
Deakin Research Onlinedro.deakin.edu.au/.../ball-effectsofaholistichealth-2006.pdf · Deakin...
23
Deakin Research Online Deakin University’s institutional research repository DDeakin Research Online Research Online This is the author’s final peer reviewed version of the item published as: Jorna, Michelle, Ball, Kylie and Salmon, Jo 2006-10, Effects of a holistic health program on women's physical activity and mental and spiritual health, Journal of science and medicine in sport, vol. 9, no. 5, pp. 395-401. Copyright : 2006, Sports Medicine Australia.
Transcript of Deakin Research Onlinedro.deakin.edu.au/.../ball-effectsofaholistichealth-2006.pdf · Deakin...

Deakin Research Online Deakin University’s institutional research repository
DDeakin Research Online Research Online This is the author’s final peer reviewed version of the item published as: Jorna, Michelle, Ball, Kylie and Salmon, Jo 2006-10, Effects of a holistic health program on women's physical activity and mental and spiritual health, Journal of science and medicine in sport, vol. 9, no. 5, pp. 395-401. Copyright : 2006, Sports Medicine Australia.

Effects of a holistic health program on women’s physical
activity and mental and spiritual health
Michelle Jorna1, Kylie Ball1, Jo Salmon1
1: Centre for Physical Activity and Nutrition Research, School of Exercise and Nutrition
Sciences, Deakin University, Melbourne, Australia
Submission Date: 19.12.05
Keywords: physical activity intervention, women, mental health
Corresponding Author: Michelle Jorna
School of Exercise and Nutrition Sciences Deakin University
221 Burwood Hwy Burwood VIC 3125
AUSTRALIA Fax: 03 9244 6017
Email: [email protected]

HOLISTIC PHYSICAL ACTIVITY STUDY 2
ABSTRACT
Intervention studies aimed at promoting increased physical activity have been
trialled in many different settings including primary care, worksites and the
community. Churches are also potential settings for physical activity promotion.
However, little is known about the effectiveness of this setting for promoting
physical activity, particularly in Australia. The purpose of this study was to
evaluate the effectiveness of a mind, body and spiritually-based health
promotion program in increasing physical activity and promoting mental and
spiritual health. Nineteen women completed the 8-week intervention, and 30
women in a non-health related 8-week program at the same church comprised
a comparison group. Pre- and post-program surveys assessed outcome
measures. Between-group differences over time were examined using one-way
MANOVA’s. Physical activity was higher in the intervention group than the
comparison group. In contrast to the comparison group, both mental health
(depression symptoms) and spiritual health improved significantly more among
intervention participants. The data highlight the potential for a church-based
setting and holistic approach to health promotion as a successful means of
increasing physical activity and promoting mental and spiritual health among
Australian women.
Abstract Word Count: 183
HOLISTIC PHYSICAL ACTIVITY STUDY 3
INTRODUCTION
Despite the widely recognised benefits of physical activity for both physical and
mental health [1], almost 50% of the Australian population is insufficiently active
[2]. Women tend to be less physically active in their leisure-time than men [2].
The development and trialling of interventions to promote increased physical
activity, particularly among women, is thus an increasingly important public
health priority. Physical activity promotion approaches that target a particular
location or setting (e.g. schools, workplaces, communities) where members of
the population congregate, provide potential opportunities to influence health in
everyday life. There remains much to be learned about the most effective
strategies for promoting physical activity in different settings, with even less
known about effectiveness in women specifically.
One setting that has only recently been utilised as a location for physical activity
interventions is the local community church. One advantage of the church as a
setting is that it can involve a holistic approach to health behaviour change, in
which physical, mental and spiritual health are addressed. Spiritual health refers
to an inherent human quality involving a belief in something greater than the
self, and a faith that positively affirms life [3]. Another benefit of the church
setting for behaviour change is the existing social support structure. Church
support groups have been shown to be valuable in assisting individuals to
initiate and maintain behaviour change [4].
