
Default Mode Connectivity in Major Depressive Disorder...
9
Archival Report Default Mode Connectivity in Major Depressive Disorder Measured Up to 10 Days After Ketamine Administration Jennifer W. Evans, Joanna Szczepanik, Nancy Brutsché, Lawrence T. Park, Allison C. Nugent, and Carlos A. Zarate Jr. ABSTRACT BACKGROUND: The symptoms of major depressive disorder (MDD) are rapidly alleviated by administration of a single dose of the glutamatergic modulator ketamine. However, few studies have investigated the potential sustained neural effects of this agent beyond immediate infusion. This study used functional magnetic resonance imaging to examine the effect of a single ketamine infusion on the resting state default mode network (DMN) at 2 and 10 days after a single ketamine infusion in unmedicated subjects with MDD as well as healthy control subjects (HCs). METHODS: Data were drawn from a double-blind, placebo-controlled crossover study of 58 participants (33 with MDD and 25 HCs) who received an intravenous infusion of either ketamine hydrochloride (0.5 mg/kg) or placebo on 2 separate test days spaced 2 weeks apart. Eight minutes of functional magnetic resonance imaging resting state data was acquired at baseline and at about 2 and 10 days after both infusions. The DMN was defined using seed-based correlation and was compared across groups and scans. RESULTS: In subjects with MDD, connectivity between the insula and the DMN was normalized compared with HCs 2 days postketamine infusion. This change was reversed after 10 days and did not appear in either of the placebo scans. Group-specific connectivity differences in drug response were observed, most notably in the insula in subjects with MDD and in the thalamus in HCs. CONCLUSIONS: Connectivity changes in the insula in subjects with MDD suggest that ketamine may normalize the interaction between the DMN and salience networks, supporting the triple network dysfunction model of MDD. Keywords: Default mode network, Functional magnetic resonance imaging (fMRI), Glutamatergic modulator, Ketamine, Major depressive disorder, Resting state https://doi.org/10.1016/j.biopsych.2018.01.027 Major depressive disorder (MDD) is a common mental disorder (1,2) predicted to be the leading cause of disease burden worldwide by 2030 (3). Despite the severity and prevalence of this disorder, currently available therapeutics may take weeks to exert an antidepressant effect, and only slightly more than one third of patients will remit after a first treatment (4). Furthermore, up to one third of patients with MDD will not enter remission even after treatment with four different antidepres- sants (4). In the search for more effective treatments, numerous studies have found that a single subanesthetic dose of the gluta- matergic modulator ketamine has rapid, robust, and relatively sustained antidepressant effects (5–9), even in patients with treatment-resistant MDD or bipolar depression (7–10). Neural correlates of the acute effects of ketamine administration have been investigated in several functional magnetic resonance imaging (fMRI) studies. These identified immediate, robust, and reliable changes in blood oxygen level–dependent resting state signal in healthy volunteers (11–15). However, few studies have investigated the potential sustained neural effects of ketamine beyond immediate infusion or correlated these changes with symptom improvement in MDD (16). Intrinsic brain connectivity differences between MDD and healthy control (HC) samples have been well studied with fMRI (17,18). In particular, the triple network model of dysfunction among the default mode network (DMN), salience network (SAL), and central executive network (CEN) has been proposed to explain depressive symptomology as well as other neuro- psychiatric disorders (19). With regard to MDD, this hypothesis posits that depressive symptoms result from increased activity in the DMN, a network responsible for introspection and rumination (20), in contrast to reduced activity in the SAL and CEN; the former mediates the processing of salient information from the external world, and the latter is responsible for working memory and attention (19). Only two studies have investigated fMRI changes 24 hours postketamine infusion in subjects with MDD. Murrough et al. found that reduced activation of the right caudate in response Published by Elsevier Inc on behalf of Society of Biological Psychiatry. 1 ISSN: 0006-3223 Biological Psychiatry --, 2018; -:-–- www.sobp.org/journal Biological Psychiatry Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax Hospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved.
Transcript of Default Mode Connectivity in Major Depressive Disorder...

iologicalsychiatry
Archival Report BP
Default Mode Connectivity in Major DepressiveDisorder Measured Up to 10 Days AfterKetamine Administration
Jennifer W. Evans, Joanna Szczepanik, Nancy Brutsché, Lawrence T. Park,Allison C. Nugent, and Carlos A. Zarate Jr.ISS
ABSTRACTBACKGROUND: The symptoms of major depressive disorder (MDD) are rapidly alleviated by administration of asingle dose of the glutamatergic modulator ketamine. However, few studies have investigated the potential sustainedneural effects of this agent beyond immediate infusion. This study used functional magnetic resonance imaging toexamine the effect of a single ketamine infusion on the resting state default mode network (DMN) at 2 and 10 daysafter a single ketamine infusion in unmedicated subjects with MDD as well as healthy control subjects (HCs).METHODS: Data were drawn from a double-blind, placebo-controlled crossover study of 58 participants (33 withMDD and 25 HCs) who received an intravenous infusion of either ketamine hydrochloride (0.5 mg/kg) or placeboon 2 separate test days spaced 2 weeks apart. Eight minutes of functional magnetic resonance imaging restingstate data was acquired at baseline and at about 2 and 10 days after both infusions. The DMN was defined usingseed-based correlation and was compared across groups and scans.RESULTS: In subjects with MDD, connectivity between the insula and the DMN was normalized compared with HCs2 days postketamine infusion. This change was reversed after 10 days and did not appear in either of the placeboscans. Group-specific connectivity differences in drug response were observed, most notably in the insula in subjectswith MDD and in the thalamus in HCs.CONCLUSIONS: Connectivity changes in the insula in subjects with MDD suggest that ketamine may normalize theinteraction between the DMN and salience networks, supporting the triple network dysfunction model of MDD.
Keywords: Default mode network, Functional magnetic resonance imaging (fMRI), Glutamatergic modulator, Ketamine,Major depressive disorder, Resting state
https://doi.org/10.1016/j.biopsych.2018.01.027
Major depressive disorder (MDD) is a common mental disorder(1,2) predicted to be the leading cause of disease burdenworldwide by 2030 (3). Despite the severity and prevalence ofthis disorder, currently available therapeutics may take weeksto exert an antidepressant effect, and only slightly more thanone third of patients will remit after a first treatment (4).Furthermore, up to one third of patients with MDD will not enterremission even after treatment with four different antidepres-sants (4).
