in 1995, when the telephone was
the principal option for reaching outthe principal option for reaching out Current state of internet treatments for Current state of internet treatments for
depressiondepression Our developing research in integrating Our developing research in integrating
internet and telephone.internet and telephone.
Telephones in Telephones in PsychotherapyPsychotherapy
In 1876 Alexander Graham Bell invented the In 1876 Alexander Graham Bell invented the telephonetelephone
Three years later, in 1879, BMJ published the Three years later, in 1879, BMJ published the first report of a the use of a telephone to first report of a the use of a telephone to diagnose a child’s cough.diagnose a child’s cough.
Another 70 years was required before the Another 70 years was required before the first reports of the use of telephones in first reports of the use of telephones in psychotherapy were published (1949).psychotherapy were published (1949).
A 1996 APA task force report stated that A 1996 APA task force report stated that empirical evidence of the efficacy of empirical evidence of the efficacy of telphone-administered psychotherapy was telphone-administered psychotherapy was scant to non-existent.scant to non-existent.

Why look at Why look at telephone telephone
psychotherapy?psychotherapy?
Nearly 2/3rds of practicing clinical psychologists Nearly 2/3rds of practicing clinical psychologists today report using the phone to some degree to today report using the phone to some degree to deliver care.deliver care.
Mental Health carve-outs, HMOs, the VA and Mental Health carve-outs, HMOs, the VA and others are beginning to develop and implement others are beginning to develop and implement tele-mental health programs totele-mental health programs to Extend careExtend care Save costsSave costs
Research to develop and validate tele-mental Research to develop and validate tele-mental health programs wouldhealth programs would Facilitate policy decision makingFacilitate policy decision making Support standards for qualitySupport standards for quality

How we beganHow we began We began in 1995, when We began in 1995, when
the telephone was the the telephone was the principal tool for outreachprincipal tool for outreach
Many patients at the Many patients at the UCSF Multiple Sclerosis UCSF Multiple Sclerosis Center were unable to Center were unable to attend regularly attend regularly scheduled appointments scheduled appointments due todue to DisabilityDisability Distance from centerDistance from center
Two-thirds of patients would prefer Two-thirds of patients would prefer psychotherapy or counseling to psychotherapy or counseling to pharmacotherapy.pharmacotherapy.
Initial Pilot ResearchInitial Pilot Research
We developed a telephone-administered We developed a telephone-administered cognitive behavioral therapy (T-CBT) that cognitive behavioral therapy (T-CBT) that includes:includes: A patient workbook to A patient workbook to
facilitate communicationfacilitate communicationprovide informationprovide informationprovide support between sessions.provide support between sessions.
32 Kaiser multiple sclerosis patients with POMS 32 Kaiser multiple sclerosis patients with POMS depression > 15 were randomly assigned to:depression > 15 were randomly assigned to: 8 weeks of T-CBT administered by 28 weeks of T-CBT administered by 2ndnd-3-3rdrd year year
graduate students.graduate students. Usual care control (UCC) through Kaiser Usual care control (UCC) through Kaiser
PermanentePermanente
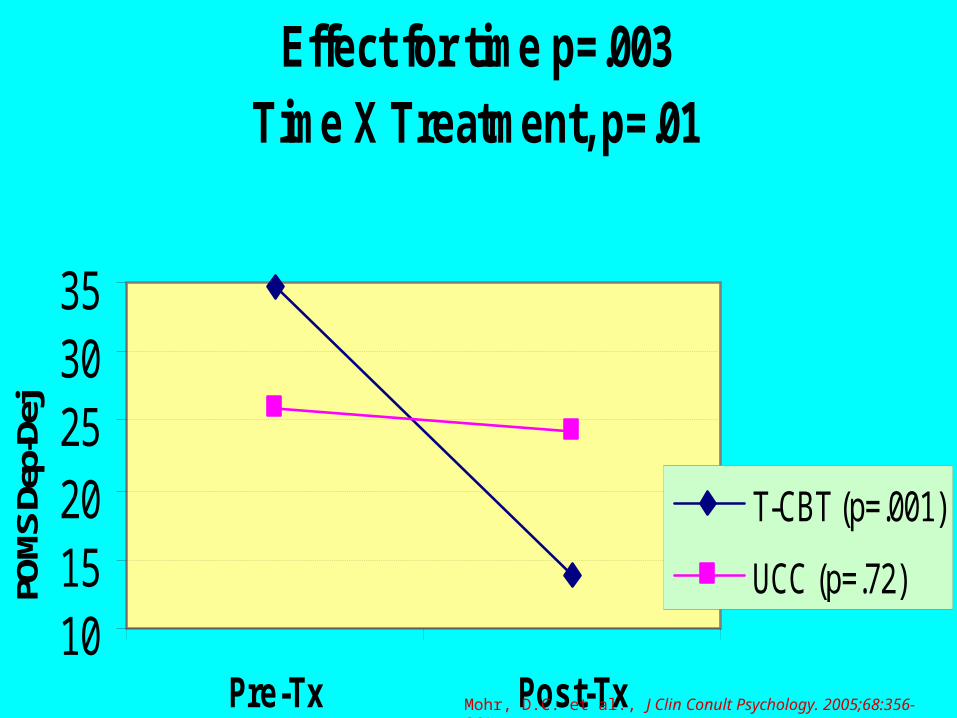
Effect for time p=.003Time X Treatment, p=.01
101520253035
Pre-Tx Post-Tx
POM
S De
p-De
j
T-CBT (p=.001)
UCC (p=.72)
Mohr, D.C. et al., J Clin Conult Psychology. 2005;68:356-361

