
Design Book Cras - ColorMaster, Dual Paint & Primer, Glitter

241
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited EditorialsThe cardiorenal syndrome as the cardiologist sees it - H. J. Dargie 243
The cardiorenal syndrome as the nephrologist sees it - D. Goldsmith 248
Lead Article Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - P. R. Kalra, P. A. Kalra 251
Expert Answers to Three Key Questions How can we reduce sudden cardiac death in cardiorenal syndrome? - R. N. Foley, C. A. Herzog 267
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - L. M. Ruilope 277
Should anemia be actively treated in cardiorenal syndrome? - E. A. Jankowska, P. Ponikowski 284
Fascinoma Cardiologica A Lexicon of the Heart: Heart and kidney in early Chinese medicine - F. Scheffler 295
Summaries of Ten Seminal Papers - P. R. Kalra, P. A. Kalra 299
Bibliography of One Hundred Key Papers 311
The clinical epidemiology of cardiac disease in chronic renalfailure – P. S. Parfrey, R. N. Foley
Hormones and hemodynamics in heart failure – R. W. Schrier,
W. T. Abraham
The use of subcutaneous erythropoietin and intravenous ironfor the treatment of the anemia… – D. S. Silverberg and others
Albuminuria and risk of cardiovascular events, death, andheart failure in diabetic and nondiabetic individuals H. C. Gerstein
Arterial media calcification in end-stage renal disease: impact onall-cause and cardiovascular mortality – G. M. London and others
Chronic kidney disease and the risks of death, cardiovascularevents, and hospitalization – A. S. Go and others
The severe cardiorenal syndrome: “Guyton revisited” L. G. Bongartz and others
Renal function as a predictor of outcome in a broad spectrumof patients with heart failure – H. L. Hillege and others
Cardiorenal syndrome – C. Ronco and others
Ferric carboxymaltose in patients with heart failure and irondeficiency – S. D. Anker and others
Cardiorenal Syndrome
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 241