In the search for more effective treatments, numerous studieshave found that a single subanesthetic dose of the gluta-matergic modulator ketamine has rapid, robust, and relativelysustained antidepressant effects (5–9), even in patients withtreatment-resistant MDD or bipolar depression (7–10). Neuralcorrelates of the acute effects of ketamine administration havebeen investigated in several functional magnetic resonanceimaging (fMRI) studies. These identified immediate, robust, andreliable changes in blood oxygen level–dependent resting statesignal in healthy volunteers (11–15). However, few studies have
PubN: 0006-3223
Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax HFor personal use only. No other uses without permissio
investigated the potential sustained neural effects of ketaminebeyond immediate infusion or correlated these changes withsymptom improvement in MDD (16).
Intrinsic brain connectivity differences between MDD andhealthy control (HC) samples have been well studied with fMRI(17,18). In particular, the triple network model of dysfunctionamong the default mode network (DMN), salience network(SAL), and central executive network (CEN) has been proposedto explain depressive symptomology as well as other neuro-psychiatric disorders (19). With regard to MDD, this hypothesisposits that depressive symptoms result from increased activityin the DMN, a network responsible for introspection andrumination (20), in contrast to reduced activity in the SAL andCEN; the former mediates the processing of salient informationfrom the external world, and the latter is responsible forworking memory and attention (19).
Only two studies have investigated fMRI changes 24 hourspostketamine infusion in subjects with MDD. Murrough et al.found that reduced activation of the right caudate in response
lished by Elsevier Inc on behalf of Society of Biological Psychiatry. 1Biological Psychiatry - -, 2018; -:-–- www.sobp.org/journal
ospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.n. Copyright ©2018. Elsevier Inc. All rights reserved.
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
to negatively valenced emotional stimuli in patients withtreatment-resistant MDD was normalized after ketamineadministration (21). They also found that resting state con-nectivity in the right caudate predicted treatment response,suggesting that the caudate was specifically affected by ke-tamine. In a resting state analysis, Abdallah et al. found that thedecreased global connectivity observed in their subjects withMDD at baseline was normalized to HC levels in ketamine re-sponders (22).
In addition, only two fMRI studies have examinedketamine-induced changes in HCs the day after ketamineadministration. One resting state study found that ketaminereduced connectivity of the dorsal nexus with the DMN andcognitive control network 1 day after blinded infusion (23).The other study found reduced neural reactivity in the bilat-eral amygdalo-hippocampal complex during emotionalstimulation with negative emotional faces (24). Takentogether, these studies suggest that ketamine decreasesbrain response in regions typically identified as hyperactivein depression (25).
The current study sought to investigate the neural correlatesof longer-term, sustained mood improvements within the first 10days after ketamine infusion in medication-free patients withtreatment-resistant MDD compared with a group of HCs. TheDMN was used to investigate differences in resting state fMRIafter ketamine infusion. Based on previous findings that ketaminenormalizes blood oxygen level–dependent activity in regionsaltered in depression (22,26), we hypothesized that the DMNdifferences between the subjects with MDD and HCs would bereduced after ketamine administration, particularly in regionsassociated with the SAL and CEN.
METHODS AND MATERIALS
Subjects
In total, 33 subjects with MDD and 25 HCs who had a restingstate fMRI scan as part of a larger study (NCT00088699, Na-tional Institutes of Health Protocol No. 04-M-0222, substudy 4)were included in this analysis. All subjects were between 18and 65 years old and were recruited between 2011 and 2016.Subject demographics are listed in Supplemental Table S1.Each subject provided written informed consent as approvedby the National Institutes of Health Combined Central NervousSystem Institutional Review Board.
Subjects with MDD were diagnosed with recurrent MDDwithout psychotic features and were experiencing a currentdepressive episode of at least moderate severity lasting atleast 4 weeks; severity was defined as a Montgomery–ÅsbergDepression Rating Scale (MADRS) (27) total score $ 20 atscreening and prior to each infusion. Patient diagnoses wereconfirmed using the Structured Clinical Interview for Axis IDSM-IV Disorders with psychiatric screen, patient version (28).Subjects with MDD were also required to be treatment resis-tant, defined as not having responded to at least one adequateantidepressant dose/duration trial as assessed using the An-tidepressant Treatment History Form (29). In addition, theywere required to be free of comorbid substance abuse ordependence for at least 3 months (except for nicotine orcaffeine) prior to inpatient admission, have a negative drug andalcohol urine toxicology screen and pregnancy test within 24
2 Biological Psychiatry - -, 2018; -:-–- www.sobp.org/journalDownloaded for Christopher Sendi ([email protected]) at Inova Fairfax Hos
For personal use only. No other uses without permission. C
hours prior to each MRI session, have no unstable medicalproblems, and be in good physical health as assessed bymedical history, physical examination, blood labs, urinalysis,and toxicology. Other exclusion criteria included concomitanttreatment with psychotropic medications during the 2 weeksbefore randomization (5 weeks for fluoxetine and 3 weeks foraripiprazole) and the presence of metallic (ferromagnetic)implants.
HCs were screened using the Structured Clinical Interviewfor Axis I DSM-IV Disorders, nonpatient version (30) and had nopersonal or family history (first-degree relative) of mood or AxisI disorder. All subjects were medically healthy as determinedby medical history, physical examination, blood labs, urinaly-sis, and toxicology.
Study Design
The double-blind, placebo-controlled crossover study design isillustrated in Figure 1, which also lists the scans and rating scalesobtained. All subjects received an intravenous infusion of eithersaline solution or 0.5 mg/kg of ketamine hydrochloride; 2 weekslater (to avoid carryover effects), subjects were blindly crossedover to the other arm of the study. Medical staff administering theinfusion, investigators, raters, and subjects all were blinded torandomization, which was performed by the National Institutes ofHealth Clinical Center pharmacy department. All subjectsparticipated in both arms of the study because depressivesymptoms returned for all subjects with MDD before the secondinfusion. Ketamine infusions were administered intravenouslyover 40 minutes via an infusion pump on an inpatient unit bymedical staff with advanced cardiac life support training.