T-CBT vs. T-SEFTT-CBT vs. T-SEFT
Compared 16 weeks of T-CBT to T-Supportive Emotion-Focused Compared 16 weeks of T-CBT to T-Supportive Emotion-Focused Therapy (T-SEFT).Therapy (T-SEFT). T-SEFT a manualized, client centered tx, aimed at enhancing T-SEFT a manualized, client centered tx, aimed at enhancing
awareness of emotions and inner experience, with operationalized awareness of emotions and inner experience, with operationalized procedures for enhancing therapeutic relationship. Interventions procedures for enhancing therapeutic relationship. Interventions focused on behavior or cognition were prohibited.focused on behavior or cognition were prohibited.
127 Patients were randomized: 127 Patients were randomized: MSMS BDI ≥ 16BDI ≥ 16 1+ physical symptoms causing participation restriction (handicap)1+ physical symptoms causing participation restriction (handicap) 99 (77%) women99 (77%) women
Therapists were Ph.D psychologists, with allegiance to their Therapists were Ph.D psychologists, with allegiance to their treatment arm.treatment arm.
Supervisors were specialists in CBT and SEFTSupervisors were specialists in CBT and SEFT Patients were followed for one year after treatment cessationPatients were followed for one year after treatment cessation

Hamilton: Baseline To End of Follow-UpTreatment Outcome: Time - p< .00001; Time X Tx - p=.019Maintenance of Gains: Time - p=.004; Time x Tx - p=.42
10
12
14
16
18
20
22
0 8 16 28 40 52 64Week
HR
SD
T-SEFT
T-CBT
*
*
End of Tx
Mohr, D.C. et al., Arch Gen Psychaitr. 2005;62:1007-1014
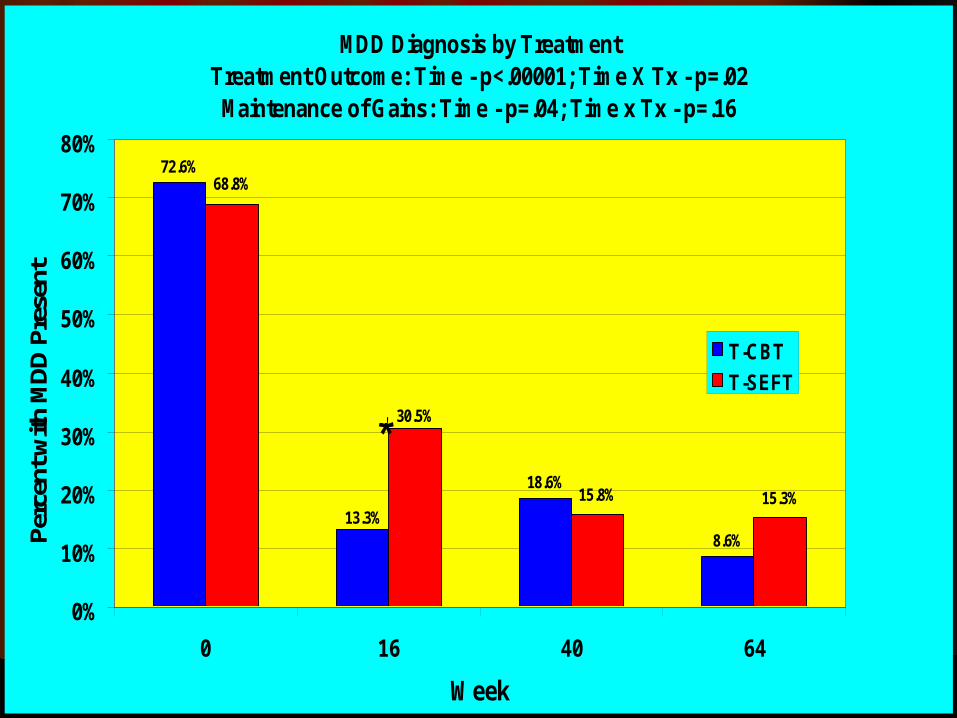
MDD Diagnosis by TreatmentTreatment Outcome: Time - p<.00001; Time X Tx - p=.02Maintenance of Gains: Time - p=.04; Time x Tx - p=.16
72.6%
18.6%
8.6%13.3%
15.3%15.8%
30.5%
68.8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0 16 40 64
Week
Perc
ent w
ith M
DD
Pre
sent
T-CBT
T-SEFT
*
End of Tx

Disability (GNDS) Controlling for HRSDTreatment Effect (p=.002)Time X treatment (p=.004)
14
16
18
20
22
24
0 8 16Week
Dis
abili
ty (
GN
DS
) T-SEFT
T-CBT*
*

T-CBT vs. T-SEFTT-CBT vs. T-SEFT
A large literature has shown most A large literature has shown most psychotherapies are equivalent in psychotherapies are equivalent in reducing depression.reducing depression.
CBT and SEFT, face-to-face, have been CBT and SEFT, face-to-face, have been shown to be equivalent in face-to-face shown to be equivalent in face-to-face administration administration (Watson et al. JCCP 2003;71:773-81)(Watson et al. JCCP 2003;71:773-81)
Our finding that T-CBT is superior suggests Our finding that T-CBT is superior suggests that this this may not be true with tele-that this this may not be true with tele-therapy to patients with barriers. therapy to patients with barriers.
Skills training is important!Skills training is important!

