Definition + Diabetes Mellitus is a group of Metabolic Diseases characterized by Hyperglycemia...
77
-
Upload
winifred-chase -
Category
Documents
-
view
222 -
download
2
Transcript of Definition + Diabetes Mellitus is a group of Metabolic Diseases characterized by Hyperglycemia...

DefinitionDefinition
Diabetes Mellitus is a group of Metabolic Diseases
characterized by Hyperglycemia resulting from
defects in insulin secretion, insulin action, or both.
American Diabetes Association
Diabetes: Clinical FeaturesDiabetes: Clinical Features
Symptoms:Symptoms: PolyuriaPolyuria PolydipsiaPolydipsia == thirstthirst Polyphagia=Polyphagia= appetiteappetite Asthenia & Loss of weightAsthenia & Loss of weight
Signs:Signs:
No specific signs may be No specific signs may be signs of complicationssigns of complications
Signs:Signs:
No specific signs may be No specific signs may be signs of complicationssigns of complications

““Leonard Thompson (14 year Leonard Thompson (14 year old boy) & Elizabeth Hughes old boy) & Elizabeth Hughes (aged 14 years), were the first (aged 14 years), were the first
patients to be treated with patients to be treated with insulin in 1922.insulin in 1922.

““Fredrick BantingFredrick Banting (1921), (1921), successfully, extracted successfully, extracted
insulin, gaining the Nobel insulin, gaining the Nobel prize for this great prize for this great
discovery”.discovery”.

““Claude Bernard and Claude Bernard and Von Mering (1889), Von Mering (1889),
discovered in the same discovered in the same year that pancreatectomy year that pancreatectomy
causes diabetes”causes diabetes”

““Mathew Dobson (1776), Mathew Dobson (1776), identified glycosuria.identified glycosuria.
“ “ Thomas Willis (1621 - Thomas Willis (1621 - 1679), discovered the 1679), discovered the
sweetness of urine, hence, sweetness of urine, hence, the name Diabetes Mellitus the name Diabetes Mellitus
arised”arised”
“ “ Diabetes was long thought Diabetes was long thought to be a kidney disease (Greek to be a kidney disease (Greek
& Arabic Methodology).& Arabic Methodology).

Predisposing FactorsPredisposing FactorsIDDMIDDM
Heredity.Heredity. Histocomptability.Histocomptability. Virus infection.Virus infection. Seasonality.Seasonality. Cell-mediated immunity.Cell-mediated immunity.

Insulin SynthesisInsulin Synthesis
PrePro Insulin
Pro Insulin
C peptideInsulin
Split at position61/62

Insulin Secretion CurveInsulin Secretion Curve
Biphasic insulin response to a constant glucose stimulation(IVGTT - hyperglycemic Clamp)
Insulin rate
Time (min)
Basal
4 60
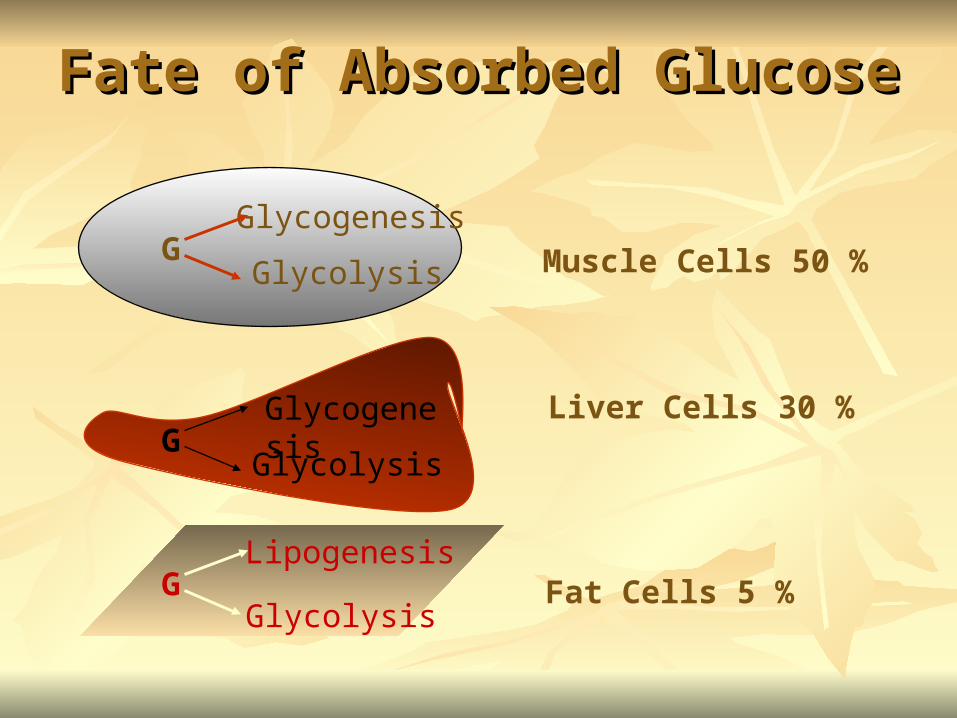
Fate of Absorbed GlucoseFate of Absorbed Glucose
GGlycogenesis
Glycolysis Muscle Cells 50 %
GGlycolysis
Lipogenesis
GGlycogenesis
Glycolysis
Liver Cells 30 %
Fat Cells 5 %