All subjects with MDD were medication free for 2 weeksbefore randomization and throughout the entire study. Simi-larly, HCs were not permitted to take any medications withcentral nervous system effects throughout the study.
Rating Scales
The MADRS was used throughout the study to obtain moodratings. Ratings were obtained at 260 (baseline), 40, 80, 120,and 230 minutes postinfusion as well as on days 1, 2, 3, 7, 10,and 11. Average MADRS scores were estimated using a linearmixed effects model with baseline as a covariate using all timepoints. A separate model was used for each group.
fMRI Scanning
Resting state fMRI scans (duration of 8 minutes and resolutionof 3.753 3.753 3.5 mm) were acquired on a 3T scanner (HDX;General Electric Healthcare, Milwaukee, WI) along with ananatomical scan (1 mm isotropic resolution) using an eight-channel coil. The scans were conducted at baseline (b; inthis case, 2 or 3 days before the first infusion) and at days 2 or3 and 10 or 11 after placebo (p2 and p10, respectively) andketamine (k2 and k10, respectively) infusions, yielding anintended total of five scans per subject (b, p2, p10, k2, andk10). Subjects were instructed to close their eyes, relax, andnot fall asleep. Cardiac and respiration traces were alsorecorded using the manufacturer’s photoplethysmograph andrespiratory belt, respectively. Imaging acquisition parametersand details of the preprocessing methods can be found in theSupplement.
pital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.opyright ©2018. Elsevier Inc. All rights reserved.

Figure 1. Summary of the study’s double-blind,placebo-controlled crossover design showing themedication taper and drug-free period in relation tothe imaging scans (green circles), infusions (red tri-angles), and rating scales (blue rectangles) in boththe placebo and ketamine study arms. MRI, mag-netic resonance imaging.
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
Data Analysis
Across all analyses, data were processed using AFNI version17.3.05 (November 2016) (31). The DMN was defined using aseed-based correlation method (3dTcorr) where the averagetime course from a 6-mm-radius sphere placed at the posteriorcingulate cortex (3dROIstats) at the Montreal NeurologicalInstitute template coordinates of (0, 252, 27) (32) was corre-lated with all other brain voxels. The correlation values wereconverted to Z scores using Fisher transform.
Group analyses were performed with 3dLME (33) using alinear mixed effects model including both the MDD and HCgroups. Themodel had a fixed effect of scan type across all scandays (b, k2, k10, p2, and p10) and a random effect of subject (toaccount for the repeated scans). Between-group differenceswere included for each scan time point (b, k2, k10, p2, and p10).Post hoc contrasts were also calculated in order to examinedifferences between each postinfusion scan and baseline (k2-b,k10-b, p2-b, and p10-b) as well as the difference betweenpostketamine and postplacebo scans at days 2 and 10 (k2-p2and k10-p10). Familywise error multiple comparison correctionfor the group maps was performed by first estimating thesmoothness of the data after preprocessing (3dFWHMx). Cor-rected cluster size was calculated using 3dClustSim with thisvalue. Group maps were familywise error–corrected to p , .05with an initial threshold of p, .05 using a cluster size of. 120.
To specifically investigate the triple network model, a regionof interest (ROI) analysis was performed using the FIND ROI (34)set for the SAL (anterior and posterior) and CEN (left and right).Further details regarding the ROIs for these networks can befound in the Supplement and are also shown in SupplementalFigure S1. The average correlation values with the DMNwithin these ROIs was calculated per subject and averagedover the group. Statistics for these values were calculatedusing a linear mixed effects model in R (35) separately foreach group, with scan type as a fixed factor (five levels) andsubject as a random factor. Significance was established atp , .05.
RESULTS
Subject and Scan Characteristics
The MDD and HC groups did not differ significantly with regardto age (MDD: 36 6 10 years; HC: 33 6 10 years; t58 = 0.96, p =.34) or gender (MDD: 61% female; HC: 60% female; c2
1 = 0.05,p = .82). Supplemental Table S2 lists the number of scanscompleted at each time point as well as the final number
B
Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax HFor personal use only. No other uses without permissio
included in the analyses. Of the 236 total scans obtained, 36were excluded from the analysis; of these, 10 scans (6 MDDand 4 HC) were excluded due to incomplete physiologicaldata, 20 scans (9 MDD and 11 HC) were excluded for exces-sive motion, and 6 scans (3 MDD and 3 HC) were excluded dueto high correlation between the respiration volume trace andthe average global signal, which increased correlations acrossthe brain. No significant differences in motion between groupsor scan pairs were observed except for the p2 scan (averagemotion per timepoint of 0.03 mm for the MDD group and 0.04mm for the HC group [t44 = 23.17, p = .003]). No significantdifferences in respiration or heart rate were found betweengroups or scans (details appear in Supplemental Figure S2).
MADRS Changes
Within hours of ketamine infusion, subjects with MDD hadsignificantly improved MADRS scores, a change that was main-tained at the day 2 time point (mean difference of 9.4, p , .001)(see Figure 2). This change was significantly different (p , .001)from the placebo response for this group at day 2 and until thescan at day 10 (p , .02).
No significant differences in MADRS score were observedfor the HCs from baseline or placebo at either day 2 or day 10.These results are consistent with findings from a recentlypublished study of a larger cohort; details are available in (36).
DMN Between-Group Differences for EachScan Day
At baseline, the HCs had greater connectivity with the DMNthan the MDD group in the right dorsolateral prefrontalcortex (Brodmann areas [BA] 6 and 9) and left postcentralgyrus (insula to BA 43) (see Figure 3 and SupplementalTable S3 for cluster coordinate locations). Across all thescans (b, k2, p2, k10, and p10), the HCs had greater con-nectivity with the DMN than the MDD group in the rightprecentral gyrus (BA 44) as well as the left and right post-central gyrus (BA 40).
