
Definition of Hypersensitivity - UAB School of Optometry year/Micro/powerpoint/hyper...2 Gell and...
27
1 Type I Hypersensitivity Definition of Hypersensitivity An immunologic reaction which produces tissue damage on reexposure to antigen.
Transcript of Definition of Hypersensitivity - UAB School of Optometry year/Micro/powerpoint/hyper...2 Gell and...
1
Type I Hypersensitivity
Definition of Hypersensitivity
An immunologic reaction whichproduces tissue damage onreexposure to antigen.
2
Gell and Coombs Classification
• Type I (IgE-mediated)• Type II (Fc and complement-mediated)• Type III (Immune complex-mediated)• Type IV (Delayed-type hypersensitivity)
Gell and Coombs Classification
•• Type I (IgE-mediated)Type I (IgE-mediated)• Type II (Fc and complement-mediated)• Type III (Immune complex-mediated)• Type IV (Delayed-type hypersensitivity)
3
Type I Hypersensitivity:History of Discoveries
• Anaphylaxis: Portier and Richet, 1902• Histamine: Dale and Laidlaw, 1911• Transfer of sensitivity: Prausnitz &
Küstner• Mast cells as main tissue source of
histamine: Riley and West, 1952• IgE immunoglobulin: Ishizaka and
Ishizaka, 1966
Type I Hypersensitivity Diseases
• Allergic rhinoconjunctivitis (hayfever)
• Asthma• Eczema (atopic dermatitis)• Acute urticaria• Anaphylaxis
4
5
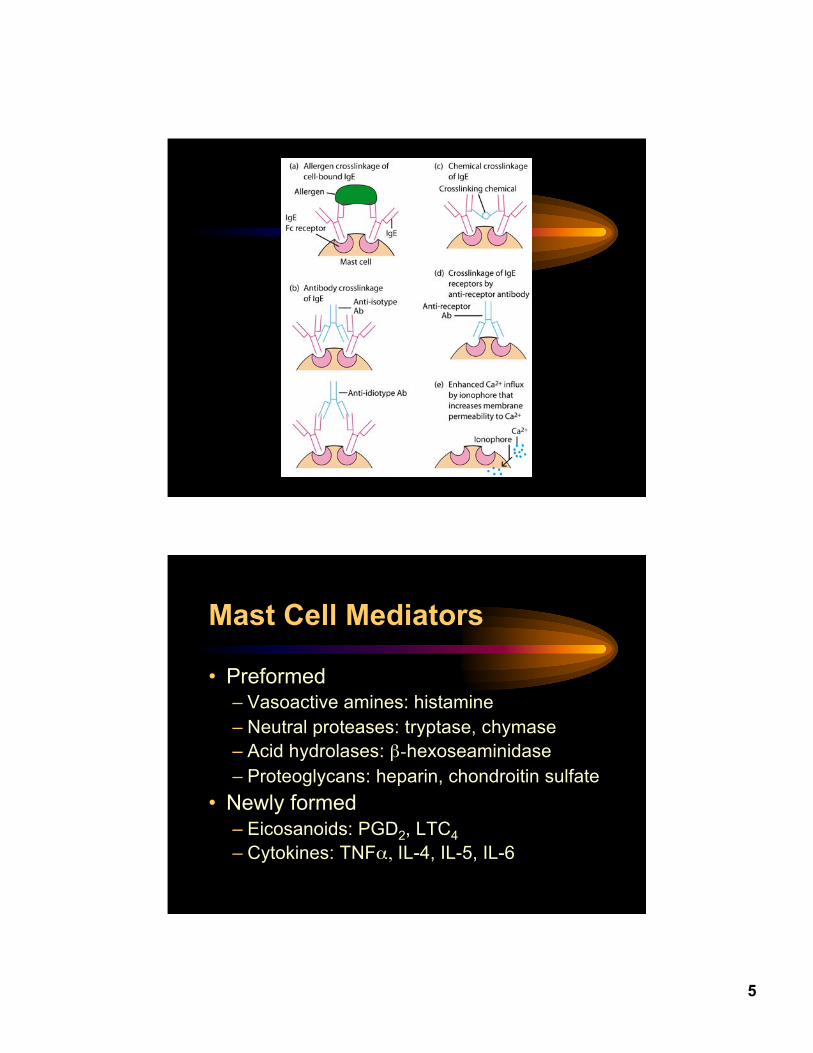
Mast Cell Mediators
• Preformed– Vasoactive amines: histamine– Neutral proteases: tryptase, chymase– Acid hydrolases: β-hexoseaminidase– Proteoglycans: heparin, chondroitin sulfate
• Newly formed– Eicosanoids: PGD2, LTC4– Cytokines: TNFα, IL-4, IL-5, IL-6
6
Mast Cell Tryptase
• Tetrameric serine protease• Found only in mast cells, not basophils• Peaks in 1 hour and remains elevated 4-6 hours in
serum following release in anaphylaxis• Alpha isoform is predominant in blood: most
mastocytosis patients with systemic disease havetotal tryptase levels that are elevated (> 20 ng/ml)and are at least 10-fold greater than their βtryptase level.