242
Avkiran M, PhD Cardiovascular Research The Rayne InstituteSt Thomas’ HospitalLondon, UK
Bassand JP, MDDept of CardiologyUniversity Hospital Jean MinjozBesançon, France
Bertrand ME, MDHôpital CardiologiqueLille, France
Bolli R, MDDivision of CardiologyUniversity of LouisvilleLouisville, KY, USA
Camm JA, MDDept of Cardiac and Vascular SciencesSt George’s University of LondonLondon, UK
Coats A, MDFaculty of MedicineUniversity of SydneySydney, Australia
Cobbe SM, MDDept of Medical CardiologyGlasgow Royal InfirmaryGlasgow, UK
Cohn JN, MDRasmussen Center for Cardiovascular Disease PreventionMinneapolis, MN, USA
Cokkinos DV, MD1st Cardiology DeptOnassis Cardiac Surgery CenterAthens, Greece
Cowie M, MD, PhDDept of Clinical CardiologyNational Heart & Lung InstituteLondon, UK
Danchin N, MDDept of CardiologyHôpital Européen Georges PompidouParis, France
Dargie HJ, MDCardiac ResearchWestern InfirmaryGlasgow, UK
Di Pasquale G, MDDpt of CardiologyMaggiore HospitalBologna, Italy
Dzau VJ, MDDuke University Medical Center & Health System DUMCDurham, NC, USA
Consulting Editors
Editors in ChiefFerrari R, MD, PhDDept of Cardiology, Arcispedale S. AnnaUniversity of Ferrara, Ferrara, Italy
Hearse DJ, BSc, PhDThe Cardiothoracic Centre, The Rayne InstituteSt Thomas’ Hospital, London, UK
Fernandez-Aviles F, MDInstitute of Hematology and Oncology, IDIBAPSHospital University Clinic of Barcelona Barcelona, Spain
Fox KM, MDDept of CardiologyRoyal Brompton HospitalLondon, UK
Fox KA, MDDept of Cardiological ResearchUniversity of EdinburghEdinburgh, UK
Fuster V, MD, PhDCardiovascular InstituteMount Sinai Medical CenterNew York, NY, USA
Hasenfuss G, MDDept of CardiologyGeorg-August UniversitätGöttingen, Germany
Hori M, MD, PhDDept of Internal Medicine and TherapeuticsOsaka University Graduate School of MedicineOsaka, Japan
Katz AM, MDUniversity of Connecticut School of MedicineFarmington, CT, USA
Komajda M, MDDept of CadiologyCHU Pitié-SalpêtrièreParis, France
Komuro I, MD, PhDDept of Cardiovascular Sciences & MedicineChiba University Graduate School of MedicineChiba, Japan
Lakatta EG, MDNational Institute on AgingGerontology Research CenterBaltimore, MD, USA
Libby P, MDCardiovascular MedicineBrigham & Women’s HospitalBoston, MA, USA
Lonn E, MDHamilton Health Sciences General SiteHamilton, Ontario, Canada
Lopez-Sendon JL, MDCCU Dept of CardiologyHospital University Gregorio MaranonMadrid, Spain
Maggioni AP, MDANMC Research CenterFirenze, Italy
Marber MS, MD, PhDCardiovascular Research The Rayne Institute St Thomas’ HospitalLondon, UK
Oto A, MDMedical Office, Hacettepe University School of MedicineAnkara, Turkey
Patrono C, MDDept of PharmacologyUniversity La SapienzaRome, Italy
Pepine CJ, MDDept of MedicineUniversity of FloridaGainesville, FL, USA
Rapezzi C, MDInstitute of CardiologyUniversity of BolognaBologna, Italy
Remme WJ, MD, PhDSticares FoundationRotterdam, The Netherlands
Rosen MR, MDDept of Pharmacology &PediatricsColumbia University College of Physicians & SurgeonsNew York, NY, USA
Ruzyllo W, MDNational Institute of CardiologyWarsaw, Poland
Ryden L, MD, PhDDept of CardiologyKarolinska University Hospital SolnaStockholm, Sweden
Schneider MD, MDBaylor College of MedicineHouston, TX, USA
Seabra-Gomes RJ, MDInstituto do CoracaoHospital Santa CruzCarnaxide, Portugal
Sechtem U, MDDept of Internal Medicine & CardiologyRobert Bosch KrankenhausStuttgart, Germany
Simoons ML, MDThoraxcenterErasmus University Medical CenterRotterdam, The Netherlands
Sleight P, MDDept of Cardiovascular MedicineJohn Radcliffe HospitalOxford, UK
Soler-Soler J, MD Dept of CardiologyHospital General Vall d’HebronBarcelona, Spain
Steg PG, MDDept of CardiologyHôpital Bichat–Claude BernardParis, France
Swedberg K, MD, PhDDept of MedicineSahlgrenska University Hospital OstraGöteborg, Sweden
Tardif JC, MDMontreal Heart InstituteMontreal, Quebec, Canada
Tavazzi L, MDDivision of CardiologyPoliclinico San Matteo IRCCSPavia, Italy
Tendera M, MD3rd Division of CardiologySilesian School of MedicineKatowice, Poland
Vanhoutte PM, MDDept of PharmacologyUniversity of Hong Kong Faculty of MedicineHong Kong, China
Widimsky P, MD, PhDVinohrady CardiocenterCharles University HospitalPrague, Czech Republic
Wijns WC, MDCardiovascular Center AalstOLV Hospital, Aalst, Belgium
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 242

Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
243
Henry J. Dargie, MB, ChB, FRCP, FESC, FRSEDepartment of Cardiology - Western Infirmary - Glasgow - Scotland - UK
eons before modern treatments, worsening kidney function in heart failure
was commonplace. It was not called “cardiorenal syndrome.” It signaled the
end stage of heart failure. Although angiotensin-converting enzyme (ACE)
inhibitors, β-blockers, aldosterone antagonists, and angiotensin receptor
blockers have greatly improved symptoms and outcomes, the fickle kidneys still plague
the lives of both patient and doctor. The kidneys have always been at the heart of heart
failure treatment. William Withering, in his “An Account of the Foxglove and Some of itsMedical Uses” published in 1785, describes many cases of “dropsy,” which responded
well to digitalis. “The patient took five draughts which made her very sick and acted
very powerfully upon the kidney, for within the first twenty-four hours she made up-
wards of eight quarters of water.” This fluid loss of nearly 7 liters was associated with
dramatic symptomatic relief in a patient who lived for many more years sustained by
intermittent less toxic doses of digitalis. Withering recounts that those who responded
best to digitalis had a “weak, often intermittent pulse” suggestive of atrial fibrillation
and a cardiac cause for the widespread edema.1
Richard Bright was one of three great “guys” of Guy’s Hospital in19th-century London, his
compatriots being Thomas Addison and Thomas Hodgkin. Bright described the clinical
features of nephritis, which in many patients also included dropsy, thus demonstrating
that “dropsy” was not universally attributable to heart failure. In some of these patients
there was cardiac hypertrophy often, but not always, associated with hypertension.
Withering, therefore, in his description of what the heart could do to the kidney, and
Bright, on what the kidney could do to the heart, were early commentators on the
“cardiorenal syndrome.”
Invited Editorial
A
•••
THE CARDIORENAL SYNDROME AS THE CARDIOLOGIST SEES IT
See page 248 for the companion Invited Editorial by David Goldsmith:THE CARDIORENAL SYNDROME AS THE NEPHROLOGIST SEES IT
Professor Henry J. Dargie, MB, ChB, Department of Cardiology, Western Infirmary, Dumberton Road, Glasgow G11 6NT, UK(e-mail: [email protected])
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 243

