Dear Customer Estimado(a) Cliente L OTHER PROGRAMS AND ... · 6 $69,180 7 $78,020 8 $86,860 What is...
2
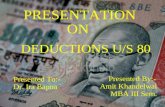
Estimado(a) Cliente A través del programa Tarifas Alternas Para Energía de California (CARE), SoCalGas ® ofrece un 20 por ciento de descuento en la factura mensual de gas natural a los clientes que reúnan los requisitos. El descuento será aplicado en la factura mensual de gas natural, siguiente a la fecha en que su aplicación es aprobada por SoCalGas. Llene el formulario de solicitud y envíenoslo, o visite socalgas.com/careparami para presentar su solicitud. Dear Customer Through the California Alternate Rates for Energy (CARE) program, SoCalGas ® offers eligible customers a 20 percent discount on their monthly natural gas bill. The discount will be applied to the monthly natural gas bill following the date that the application is approved by SoCalGas. Please complete the enclosed application and return, or visit socalgas.com/care to apply online. 1-800-427-1429 1-800-427-1420 1-800-427-0478 1-800-427-0471 ATTN: CARE PROGRAM ML GT19A1 SOCALGAS PO BOX 515005 LOS ANGELES CA 90099-5404 NO POSTAGE NECESSARY IF MAILED IN THE UNITED STATES BUSINESS REPLY MAIL FIRST-CLASS MAIL LOS ANGELES CA 90051 PERMIT NO. 11564 POSTAGE WILL BE PAID BY ADDRESSEE APPLY FOR A 20% DISCOUNT APLIQUE PARA UN DESCUENTO DEL 20% © 2019 Southern California Gas Company. These programs are funded by California utility customers and administered by Southern California Gas Company under the auspices of the California Public Utilities Commission. Trademarks are property of their respective owners. All rights reserved. N19E0128A 0919 21-1911 For information on CARE, call SoCalGas at 1-800-427-2200 Para información en Español: 1-800-342-4545 MEDICAL BASELINE ALLOWANCE Get additional natural gas at the lowest baseline rate if you have a serious health condition ASIGNACIÓN MÉDICA INICIAL Reciba gas natural adicional, a la tarifa inicial más baja si tiene una condición médica seria socalgas.com/medical 1-866-431-3517 socalgas.com/medical 1-866-431-3517 HELP FOR MEDICAL NEEDS CALIFORNIA LIFELINE Discounted telephone services for eligible customers For more information, contact your telephone service provider CALIFORNIA LIFELINE Ofrece servicio telefónico a precios de descuento para los clientes Para más información, llame al proveedor de servicio telefónico de su localidad LOW INCOME HOME ENERGY ASSISTANCE Bill payment assistance, emergency bill assistance and weatherization services ASISTENCIA DE ENERGÍA PARA HOGARES DE BAJOS INGRESOS Asistencia de pago de facturas, asistencia de facturas de emergencia y servicios de climatización 1-866-675-6623 HELP WITH YOUR BILL ENERGY SAVINGS ASSISTANCE PROGRAM Offers no-cost, energy-saving home improvements socalgas.com/improvements 1-800-331-7593 ENERGY SAVINGS ASSISTANCE PROGRAM Ofrece mejoras para el hogar sin costo que ahorran energía socalgas.com/mejoras 1-800-331-7593 HELP FOR YOUR HOME HELP WITH YOUR PHONE AYUDA CON NECESIDADES MÉDICAS AYUDA CON LA FACTURA AYUDA PARA EL HOGAR AYUDA CON LA TELÉFONO 1-866-675-6623 OTHER PROGRAMS AND SERVICES YOU MAY QUALIFY FOR OTROS PROGRAMAS Y SERVICIOS PARA LOS QUE PODRÍA CALIFICAR CALIFORNIA ALTERNATE RATES FOR ENERGY (CARE) DID YOU KNOW... You can apply for CARE online and get approved instantly Visit socalgas.com/care for details « «
Transcript of Dear Customer Estimado(a) Cliente L OTHER PROGRAMS AND ... · 6 $69,180 7 $78,020 8 $86,860 What is...