Hormonal RegulationHormonal Regulation
Blood Glucose Level
< 110 mg/L
Insulin
GlucagonsGrowth Hormone
AdrenalineCortisol
Hypoglycaemic Hormone Counter regulatory Hormones
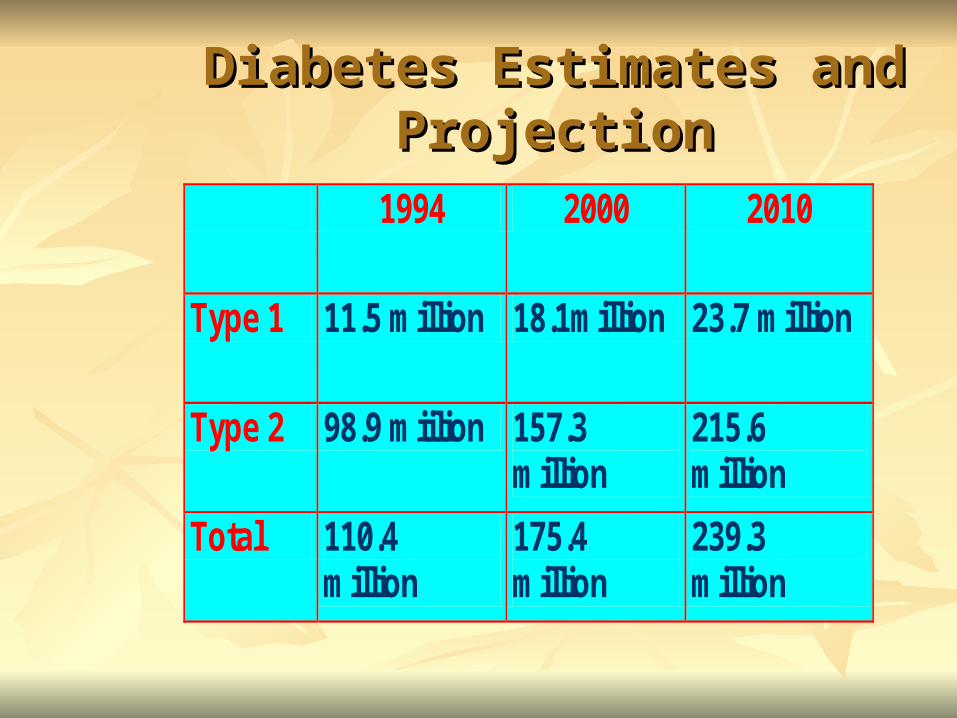
Diabetes Estimates and Diabetes Estimates and ProjectionProjection
1994 2000 2010
Type 1 11.5 million 18.1million 23.7 million
Type 2 98.9 miilion 157.3 million
215.6 million
Total 110.4 million
175.4 million
239.3 million
Classification of Diabetes Classification of Diabetes MellitusMellitus
Primary DiabetesPrimary Diabetes
Type 1Type 1 insulin dependent insulin dependent
diabetesdiabetes
Type 2Type 2 non insulin non insulin
dependent diabetesdependent diabetes

Secondary DiabetesSecondary Diabetes Gestational diabetesGestational diabetes Malnutrition related diabetesMalnutrition related diabetes Diabetes resulting from:Diabetes resulting from:
Pancreatic diseasePancreatic disease Hormonal diseasesHormonal diseases Drug/chemical inducedDrug/chemical induced Genetic syndromesGenetic syndromes
Secondary DiabetesSecondary Diabetes Gestational diabetesGestational diabetes Malnutrition related diabetesMalnutrition related diabetes Diabetes resulting from:Diabetes resulting from:
Pancreatic diseasePancreatic disease Hormonal diseasesHormonal diseases Drug/chemical inducedDrug/chemical induced Genetic syndromesGenetic syndromes
Classification of Diabetes Classification of Diabetes MellitusMellitus

