Delayed Neurotoxicity The cumulative risk at 5 years to develop overt dementia is 24-30% (1,2). For...
17
Delayed Neurotoxicity • The cumulative risk at 5 years to develop overt dementia is 24-30% (1,2). • For patients aged > 60 year the risk of dementia at 7 years is 58% (2). • Multivariate analysis shows that only radiotherapy is a significant factor related to neurotoxicity (1). • By 4 years fatal neurotoxicity rate is 10% (3). ) 1 ( Omuro A.M. et al: Arch Neurol 62:1595-1600, 2005 ) 2 ( O’Brien P.C. et al: Int J Rad Oncol Biol Phys 64:408-16, 2006 ) 3 ( Fisher B et al: J Neuro-Oncol 74:201-205, 2005
-
Upload
malik-guppy -
Category
Documents
-
view
214 -
download
1
Transcript of Delayed Neurotoxicity The cumulative risk at 5 years to develop overt dementia is 24-30% (1,2). For...

Delayed Neurotoxicity
• The cumulative risk at 5 years to develop overt dementia is 24-30% (1,2).
• For patients aged >60 year the risk of dementia at 7 years is 58% (2).
• Multivariate analysis shows that only radiotherapy is a significant factor related to neurotoxicity (1).
• By 4 years fatal neurotoxicity rate is 10% (3).
)1 (Omuro A.M. et al: Arch Neurol 62:1595-1600, 2005)2 (O’Brien P.C. et al: Int J Rad Oncol Biol Phys 64:408-16, 2006
)3 (Fisher B et al: J Neuro-Oncol 74:201-205, 2005

Delayed Neurotoxicity
• By 4 years fatal neurotoxicity rate is 10%
• Modification of the RT schedule to a25% reduction in biologically effective tumor dose (36Gy/30 fractions/3 wks) – delayed but did not eliminate fatal neurotoxicity
• Reduction of RT dosedid not compromisetreatment outcome
Fisher B et al: J Neuro-Oncol 74:201-205, 2005

Delayed Neurotoxicity
O’Brien P.C. et al: Int J Rad Oncol Biol Phys 64:408-13, 2006

Fractional Delivery of Chemotherapeutic Agents Across the BBB and BTB
Local Exposure Fraction
MTX 0.017 0.18
5-FU 0.11 0.25
AZQ 0.70 0.72
BCNU 0.54 0.55
Drug Normal Brain Increased Permeability = 0.1 ml/g/min

Methods to Increase Drug DeliveryMethods to Increase Drug Delivery
• Increase delivery of systemic drug administration (intravascular drugs)
• Increase drug delivery bylocal administration(intra-CSF; intra-parenchymal-CED)

Manipulating the drug(chemical modifications, prodrugs)
Increasing the fraction of the drug reaching the tumor (High-dose chemotherapy, intra-arterial administration)
Manipulating the capillary permeability (osmotic BBBD, chemical modification of BBB/BTB, receptor mediated transport)
Increase Delivery of Intravascular DrugsIncrease Delivery of Intravascular Drugs