Estimado(a) ClienteA través del programa Tarifas Alternas Para Energía de California (CARE), SoCalGas® ofrece un 20 por ciento de descuento en la factura mensual de gas natural a los clientes que reúnan los requisitos. El descuento será aplicado en la factura mensual de gas natural, siguiente a la fecha en que su aplicación es aprobada por SoCalGas.
Llene el formulario de solicitud y envíenoslo, o visite socalgas.com/careparami para presentar su solicitud.
Dear CustomerThrough the California Alternate Rates for Energy (CARE) program, SoCalGas® offers eligible customers a 20 percent discount on their monthly natural gas bill. The discount will be applied to the monthly natural gas bill following the date that the application is approved by SoCalGas.
Please complete the enclosed application and return, or visit socalgas.com/care to apply online.
1-800-427-1429
1-800-427-1420
1-800-427-0478
1-800-427-0471
1-800-427-1429
1-800-427-1420
1-800-427-0478
1-800-427-0471
ATT
N: C
AR
E P
RO
GR
AM
ML
GT1
9A1
SO
CA
LGA
S
PO
BO
X 5
1500
5 LO
S A
NG
ELE
S C
A 9
0099
-540
4
NO
PO
STAG
EN
ECES
SAR
YIF
MAI
LED
IN T
HE
UN
ITED
STA
TES
BUSI
NES
S R
EPLY
MAI
LFI
RST
-CLA
SS M
AIL
LOS
ANG
ELES
CA
9005
1PE
RM
IT N
O. 1
1564
POST
AGE
WIL
L BE
PAI
D B
Y AD
DR
ESSE
E
Artw
ork
for
Use
r Def
ined
(3.6
25" x
7")
Layo
ut: 1
-BR
M-3
.625
x7-IM
b.LY
TAp
ril 1
0, 2
015
Prod
uced
by
DAZ
zle,
Ver
sion
12.
2.02
(c) 1
993-
2012
, DYM
O E
ndic
ia, w
ww.
Endi
cia.
com
Auth
oriz
ed U
ser,
Seria
l #
IMPO
RTA
NT:
DO
NO
T EN
LAR
GE,
RED
UC
E O
R M
OVE
the
FIM
and
bar
code
s. T
hey
are
only
valid
as
prin
ted!
Spe
cial
car
e m
ust b
e ta
ken
to e
nsur
e FI
M a
nd b
arco
de a
re a
ctua
l siz
e AN
D p
lace
d pr
oper
ly on
the
mai
l pie
ce t
o m
eet b
oth
USP
S re
gula
tions
and
aut
omat
ion
com
patib
ility
stan
dard
s.
APPLY FOR A 20% DISCOUNT
APLIQUE PARA UN DESCUENTO DEL 20%
© 2019 Southern California Gas Company. These programs are funded by California utility customers and administered by Southern California Gas Company under the auspices of the California Public Utilities Commission. Trademarks are property of their respective owners. All rights reserved. N19E0128A 0919 21-1911
For information on CARE, call SoCalGas at 1-800-427-2200Para información en Español: 1-800-342-4545
MEDICAL BASELINE ALLOWANCE Get additional natural gas at the lowest baseline rate if you have a serious health condition
ASIGNACIÓN MÉDICA INICIAL Reciba gas natural adicional, a la tarifa inicial más baja si tiene una condición médica seria
socalgas.com/medical 1-866-431-3517 socalgas.com/medical 1-866-431-3517
HELP FOR MEDICAL NEEDS
CALIFORNIA LIFELINE Discounted telephone services for eligible customersFor more information, contact your telephone service provider
CALIFORNIA LIFELINEOfrece servicio telefónico a precios de descuento para los clientesPara más información, llame al proveedor de servicio telefónico de su localidad
LOW INCOME HOME ENERGY ASSISTANCE Bill payment assistance, emergency bill assistance and weatherization services
ASISTENCIA DE ENERGÍA PARA HOGARES DE BAJOS INGRESOSAsistencia de pago de facturas, asistencia de facturas de emergencia y servicios de climatización
1-866-675-6623
HELP WITH YOUR BILL
ENERGY SAVINGS ASSISTANCE PROGRAM Offers no-cost, energy-saving home improvements
socalgas.com/improvements 1-800-331-7593
ENERGY SAVINGS ASSISTANCE PROGRAM Ofrece mejoras para el hogar sin costo que ahorran energíasocalgas.com/mejoras 1-800-331-7593
HELP FOR YOUR HOME
HELP WITH YOUR PHONE
AYUDA CON NECESIDADES MÉDICAS
AYUDA CON LA FACTURA
AYUDA PARA EL HOGAR
AYUDA CON LA TELÉFONO
1-866-675-6623
OTHER PROGRAMS AND SERVICES YOU MAY QUALIFY FOR
OTROS PROGRAMAS Y SERVICIOS PARA LOS QUE PODRÍA CALIFICAR
CALIFORNIA ALTERNATE RATES FOR ENERGY (CARE)
DID
YO
U K
NO
W...