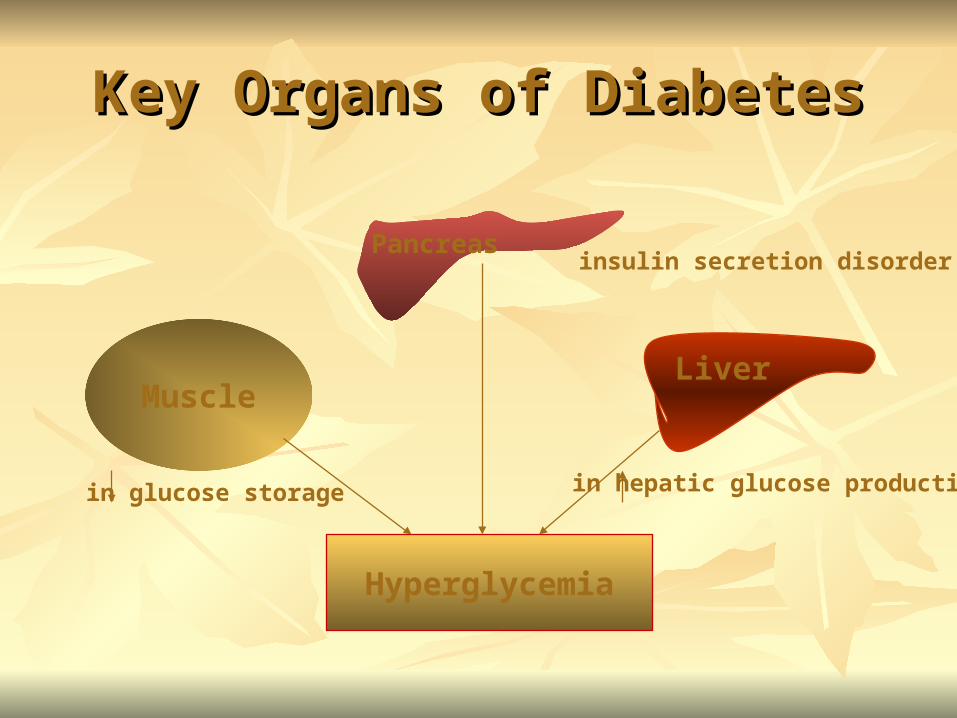
Key Organs of DiabetesKey Organs of Diabetes
Muscle
Pancreas
Liver
Hyperglycemia
in glucose storage in hepatic glucose production
insulin secretion disorder
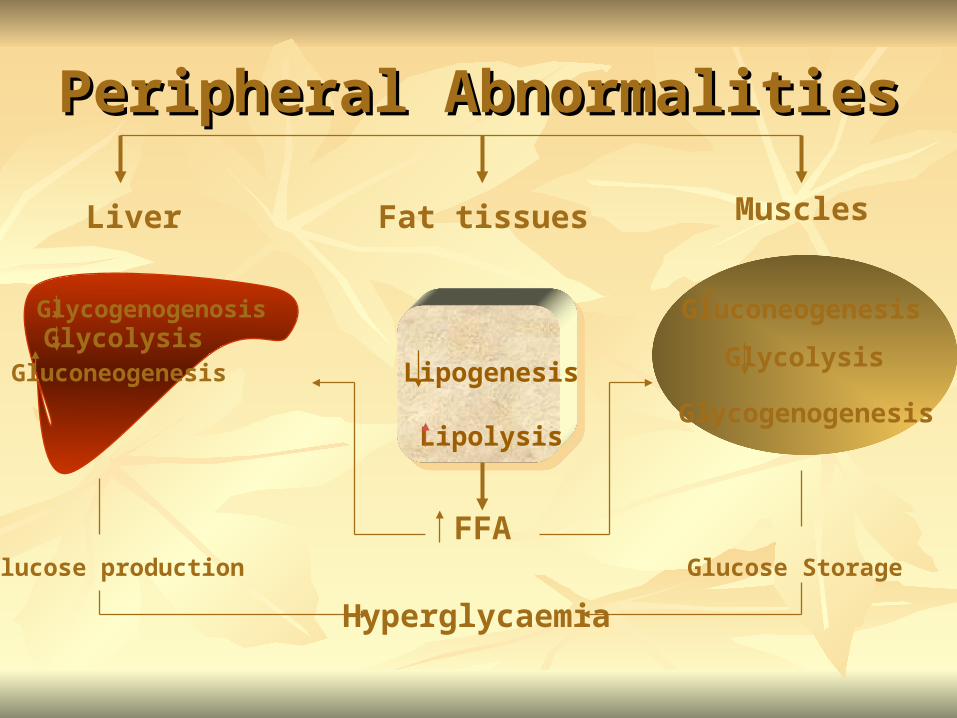
Peripheral AbnormalitiesPeripheral Abnormalities
GlycogenogenosisGlycolysis
Gluconeogenesis Lipogenesis
LipolysisGlycogenogenesis
Glycolysis
Gluconeogenesis
Liver Fat tissues Muscles
FFA
Hyperglycaemia
Glucose StorageGlucose production
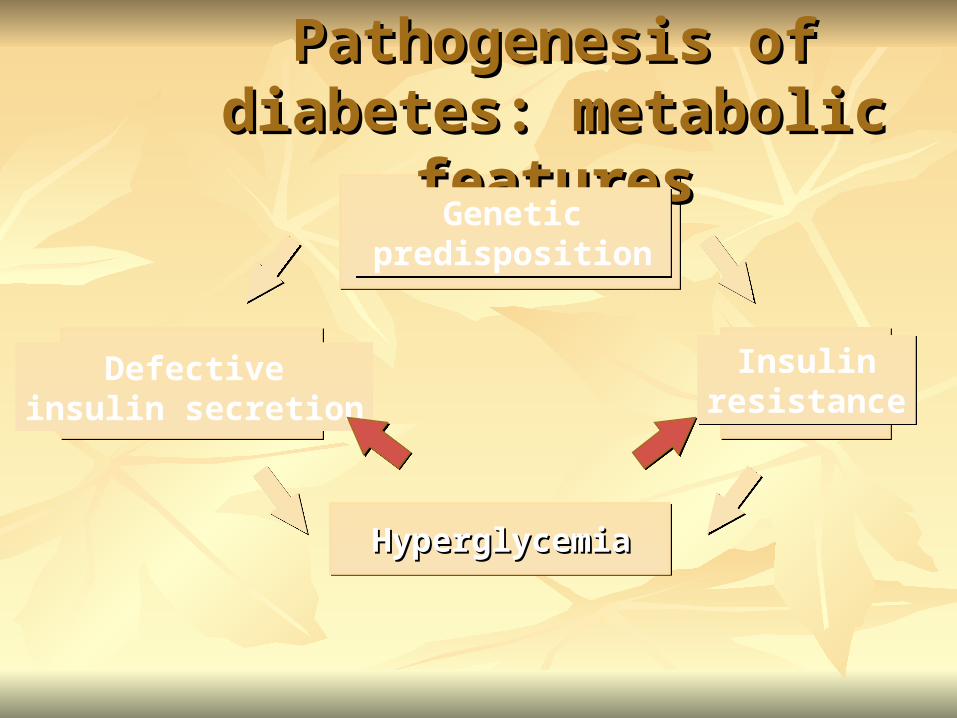
Pathogenesis of diabetes: Pathogenesis of diabetes: metabolic featuresmetabolic features
Genetic predisposition
Genetic predisposition
Insulinresistance
Insulinresistance
Defectiveinsulin secretion
HyperglycemiaHyperglycemia