A smaller difference unique to the k2 scan was noted withregard to connectivity of the insula with the DMN between theMDD and HC groups. This normalization between the groupsreturned to baseline by day 10. The anterior cingulate cortex(ACC) (BA 24) showed increased connectivity in the HCscompared with subjects with MDD at k2 that was stillapparent at k10 but was not apparent at b or in the p2 scan.In the k10 scan, the right supramarginal gyrus (BAs 22 and39) showed increased connectivity in subjects with MDD that
iological Psychiatry - -, 2018; -:-–- www.sobp.org/journal 3ospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.
n. Copyright ©2018. Elsevier Inc. All rights reserved.
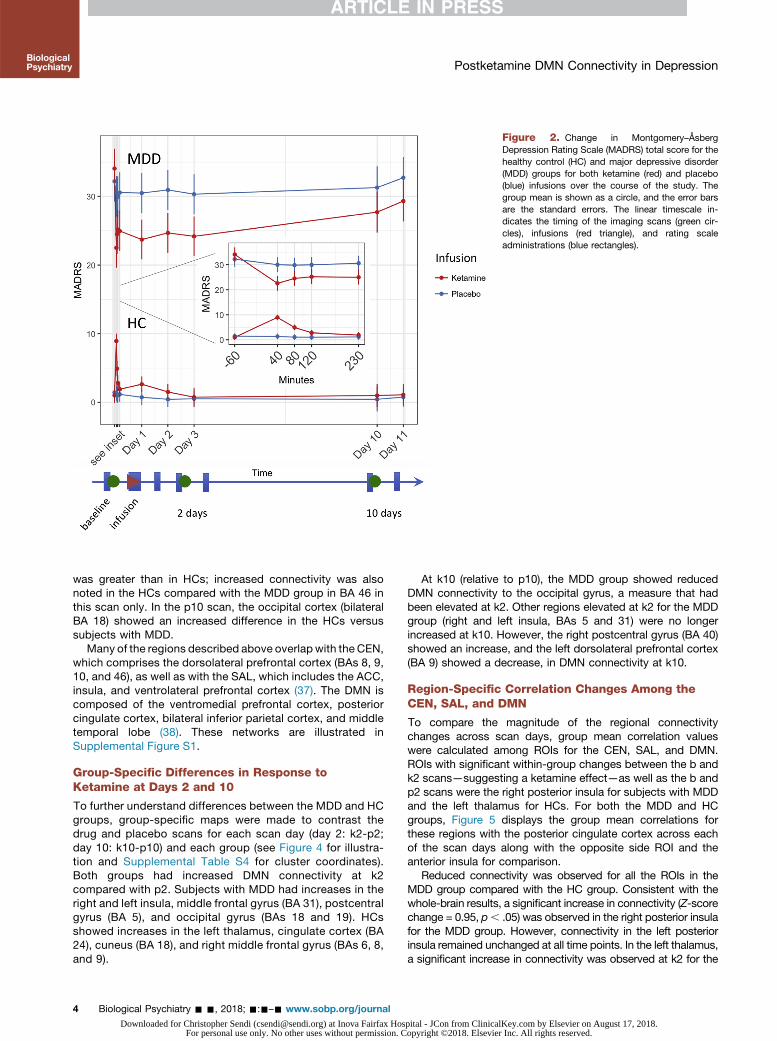
Figure 2. Change in Montgomery–ÅsbergDepression Rating Scale (MADRS) total score for thehealthy control (HC) and major depressive disorder(MDD) groups for both ketamine (red) and placebo(blue) infusions over the course of the study. Thegroup mean is shown as a circle, and the error barsare the standard errors. The linear timescale in-dicates the timing of the imaging scans (green cir-cles), infusions (red triangle), and rating scaleadministrations (blue rectangles).
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
was greater than in HCs; increased connectivity was alsonoted in the HCs compared with the MDD group in BA 46 inthis scan only. In the p10 scan, the occipital cortex (bilateralBA 18) showed an increased difference in the HCs versussubjects with MDD.
Many of the regions described above overlap with the CEN,which comprises the dorsolateral prefrontal cortex (BAs 8, 9,10, and 46), as well as with the SAL, which includes the ACC,insula, and ventrolateral prefrontal cortex (37). The DMN iscomposed of the ventromedial prefrontal cortex, posteriorcingulate cortex, bilateral inferior parietal cortex, and middletemporal lobe (38). These networks are illustrated inSupplemental Figure S1.
Group-Specific Differences in Response toKetamine at Days 2 and 10
To further understand differences between the MDD and HCgroups, group-specific maps were made to contrast thedrug and placebo scans for each scan day (day 2: k2-p2;day 10: k10-p10) and each group (see Figure 4 for illustra-tion and Supplemental Table S4 for cluster coordinates).Both groups had increased DMN connectivity at k2compared with p2. Subjects with MDD had increases in theright and left insula, middle frontal gyrus (BA 31), postcentralgyrus (BA 5), and occipital gyrus (BAs 18 and 19). HCsshowed increases in the left thalamus, cingulate cortex (BA24), cuneus (BA 18), and right middle frontal gyrus (BAs 6, 8,and 9).
4 Biological Psychiatry - -, 2018; -:-–- www.sobp.org/journalDownloaded for Christopher Sendi ([email protected]) at Inova Fairfax Hos
For personal use only. No other uses without permission. C
At k10 (relative to p10), the MDD group showed reducedDMN connectivity to the occipital gyrus, a measure that hadbeen elevated at k2. Other regions elevated at k2 for the MDDgroup (right and left insula, BAs 5 and 31) were no longerincreased at k10. However, the right postcentral gyrus (BA 40)showed an increase, and the left dorsolateral prefrontal cortex(BA 9) showed a decrease, in DMN connectivity at k10.
Region-Specific Correlation Changes Among theCEN, SAL, and DMN
To compare the magnitude of the regional connectivitychanges across scan days, group mean correlation valueswere calculated among ROIs for the CEN, SAL, and DMN.ROIs with significant within-group changes between the b andk2 scans—suggesting a ketamine effect—as well as the b andp2 scans were the right posterior insula for subjects with MDDand the left thalamus for HCs. For both the MDD and HCgroups, Figure 5 displays the group mean correlations forthese regions with the posterior cingulate cortex across eachof the scan days along with the opposite side ROI and theanterior insula for comparison.