Physical activity interventions conducted in the church setting are few, with the
majority involving African-American samples [5, 6]. Yanek et al. [5] showed a
20-week holistic intervention program was more effective than a self-help
HOLISTIC PHYSICAL ACTIVITY STUDY 4
control group in improving dietary and physical activity behaviours of church-
going African-Americans one year after completing the program. In the ‘Healthy
Body/Healthy Spirit’ project, 16 Atlanta churches [6, 7] were randomised to
either a comparison, self-help or self-help plus telephone counselling
intervention, the latter based on a combination of psychotherapy and
behavioural change theories. Both intervention groups showed significant
increases in physical activity at one-year follow-up. However, the
generalisability of these findings to populations other than African-Americans is
currently unknown.
In Australia, one 12-week church-based physical activity intervention was
conducted among Greek-Australian migrant women [8]. Intervention participants
(n=26) were recruited through the Greek-Orthodox church, and the program
was run in the church building to make use of existing support groups.
However, the comparison group (n=22) was recruited from a different location
and were not church-going. Small improvements in exercise heart rate were
demonstrated within the intervention group, but effects on habitual physical
activity levels were not reported. The program was also not holistic, in that it did
not incorporate a spiritual or mental health component, which is often a key
element of the church-based setting.
Evidence suggests that incorporating a theoretical model of behaviour change
may result in more successful physical activity interventions [9]. Social
Cognitive Theory [10] provides a useful framework for promoting physical
activity, with its focus on relationships between personal, environmental and
behaviour factors. Therefore, this study aimed to investigate the effectiveness

HOLISTIC PHYSICAL ACTIVITY STUDY 5
of a holistic church-based health promotion program, based on Social Cognitive
Theory, among women. In particular, the study aimed to examine the effects of
the program on the key outcome: physical activity; and secondary outcomes:
mental and spiritual health.
METHODS
Participants
Participants in both the intervention and comparison groups were recruited
through local newspaper advertisements, church newsletters, and verbal
announcements via a testimonial video clip played during Sunday church
services. All participants self selected into either the intervention or comparison
groups and paid a fee of $70 ($7 per session) to cover the administration cost of
each program. Participants were deemed eligible if they were women between
the ages of 18-70 years and were able to commit to attend at least 8 of the 10
sessions of the program. Participants in the intervention group were also
required to obtain written medical clearance from a physician, and to agree to
increase their physical activity levels throughout the duration of the program.
This research study was approved by the Deakin University Human Research
Ethics Committee. All participants provided written informed consent before
commencing the program.
Measures
Participants in both the intervention and the comparison groups completed
questionnaires to assess physical activity, mental health, and spiritual health, at
baseline and week 8, immediately pre- and post-intervention. Demographic
characteristics assessed at baseline included age, gender, marital status and

HOLISTIC PHYSICAL ACTIVITY STUDY 6
education. Since body weight may be a barrier to physical activity among
women [11], self-reported weight and height were assessed and used to
calculate body mass index [BMI: body weight (kg) / height (m2)] as a potential
confounder.
Physical activity
Physical activity was assessed using the self-report, self-completion survey
instrument called the CHAMPS (Community Healthy Activity Models Program
for Seniors) survey, which has been validated in the USA and Australia, which
assesses physical activity behaviours and attitudes [12, 13]. This measure has
been shown to be sensitive to change in physical activity in trials in both the
USA [12, 14] and Australia [15].
Two components from the CHAMPS questionnaire were used to indicate
physical activity. Firstly, participants’ time spent walking was assessed by
summing the total weekly duration recorded for each CHAMPS item for this
variable (including brisk walking, hill walking, leisurely walking and walking for
errands) and converting to hours per week. Secondly, participants’ time spent in
moderate and vigorous physical activity (MVPA) was assessed by combining
CHAMPS activities of 3-6 metabolic equivalents (METS; moderate intensity)
[16] or greater than 6 METS (vigorous intensity), and converting to total duration
in hours per week. To take into account the greater health benefits associated
with higher intensity physical activity [1], time spent in CHAMPS items for
activities of vigorous intensity (6 METS or greater) were weighted by two [2]. It
should be noted that the two measures of physical activity (walking, MVPA)
HOLISTIC PHYSICAL ACTIVITY STUDY 7
were not mutually exclusive, as there was some overlap of walking activities
counted in the two measures.