Histamine
• Produced almost exclusively by basophilsand mast cells (3-8 pg/cell)
• Immediate pharmacologic effects:– pruritus (H1)– ↑ vascular permeability/vasodilatation (H1)– smooth muscle contraction (H1)– gastric acid secretion (H2)
7
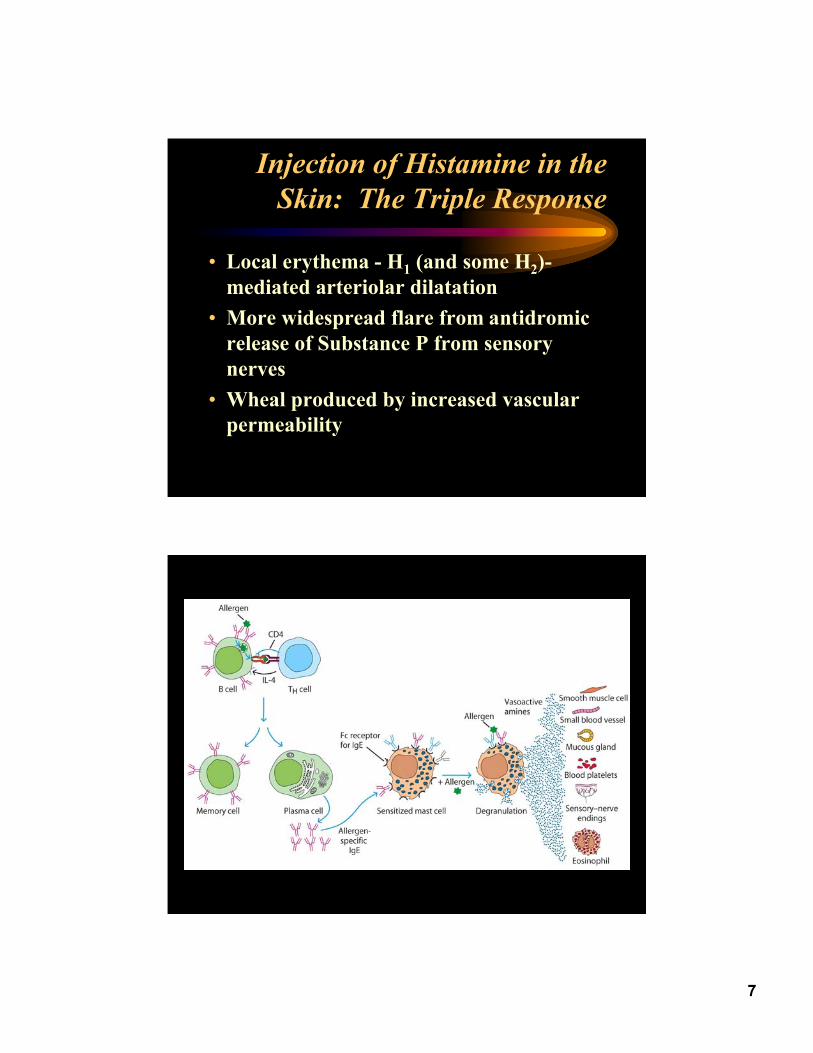
Injection of Histamine in theSkin: The Triple Response
• Local erythema - H1 (and some H2)-mediated arteriolar dilatation
• More widespread flare from antidromicrelease of Substance P from sensorynerves
• Wheal produced by increased vascularpermeability
8
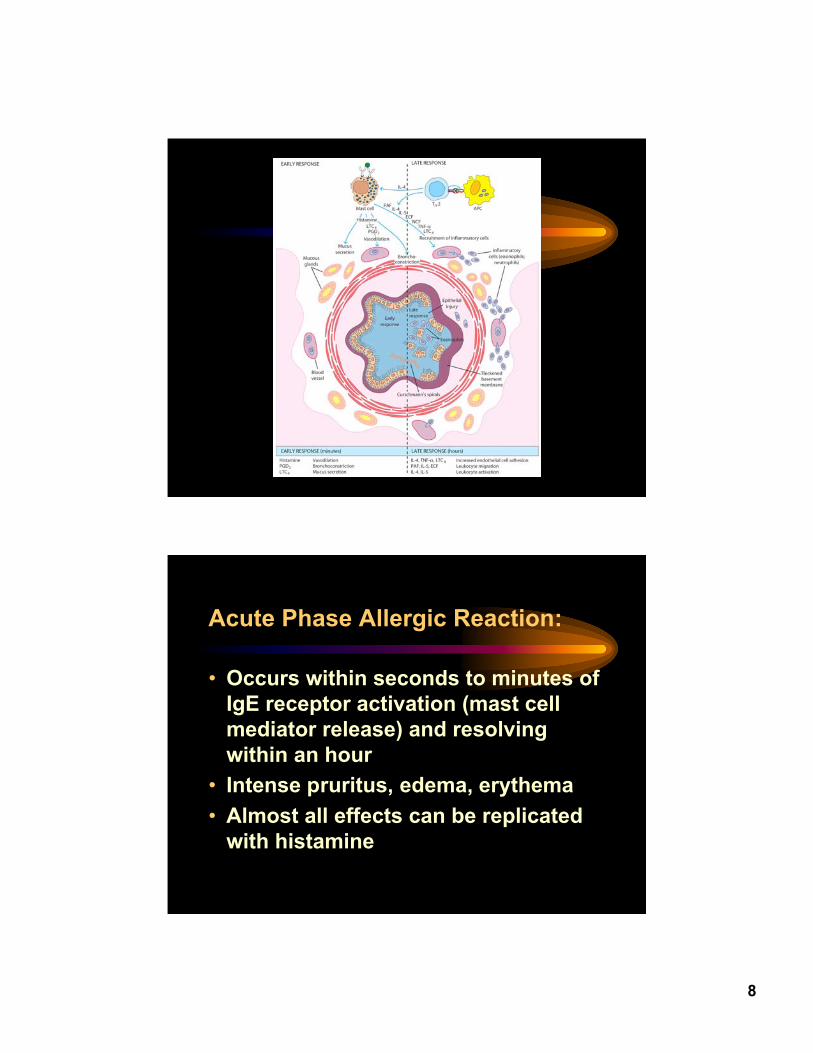
Acute Phase Allergic Reaction:
• Occurs within seconds to minutes ofIgE receptor activation (mast cellmediator release) and resolvingwithin an hour
• Intense pruritus, edema, erythema• Almost all effects can be replicated