The increasing awareness of the bidirectional influences of heart and kidney was the
stimulus to the broadening of the term “cardiorenal syndrome.” In their review of
the topic in the Journal of the American College of Cardiology in 2008, Ronco and his
colleagues recognized no fewer than five varieties of the cardiorenal syndrome.2 It has
also been argued that anemia is such a common and important aspect of the coexis-
tence of heart and kidney disease that “cardio-renal-anemia syndrome” (CRAS) is a
legitimate subtype of cardiorenal syndrome; and, since iron deficiency is a major cause
of the anemia that the term “cardio-renal-anemia-ID syndrome” (CRAIDS) is also valid
and useful.3
At this point the reader may be excused for being daunted by the apparent considerable
complexity of the cardiorenal syndrome and related subsyndromes. In this issue of
Dialogues, however, four excellent articles combine to demonstrate the present scope
and scale of malevolent heart and kidney interactions. They also seek to clarify their
various presentations.
Firstly, the brothers Paul R. Kalra and Philip A. Kalra, of whom one is a cardiologist and
the other a nephrologist, succinctly summarize the cardiorenal syndrome. Essentially,
Types 1 and 3 are acute heart failure as a cause or effect of acute kidney injury. In
Types 2 and 4, chronic heart failure is either a cause or effect of chronic kidney disease
(CKD). In Type 4, however, when severe CKD appears to have caused cardiac dysfunction,
clinical heart failure need not be present for the case to be considered a cardiorenal
syndrome. In Type 5 cardiorenal syndrome, both heart and kidney may be affected
simultaneously by the same pathology. Acutely, this may result from severe systemic
infections and chronically by diseases that can affect either organ, especially athero-
sclerosis, diabetes, and hypertension, and, more rarely, amyloidosis.
For cardiologists, the most common clinical scenario of the cardiorenal syndrome is the
patient with, primarily, heart failure, in whom renal dysfunction supervenes. There are
several candidate causes. The common clinical assumption is a presumed fall in renal
blood flow, though this is rarely confirmed due to lack of suitable clinical methods of
measurement. Renal perfusion is preserved over a wide range of blood pressures, but
either due to heart failure itself and a poor cardiac output all specific treatments for heart
failure lower the blood pressure and risk compromising renal blood flow and function.
More recently, as discussed by Paul R. Kalra and Philip A. Kalra in their Lead Article,
tubular dysfunction may supervene especially in acute heart failure.3 The development
of novel markers for this, such as NGal (neutrophil gelatinase-associated lipocalin),
opens a new door of therapeutics since earlier objective recognition of renal damage
may lead to a more urgent, possibly better targeted approach to its treatment.4
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
244
•••
•••
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 244