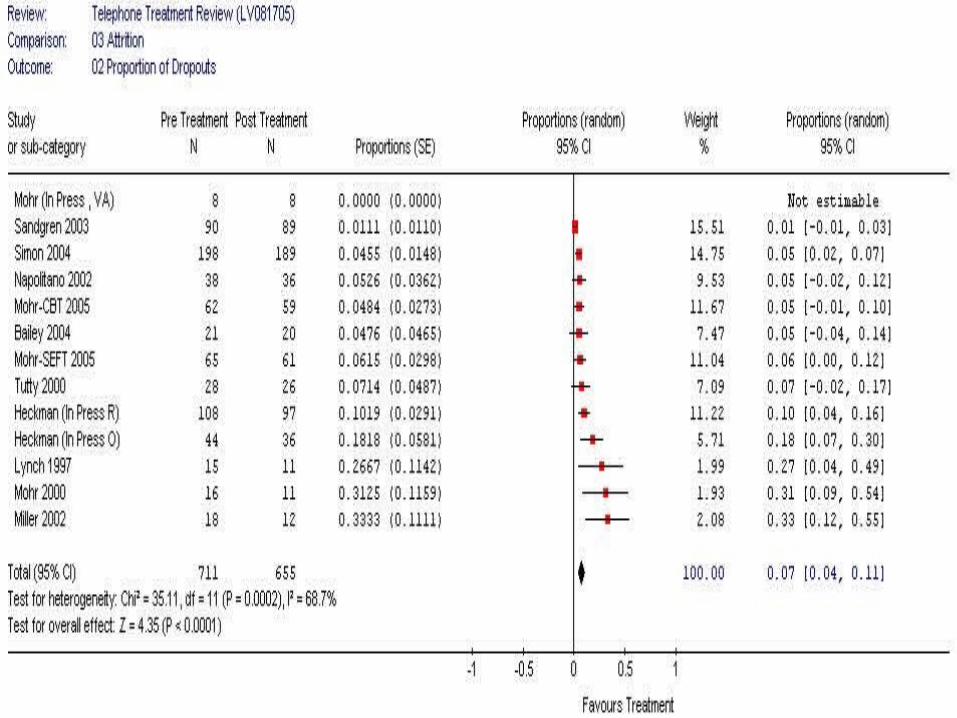
AttritionAttrition
Attrition in trials of face-to-face Attrition in trials of face-to-face psychotherapy ranges from 15-psychotherapy ranges from 15-60% with a means of 26% to 47%60% with a means of 26% to 47%
Attrition was 7 (5.5%)Attrition was 7 (5.5%) 3 (4.8%) for T-CBT 3 (4.8%) for T-CBT
One was removed secondary to trauma.One was removed secondary to trauma. 4 (6.2%) for T-SEFT4 (6.2%) for T-SEFT
Barriers to Psychotherapy Barriers to Psychotherapy in Primary Carein Primary Care
Primary care is the de facto site for Primary care is the de facto site for identification and treatment of depression.identification and treatment of depression.
Approximately 2/3rds of depressed patients Approximately 2/3rds of depressed patients state that they would prefer psychotherapy state that they would prefer psychotherapy to antidepressant medications. But…to antidepressant medications. But… Only approximately 20% follow-up on referrals by Only approximately 20% follow-up on referrals by
their primary care physician.their primary care physician. Of those who begin nearly half dropout of Of those who begin nearly half dropout of
treatment.treatment. This suggests that there are significant This suggests that there are significant
barriers to psychotherapy.barriers to psychotherapy.
Barriers to Psychotherapy in 290 Barriers to Psychotherapy in 290 UCSF Primary Care patientsUCSF Primary Care patients
Depressed patients are more likely to Depressed patients are more likely to perceive barriers (74.0% vs. 51.4%, p=.0002)perceive barriers (74.0% vs. 51.4%, p=.0002)
Among depressed patients 68.3% report Among depressed patients 68.3% report practical barriers includingpractical barriers including Transportation (21.2%)Transportation (21.2%) Time constraints (20.6%)Time constraints (20.6%) Caregiving responsibilities (13.6%)Caregiving responsibilities (13.6%)
19.2% report emotional barriers including19.2% report emotional barriers including Concerns about being seen while emotional (6.8%)Concerns about being seen while emotional (6.8%) People finding out they are in psychotherapy People finding out they are in psychotherapy
(6.8%)(6.8%)

Depression is both a indication for psychotherapy Depression is both a indication for psychotherapy and a barrier to receiving it.and a barrier to receiving it.
Inserting behavioral medicine into primary care has Inserting behavioral medicine into primary care has not been widely adopted.not been widely adopted.