Mental health, in particular depression, was assessed using the well-validated
CES-D scale [17]. Spiritual health was assessed using the validated Spiritual
Well-Being Scale [18]. We calculated that the two scales had internal reliability
of 0.91 and 0.94 (Cronbach’s Alpha) respectively.
Procedure
This research project was conducted as part of an existing externally run
program provided by Careforce Lifekeys Ministries, an initiative of a local
church. The program was piloted-tested several times before evaluation.
Intervention Group
This ten-session, eight-week women’s health program titled “Embracing a
Healthy Lifestyle”, used a holistic mind-body-spirit framework, and involved
education, social support and experiential approaches to promoting health. The
program was conducted by trained staff with tertiary qualifications in a relevant
health discipline. During the first session (baseline), the initial survey was
administered followed by an introduction/orientation to the program. The
remaining sessions were conducted weekly at a local church. Each of these
sessions included a 45-minute group teaching session on varying topics, a 45-
minute focus group discussing each topic, and a 30-minute moderate intensity
group physical activity session. The topics covered in the education component
included: aerobic physical activity, motivation, nutrition, emotional eating, body
image, strength training, weight management, women’s health issues, and long
term maintenance of a healthy lifestyle. The focus group sessions facilitated
HOLISTIC PHYSICAL ACTIVITY STUDY 8
discussion on the weekly topic and application to each individual in the group.
Individual goals and barriers in each area were discussed and personalised
suggestions for incorporating lifestyle changes were given by a qualified
facilitator. The intervention also supported the women in identifying and
accessing walking tracks and other physical activity facilities, clubs and support
groups in their local neighbourhoods. The intervention thus incorporated
multiple key elements hypothesised by Social Cognitive Theory to be important
(e.g. fostering self-efficacy, observational learning and social support,
overcoming environmental barriers). The final survey was administered during
the final session for both groups.
Comparison Group
The comparison group was made up of individuals who had enrolled in a non-
health-related relationship education and social support program run by the
same local church. That program was designed to help participants learn how to
overcome negative past experiences, and to provide strategies and skills
needed to make positive and lasting changes in relationships. The program was
run concurrently with the intervention group for the same duration and at the
same venue, and was hence matched on contact time (with a course instructor
and with other group participants) to the intervention group. Participants in the
relationship program were invited to take part in the research study as a
comparison group, which involved completing the same assessment measures
as the intervention group, at baseline and post-intervention.
HOLISTIC PHYSICAL ACTIVITY STUDY 9
Statistical analyses
All data were analysed using SPSS 12.0. Ten participants in total (3 from the
intervention group and 7 from the comparison group) did not complete the week
8 survey. Data for these participants were included in analyses, and a
conservative approach to imputing missing data was adopted [19] by which
available baseline scores on variables were imputed as week 8 scores.
Baseline values of all demographic and outcome variables were examined for
intervention group differences using independent t-tests for continuous
measures, and chi-square tests for categorical measures. For all outcome
variables, a series of one-way MANOVAs was conducted to assess between-
group differences in outcome measures over time (i.e. a time by group
interaction). Follow-up paired t-tests were conducted to compare within-group
differences over time.
Body weight has been previously established as a correlate of physical activity
[11]. To assess the need to adjust for potential confounding by body weight in
this study, correlations of BMI with each outcome measure were tested using
Pearson’s bivariate test for statistical significance. Where a significant
relationship was found between baseline BMI and the outcome variable of
interest (spiritual health only), BMI was included as a covariate in a multivariate
analysis of covariance (MANCOVA).