Causes of Impaired Insulin Causes of Impaired Insulin SecretionSecretion
Causes of Impaired Insulin Causes of Impaired Insulin SecretionSecretion
Decrease in number of Beta cells by 40-50 %Decrease in number of Beta cells by 40-50 %
{{In Insulin resistance statesIn Insulin resistance states,,
the number is either normal or increased}the number is either normal or increased}

Amyloid depositsAmyloid deposits
Amylin : amyloid materialAmylin : amyloid materialsecreted by B cells secreted by B cells Interferes Interferes with the with the recognition ofrecognition of
the glucose signalthe glucose signal
Causes of Impaired Insulin Causes of Impaired Insulin SecretionSecretion
Causes of Impaired Insulin Causes of Impaired Insulin SecretionSecretion
Reduced activity of the Reduced activity of the glucokinaseglucokinase
ATP production reduced inside B cellsATP production reduced inside B cells
Closure of K channel decreasesClosure of K channel decreases
Entry of Calcium reduced Entry of Calcium reduced
release of Insulin reducedrelease of Insulin reduced
Causes of Impaired Insulin Causes of Impaired Insulin SecretionSecretion


Types of Insulin ResistanceTypes of Insulin Resistance
Receptor defectReceptor defect
Post Receptor defectPost Receptor defect
Types of Insulin Types of Insulin ResistanceResistance
Receptor defectReceptor defect
Decrease in the affinityDecrease in the affinity
Decrease in number (rare)Decrease in number (rare)