Data suggest T-CBT may increase access for and Data suggest T-CBT may increase access for and reduce attrition from psychotherapy for depression.reduce attrition from psychotherapy for depression.
A current trial is examining T-CBT for the treatment A current trial is examining T-CBT for the treatment of depression in veterans in rural areas with limited of depression in veterans in rural areas with limited mental health services.mental health services.
A randomized trial of T-CBT compared to face-to-A randomized trial of T-CBT compared to face-to-face CBT for depression in primary care has been face CBT for depression in primary care has been funded by the NIMH and will begin in the coming funded by the NIMH and will begin in the coming months.months.
And so, can we reach And so, can we reach out?out?
Telecommunications Telecommunications innovations since 1995innovations since 1995
Internet penetrationInternet penetration 73% of Americans have internet access (compared to 73% of Americans have internet access (compared to
95% with telephone access).95% with telephone access). 42% have broadband access (40% increase in one year).42% have broadband access (40% increase in one year). Access is much higher in urban areasAccess is much higher in urban areas
Promise of Internet CBTPromise of Internet CBT Standardized presentation of therapy materialStandardized presentation of therapy material Interactive programming for exercisesInteractive programming for exercises No geographic limitations to services.No geographic limitations to services. Patient access 24/7Patient access 24/7 Costs are potentially minimalCosts are potentially minimal Multiple avenues for contact with therapistMultiple avenues for contact with therapist
Why should we be worried Why should we be worried about standardization of about standardization of
content?content? RCT data shows CBT is largely equivalent to RCT data shows CBT is largely equivalent to
antidepressant medication.antidepressant medication. Among 6,047 pts treated with Among 6,047 pts treated with
psychotherapy in HMOs, CMHCs, EAPs etc. psychotherapy in HMOs, CMHCs, EAPs etc. (Hansen 2002,2003)(Hansen 2002,2003) 8.2% deteriorated8.2% deteriorated 56.8% showed no change56.8% showed no change 20.9% showed some measurable improvement20.9% showed some measurable improvement 14.1% met criteria for recovery14.1% met criteria for recovery
After 16 sessions, only 50% of patients show After 16 sessions, only 50% of patients show measurable improvement.measurable improvement.