Reduced connectivity was observed for all the ROIs in theMDD group compared with the HC group. Consistent with thewhole-brain results, a significant increase in connectivity (Z-scorechange = 0.95, p, .05) was observed in the right posterior insulafor the MDD group. However, connectivity in the left posteriorinsula remained unchanged at all time points. In the left thalamus,a significant increase in connectivity was observed at k2 for the
pital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.opyright ©2018. Elsevier Inc. All rights reserved.

Figure 3. Group (healthy control [HC] and majordepressive disorder [MDD]) differences in connec-tivity with the posterior cingulate cortex seed of thedefault mode network across scans at each scanday. The mean Z-score maps are shown at athreshold of p , .05 (familywise error corrected). Thered circles highlight regions of significant difference(second row: bilateral insula [salience network] andanterior cingulate cortex [central executive network];third row: right Brodmann area 22 and left Brodmannarea 46 [salience network]; fifth row: Brodmann area18). R, right.
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
HC group (change = 1.26, p = .05) that was not found at otherscan time points or for the MDD group.
DISCUSSION
This double-blind, placebo-controlled, crossover fMRI studyexamined the effects of a single ketamine infusion on DMNconnectivity in both subjects with MDD and HCs. We foundthat, compared with HCs, insular connectivity with the DMNwas normalized in subjects with MDD 2 days after a ketamineinfusion, particularly in the right hemisphere. This change wasreversed after 10 days and did not appear in either placeboscan. Furthermore, there were group-specific differences inregional connectivity with regard to drug response, notably forthe insula in subjects with MDD and for the thalamus in HCs.
Interestingly, connectivity regions were consistentlydifferent between the MDD and HC groups across the baselineand placebo scans, suggesting a reliable baseline differencebetween the groups. This is particularly important given theconsiderable overlap between previously described drug andplacebo responses (39–41), and it enabled the accuratedetermination of regions affected by ketamine. It should benoted, however, that several regions previously identified ashaving increased connectivity with the DMN in subjects withMDD (compared with HCs) did not achieve significance in thecurrent study, including the limbic regions (18,42). Onepossible explanation is that DMN connectivity in our treatment-resistant population differed from that in other depressedpopulations, possibly due to the existence of depressionsubtypes (43). One study that focused specifically on
B
Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax HFor personal use only. No other uses without permissio
differences between treatment-resistant (refractory) and non-refractory depression similarly found overall decreases inconnectivity between subjects with MDD and HCs (44). Thatstudy further identified the prefrontal areas (middle temporaland frontal gyri) regions as hypoactive in the treatment-resistant group compared with HCs, consistent with ourstudy. It should be noted that the definition of treatmentresistance may vary between research groups, which may alsocontribute to variance in reported results. However, the use ofsubtypes that can be defined from resting state data (43) mayhelp to improve reproducibility.
In the current study, normalization of the connectivity be-tween the insula and the DMN in subjects with MDD 2 dayspostketamine infusion was consistent with the improvement inglobal brain connectivity previously observed in patients withMDD 1 day postketamine infusion in this region (22). However,we also found that this region experienced a change in con-nectivity that corresponded to the response relapse seen in theMADRS scores. This finding is particularly important becausethe insula shares substantial anatomical and functional con-nections with regions that have been implicated in the neuro-logical differences observed in individuals with MDD (45). Theinsula is also implicated as a key node in the integration ofexternal emotional stimuli and has been shown to play a role ininterpreting emotional information and switching between theCEN and DMN (37). Thus, the postketamine increased con-nectivity between the insula and the DMN observed in thecurrent study suggests an improved ability to process externalstimuli that, in turn, may be linked to symptom improvement.Interestingly, the posterior insula, where we found the
iological Psychiatry - -, 2018; -:-–- www.sobp.org/journal 5ospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.
n. Copyright ©2018. Elsevier Inc. All rights reserved.

Figure 4. Group-specific differences for connec-tivity with the posterior cingulate cortex seed of thedefault mode network across scans for the majordepressive disorder (MDD) and healthy control (HC)groups. The mean Z-score maps illustrate thecontrast between ketamine and placebo scans at 2and 10 days postinfusion, respectively, and areshown at a threshold of p , .05 (familywise errorcorrected). The blue circles highlight regions of sig-nificant difference (first row: insula and Brodmannarea 18; third row: Brodmann areas 6 and 18). R,right.
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
strongest pattern of normalization in subjects with MDD, islinked to pain, sensorimotor processes, and language (46).This normalization may indicate relief of somatic depressivesymptoms linked to the abnormal interoception associatedwith the insula (47). Indeed, a post hoc correlation of con-nectivity between the right posterior insula and the DMN withthe MADRS values for the subjects with MDD supports theexistence of this positive association (see SupplementalFigure S4).
A notable degree of change was also observed in the oc-cipital cortex in the MDD group. Connectivity between the DMNand the occipital cortex was increased at day 2 postketaminecompared with baseline, but it was decreased at day 10,potentially indicating a rebound effect. Changes in the occipitalcortex have previously been associated with antidepressant use(48), and middle occipital activity has been shown to correlatewith subsequent antidepressant response (49).
Our analysis also found regions of increased connectivity inthe precentral and postcentral gyri of the MDD group. Otherstudies have noted that gray matter is reduced in these regionsin subjects with MDD compared with HCs (50); thus, our re-sults may reflect a ketamine-modulated increase in neuralplasticity. Overall, many of the regions showing increasedconnectivity with the DMN posterior cingulate cortex seed insubjects with MDD postketamine overlapped with nodes in theCEN and SAL. This is consistent with the triple network modelof dysfunction, which posits that DMN connectivity with theCEN and SAL is disturbed in MDD and further suggests thatketamine may normalize the interaction of these networks withthe DMN following symptom improvement. Although our dis-cussion is currently limited to the regions used in our ROIanalysis, future work using complex functional network
6 Biological Psychiatry - -, 2018; -:-–- www.sobp.org/journalDownloaded for Christopher Sendi ([email protected]) at Inova Fairfax Hos
For personal use only. No other uses without permission. C
analysis techniques (51) may provide more insight into theinterplay between these networks.