You can apply for CARE online and get approved instantly
Visit socalgas.com/carefor details«
«

AP
PLY
ON
LIN
E
socalgas.com/care
AP
LIQ
UE
EN
LÍN
EA
socalgas.com/careparam
i
QU
AL
IFIC
AT
ION
S F
OR
TH
E C
AR
E P
RO
GR
AM
CA
LIF
ICA
CIO
NE
S P
AR
A E
L P
RO
GR
AM
A C
AR
E
FO
RM
9E
No
Tap
e/N
o u
se cinta ad
hesiva
M
oiste
n an
d S
eal/H
um
edezca y selle
N
o S
taple
s/No
eng
rape
HO
W T
O Q
UA
LIF
Y / C
ÓM
O P
UE
DE
CA
LIF
ICA
RP
UB
LIC
AS
SIS
TA
NC
E P
RO
GR
AM
SP
RO
GR
AM
AS
DE
AS
IST
EN
CIA
PÚ
BL
ICA
If you
or an
oth
er p
erso
n in
you
r ho
use
ho
ld re
ceives b
en
efits fro
m any
of th
e fo
llowin
g p
rog
rams:
Si u
sted
u o
tra pe
rson
a qu
e vive
en
su h
og
ar recib
e b
en
eficios
de
cualq
uie
ra de
los sig
uie
ntes p
rog
ramas:
Me
di-C
al/Me
dicaid
Me
di-C
al for F
amilie
s A&
B
Wo
me
n, In
fants &
Ch
ildre
n (W
IC)
CalW
OR
Ks (T
AN
F)
1 or / o
Trib
al TA
NF
He
ad S
tart Inco
me
Elig
ible
— T
ribal O
nly
/ So
lame
nte
tribal
Bu
reau
of In
dian
Affairs G
en
eral A
ssistance
CalF
resh
(Fo
od
Stam
ps / E
stamp
illas para co
mid
a)
Natio
nal S
cho
ol L
un
ch P
rog
ram (N
SL
P)
Lo
w In
com
e H
om
e E
ne
rgy
Assistan
ce P
rog
ram (L
IHE
AP
)
Su
pp
lem
en
tal Se
curity
Inco
me
MA
XIM
UM
HO
US
EH
OL
D IN
CO
ME
IN
GR
ES
O M
ÁX
IMO
EN
EL
HO
GA
R
(effective
Ju
ne
1, 20
19 to
May
31, 2
02
0)
(en
vigo
r de
l 1 de
jun
io d
e 2
019
al 31 d
e m
ayo d
e 2
02
0)
N
umber of P
ersons in Household
Total Annual Incom
e*
Nú
me
ro d
e P
erso
nas e
n e
l Ho
gar
Ing
reso To
tal An
ual *
1–2
$
33
,82
0
3
$
42
,66
0
4
$
51,5
00
5
$6
0,3
40
6
$6
9,18
0
7
$
78
,02
0
8
$
86
,86
0
For each
add
ition
al ho
use
ho
ld m
em
be
r, add
$8
,84
0P
or cad
a mie
mb
ro ad
icion
al en
el h
og
ar, añad
a $8
,84
0*In
clud
es curre
nt h
ou
seh
old
inco
me
from
all sou
rces befo
re d
ed
uctio
ns
*Inclu
ye lo
s ing
resos actu
ales de
l ho
gar d
e to
das las fu
en
tes d
e in
greso
antes d
e d
ed
uccio
nes
O
R/O
1 Inclu
des W
elfare-to-W
ork
CO
ND
ITIO
NS
FO
R P
AR
TIC
IPA
TIO
N1) You m
ust meet the qualification requirem
ents in the table above. 2) The natural
gas bill must be in your nam
e and the address must be your prim
ary address. 3) You
m
ust not be claimed as a dependent on another person’s incom
e tax return
other
than
you
r spou
se. 4) Yo
u m
ust recertify yo
ur applicatio
n w
hen
requested. 5
) You
m
ust n
otify So
CalG
as with
in 30
days if you
no
lon
ger qualify. 6
) You
may be
asked to verify yo
ur eligibility fo
r CA
RE
.