with histamine
9
Late Phase Allergic Reaction:
• A delayed inflammatory response (peaking at4-8 hrs and persisting up to 24 hrs) followingan intense acute phase reaction– Skin: erythema, induration, burning– Lungs: airway obstruction poorly responsive to
bronchodilators– Nose/eyes: erythema, congestion, burning
• Histology: mast cell degranulation followedby influx of first neutrophils and eosinophilsfollowed by mononuclear cells
• Major portion of effects replicated by TNFα
10
Therapy of Allergic Disease
• Inhibition of IgE synthesis: Immunotherapy• Inhibition of IgE binding to receptor:
– Monoclonal anti-IgE (Xolair (Omalizumab)• Inhibition of mast cell mediator release:
– Topical corticosteroids– Cromolyn, nedocromil
• Inhibition of mediator action:– Antihistamines– Leukotriene receptor antagonists– Topical and systemic corticosteroids
Gell and Coombs Classification
• Type I (IgE-mediated)•• Type II (Fc and complement-mediated)Type II (Fc and complement-mediated)• Type III (Immune complex-mediated)• Type IV (Delayed-type hypersensitivity)
11
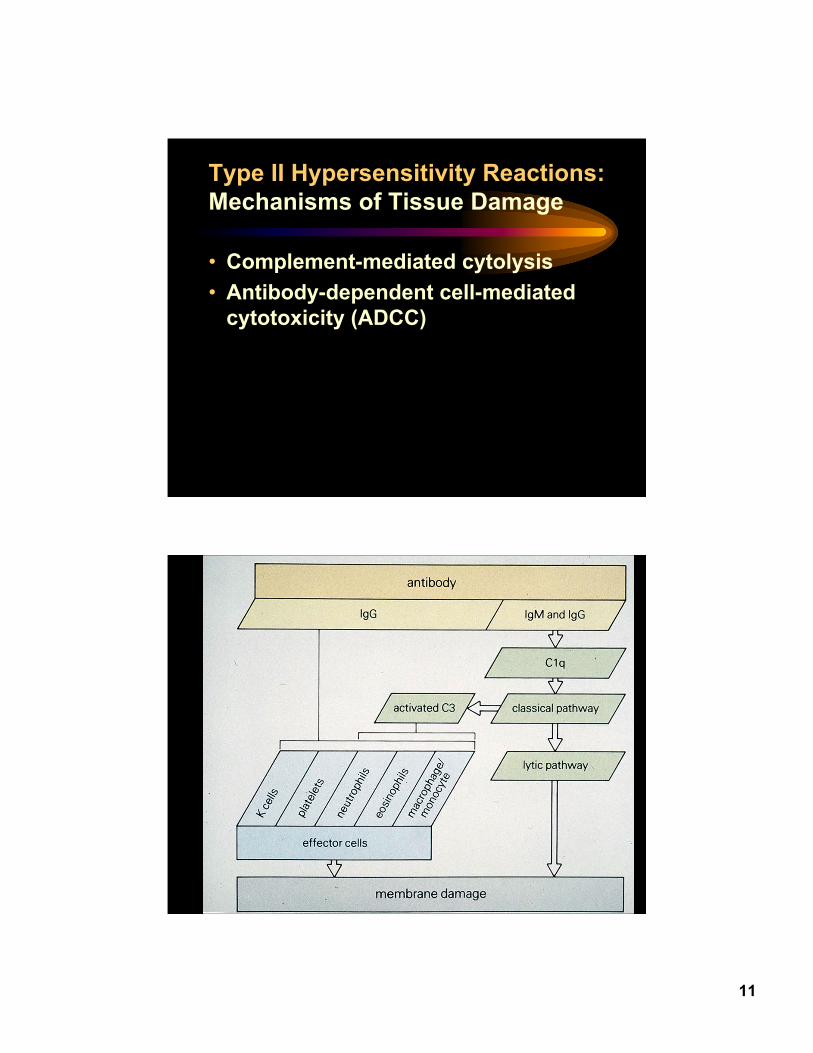
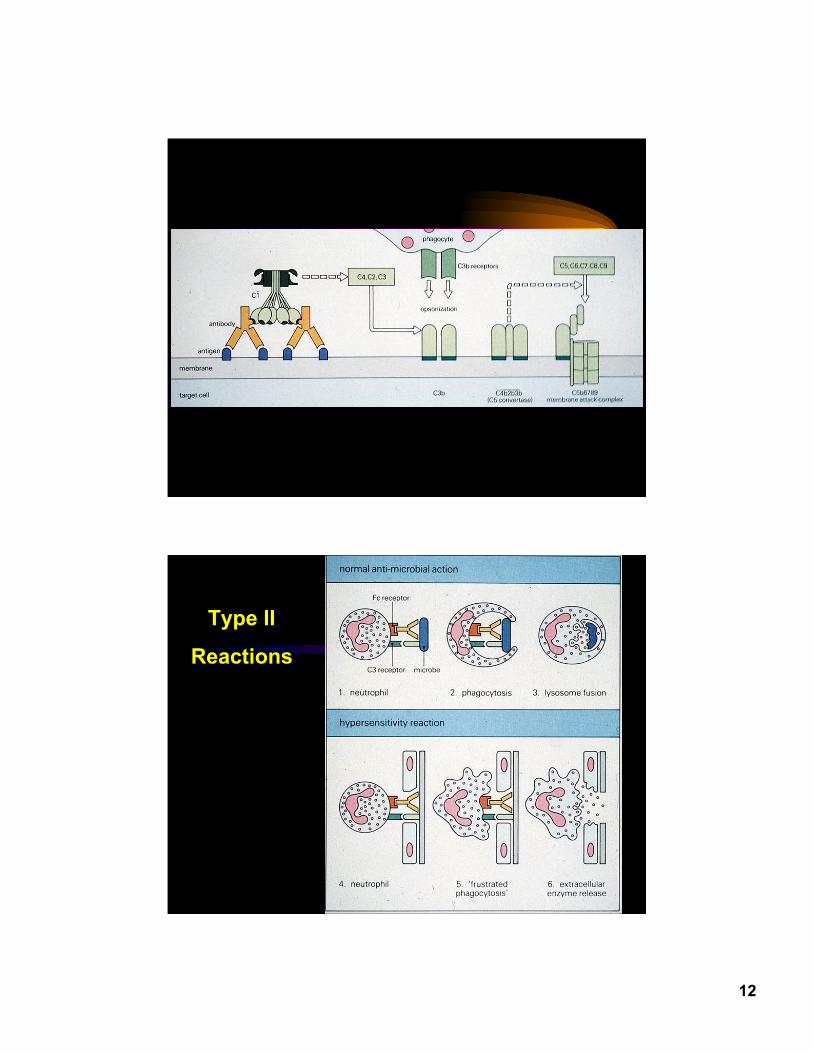
Type II Hypersensitivity Reactions:Mechanisms of Tissue Damage
• Complement-mediated cytolysis• Antibody-dependent cell-mediated
cytotoxicity (ADCC)
12
Type II
Reactions
13
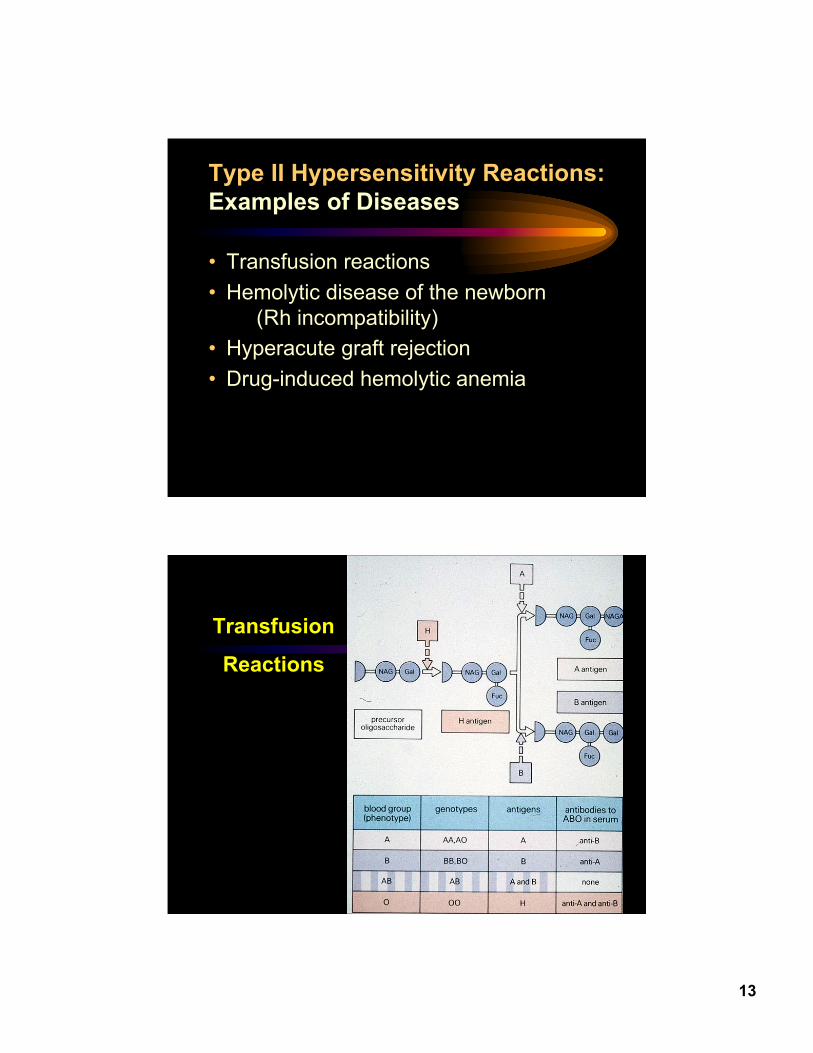
Type II Hypersensitivity Reactions:Examples of Diseases
• Transfusion reactions• Hemolytic disease of the newborn
(Rh incompatibility)• Hyperacute graft rejection• Drug-induced hemolytic anemia