Post receptor defectPost receptor defect
Glucose TransportersGlucose Transporters
Intra cellular utilizationIntra cellular utilization
Enzymatic activityEnzymatic activity
Types of Insulin ResistanceTypes of Insulin Resistance
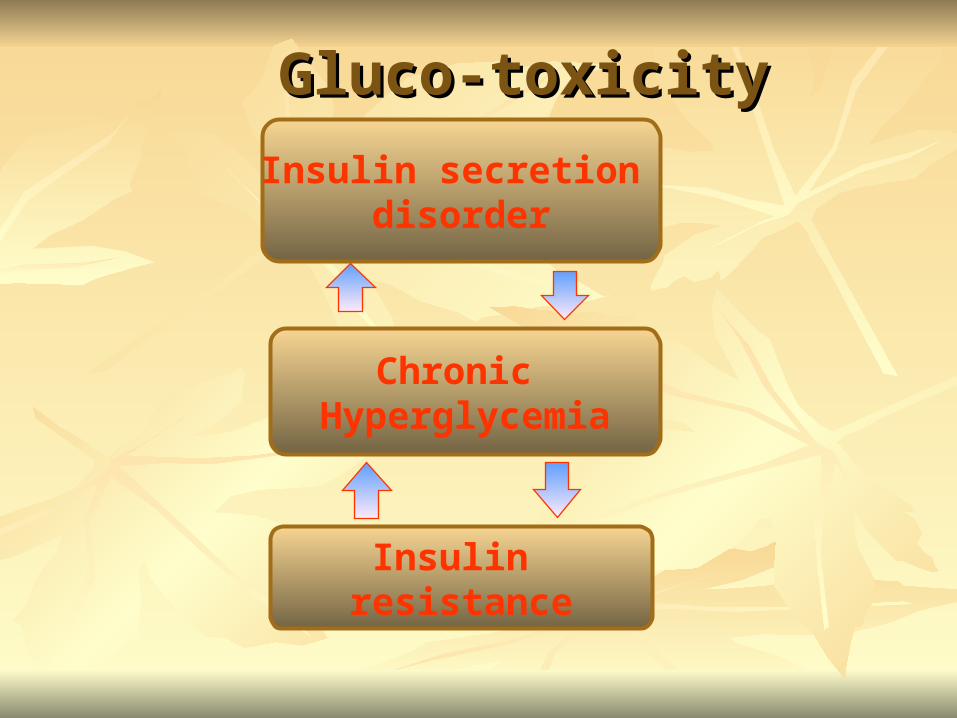
Chronic Hyperglycemia
Insulin secretion disorder
Insulin resistance
Gluco-toxicityGluco-toxicity

Vascular complicationsVascular complications
Micro-vascular complicationsMicro-vascular complications
Macro-vascular complicationsMacro-vascular complications
Micro-vascular complicationsMicro-vascular complications
Retinopathy Retinopathy
NephropathyNephropathy
Neuropathy Neuropathy

Macro-vascular complicationsMacro-vascular complications
CHDCHD
CVDCVD
PADPAD
10 years accelerated 10 years accelerated


Treatment of diabetesTreatment of diabetes::
Life style modificationLife style modification
InsulinInsulin
Oral hypoglycemic agentsOral hypoglycemic agents
Life style modificationLife style modification
Diet controlDiet control
ExerciseExercise
Smoking cessation Smoking cessation

DIET CONTROLDIET CONTROL
All diabetic patients should be on diet All diabetic patients should be on diet
control.control.
Diet control is a must either the patient Diet control is a must either the patient
is taking insulin or oral therapy. is taking insulin or oral therapy.
Over weight should be reduced .Over weight should be reduced .
Diet control should be tried at first Diet control should be tried at first
before the next step [insulin or before the next step [insulin or
tablets] especially in obese tablets] especially in obese
patients, When diet fails drugs are patients, When diet fails drugs are
indicated. indicated.
DIET CONTROLDIET CONTROL

The diet for a diabetic patient is not so The diet for a diabetic patient is not so
different from the healthy diets for the different from the healthy diets for the
whole population.whole population.
Simple sugars Carbohydrate [as Simple sugars Carbohydrate [as
sucrose], should be limited for the diet sucrose], should be limited for the diet
of diabetic patients.of diabetic patients.
DIET CONTROLDIET CONTROL
Carbohydrate content should be in a Carbohydrate content should be in a
fiber-rich diet [for example fruits fiber-rich diet [for example fruits
containing fibers as apples]. containing fibers as apples].
… ….. because the fiber content of diet .. because the fiber content of diet
delays absorption of carbohydrates delays absorption of carbohydrates
avoiding the rapid elevation of blood avoiding the rapid elevation of blood
glucose levels. glucose levels.
DIET CONTROLDIET CONTROL