An important aspect of this is the extent to which such damage is reversible and whether
this might mitigate or prevent the resultant renal dysfunction. In acute coronary syn-
dromes (ACS), there is a sense of urgency in addressing the underlying pathophysiology
with antithrombotic or fibrinolytic treatments being applied immediately and appro-
priately on diagnosis. Aspects of quality of care in ACS are time to application of treat-
ment as it is recognized that time delays mean loss of myocytes. By analogy, time delay
could also be regarded as loss of nephrons. Thus, simple time to the institution of
appropriate diuretic, vasodilator, or even inotropic therapy in order to reduce renal
congestion and improve renal blood flow could become a quality marker.
Secondly, Robert N. Foley and Charles A. Herzog focus on severe or end-stage kidney
disease (ESKD) causing ventricular dysfunction leading not only to heart failure, but
also to sudden cardiac death from presumed ventricular arrhythmia.4 Indeed, this is a
major unsolved problem for such patients. In recent years, the impact of primary renal
disease on the heart, apart from, or in addition to, the secondary effects of associated
hypertension has attracted much interest.5,6
It was the development of renal replacement therapy with chronic dialysis that has
allowed large numbers of patients with ESKD to survive long enough for the effects of
sustained renal failure on the heart to become apparent. And, although the major success
of renal transplantation is greatly appreciated, it has brought another set of issues
related to long survival times for patients with hearts previously affected by uremia and
chronic hypervolemia only partially corrected by hemodialysis. The notion of a specific
uremic cardiomyopathy receives support from recent studies in which cardiac magnetic
resonance imaging has demonstrated patchy late enhancement consistent with fibrosis
occurring in a noninfarction distribution.
Robert N. Foley and Charles A. Herzog raise the issue of the severe lack of adequately
powered clinical trials of prevention of sudden death in these patients. Encouraging,
but not conclusive, evidence of benefit comes from small studies of β-blockers in ESKD
especially with carvedilol.7 Foley also raises the issue of large randomized studies of
intracardiac defibrillators (ICDs) in this population for many of whom the first clinical
manifestation of heart disease may be sudden cardiac death due to presumed lethal
ventricular arrhythmia. Interesting in itself, that research also would contribute greatly to
establishing the cause of sudden cardiac death as any arrhythmia would be captured
by the device.
Thirdly, Ewa A. Jankowska and Piotr Ponikovski discuss the multiple causes and con-
sequences of anemia in patients with heart failure.4 Deficiency of, or resistance to,
the normal physiological effects of hemopoietic factors, especially erythropoietin and
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
245
•••
•••
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 245

iron, are the major causes of anemia, similar to the anemia of other chronic illnesses.8
They recommend that patients with CKD be screened for anemia and iron deficiency and
that full hematological testing is appropriate for the adequate management of anemia.
Large clinical trials are under way to investigate the impact of iron therapy, especially
intravenously, on quality of life and outcomes in patients with heart failure.
Finally, Luis M. Ruilope argues that the cardiorenal syndrome is an intrinsic component
of the “cardiovascular continuum” from risk factors to target organ damage and hence
to overt atherosclerotic cardiovascular disease.9 Diabetes and hypertension remain the
major population-attributable causes of kidney disease in the community contributing
substantially to both covert and overt renal dysfyunction.4 Early kidney disease has
not convincingly been shown to cause cardiovascular disease (CVD) and if CVD is
present in early CKD it seems most likely that hypertension and or diabetes will have
been responsible for both the CVD and renal impairment.10
The strong clinical message here, as stressed by Luis M. Ruilope, is the utmost impor-
tance of the primary and secondary prevention of target organ damage from hypertension,
atherosclerosis, and diabetes. This review also reminds us that when patients with heart
failure develop problems with kidney function there may well be covert permanent
structural damage, which their worsening heart failure has rendered overt. This is a
common clinical conundrum that is of vital importance to all patients with heart failure
and especially to those who otherwise would be good candidates for heart transplanta-
tion. At present, our ability, clinically, to assess early intrinsic kidney disease, is limited.
It is beyond doubt that the “cardiorenal syndrome” is no single entity. The sheer variety
of causes, consequences, and mechanisms, together with their multiple implications
for treatment, demand that it should surely always be referred to in the plural. The
obvious clinical comparison is with acute coronary syndromes (ACS), a term that
emphasizes differences among its components according to clinical presentation with
distinct management pathways based on the underlying pathophysiology. Current
classifications of cardiorenal interactions have been helpful in categorizing the different
clinical scenarios, but they are essentially descriptive and should stimulate more tar-
geted research into mechanisms and treatment.
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
246
•••
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 246

Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
247
1. Withering W.
An Account of the Foxglove and Some of its Medical Uses.1735.
2. Ronco C, Haapio M, House AA, Anavekar N,Bellomo R.
Cardiorenal syndrome.
J Am Coll Cardiol. 2008;52(19):1527-1539.
3. Palazzuoli A, Gallotta M, Iovine F, Nuti R,Silverberg DS.
Anaemia in heart failure: a common interaction with renalinsufficiency called the cardio-renal-anaemia syndrome.
Int J Clin Pract. 2010;15:290-301.
4. Damman K, Masson S, Hillege HL, et al.
Clinical outcome of renal tubular damage in chronicheart failure.
Eur Heart J. 2011;32(21):2705-2712.
5. Foley RN, Parfrey, PS, Harnett JD, et al.
Clinical and echocardiographic disease in patientsstarting end-stage renal disease therapy.
Kidney Int. 1995;47(1):186-192.
6. Silverberg JS, Barre PE, Prichard SS, et al.
Impact of left ventricular hypertrophy on survival inend stage renal disease.
Kidney Int. 1989;36(2):286-290.
7. Cice G, Ferrara L, D’Andrea A, et al.
Carvedilol increases two-year survival in dialysis patientswith dilated cardiomyopathy: a prospective placebocontrolled study.
J Am Coll Cardiol. 2003;41(9):1438-1444.
8. Anand IS.
Heart failure and anemia: mechanisms and patho-physiology.
Heart Fail Rev. 2008;13(4):379-386.
9. Dzau V, Antman EM, Black HR, et al.
The cardiovascular continuum validated: clinical evi-dence of improved patient outcomes: part 1 Pathophysi-ology and clinical trial evidence (risk factors throughstable coronary disease).
Circulation. 2006;114(25):2850-2870.
10. National Kidney Foundation. K/DOQUIclinical practice guidelines for chronic kidneydisease: evaluation.
Classification and stratification.
Am J Kidney Dis. 2002;39(suppl 2):S1-S246.
REFERENCES
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 247

he need for a deepening and more solid basis for collaboration and cooperation
between cardiologists and nephrologists has never been more important than
it is now. So many of the patients seen by cardiologists have chronic kidney
disease (CKD) (made easier to spot now using estimated glomerular filtration
rate [eGFR measurements])—manifest by reduced kidney function, and, when tested
for, by albuminuria-proteinuria. Patients with reduced GFR and albuminuria-proteinuria
are at an especially high cardiovascular risk. Luis M. Ruilope in this journal edition
makes that point forcefully. Moreover, so many of the pharmacological interventions
used by cardiologists—diuretics, renin-angiotensin-aldosterone system (RAAS)
blockers to name but two—have an impact on kidney function (and often plasma
potassium, too).
Looking at the situation the other way around, from the nephrological perspective,
so many of our CKD stage 3a and 3b patients (GFR 45-60 and 30-44 mL/min/1.73 m2
respectively) have co-incident cardiovascular disease burdens, usually, but not exclu-
sively, in the form of abnormal endothelial function, macrovascular atherosclerosis,
arterial stiffness, and left ventricular hypertrophy. The major cause of death in CKD
stage 3a and 3b is cardiovascular, and it is a much rarer outcome to progress to CKD
stage 4 and beyond.
How to reduce the toll of cardiovascular disease in this numerically quite large
cohort—perhaps 4% to 6% of the population, so numerous as say diabetes—is still
a challenge, though strict blood pressure control and lipid-lowering therapy seem
sensible, rational, and safe interventions for either or both of the kidney and the
cardiovascular system.
248
David Goldsmith, MA, MB, BChir, FRCP(UK), FRCP (Edin), FASN, FERAReader in Renal Medicine - King’s College London - UK
Invited Editorial
T
•••
THE CARDIORENAL SYNDROME AS THE NEPHROLOGIST SEES IT
See page 243 for the companion Invited Editorial by Henry J. Dargie:THE CARDIORENAL SYNDROME AS THE THE CARDIOLOGIST SEES IT
Dr David Goldsmith, MB, BChir, Renal and Transplantation Department, 6th Floor, Borough Wing, Guy’s Hospital, Great MazePond, London SE1 9RT, UK ([email protected])
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 248