Transfusion
Reactions
14
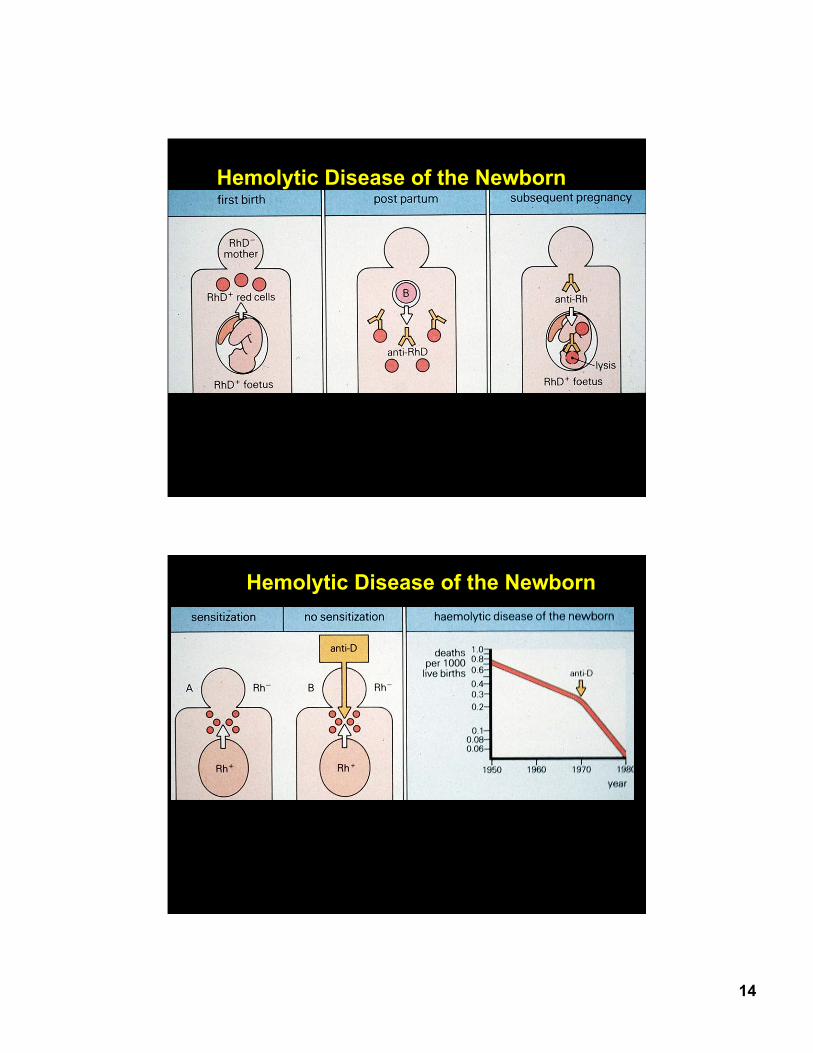
Hemolytic Disease of the Newborn
Hemolytic Disease of the Newborn
15
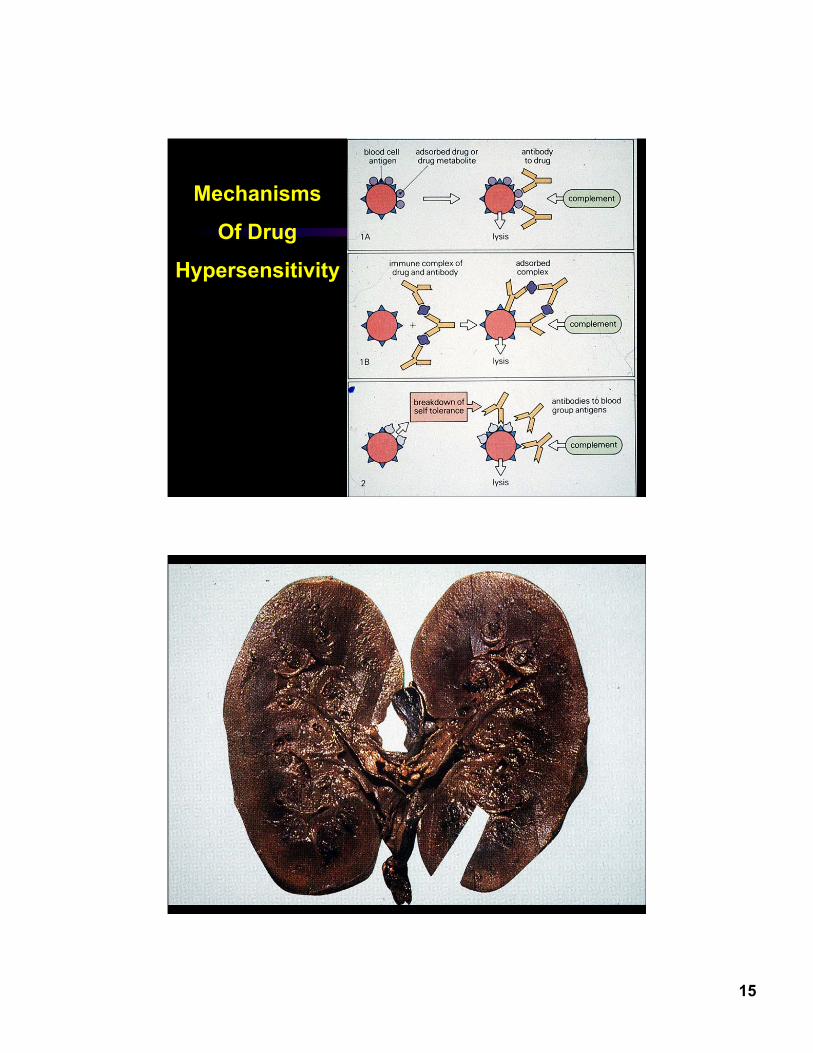
Mechanisms
Of Drug
Hypersensitivity
16
Gell and Coombs Classification
• Type I (IgE-mediated)• Type II (Fc and complement-mediated)•• Type III (Immune complex-mediated)Type III (Immune complex-mediated)• Type IV (Delayed-type hypersensitivity)
Type III HypersensitivityMechanisms of Tissue Injury
• In situ activation of complement• Anaphylatoxin-mediated activation of
mast cells and phagocytes• Complex-mediated phagocytosis and
release of phagocyte granule enzymesand cytokines into the localmicroenvironment
17
Type III HypersensitivityExamples of Diseases