RESULTS
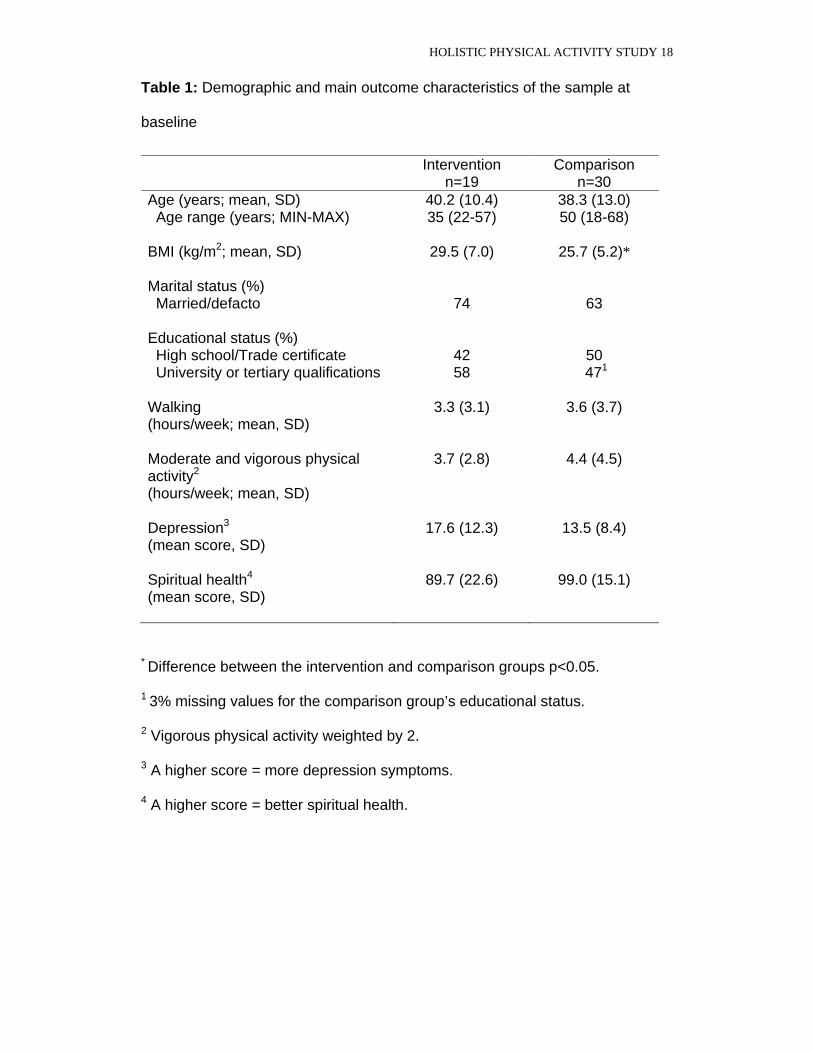
Descriptive data on demographics and each of the outcome variables at
baseline are presented in Table 1. With the exception of BMI, there were no
HOLISTIC PHYSICAL ACTIVITY STUDY 10
differences between the intervention and the comparison groups on any of the
demographic or outcome variables. The mean BMI of the participants in the
intervention group was significantly higher than that of participants in the
comparison group (p=0.037).
Insert Table 1 here
Mean time spent walking at baseline and week 8 for the intervention and
comparison groups are presented in Figure 1. Results of the MANOVA
predicting time spent walking showed a significant interaction between
intervention group and time, suggesting that the difference between baseline
and week 8 scores varied across the two groups (Wilks = 0.87, F(1, 46) = 6.96,
p=0.011). Follow-up paired t-tests showed that for intervention group only, time
spent walking per week was significantly higher at week 8 compared to baseline
(intervention: mean change 0.53 hrs/week, CI 0.18, 0.87; t(18) = 3.22, p=0.005;
comparison: mean change 0.04 hrs/week, CI -0.16, 0.25; t(28) = 0.44, p=0.664).