CO
ND
ICIO
NE
S P
AR
A P
AR
TIC
IPA
R1) D
ebe cumplir los requisitos de elegibilidad que se m
uestran en la tabla anterior. 2
) La factu
ra de gas natu
ral debe estar a su n
om
bre y la dirección
debe ser su
dom
icilio principal 3
) No
debe aparecer com
o depen
diente en la declaración de
impuestos sobre el ingreso de otra persona que no sea su cónyuge. 4
) Debe
recertificar su so
licitud cu
ando
se le solicite. 5
) Debe n
otificar a So
CalG
as en u
n
términ
o de 30
días si deja de calificar. 6) Tal vez se le pida co
mpro
bar que reú
ne
los requisitos para C
AR
E.
Decla
ratio
n / D
eclara
ción
: Ple
ase re
ad an
d sig
n b
elo
w / P
or favo
r lea y
firme
abajo
I state that th
e inform
ation
I have provided in
this applicatio
n is tru
e and co
rrect. I agree to provide pro
of of CA
RE
eligibility if asked. I agree to info
rm S
ou
thern
C
aliforn
ia Gas C
om
pany with
in 30
days if I no
lon
ger qualify to
receive a discou
nt. I un
derstand th
at if I receive the disco
unt w
itho
ut qu
alifying fo
r it, I am requ
ired to
pay back the disco
unt I received. I u
nderstan
d that S
oC
alGas can
share m
y inform
ation
with
other u
tilities or agents to
enro
ll me in
their assistan
ce program
s.
Declaro
que la info
rmació
n qu
e propo
rcion
é en este fo
rmu
lario de so
licitud es verdadera y co
rrecta. Co
nvengo
en pro
porcio
nar pru
eba de elegibilidad en el pro
grama
CA
RE
si se me requ
iere. Co
nvengo
en info
rmar a S
ou
thern
Califo
rnia G
as Co
mpany (S
oC
alGas
®) en u
n térm
ino
de 30 días si dejo
de calificar para recibir el descuento.
Entien
do qu
e, si recibo el descu
ento sin
tener derech
o al m
ismo, se m
e exigirá la devolu
ción
del descuento
recibido. Entien
do qu
e So
CalG
as puede co
mpartir m
is datos co
n otras em
presas de servicios públicos o
agentes para inscribirm
e en pro
gramas de asisten
cia.
3 ACCO
UN
T NO
. Please provide your account num
ber to expedite processing. N
O. D
E CUEN
TA
Por favor proporcione su número de cuenta para facilitar procesam
iento.
CUSTO
MER
NA
ME: First and Last as it appears on your bill / N
OM
BR
E DEL CLIEN
TE: Nom
bre y apellido que aparce en su factura
AD
DR
ESS / DO
MICILIO
A
PT # / N
O. D
E APTO
.