• Arthus reaction• Hypersensitivity pneumonitis• Immune complex-mediated
glomerulonephritis• Serum sickness
The Arthus Reaction
• Occurs with introduction of antigen intoan individual with high titer antibody
• Requires both complement & phagocytes• Peaks at 3-6 hours after exposure• Histology: massive influx of neutrophils,
edema, sometimes necrosis
18
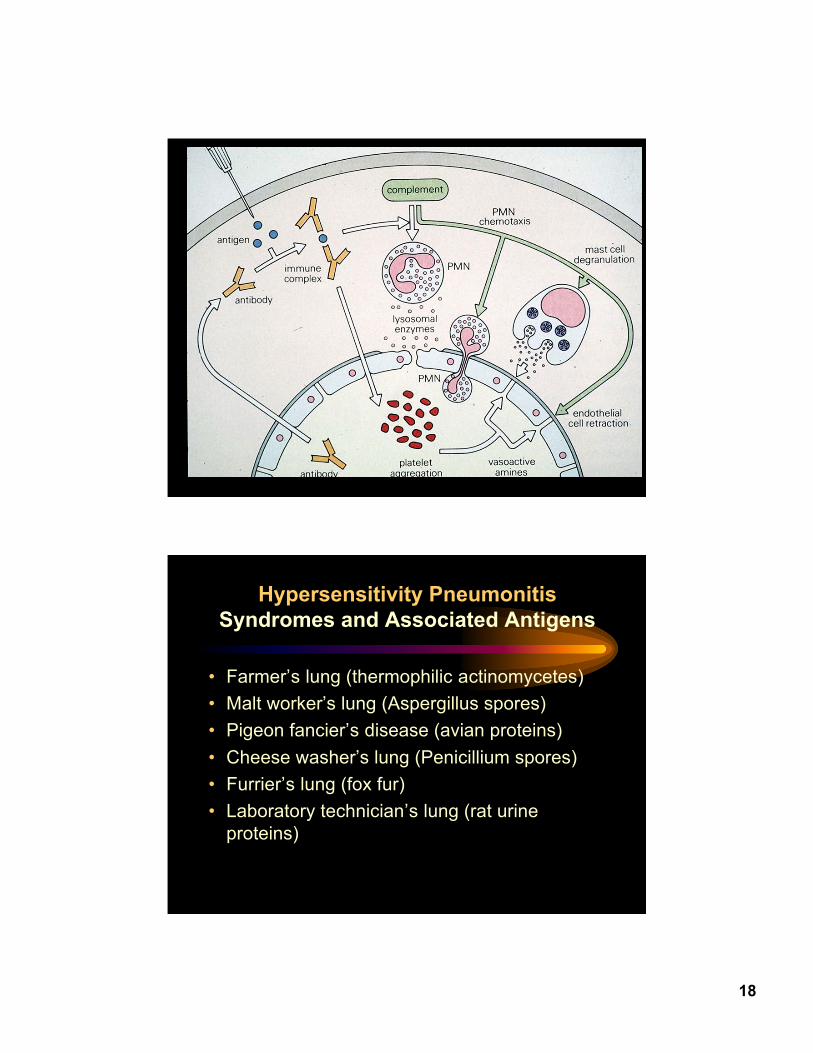
Hypersensitivity PneumonitisSyndromes and Associated Antigens
• Farmer’s lung (thermophilic actinomycetes)• Malt worker’s lung (Aspergillus spores)• Pigeon fancier’s disease (avian proteins)• Cheese washer’s lung (Penicillium spores)• Furrier’s lung (fox fur)• Laboratory technician’s lung (rat urine
proteins)
19
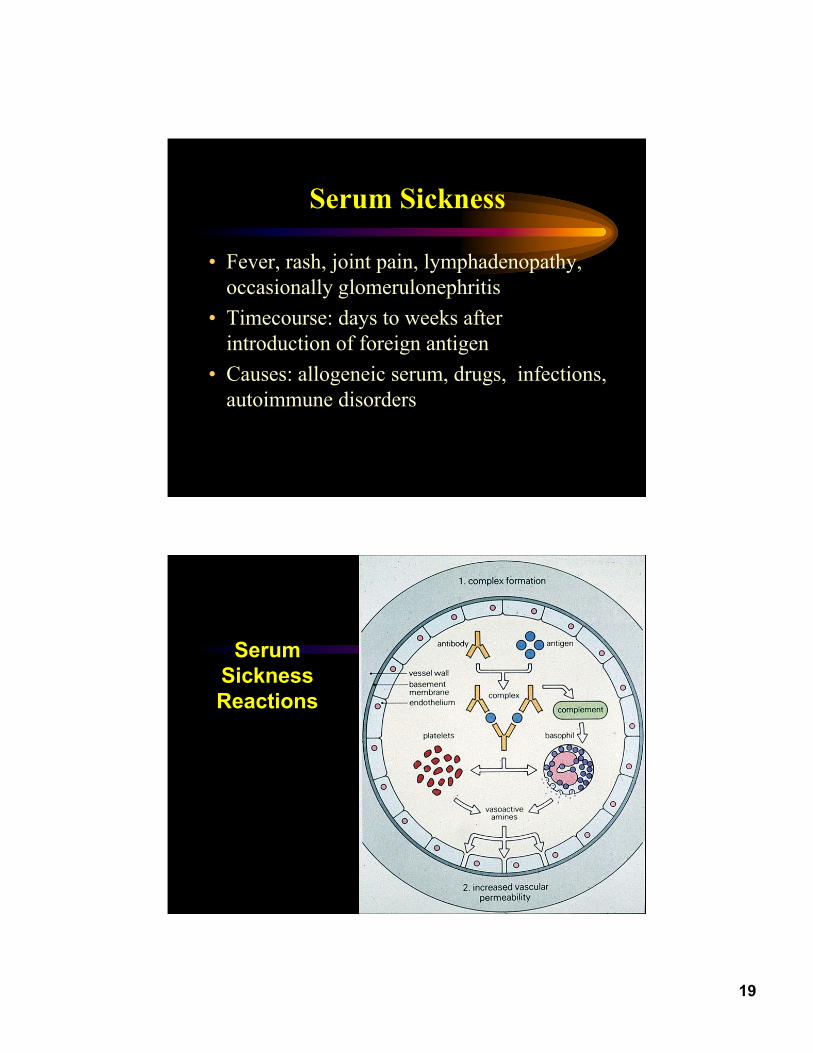
Serum Sickness