Mean times spent in combined moderate and vigorous physical activity (MVPA)
at baseline and week 8 for the intervention and comparison groups are
presented in Figure 2. Results of the MANOVA predicting time spent in MVPA
showed a significant interaction between intervention group and time,
suggesting that the difference between baseline and week 8 scores varied
across the two groups (Wilks = 0.89, F(1, 44) = 5.52, p=0.023). Follow-up
paired t-tests showed that for intervention group only, time spent in MVPA per
week was significantly higher at week 8 compared to baseline (intervention:

HOLISTIC PHYSICAL ACTIVITY STUDY 11
mean change 0.62 hrs/week, CI -0.03, 1.21; t(18) = 2.21, p=0.040; comparison:
mean change 0.01 hrs/week, CI -0.21, 0.23; t(28) = 0.44, p=0.920).
Insert Figures 1 and 2 about here
Mean depression scores at baseline and week 8 for the intervention and
comparison groups are presented in Figure 3. There was a significant
interaction between intervention group and time (Wilks = 0.90, F(1, 47) = 5.07,
p=0.029). Paired t-tests showed that for intervention group only, depression
symptoms were significantly lower at week 8 compared to baseline
(intervention: mean change -5.26, CI -0.61, -9.91; t(18) = 2.38, p=0.029;
comparison: mean change 0.43, CI -2.53, 3.39; t(29) = 0.30, p=0.767).
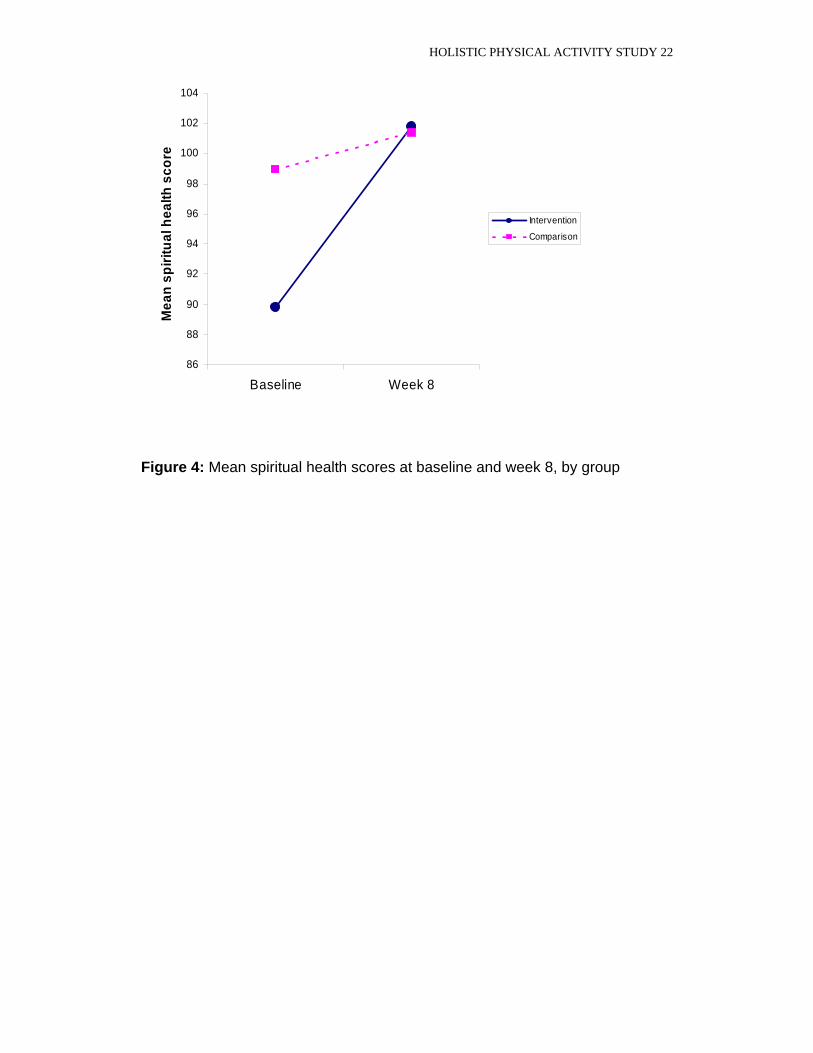
Mean spiritual health scores at baseline and week 8 for the intervention and
comparison groups are presented in Figure 4. Results of the MANCOVA
(controlling for baseline BMI) showed a significant intervention group-time
interaction (Wilks = 0.85, F(1, 43) = 7.41, p=0.009). Paired t-tests showed that
for intervention group only, spiritual health was significantly higher at week 8
compared to baseline (intervention: mean change 12.22, CI 5.13, 19.32; t(17) =
3.64, p=0.002; comparison: mean change 2.40, CI -0.09, 4.89; t(29) = 1.97,
p=0.059).