In the HCs, the general increase of connectivity observed2 days postinfusion is potentially inconsistent with the onlystudy (23) that has explored response to ketamine at 1 daypostinfusion in HCs. That study found reduced functional con-nectivity of the pregenual ACC and medial prefrontal cortex withthe DMN. Nevertheless, it is possible that the increase observed2 days postinfusion may reflect a renormalization effect occur-ring after the decrease seen at day 1 by Scheidegger et al. (23).
Finally, the current study also found increased connectivityin the thalamus, occipital cortex, and prefrontal cortex;changes in these areas are consistent with other studies thatexamined changes during and immediately after ketamineinfusion (52,53). The increases we observed in the ACC andvisual cortex may be attributable to changes in the balance ofthe SAL and CEN. It is interesting, however, that any con-nectivity differences were found at 2 days postinfusion in HCsgiven that ketamine is quickly metabolized and that HCsshowed no lasting behavioral effects beyond a few hours.
The study is associated with several limitations. First, weused an initial threshold of p , .05 in order to enable investi-gation of regional differences between the groups and condi-tions in this study; however, increasing the initial thresholdwould have considerably decreased the number of significantregions identified (see Supplemental Figure S3). In addition,using a strict initial threshold of p , .001, as recommended bysome in the literature (54), would leave very few regions ofsignificance. Thus, we chose a more lenient threshold in orderto give a balanced report. This sensitivity to initial threshold ispartly due to the relatively modest MDD and HC sample sizescompared with the heterogeneity of the population and drug
pital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.opyright ©2018. Elsevier Inc. All rights reserved.

Figure 5. Mean connectivity for regions of interest with significant differences across scans for both healthy control (HC; red) and major depressive disorder(MDD; blue) groups for the bilateral anterior (first row), posterior insula (second row), and thalamus (third row). Error bars represent standard deviations.
Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
response. Second, because this was a longitudinal study withrepeated scans, we inevitably had a reduced number of sub-jects completing all scans, leading to missing data in theanalysis; we controlled for this problem by using a linear mixedeffects model that is specifically designed to handle this issue(33). Third, the baseline for a resting state study is not welldefined, nor are the potential neural effects of expectancy,both of which are confounding factors. To address this, weincluded both a baseline scan and a placebo scan—eachadministered at two time points—to control for variations inthe resting state data that would be unrelated to ketamineresponse in terms of both drug anticipation and physiologicalor natural neural fluctuation. We further tried to mitigate con-founding factors by measuring and directly regressing physi-ological noise, and the results presented here should be
B
Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax HFor personal use only. No other uses without permissio
considered in this context. Lastly, we did not include ratingscale as a covariate in this analysis because the depressionrating scales used here did not have sufficient dynamic rangeto capture mood changes in the HC cohort at the scan timepoint of day 2. Thus, our MDD results may be strengthened byusing a behavioral response measure that captures inter-subject variability at that time or by investigating scans atearlier times, which is an area of future interest.
Taken together, the results of this study demonstrate that itis possible to characterize the neural correlates associatedwith the onset and offset of ketamine’s antidepressant effects.While subjects with MDD and HCs responded differently toketamine, response was generally characterized by increasedconnectivity with the DMN at 2 days postinfusion, an increasethat had dissipated by day 10. Furthermore, the connectivity
iological Psychiatry - -, 2018; -:-–- www.sobp.org/journal 7ospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.
n. Copyright ©2018. Elsevier Inc. All rights reserved.

Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
changes observed in the insula in subjects with MDD imply anormalization of the interaction between the DMN and SAL,supporting the triple network dysfunction theory in MDD. In thecontext of real-world ketamine use and the increased interestin using repeat doses of this agent to maintain antidepressantresponse, these findings could help to identify the window ofplasticity and plan the optimal time for subsequent doses. Theresults also suggest an avenue whereby neural response topharmaceutical drug interventions can be monitored and in-dividual dose regimens can be optimized.
ACKNOWLEDGMENTS AND DISCLOSURESFunding for this work was provided by the Intramural Research Program atthe National Institute of Mental Health (NIMH), National Institutes of Health(NIH) Grant Nos. IRP-NIMH-NIH and ZIA-MH002857 (to CAZ), by a NARSADIndependent Investigator Grant (to CAZ), and by a Brain & Behavior MoodDisorders Research Award (to CAZ). This work used the computational re-sources of the NIH High-Performance Computing Biowulf cluster (http://hpc.nih.gov).
We thank the 7SE research unit and staff for their support and ElizabethBallard for helpful comments on the manuscript. Ioline Henter (NIMH) pro-vided invaluable editorial assistance.
CAZ is listed as a coinventor on a patent for the use of ketamine in majordepression and suicidal ideation; as a coinventor on a patent for the use of(2R,6R)-hydroxynorketamine, (S)-dehydronorketamine, and other stereo-isomeric dehydro and hydroxylated metabolites of (R,S)-ketamine metabo-lites in the treatment of depression and neuropathic pain; and as acoinventor on a patent application for the use of (2R,6R)-hydroxynorket-amine and (2S,6S)-hydroxynorketamine in the treatment of depression,anxiety, anhedonia, suicidal ideation, and posttraumatic stress disorder. Hehas assigned his patent rights to the U.S. government but will share apercentage of any royalties that may be received by the government. Theother authors report no biomedical financial interests or potential conflicts ofinterest.
ClinicalTrials.gov: Rapid Antidepressant Effects of Ketamine in MajorDepression; https://clinicaltrials.gov/ct2/show/NCT00088699; NCT00088699.
ARTICLE INFORMATIONFrom the Experimental Therapeutics and Pathophysiology Branch, NationalInstitute of Mental Health, National Institutes of Health, Bethesda, Maryland.
Address correspondence to Jennifer W. Evans, Ph.D., ExperimentalTherapeutics and Pathophysiology Branch, National Institute of MentalHealth, National Institutes of Health, 10 Center Drive, Bldg. 10, Room 7-5331,Bethesda, MD 20814; E-mail: [email protected].
Received Nov 3, 2017; revised Jan 5, 2018; accepted Jan 23, 2018.Supplementary material cited in this article is available online at https://
doi.org/10.1016/j.biopsych.2018.01.027.
REFERENCES1. Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR,
et al. (2003): The epidemiology of major depressive disorder. JAMA289:3095–3105.
2. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE(2005): Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication. Arch GenPsychiatry 62:593–602.