Calories :Calories : • Calories should be tailored to the need Calories should be tailored to the need
of the patient. of the patient.
Diet should containDiet should contain:: Carbohydrates → 50 - 55% Carbohydrates → 50 - 55% Fat→ 30-35% Fat→ 30-35% Protein →10 - 15%Protein →10 - 15%
DIET CONTROLDIET CONTROL


Indication of InsulinIndication of Insulin
Type 1 diabetesType 1 diabetes
Unstable diabetesUnstable diabetes
Type 2 diabetes failed on SUs.Type 2 diabetes failed on SUs.
Pregnant diabetic patientsPregnant diabetic patients
Surgery (all diabetic patients)Surgery (all diabetic patients)
Diabetic comaDiabetic coma


Oral hypoglycemic agentsOral hypoglycemic agents
BiguanidesBiguanides
SulfonylureasSulfonylureas
αα- glucosidase inhibitors - glucosidase inhibitors
ThiazolidinedionesThiazolidinediones
Prandial glucose regulatorPrandial glucose regulator

BiguanidesBiguanides
Biguanides are derivatives of the Biguanides are derivatives of the
antimalarial agent Chloroguanide. antimalarial agent Chloroguanide.
Which is found to have hypoglycemic Which is found to have hypoglycemic
action. action.
The most commonly used member of The most commonly used member of
biguanides is Metformin [Cidophage]. biguanides is Metformin [Cidophage].

BiguanidesBiguanides
Indication:Indication:
Type 2 diabetes failed on dietType 2 diabetes failed on diet
Metformin can be given alone or in Metformin can be given alone or in
combination with sulfonylureas or Insulincombination with sulfonylureas or Insulin

BiguanidesBiguanides
Mode of actionMode of action
Biguanides [Metformin] is an Biguanides [Metformin] is an
Antihyperglycemic and not Hypoglycemic Antihyperglycemic and not Hypoglycemic
agent. agent. It does not stimulate pancreas to secrete insulin It does not stimulate pancreas to secrete insulin
and does not cause hypoglycemia (as a side and does not cause hypoglycemia (as a side
effect) even in large doses. effect) even in large doses.
Also it has no effect on secretion of Glucagon or Also it has no effect on secretion of Glucagon or
Somatostatin. Somatostatin.
BiguanidesBiguanides
Mode of action:Mode of action: Decreases the intestinal absorption of Decreases the intestinal absorption of
CHOCHO Increases glucose uptake (GLUT 4)Increases glucose uptake (GLUT 4) Increases glucose utilization Increases glucose utilization
(glycogensynthase)(glycogensynthase) Increases glycolysis via anaerobic Increases glycolysis via anaerobic
pathway (lactic acidosis)pathway (lactic acidosis)

BiguanidesBiguanides
Pharmacokinetics:Pharmacokinetics: Metformin is well absorbed from Metformin is well absorbed from
small intestine, stable, does not small intestine, stable, does not bind to plasma proteins, excreted bind to plasma proteins, excreted unchanged in urine. unchanged in urine.
Half life of Metformin is 1.5 - Half life of Metformin is 1.5 - 4.5 hours, taken in three doses 4.5 hours, taken in three doses with mealswith meals
BiguanidesBiguanides
Side effects:Side effects:
occur in 20-25 % of patients. occur in 20-25 % of patients.
include.. Diarrhea, abdominalinclude.. Diarrhea, abdominal
discomfort, nausea, metallic taste discomfort, nausea, metallic taste
and decreased absorption of and decreased absorption of
vitamin Bvitamin B1212. .

BiguanidesBiguanides
ContraindicationsContraindications Patients with renal or hepatic Patients with renal or hepatic
impairment. impairment. Past history of lactic acidosis. Past history of lactic acidosis. Heart failure, Chronic lung disease. Heart failure, Chronic lung disease.
.. These conditions predispose to .. These conditions predispose to increased lactate production which increased lactate production which causes lactic acidosis which is fatal. causes lactic acidosis which is fatal.