Insert Figures 3 and 4 about here
HOLISTIC PHYSICAL ACTIVITY STUDY 12
DISCUSSION
To our knowledge, this study is the first of its kind in Australia, aimed to
evaluate the effectiveness of a mind, body and spiritually-based health
promotion program in increasing physical activity, as well as improving mental
and spiritual health in women. Results suggest that the intervention was
effective in significantly increasing physical activity levels as assessed by two
different measures: total walking duration; and total time spent in moderate and
vigorous physical activity, compared to a comparison group. The intervention
group reported increasing their walking time by an average of half an hour per
week, and increasing their time spent in moderate and vigorous physical activity
by 0.63 hours per week (these two increases share some overlap, as the
variables walking uphill and brisk walking were included in both scores). The
present findings are consistent with the limited research available in African-
American samples in the US [20, 21], and indicate the potential for church-
based settings in assisting women in the community to become more active.
Positive effects of the intervention on mental health were also observed in the
present study. Symptoms of depression decreased significantly within the
intervention group relative to the control group. This is somewhat consistent
with the known benefits of physical activity [1], although this finding may be an
effect of improvements in other health areas. Having increased social support,
encouragement and individual goal achievement and counselling in the support
group component of the program may have contributed to improvements in
mental health. The difference between the intervention and comparison groups
was somewhat surprising considering the comparison group were undertaking
steps to more positive relationship building and were exposed to the same
HOLISTIC PHYSICAL ACTIVITY STUDY 13
amount of time in a support group as part of their program. The experiential
physical activity component of the intervention combined with the holistic
approach may have contributed to the improvements in mental health among
women in the intervention group.
The connection between spirituality, or religious practices, and reduced risk of
all-cause mortality has been well documented [22-24], but a relationship
between physical activity and spiritual health has not been previously
researched. In the present study, spiritual health scores in the intervention
group significantly improved compared to the comparison group. This finding
was unexpected as the comparison group had a similar spiritual component in
their program. It may be that a program including multiple aspects of health,
mind, body and spirit produces additional benefits to spiritual health, beyond
those of a spiritual component alone. It is however difficult to separate program
components and attribute the positive effects to any one particular aspect of the
program, as all occurred simultaneously. Further research that assesses
separate components of the program could help to determine those aspects
most important in promoting increased physical activity and improved mental
and spiritual health.
Ideally, effective physical activity intervention studies could provide insights into
the specific factors that mediate increases in physical activity behaviour. Due to
the small number of participants in the present study, we did not have the power
to conduct mediational analyses. However, supplementary analyses
investigating changes in key cognitive and social factors hypothesised by Social
Cognitive Theory to be important (data not shown) demonstrated that self-

HOLISTIC PHYSICAL ACTIVITY STUDY 14
efficacy and perceived social support significantly improved, and perceived
personal barriers significantly decreased, in the intervention group relative to
the comparison group between pre- and post-intervention. These findings,
which corroborate those of previous research [25], are consistent with the
hypothesis that self-efficacy, perceived barriers and social support are important
mediators of changes in physical activity among adults.