3. World Health Organization (2012): Global burden of mental disordersand the need for a comprehensive, coordinated response from healthand social sectors at the country level: Report by the Secretariat.Available at: http://apps.who.int/gb/ebwha/pdf_files/WHA65/A65_10-en.pdf.
4. Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW,Warden D, et al. (2006): Acute and longer-term outcomes in depressedoutpatients requiring one or several treatment steps: A STAR*D report.Am J Psychiatry 163:1905–1917.
8 Biological Psychiatry - -, 2018; -:-–- www.sobp.org/journalDownloaded for Christopher Sendi ([email protected]) at Inova Fairfax Hos
For personal use only. No other uses without permission. C
5. Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR,Charney DS, Krystal JH (2000): Antidepressant effects of ketamine indepressed patients. Biol Psychiatry 47:351–354.
6. Li L, Vlisides PE (2016): Ketamine: 50 years of modulating the mind.Front Hum Neurosci 10:612.
7. Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R,Luckenbaugh DA, et al. (2006): A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. ArchGen Psychiatry 63:856–864.
8. Zarate CA, Brutsche NE, Ibrahim L, Franco-Chaves J, Diazgranados N,Cravchik A, et al. (2012): Replication of ketamine’s antidepressantefficacy in bipolar depression: A randomized controlled add-on trial.Biol Psychiatry 71:939–946.
9. Ibrahim L, Diazgranados N, Franco-Chaves J, Brutsche N, Henter ID,Kronstein P, et al. (2012): Course of improvement in depressivesymptoms to a single intravenous infusion of ketamine vs add-onriluzole: Results from a 4-week, double-blind, placebo-controlledstudy. Neuropsychopharmacology 37:1526–1533.
10. Murrough JW, Iosifescu DV, Chang LC, Al Jurdi RK, Green CE,Perez AM, et al. (2013): Antidepressant efficacy of ketamine intreatment-resistant major depression: A two-site randomizedcontrolled trial. Am J Psychiatry 170:1134–1142.
11. Doyle OM, De Simoni S, Schwarz AJ, Brittain C, O’Daly OG,Williams SCR, Mehta MA (2013): Quantifying the attenuation of theketamine pharmacological magnetic resonance imaging response inhumans: A validation using antipsychotic and glutamatergic agents.J Pharmacol Exp Ther 345:151–160.
12. De Simoni S, Schwarz AJ, O’Daly OG, Marquand AF, Brittain C,Gonzales C, et al. (2013): Test–retest reliability of the BOLD pharma-cological MRI response to ketamine in healthy volunteers. NeuroImage64:75–90.
13. Shcherbinin S, Doyle O, Zelaya FO, de Simoni S, Mehta MA,Schwarz AJ (2015): Modulatory effects of ketamine, risperidone andlamotrigine on resting brain perfusion in healthy human subjects.Psychopharmacology (Berl) 232:4191–4204.
14. Deakin JFW, Lees J, McKie S, Hallak JEC, Williams SR, Dursun SM,et al. (2008): Glutamate and the neural basis of the subjective effects ofketamine. Arch Gen Psychiatry 65:154–164.
15. Driesen NR, McCarthy G, Bhagwagar Z, Bloch M, Calhoun V,D’Souza DC, et al. (2013): Relationship of resting brain hyper-connectivity and schizophrenia-like symptoms produced by theNMDA receptor antagonist ketamine in humans. Mol Psychiatry18:1199–1204.
16. Li M, Walter M (2016): The acute and chronic effects of ketamine asrevealed by noninvasive brain imaging. In: Preedy V, editor. Neuro-pathology of Drug Addictions and Substance Misuse. San Diego:Elsevier, 689–702.
17. Greicius MD, Flores BH, Menon V, Glover GH, Solvason HB, Kenna H,et al. (2007): Resting-state functional connectivity in major depression:Abnormally increased contributions from subgenual cingulate cortexand thalamus. Biol Psychiatry 62:429–437.
18. Kaiser RH, Andrews-Hanna JR, Wager TD, Pizzagalli DA (2015): Large-scale network dysfunction in major depressive disorder: A meta-analysis of resting-state functional connectivity. JAMA Psychiatry72:603–611.
19. Menon V (2011): Large-scale brain networks and psychopathol-ogy: A unifying triple network model. Trends Cogn Sci 15:483–506.
20. Hamilton JP, Farmer M, Fogelman P, Gotlib IH (2015): Depressiverumination, the default-mode network, and the dark matter of clinicalneuroscience. Biol Psychiatry 78:224–230.
21. Murrough JW, Collins KA, Fields J, DeWilde KE, Phillips ML,Mathew SJ, et al. (2015): Regulation of neural responses to emotionperception by ketamine in individuals with treatment-resistant majordepressive disorder. Transl Psychiatry 5:e509.
22. Abdallah CG, Averill LA, Collins KA, Geha P, Schwartz J, Averill C,et al. (2017): Ketamine treatment and global brain connectivity in majordepression. Neuropsychopharmacology 42:1210–1219.
23. Scheidegger M, Walter M, Lehmann M, Metzger C, Grimm S,Boeker H, et al. (2012): Ketamine decreases resting state functional
pital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.opyright ©2018. Elsevier Inc. All rights reserved.

Postketamine DMN Connectivity in DepressionBiologicalPsychiatry
network connectivity in healthy subjects: Implications for antidepres-sant drug action. PLoS One 7:e44799.
24. Scheidegger M, Henning A, Walter M, Lehmann M, Kraehenmann R,Boeker H, et al. (2016): Ketamine administration reduces amygdalo-hippocampal reactivity to emotional stimulation. Hum Brain Mapp37:1941–1952.
25. Sheline YI, Price JL, Yan Z, Mintun MA (2010): Resting-state functionalMRI in depression unmasks increased connectivity between networksvia the dorsal nexus. Proc Natl Acad Sci U S A 107:11020–11025.
26. Murrough JW, Wan L Ben, Iacoviello B, Collins KA, Solon C,Glicksberg B, et al. (2014): Neurocognitive effects of ketamine intreatment-resistant major depression: Association with antidepressantresponse. Psychopharmacology (Berl) 231:481–488.