Why are psychotherapy Why are psychotherapy outcomes so bad in the outcomes so bad in the
community, compared to community, compared to RCTsRCTs
Patients in the community may be more Patients in the community may be more difficult than those selected for clinical trials.difficult than those selected for clinical trials. Multiple psychiatric problems, substance abuse, Multiple psychiatric problems, substance abuse,
etc.etc. But RCTs rule most people out for not being severe But RCTs rule most people out for not being severe
enough.enough. Assuring competence in a private endeavorAssuring competence in a private endeavor
Evidence that adherence to tx model improves Evidence that adherence to tx model improves outcomes.outcomes.
Even in RCTs at least 25% of sessions do not meet Even in RCTs at least 25% of sessions do not meet criteria.criteria.
Nobody knows what therapists in the community Nobody knows what therapists in the community do.do.

I-CBTI-CBT
Opportunity to provide standardized Opportunity to provide standardized carecare
Provide over a long distanceProvide over a long distanceAt minimal cost.At minimal cost.
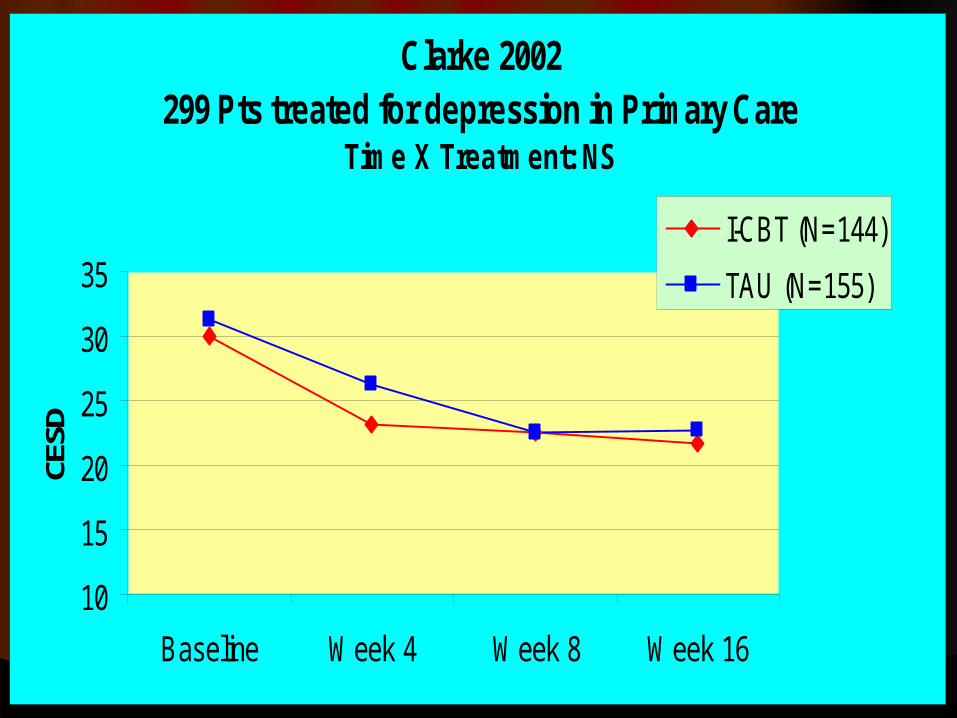
Clarke 2002299 Pts treated for depression in Primary Care
Time X Treatment: NS
10
15
20
25
30
35
Baseline Week 4 Week 8 Week 16
CESD
I-CBT (N=144)
TAU (N=155)