SUs., have been discovered during SUs., have been discovered during
the 2the 2ndnd. World war (sulfonamide).. World war (sulfonamide).
SUs are drugs that used orally to SUs are drugs that used orally to
control blood glucose levels of type 2 control blood glucose levels of type 2
diabetes.diabetes.
SULFONYLUREASSULFONYLUREAS

SULFONYLUREASSULFONYLUREAS Types:Types:
First generation, First generation, Chlorpropamide (Chlorpropamide (PamidinPamidin)) Tolbutamide (Tolbutamide (DiamolDiamol))
Second generation,Second generation, Gliclazide (Gliclazide (DiamicronDiamicron)) Glibenclamide (Glibenclamide (DaonilDaonil)) Glipizide (Glipizide (MinidiabMinidiab))
Third generation,Third generation, Glimepiride (Glimepiride (DiabrideDiabride) () (AmarylAmaryl))
SULFONYLUREASSULFONYLUREAS
Mechanism of action:Mechanism of action:
Pancreatic effectPancreatic effect
Extra-pancreatic effectExtra-pancreatic effect
Pancreatic effect:Pancreatic effect:
• Increase insulin release from Increase insulin release from
pancreaspancreas
• Suppress secretions of GlucagonsSuppress secretions of Glucagons
SULFONYLUREASSULFONYLUREAS
SULFONYLUREASSULFONYLUREAS Extra pancreatic effect:Extra pancreatic effect:
Increases the number of insulin Increases the number of insulin receptorsreceptors
Increases post-receptor insulin Increases post-receptor insulin sensitivitysensitivity
Increases glucolysisIncreases glucolysis Increases glycogen storage in muscle Increases glycogen storage in muscle
and liverand liver Decreases the hepatic output of glucoseDecreases the hepatic output of glucose
SULFONYLUREASSULFONYLUREAS Pharmacokinetics:Pharmacokinetics:
They are effectively absorbed from They are effectively absorbed from gastrointestinal tract.gastrointestinal tract.
Food can reduce the absorption of Food can reduce the absorption of sulfonylurea.sulfonylurea.
Sulfonylureas are more effective Sulfonylureas are more effective when given 30 minutes before eating.when given 30 minutes before eating.
Plasma protein binding is high 90 – Plasma protein binding is high 90 – 99 % .. mainly bind to albumen.99 % .. mainly bind to albumen.

SULFONYLUREASSULFONYLUREAS
Pharmacokinetics:Pharmacokinetics: 11stst generation members have short generation members have short
half lives.half lives.
22ndnd generation is administered once, generation is administered once,
twice or several times daily.twice or several times daily.
33rdrd generation is administered once generation is administered once
daily. daily.
SULFONYLUREASSULFONYLUREAS Pharmacokinetics:Pharmacokinetics:
All sulfonylurea are metabolized by All sulfonylurea are metabolized by
liver and their metabolites are excreted liver and their metabolites are excreted
in urine with about 20 % excreted in urine with about 20 % excreted
unchanged.unchanged.
Sulfonylurea should be administered Sulfonylurea should be administered
with caution to patients with either with caution to patients with either
renal or hepatic insufficiency.renal or hepatic insufficiency.

SULFONYLUREASSULFONYLUREAS
Adverse Reactions :Adverse Reactions : Very few adverse reactions [4 %] in the first Very few adverse reactions [4 %] in the first
generation and rare in the 2generation and rare in the 2ndnd and 3 and 3rdrd generation. generation.
SUs may induce hypoglycemia especially in SUs may induce hypoglycemia especially in elderly patients with impaired hepatic or elderly patients with impaired hepatic or renal functions-These cases of hypoglycemia renal functions-These cases of hypoglycemia are treated by I/V glucose infusion. are treated by I/V glucose infusion.

SULFONYLUREASSULFONYLUREAS
Adverse Reactions :Adverse Reactions : First generation may induce other First generation may induce other
side effects as …nausea and side effects as …nausea and vomiting & dermatological vomiting & dermatological reactions reactions
……These side effects are fewer in the These side effects are fewer in the 22ndnd generation and rare in the 3 generation and rare in the 3rdrd generationgeneration..
SULFONYLUREASSULFONYLUREAS
Drug interactions:Drug interactions: Some drugs may enhance or Some drugs may enhance or
suppress the actions of suppress the actions of sulfonylureas Either by affecting:sulfonylureas Either by affecting: Their metabolism and excretion Their metabolism and excretion The concentration of free The concentration of free
sulfonylureas in plasma through sulfonylureas in plasma through competing them on plasma proteins.competing them on plasma proteins.
SULFONYLUREASSULFONYLUREAS
Contraindications :Contraindications :
Type 1 DMType 1 DM
Pregnancy and Lactation. Pregnancy and Lactation.
Significant hepatic or renal failure. Significant hepatic or renal failure.