• Fever, rash, joint pain, lymphadenopathy,occasionally glomerulonephritis
• Timecourse: days to weeks afterintroduction of foreign antigen
• Causes: allogeneic serum, drugs, infections,autoimmune disorders
SerumSicknessReactions
20
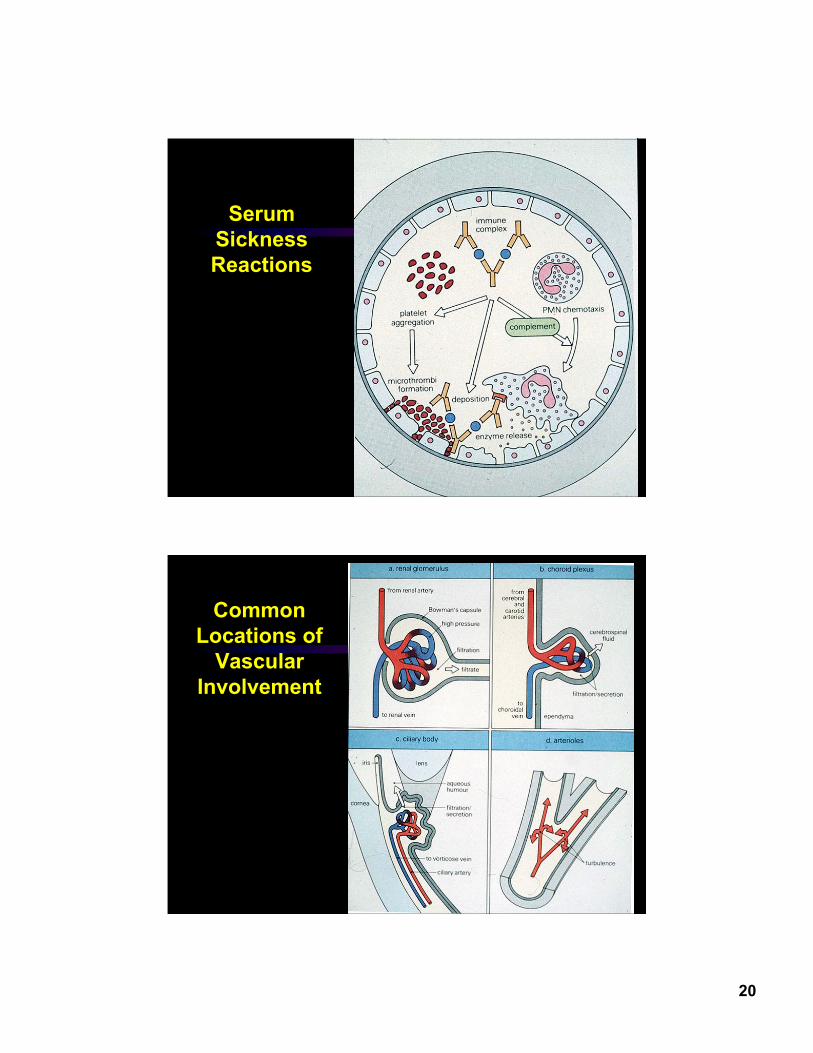
SerumSicknessReactions
CommonLocations of
VascularInvolvement
21
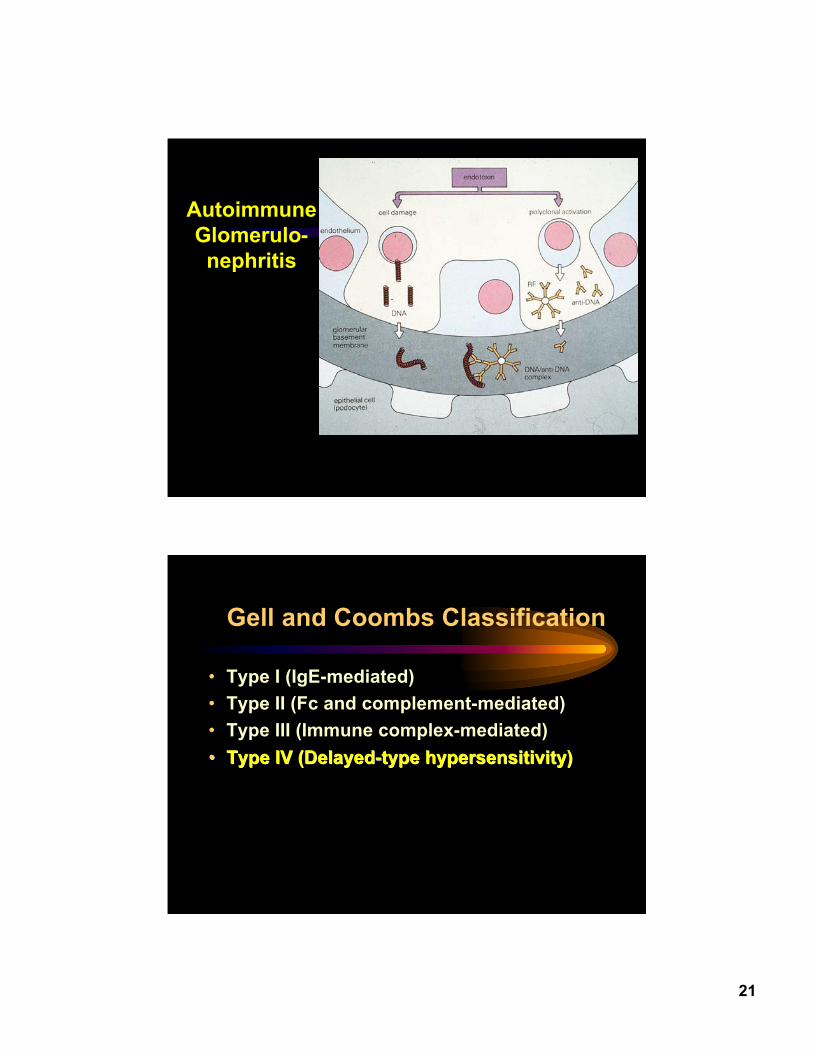
AutoimmuneGlomerulo-nephritis
Gell and Coombs Classification
• Type I (IgE-mediated)• Type II (Fc and complement-mediated)• Type III (Immune complex-mediated)•• Type IV (Delayed-type hypersensitivity)Type IV (Delayed-type hypersensitivity)
22
23
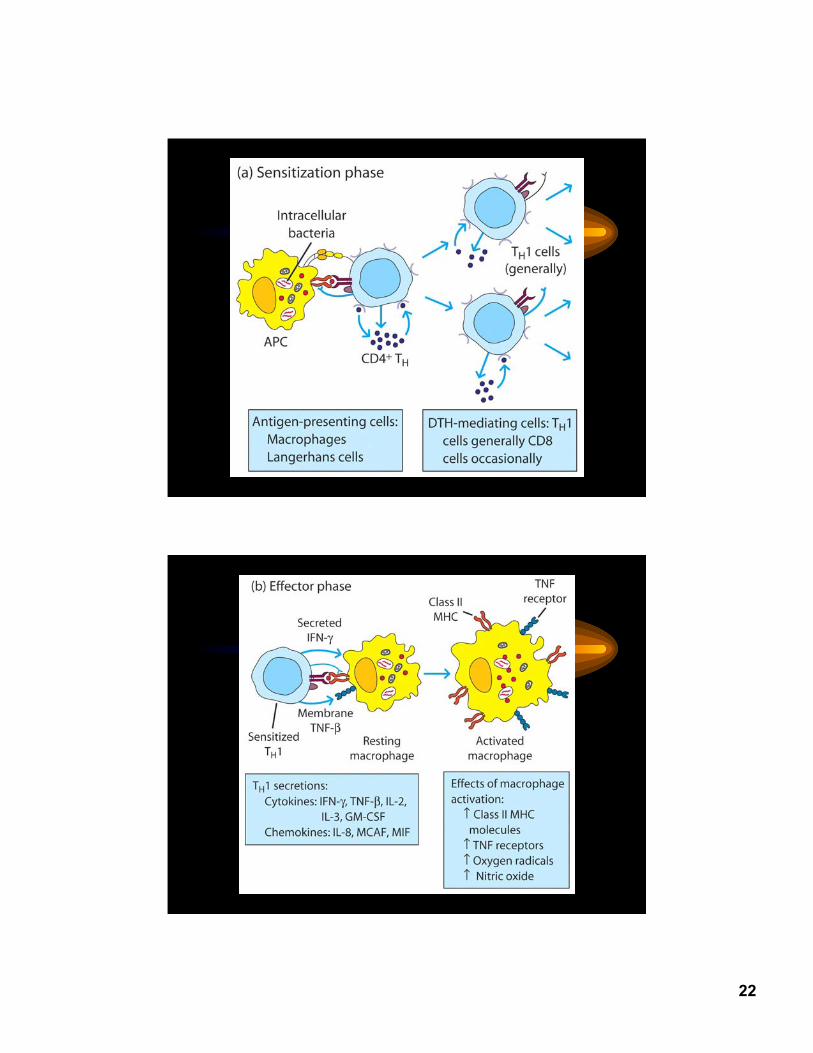
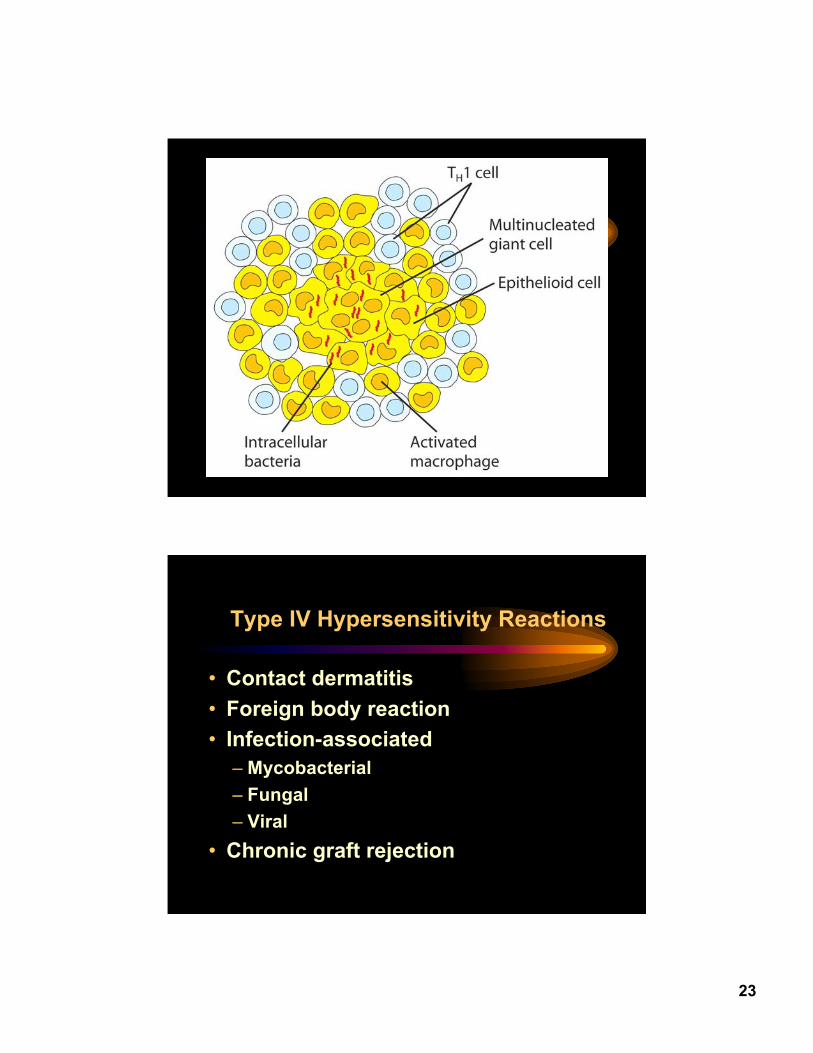
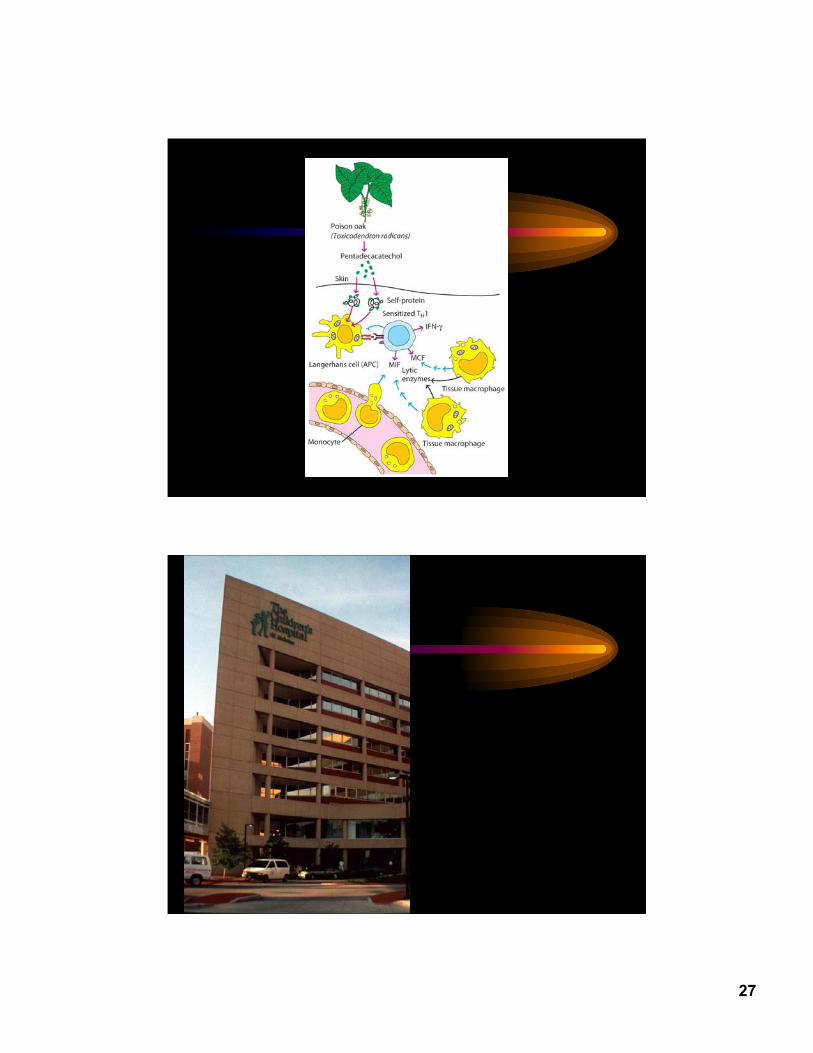
Type IV Hypersensitivity Reactions