Clarke, 2002 Cont’dClarke, 2002 Cont’d
Potential reasons for failurePotential reasons for failureLow compliance with website: Low compliance with website:
Median visits = 2Median visits = 2Mean visits = 2.6 ± 3.5Mean visits = 2.6 ± 3.5
AttritionAttrition34.4% across both treatments34.4% across both treatments

Clarke 2005 255 Pts Receiving Care for Depression in an HMO
Time X Treatment: p = .03
10
15
20
25
30
35
Baseline Week 5 Week 10 Week 16
CE
SD
I-CBT+Postcard (N=75)
I-CBT+Call (N=80)
TAU/I-CBT(N=100)

Clarke, 2005 cont’dClarke, 2005 cont’d
Compliance somewhat better but not Compliance somewhat better but not great:great: I-CBT+postcard: M = 5.0±6.2I-CBT+postcard: M = 5.0±6.2 I-CBT+telephone call: M = 5.6±5.8I-CBT+telephone call: M = 5.6±5.8 TAU (+I-CBT access): M = 2.6±2.5TAU (+I-CBT access): M = 2.6±2.5
Attrition still not goodAttrition still not good I-CBT+postcard: 38.7%I-CBT+postcard: 38.7% I-CBT+telephone call: M = 46.3%I-CBT+telephone call: M = 46.3% TAU: 20.0%TAU: 20.0%

Christensen (2004)Sample recruited from internet
Time X Treatment p<.05
00.10.20.30.40.50.60.7
Internet Information(N=165)
I-CBT + lay phone(N=182)
No tx control(N=178)
Chan
ge in
CES
D (E
ffect
Si
ze)
ITT Sample
Completer Sample
Christensen, 2005 Cont’dChristensen, 2005 Cont’d
ComplianceComplianceI-CBT + Lay phone calls: M = 14.8±9.7 I-CBT + Lay phone calls: M = 14.8±9.7
of 29 exercisesof 29 exercisesInternet information: M = 4.5±1.4 visitsInternet information: M = 4.5±1.4 visits
AttritionAttritionI-CBT + Lay phone calls: 33.5%I-CBT + Lay phone calls: 33.5%Internet information: 17.6%Internet information: 17.6%No treatment control: 11.8%No treatment control: 11.8%

Problems with I-CBTProblems with I-CBT
Assignment to I-CBT associated with Assignment to I-CBT associated with greater dropout than no-tx or TAU.greater dropout than no-tx or TAU.
People aren’t using it. People aren’t using it. 34-47% of I-CBT patients drop out.34-47% of I-CBT patients drop out.2-6 visits 2-6 visits Phone calls from lay persons don’t help Phone calls from lay persons don’t help
muchmuch I-CBT sites to date have not been I-CBT sites to date have not been
tailored to the patient.tailored to the patient.

Wright (2005)Time X treatment: p=.02
0
0.5
1
1.5
2
2.5
3
C-CBT + 1/2therapist time (N=15)
Standard CBT(N=15)
WLC (N=15)Chan
ge in
BDI
(Effe
ct S
ize)
ITT
Completers
Strengths & WeaknessStrengths & Weakness
Telephone-Psychotherapy (T-CBT)Telephone-Psychotherapy (T-CBT)+ Low attrition (<5%)+ Low attrition (<5%)+ Strong efficacy under controlled conditions+ Strong efficacy under controlled conditions+ Excellent outreach / reduction in barriers+ Excellent outreach / reduction in barriers- Relies on therapist adherence to tx modelRelies on therapist adherence to tx model- No significant cost savingsNo significant cost savings
I-CBTI-CBT+ Standardized presentation of material+ Standardized presentation of material+ Geographic coverage, 24/7 coverage+ Geographic coverage, 24/7 coverage+ Minimal cost+ Minimal cost- Effect sizes appear much lower than other treatmentsEffect sizes appear much lower than other treatments- Attrition high (comparable to face-to-face therapy)Attrition high (comparable to face-to-face therapy)- Compliance (visiting site) is low.Compliance (visiting site) is low.