Drug – Drug interactionDrug – Drug interaction
NSAIDsNSAIDs
SalicylatesSalicylates
SulfonamideSulfonamide
ß-blockersß-blockers
ChloramphenicolChloramphenicol
DiazepamDiazepam
MAOIMAOI
BarbituratesBarbiturates
Thiazide and loop Thiazide and loop
diureticsdiuretics
SympathomimeticsSympathomimetics
CorticosteroidsCorticosteroids
Oestrogen / Oestrogen /
Progesterone Progesterone
combinationscombinations

α Glycosidase Inhibititorα Glycosidase Inhibititorα Glycosidase Inhibititorα Glycosidase Inhibititor
Acarbose (Glucobay)Acarbose (Glucobay)
Indicated for type 2 diabetesIndicated for type 2 diabetes In addition with diet In addition with diet
In addition with other anti-diabetic In addition with other anti-diabetic
therapiestherapies

Acarbose (Glucobay)Acarbose (Glucobay)
Mode of action:Mode of action: Poorly absorbed 1% (act locally in Poorly absorbed 1% (act locally in
G.I.T.)G.I.T.) Inhibits Inhibits α glucosidase, so inhibits α glucosidase, so inhibits
CHO degradationCHO degradation Dose:Dose:
50mg to 100mg 3 times daily before 50mg to 100mg 3 times daily before mealsmeals

Acarbose (Glucobay)Acarbose (Glucobay)
Side effects:Side effects:
Flatulence (77%) Flatulence (77%)
DiarrheaDiarrhea
Abdominal pain (21%)Abdominal pain (21%)
Decreased iron absorptionDecreased iron absorption
ThiazolidenedioneThiazolidenedioneThiazolidenedioneThiazolidenedione
Rosiglitazone (Avandia)Rosiglitazone (Avandia)
Pioglitazone (Actos)Pioglitazone (Actos)
ThiazolidenedioneThiazolidenedione Mode of action:Mode of action:
Insulin sensitizer (increase insulin sensitivity Insulin sensitizer (increase insulin sensitivity in muscle, adipose tissue & liver)in muscle, adipose tissue & liver)
They are not insulin secretagogues (Not They are not insulin secretagogues (Not
insulin releasers)insulin releasers)
ThiazolidenedioneThiazolidenedione Drawbacks:Drawbacks:
They are not effective alone in case of They are not effective alone in case of severe insulin deficiency and should be severe insulin deficiency and should be combined with sulfonylurea or metformin combined with sulfonylurea or metformin or bothor both
Side effects:Side effects: Hepatotoxicity Hepatotoxicity weight gainweight gain Dyslipidaemia (increases LDL) Dyslipidaemia (increases LDL)

Prandial glucose regulators Prandial glucose regulators ((Meglitinide)Meglitinide)
Prandial glucose regulators Prandial glucose regulators ((Meglitinide)Meglitinide)
Example:Example: Repaglinide, Novonorm (NovoNordisk)Repaglinide, Novonorm (NovoNordisk)
Rational:Rational: Fast acting, short duration non-sulfonylureaFast acting, short duration non-sulfonylurea Designed to minimize mealtime blood Designed to minimize mealtime blood
glucose peaksglucose peaks
Repaglinide, NovonormRepaglinide, NovonormRepaglinide, NovonormRepaglinide, Novonorm
Mechanism of action:Mechanism of action: Stimulation of pancreatic insulin Stimulation of pancreatic insulin
release by closing ß-cells Krelease by closing ß-cells KATPATP
channelschannels Very rapid onset of action and short Very rapid onset of action and short
duration (Tduration (TMAXMAX = 1 hour, metabolized = 1 hour, metabolized
by liver Tby liver T1/2 1/2 = 70 minutes)= 70 minutes) No hypoglycemic metabolitesNo hypoglycemic metabolites
Repaglinide, NovonormRepaglinide, NovonormRepaglinide, NovonormRepaglinide, Novonorm
Clinical efficacy:Clinical efficacy: Improves postprandial glycemia Improves postprandial glycemia Less effective in decreasing fasting blood Less effective in decreasing fasting blood
glucose levels and HbAglucose levels and HbA1C1C
drawbacks:drawbacks: Fails to provides a stable 24 hours blood Fails to provides a stable 24 hours blood
glucose controlglucose control Complicated dosage style (3-8 tablets/daily)Complicated dosage style (3-8 tablets/daily) How to adapt the dosage to the meal How to adapt the dosage to the meal
volume?volume?

SEDICOSEDICOPharmaceuticalsPharmaceuticals