Manipulating the drug(chemical modifications, prodrugs)
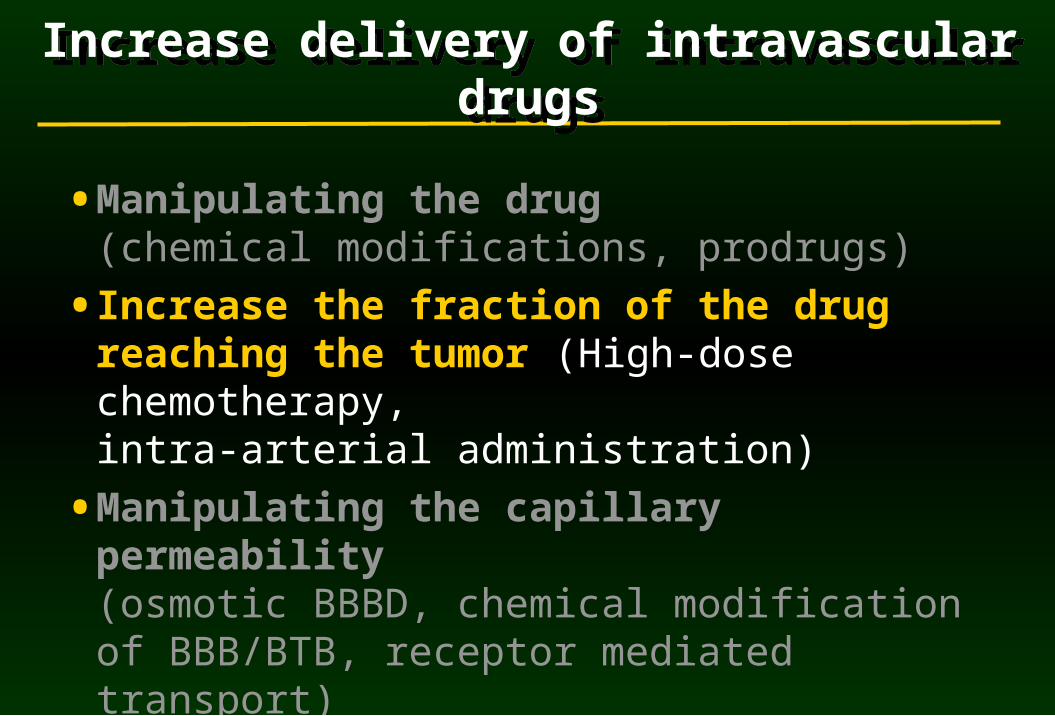
• Manipulating the drug(chemical modifications, prodrugs)
• Increase the fraction of the drug reaching the tumor (High-dose chemotherapy, intra-arterial administration)
• Manipulating the capillary permeability (osmotic BBBD, chemical modification of BBB/BTB, receptor mediated transport)
Increase delivery of intravascular drugsIncrease delivery of intravascular drugs

Increase the Fraction of the Drug Reaching the Tumor: HD-Chemotherapy
• Increase plasma concentration with systemic rescue maneuvers High-dose MTX + folinic acid rescueHigh-dose Ara-C + granulocytic growth factorHigh dose chemotherapy with stem cell support
• Rescue maneuvers reduce systemic toxicity and make the treatment relatively safe.
• Still, systemic toxicity is the major limiting factor.

• Several studies tried to use intensive chemotherapy as the sole treatment for PCNSL but their limitations proved to be either:A low response rate (25% CR) (single
agent HD-MTX) (1)A short duration of response (2)A high rate of treatment-related death
(9-10%) (3).
High Dose Chemotherapy in PCNSL
)1 (Herrlinger U. et al: Ann Neurol 51:247-252, 2002)2 (Abrey L..E. et al: J Clin Oncol 21: 4151-4156, 2003
)3 (Pels H. et al: J Clin Oncol 21: 4489-4495, 2003

% of treatment cycles
Author I.V. MTX dose with CSF MTX level
(gr/m2) > 1 mmol/L
Thyss-1987 0.5 0%
Thyss-1987 2.5 44%
Millot -1994 5.0 66%
Borsi -1987 6.0 100%
Pharmacokinetics of HD-MTXHuman Studies

Pharmacokinetics of HD-MTXHuman Studies
• CSF MTX concentrations: marked interindividual variability.
• Cytotoxic concentrations are obtained with marked increment of the total dose(to 6-8 gr/m2).
• The mean AUC ratio (CSF/serum) MTX:1.52 - 3.0% (systemic dose: 5 - 8 gr/m2 )reflecting the poor diffusion of MTX into the CNS.

MTX Pharmacokinetics
• Human studies evaluated CSF MTX.
• Peak CSF MTX concentrations are observed between 4-6 hrs after MTX infusion while serum levels are rapidly declining.
• Do CSF MTX levels reflect parenchymal drug penetration?
• CSF peak levels may reflect the sink effect or the washout of the drug from the brain and tumor extracellular space.