One hour of One hour of Psychotherapy per Psychotherapy per
weekweek
0 24 48 72 96 120 144 168
Hours in Week
Sleep
Wake
Psychotherapy
ψψ
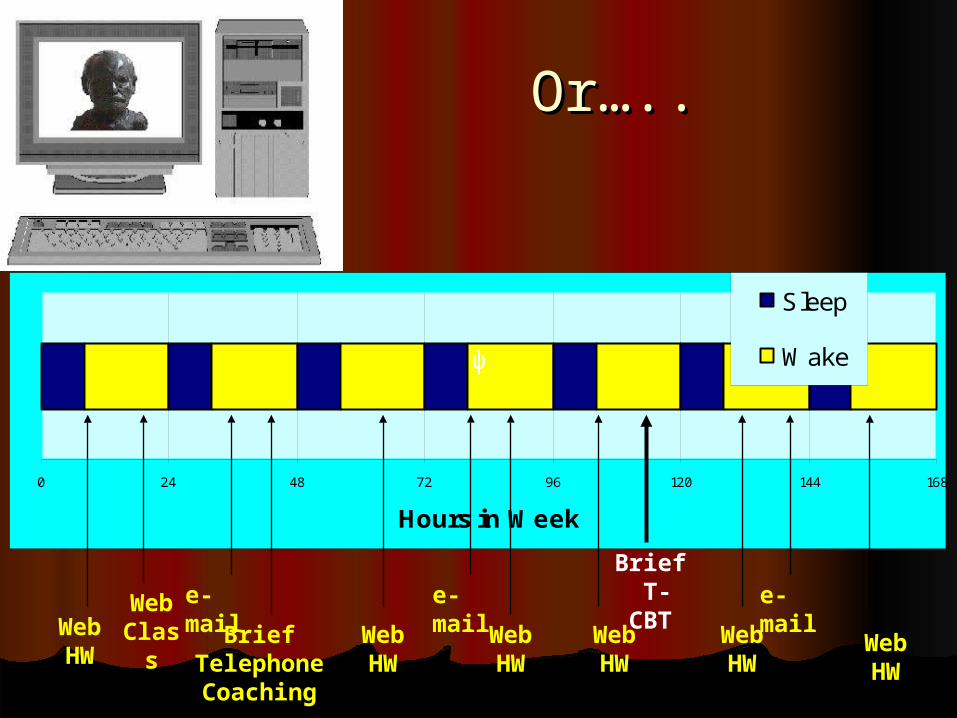
Or…..Or…..
0 24 48 72 96 120 144 168
Hours in Week
Sleep
Wake
Brief T-CBT
ψψ
Web HW
Web HW
Web HW
Web HW
Web HW
Web HW
e-mail e-maile-mail
Brief Telephone Coaching
Web Class
Telephone administered Telephone administered psychotherapy is effective in treating psychotherapy is effective in treating depression.depression.
The inclusion of CBT skills training The inclusion of CBT skills training components add benefit during 16 components add benefit during 16 weeks of treatment.weeks of treatment.
These skills may be taught more These skills may be taught more efficiently using tele-communications efficiently using tele-communications technology that brings training into technology that brings training into patients’ lives.patients’ lives.
Future research:Future research: Compare telephone administered Compare telephone administered
psychotherapy to face-to-face psychotherapy to face-to-face administered psychotherapy administered psychotherapy
Evaluate new procedures for integrating Evaluate new procedures for integrating treatment into patients’ lives using treatment into patients’ lives using internet and other telecommunications internet and other telecommunications technologies.technologies.
ConclusionsConclusions














![12 - Mohr Circles and Failure Envelopes for Students/12 - Mohr Circles and... · Title: Microsoft PowerPoint - 12 - Mohr Circles and Failure Envelopes [Compatibility Mode] Author:](https://static.fdocuments.in/doc/165x107/5b14c9377f8b9a294c8c04b9/12-mohr-circles-and-failure-for-students12-mohr-circles-and-title-microsoft.jpg)