• Contact dermatitis• Foreign body reaction• Infection-associated
– Mycobacterial– Fungal– Viral
• Chronic graft rejection
24
Ocular Allergy
• Allergic conjunctivitis• Vernal conjunctivitis• Atopic keratoconjunctivitis• Giant papillary conjunctivitis• Contact allergy
Ocular Contact Allergy: Causes
• Topical medications• Cosmetics, eyeliner, mascara• Hair products• Creams• Nail polish• Soaps, detergents• Numerous others
25
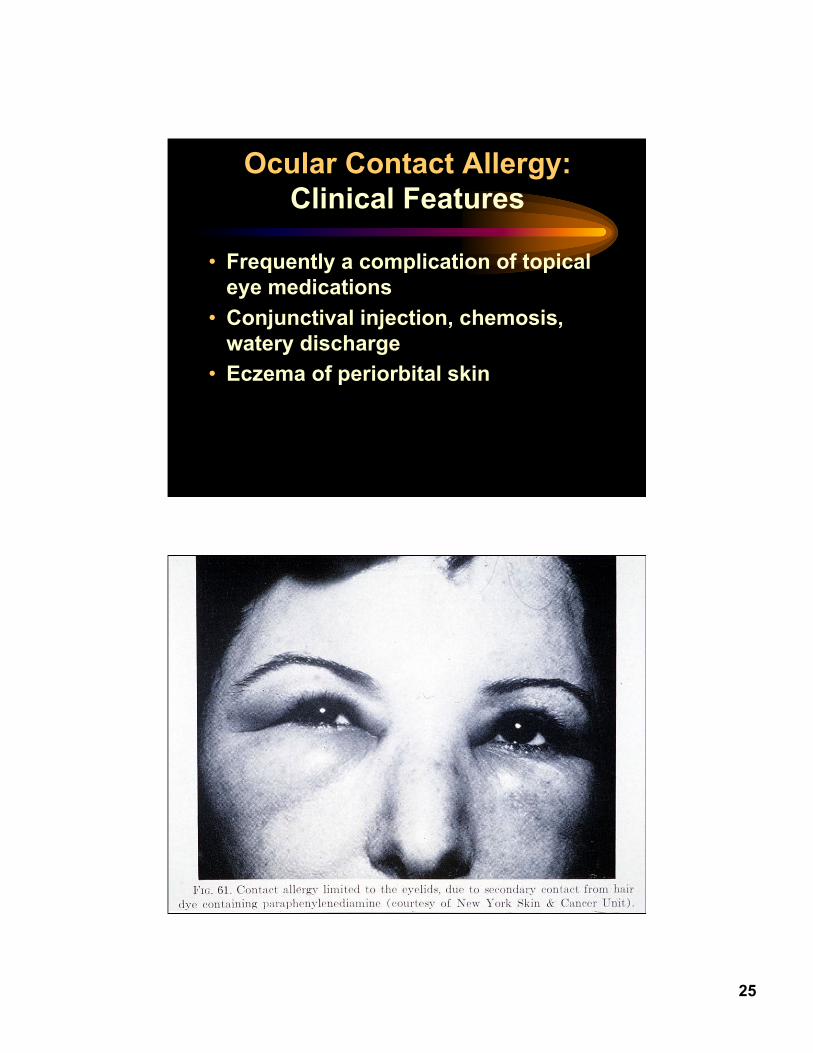
Ocular Contact Allergy:Clinical Features
• Frequently a complication of topicaleye medications
• Conjunctival injection, chemosis,watery discharge
• Eczema of periorbital skin
26
Ocular Contact Allergy:Therapy
• Remove offending agent• Cold compresses• Topical or systemic steroids
27


