27. Montgomery SA, Åsberg M, Asberg M (1979): A new depression scaledesigned to be sensitive to change. Br J Psychiatry 134:382–389.
28. First MB, Spitzer RL, Gibbon MWJ (2002): Structured Clinical Interviewfor DSM-IV-TR Axis I Disorders, Research Version, Patient Edition,With Psychotic Screen (SCID-I/P W/ PSY SCREEN). New York: Bio-metrics Research, New York State Psychiatric Institute.
29. Sackeim HA (2001): The definition and meaning of treatment-resistantdepression. J Clin Psychiatry 62(suppl 1):10–17.
30. First MB, Spitzer RL, Gibbon M, Williams JB (2002): Structured ClinicalInterview for DSM-IV-TR Axis I Disorders, Research Version, Non-patient Edition (SCID-I/NP). New York: Biometrics Research, NewYork State Psychiatric Institute.
31. Cox R (1996): AFNI: Software for analysis and visualization of func-tional magnetic resonance neuroimages. Comput Biomed Res29:162–173.
32. Raichle ME (2011): The restless brain. Brain Connect 1:3–12.33. ChenG,SaadZS,Britton JC,PineDS,CoxRW (2013): Linearmixed-effects
modeling approach to FMRI group analysis. NeuroImage 73:176–190.34. Shirer WR, Ryali S, Rykhlevskaia E, Menon V, Greicius MD (2012):
Decoding subject-driven cognitive states with whole-brain connec-tivity patterns. Cereb Cortex 22:158–165.
35. R Core Team (2013): R: A Language and Environment for StatisticalComputing. Vienna, Austria: R Foundation for Statistical Computing.Available at: http://www.r-project.org.
36. Nugent A, Ballard E, Gould TD, Park LT, Moaddel R, Brutsche N, et al.(2018): Ketamine has distinct electrophysiological and behaviouraleffects in depressed and healthy subjects [published online ahead ofprint Feb 27]. Mol Psychiatry.
37. Sridharan D, Levitin DJ, Menon V (2008): A critical role for the rightfronto-insular cortex in switching between central-executive anddefault-mode networks. Proc Natl Acad Sci U S A 105:12569–12574.
38. Buckner RL, Andrews-Hanna JR, Schacter DL (2008): The brain’sdefault network: Anatomy, function, and relevance to disease. Ann N YAcad Sci 1124:1–38.
39. Benedetti F, Mayberg HS, Wager TD, Stohler CS, Zubieta J-K (2005):Neurobiological mechanisms of the placebo effect. J Neurosci25:10390–10402.
B
Downloaded for Christopher Sendi ([email protected]) at Inova Fairfax HFor personal use only. No other uses without permissio
40. Walsh BT, Seidman SN, Sysko R, Gould M (2002): Placebo responsein studies of major depression: Variable, substantial, and growing.JAMA 287:1840–1847.
41. Mayberg HS, Silva JA, Brannan SK, Tekell JL, Mahurin RK,McGinnis S, Jerabek PA (2002): The functional neuroanatomy of theplacebo effect. Am J Psychiatry 159:728–737.
42. Hamilton JP, Furman DJ, Chang C, Thomason ME, Dennis E, Gotlib IH(2011): Default-mode and task-positive network activity in majordepressive disorder: Implications for adaptive and maladaptive rumi-nation. Biol Psychiatry 70:327–333.
43. Drysdale AT, Grosenick L, Downar J, Dunlop K, Mansouri F, Meng Y,et al. (2017): Resting-state connectivity biomarkers define neuro-physiological subtypes of depression. Nat Med 23:28–38.
44. Lui S, Wu Q, Qiu L, Yang X, Kuang W, Chan RCK, et al. (2011):Resting-state functional connectivity in treatment-resistant depres-sion. Am J Psychiatry 168:642–648.
45. Sliz D, Hayley S (2012): Major depressive disorder and alterations ininsular cortical activity: A review of current functional magnetic im-aging research. Front Hum Neurosci 6:323.
46. Chang LJ, Yarkoni T, Khaw MW, Sanfey AG (2013): Decoding the roleof the insula in human cognition: Functional parcellation and large-scale reverse inference. Cereb Cortex 23:739–749.
47. Avery JA, Drevets WC, Moseman SE, Bodurka J, Barcalow JC,Simmons WK (2014): Major depressive disorder is associated withabnormal interoceptive activity and functional connectivity in theinsula. Biol Psychiatry 76:258–266.
48. Sanacora G, Mason GF, Rothman DL, Krystal JH (2002): Increasedoccipital cortex GABA concentrations in depressed patients aftertherapy with selective serotonin reuptake inhibitors. Am J Psychiatry159:663–665.
49. Furey ML, Drevets WC, Hoffman EM, Frankel E, Speer AM,Zarate CA Jr (2013): Potential of pretreatment neural activity in thevisual cortex during emotional processing to predict treatmentresponse to scopolamine in major depressive disorder. JAMA Psy-chiatry 70:280–290.
50. Grieve SM, Korgaonkar MS, Koslow SH, Gordon E, Williams LM(2013): Widespread reductions in gray matter volume in depression.NeuroImage Clin 3:332–339.
51. Rubinov M, Sporns O (2010): Complex network measures of brainconnectivity: Uses and interpretations. NeuroImage 52:1059–1069.
52. Höflich A, Hahn A, Küblböck M, Kranz GS, Vanicek T, Ganger S, et al.(2017): Ketamine-dependent neuronal activation in healthy volunteers.Brain Struct Funct 222:1533–1542.
53. Höflich A, Hahn A, Küblböck M, Kranz GS, Vanicek T,Windischberger C, et al. (2015): Ketamine-induced modulation of thethalamo-cortical network in healthy volunteers as a model forschizophrenia. Int J Neuropsychopharmacol 18:1–11.
54. Woo C-W, Krishnan A, Wager TD (2014): Cluster-extent basedthresholding in fMRI analyses: Pitfalls and recommendations. Neuro-Image 91:412–419.
iological Psychiatry - -, 2018; -:-–- www.sobp.org/journal 9ospital - JCon from ClinicalKey.com by Elsevier on August 17, 2018.
n. Copyright ©2018. Elsevier Inc. All rights reserved.


