MethotrexatePharmacokineticsin DogAfter BBBD
MethotrexatePharmacokineticsin DogAfter BBBD
Neuwelt et al, Neurosurgery 7:36-43,1980
CSF
Brain

Pharmacokinetics of MTX in the ECF of Brain Tumor
Plasma total MTX
Plasma free MTX
ECF MTX
i.v. MTX infusion
Dukic et al, Pharmaceutical Res 16:1219-25,1999
AUCECF/AUCPlasma
1.02 + 0.75 % (0.36 -2.37)
AUCECF/AUCPlasma
1.02 + 0.75 % (0.36 -2.37)
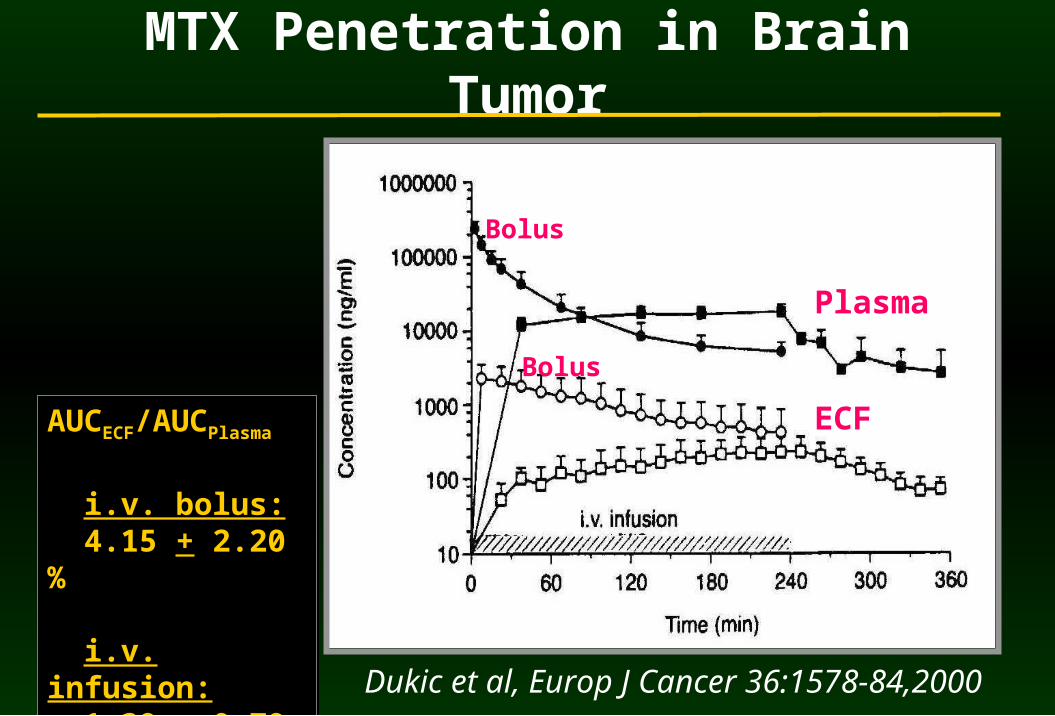
MTX Penetration in Brain Tumor
AUCECF/AUCPlasma
i.v. bolus: 4.15 + 2.20 %
i.v. infusion: 1.39 + 0.79 %
AUCECF/AUCPlasma
i.v. bolus: 4.15 + 2.20 %
i.v. infusion: 1.39 + 0.79 %
Dukic et al, Europ J Cancer 36:1578-84,2000
Plasma
ECF
Bolus
Bolus

n=13
n=16
PCNSL and HD-MTX:Rapid (3 hrs) vs. Regular (6 hrs) Infusion of MTX
Rapid
Regular
CSF MTX Concentration Tumor Volume Relapse-Free Survival
Higara et al, J Neurosurgery 91:221-30,1999
P<0.001
Rapid
Regular
P<0.001





![Reducing dementia risk by targeting modifiable risk ... · Several risk factors have been identified which can either augment or reduce one’s risk of developing dementia [6, 7].](https://static.fdocuments.in/doc/165x107/5f0212f37e708231d4027164/reducing-dementia-risk-by-targeting-modifiable-risk-several-risk-factors-have.jpg)