CITY / CIU
DA
D
PRIM
ARY
PHO
NE / TELÉFO
NO
PRINCIPA
L
CA
RE
AP
PL
ICA
TIO
NS
OL
ICIT
UD
PA
RA
EL
PR
OG
RA
MA
CA
RE
PL
EA
SE
US
E D
AR
K B
LU
E O
R B
LA
CK
INK
ON
LY
/ PO
R F
AV
OR
US
E T
INT
A A
ZU
L O
SC
UR
A O
NE
GR
A Ú
NIC
AM
EN
TE
- -
To
tal n
um
ber o
f pers
on
s in
yo
ur h
ou
seh
old
(inclu
de y
ou
rself, o
ther a
du
lts a
nd
ch
ildre
n)
Nú
mero
tota
l de p
ers
on
as q
ue v
iven
en
su
ho
ga
r (inclú
ya
se u
ste
d, o
tros a
du
ltos y
niñ
os)
1 2
3
4
5
6
12
Wh
at is y
ou
r yea
rly h
ou
sehold
inco
me (b
efore d
edu
ction
s, inclu
din
g a
ll mem
bers o
f the h
ou
sehold
)?
¿C
ual es el in
greso
an
ual d
e su h
ogar (a
ntes d
e ded
uccio
nes, in
cluy
endo a
todos m
iembro
s del h
ogar)?
$
0 – $
33
,82
0
$3
3,8
21 - $
42
,66
0
$
42
,66
1 - $5
1,50
0
$5
1,50
1 - $6
0,3
40
$
60
,34
1 - $6
9,18
0
If m
ore than $6
9,18
0, enter the dollar am
ount here:
Si es m
ás de $6
9,18
0, escriba el m
onto aquí:$
, .00
per year / al año
Are y
ou (or som
eone in
you
r hou
sehold) en
rolled in an
y of th
e followin
g assistance program
s?
¿E
stá usted (o algu
ien qu
e vive en su
hogar) in
scrito en algu
no de los sigu
ientes program
as de asistencia?
Me
di-C
al/Me
dicaid
: Un
de
r age
65
/ Me
no
r de
65
año
s L
ow Incom
e Hom
e Energy A
ssistance Program
(LIH
EA
P)
Me
di-C
al/Me
dicaid
: 65
or o
lde
r / 65
año
s o m
ás S
up
ple
me
ntal S
ecu
rity In
com
e
Me
di-C
al for F
amilie
s A&
B
Natio
nal S
cho
ol L
un
ch P
rog
ram (N
SL
P)
Wo
me
n, In
fants an
d C
hild
ren
Pro
gram
(WIC
) B
ure
au o
f Ind
ian A
ffairs Ge
ne
ral Assistan
ce
CalW
OR
Ks (T
AN
F) o
r Trib
al TA
NF
H
ead
Start In
com
e E
ligib
le – T
ribal O
nly
/ So
lame
nte
tribal
CalF
resh
(Fo
od
Stam
ps / E
stamp
illas para co
mid
a)
Social S
ecurity / Seguro S
ocial
SS
P or S
SD
I / SS
P o S
SD
I
Pensions / P
ensiones
Interest or dividends from savings, stocks, bonds, or
retirem
ent accounts / Intereses o dividendos de cuentas
de ahorro, acciones, bonos, o cuentas para el retiro
Wages and/or salary / S
alarios y/o ingresos
Cash, other incom
e, or profit from self-em
ployment /
E
fectivo, otro ingreso o ganancias de trabajo independiente
Unem
ployment benefits / B
eneficios de desempleo
Insurance or legal settlements / P
agos de pólizas de
seguro o convenios judiciales
Disability or w
orkers compensation paym
ents / Pagos por
incapacidad o indem
nización para los trabajadores
Spousal or child support / P
ension conyugal o alimenticia
Scholarships, grants, or other aid used for living expenses /
Becas, subvenciones u otros gastos de ayuda utilizados.
Rental or royalty incom
e / Ingresos por alquiler o regalías
Plea
se mark y
ou
r sou
rces of in
com
e / Por fa
vor m
arq
ue su
s fuen
tes de in
greso
If more th
an
6:
si mas d
e 6:
XSIG
NA
TURE
D
ATE
FIRMA
FECH
A
/ /
Y
ES
(If yes, please fill in
the circle(s) l
) S
Í (Si su
resp
ue
sta es afirm
ativa, po
r favor re
llen
e e
l/los círcu
lo/s l
)
NO
(If no
, please an
swer th
e yearly ho
useh
old
inco
me q
uestio
n)
NO
(Si es n
o, p
or favo
r respo
nd
a la preg
un
ta de in
greso
anu
al)
#