This program focused on self-selected women volunteers, and hence caution
should be exercised in generalising these findings to the wider population. In
addition, the longer-term maintenance of these lifestyle behaviour changes has
not yet been determined. As the present study did not randomise participants
into the intervention or comparison groups, there may have been other
important differences between groups (e.g. health status) that were not
assessed and that confounded the study findings, although statistical
adjustments were made for confounding by BMI. The study was also limited by
the small number of women. All the measures in the present study were self-
reported, and hence subject to response biases. A more objective measure of
physical activity (eg. pedometers or accelerometers) could be incorporated to
complement the self-reported measures in future research.
The present results suggest that a church-based holistic health program shows
much potential as an approach to promoting physical activity and spiritual and
mental health among women in Australia. The positive effects on physical,
mental and spiritual health evident in the present study could, if achieved across
larger segments of the population, play an important role in decreasing the
burden of a variety of chronic lifestyle diseases, and improving the health of
HOLISTIC PHYSICAL ACTIVITY STUDY 15
Australian women. Wider dissemination of the program and co-operation with
local and state governing bodies to fund and empower local churches to run
similar programs could facilitate the translation of the program to real-world
settings.
Acknowledgments
Kylie Ball is supported by a National Health & Medical Research
Council/National Heart Foundation of Australia Career Development Award. Jo
Salmon is supported by a VicHealth Public Health Fellowship.
PRACTICAL IMPLICATIONS
Setting coment.
Strategy comment.
Targeting women.
Effective in increasing physical activity, decreasing depressive symptoms
and increasing spiritual health.
HOLISTIC PHYSICAL ACTIVITY STUDY 16
REFERENCES
1. US Department of Health and Human Services, Physical Activity and Health: A Report of the Surgeon General. 1996, Atlanta: GA: Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion.
2. Armstrong T, Bauman A and Davies J, Physical activity patterns of Australian adults: Results of the 1999 National Physical Activity Survey. 2000, Australian Institute of Health and Welfare: Canberra.
3. Miller MA. Culture, spirituality, and women's health. J Obstet Gynecol Neonatal Nurs, 1995; 24(3): 257-63.
4. Lasater TM, Becker DM, Hill MN, et al. Synthesis of findings and issues from religious-based cardiovascular disease prevention trials. Ann Epidemiol, 1997; 7 (Suppl): S46-S53.
5. Yanek LR, Becker DM, Moy TF, et al. Project Joy: faith based cardiovascular health promotion for African American women. Public Health Rep, 2001; 116 (Suppl 1): 68-81.
6. Resnicow K, Jackson A, Blissett D, et al. Results of the healthy body healthy spirit trial. Health Psychol, 2005; 24(4): 339-48.
7. Resnicow K, Jackson A, Braithwaite R, et al. Healthy Body/Healthy Spirit: a church-based nutrition and physical activity intervention. Health Educ Res, 2002; 17(5): 562-73.
8. Brown WJ, Lee C and Oyomopito R. Effectiveness of a bilingual heart health program for Greek-Australian women. Health Promot Int, 1996; 11(2): 117-125.
9. Sallis JF and Owen N, Physical Activity and Behavioral Medicine. 1999, CA: Sage: Thousand Oaks.
10. Bandura A, Social foundations of thought and action. 1986, NJ: Prentice-Hall: Englewood Cliffs.
11. DiPietro L. Physical activity, body weight, and adiposity: An epidemiologic perspective. Exerc Sport Sci Rev, 1995; 23: 275-303.
12. Stewart AL, Mills KM, King AC, et al. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc, 2001; 33(7): 1126-41.
13. Cyarto EV, Marshall AL, Dickinson RK, et al. Measurement properties of the CHAMPS physical activity questionnaire in a sample of older Australians. J Sci Med Sport, 2006; In Press.
HOLISTIC PHYSICAL ACTIVITY STUDY 17
14. King AC, Rejeski WJ and Buchner DM. Physical activity interventions targeting older adults. A critical review and recommendations. Am J Prev Med, 1998; 15(4): 316-33.
15. Ball K, Salmon J, Leslie E, et al. Piloting the feasibility and effectiveness of print- and telephone-mediated interventions for promoting the adoption of physical activity in Australian adults. J Sci Med Sport, 2005; 8(2): 134-42
16. Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc, 1993; 25(1): 71-80.
17. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Ap Psych M, 1977; 1: 385-401.
18. Ellison CW. Spiritual well-being: Conceptualization and measurement. J Psychol Theol, 1983; 11(4): 330-340.
19. Pocock SJ, Clinical Trials: A Practical Approach. 1983, NY: Wiley.
20. Campbell MK, Demark-Wahnefried W, Symons M, et al. Fruit and vegetable consumption and prevention of cancer: the Black Churches United for Better Health project. Am J Public Health, 1999; 89(9): 1390-6.
21. Resnicow K, Jackson A, Wang T, et al. A motivational interviewing intervention to increase fruit and vegetable intake through Black churches: results of the Eat for Life trial. Am J Public Health, 2001; 91(10): 1686-93.
22. Powell LH, Shahabi L and Thoresen CE. Religion and spirituality. Linkages to physical health. Am Psychol, 2003; 58(1): 36-52.
23. Mullen K. Religion and health: A review of the literature. Int J Sociol Soc Policy, 1990; 10(1): 85-96.
24. Seeman TE, Dubin LF and Seeman M. Religiosity/spirituality and health. A critical review of the evidence for biological pathways. Am Psychol, 2003; 58(1): 53-63.
25. Sallis JF, Hovell MF, Hofstetter CR, et al. Explanation of vigorous physical activity during two years using social learning variables. Soc Sci Med, 1992; 34(1): 25-32.
HOLISTIC PHYSICAL ACTIVITY STUDY 18
Table 1: Demographic and main outcome characteristics of the sample at
baseline
Intervention n=19
Comparison n=30
Age (years; mean, SD) Age range (years; MIN-MAX)
40.2 (10.4) 35 (22-57)
38.3 (13.0) 50 (18-68)
BMI (kg/m2; mean, SD)
29.5 (7.0) 25.7 (5.2)*
Marital status (%) Married/defacto
74
63
Educational status (%) High school/Trade certificate University or tertiary qualifications
42 58
50
471
Walking (hours/week; mean, SD)
3.3 (3.1) 3.6 (3.7)
Moderate and vigorous physical activity2 (hours/week; mean, SD)
3.7 (2.8) 4.4 (4.5)
Depression3 (mean score, SD)
17.6 (12.3) 13.5 (8.4)
Spiritual health4 (mean score, SD)
89.7 (22.6) 99.0 (15.1)
* Difference between the intervention and comparison groups p<0.05.
1 3% missing values for the comparison group’s educational status.
2 Vigorous physical activity weighted by 2. 3 A higher score = more depression symptoms. 4 A higher score = better spiritual health.

HOLISTIC PHYSICAL ACTIVITY STUDY 19
1.4
1.5
1.6
1.7
1.8
1.9
2
2.1
2.2
Baseline Week 8
Wa
lkin
g h
rs/w
ee
k
Intervention
Comparison
Figure 1: Total time (hrs/wk) spent walking at baseline and week 8, by group

HOLISTIC PHYSICAL ACTIVITY STUDY 20
1.7
1.8
1.9
2
2.1
2.2
2.3
2.4
2.5
Baseline Week 8
MV
PA
hrs
/we
ek
Intervention
Comparison
Figure 2: Total time (hrs/wk) spent in combined moderate and vigorous
physical activity at baseline and week 8, by group

HOLISTIC PHYSICAL ACTIVITY STUDY 21
11
12
13
14
15
16
17
18
Baseline Week 8
Me
an
de
pre
ss
ion
sc
ore
Intervention
Comparison
Figure 3: Mean depression scores at baseline and week 8, by group
HOLISTIC PHYSICAL ACTIVITY STUDY 22
86
88
90
92
94
96
98
100
102
104
Baseline Week 8
Me
an
sp
irit
ua
l he
alt
h s
co
re
Intervention
Comparison
Figure 4: Mean spiritual health scores at baseline and week 8, by group


