249
In this exciting and well-written journal issue, guest-edited by the Brothers Kalra, there
is much to savor. The excellent critical analysis by Paul R. Kalra and Philip A. Kalra of
the oversimplistic and nonbiologically plausible Ronco classification of the “cardiorenal
syndrome” is long overdue. Although simplification can be, and often is, a boon and a
blessing, where the simplification leads to confusion or conflation of ideas, it stands
in the way of a deeper understanding. There is a major opportunity, likely to be taken
by many, to examine these complex, shifting, and often subtle cardiorenal interrela-
tionships using large cohorts, with nested detailed investigational and interventional
substudies, testing out novel biomarkers to help predict patients more or less likely to
reach a cardiovascular rather than a renal end point.
The pressing need for common research and investigational goals and studies is clear
for all to see now. This can be done by colocalizing good quality clinical care with
cutting-edge research projects, so that all can benefit from the latest thoughts, ideas,
and therapies, and more rapid progress can be made. In the UK, the establishment of
national research networks has driven a major increase in recruitment of subjects to
clinical trials, and in time, this will be a rich harvest.
The exciting issue of anemia and iron deficiency in heart failure is well tackled by
Ewa A. Jankowska and Piotr Ponikovski. In nephrology, we have long used iron, oral
or intravenous, as a means to augment or stimulate hemopoiesis as anemia is so
commonly associated with our chronically comorbidly challenged CKD patients. The
short-term safety and effects of iron on the bone marrow are well known, but the
longer-term safety of this approach is much less robustly understood, as iron could
theoretically help, by improving mitochondrial function, or hinder, by stoking oxidative
stress (a major player in more advanced CKD). The use of IV iron in heart failure is
now a major new theme, and many heart failure specialists are taking this up enthusi-
astically. I would strongly advocate doing as many trials as possible until it is abun-
dantly clear this is both safe and a good health-economic intervention. In nephrology,
over 25 years or more, we have learnt now a bitter lesson about accepting the “good”
that an expensive intervention can bring—erythropoietin—but not seeing the harm
(thrombosis, hypertension, possible acceleration of cancer) that can also dictate
patient outcomes.
Blood pressure control, and RAAS blockade, of course, remain central to the nephrol-
ogists’ interventional strategy to try to stem the tide of patients suffering cardiac or
renal diseases, which often progress remorselessly without treatment. Luis M. Ruilope
expertly chronicles this complex area, and its links with sympathetic nervous system
overactivity, highlighting important observations and trials to guide therapy with more
logic and precision.
•••
•••
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 249

Sudden cardiac death is of course not confined to CKD patients, but the death rates
from this are higher in dialysis patients than in any other patient cohort except those
with congenital/genetic reasons for arrhythmia. Not only is this a common problem,
but it is also currently seriously deficient in good quality research—we don’t even
know the balance between asystole and ventricular fibrillation, and the predisposing
factors and early-warning signs for either. The article by Robert N. Foley and Charles
A. Herzog elegantly lays bare the worrying lack of key information and knowledge,
while sensibly marshaling the evidence for intervention (small though it is). This is an
area where electrophysiologists and nephrologists could really potentially make a big
difference.
Let us hope that on reading this stimulating series of articles, both nephrologists and
cardiologists will feel more collaborative, more cooperative, and more ready to com-
promise and share the management of a complex and challenging patient group. We in
nephrology need commitment and help from the cardiology specialty as never before,
as we cannot pretend any longer to be able to do the job alone. We in nephrology
would venture to suggest back that we have quite a lot to offer the other way around!
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Invited Editorials - The Cardiologist, by Dargie / The Nephrologist, by Goldsmith
250
•••
DCVM 62 contents+Editorial:DCVM N°48, contents+Editorial 23/03/12 11:26 Page 250

251
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomesPaul R. Kalra*, MD, FRCP; Philip A. Kalra†, MD, FRCP*Department of Cardiology - Portsmouth Hospitals NHS Trust - Porstmouth - UK †Department of Nephrology - Salford Royal Foundation NHS Trust - Salford - UK
The cardiorenal syndrome is a broad term used todescribe the association of heart failure and renalimpairment. A recent classification has sought toseparate different clinical presentations, but the underlying pathophysiological causes are not readilydifferentiated in this way. Patients developing thecardiorenal syndrome are at major risk of mortalityand morbidity due to multiple and complex interac-tions. There is now growing interest in the role ofanemia in worsening outcome. Standard medicaltherapy, such as �-blockers and renin-angiotensinblocking agents, are effective, but underused in pa-tients with heart failure and renal impairment, andother standard therapies such as high-dose diureticspotentially have nephrotoxic effects; the response todiuretic therapy is also blunted in the presence of renal dysfunction. Emerging therapies such as peri-toneal dialysis and hemofiltration have potential toimprove the outcome of hemodynamically unstablepatients with severe cardiorenal disease. As is the casein all areas of medicine, preventative strategies areof paramount importance, and therapies that helpprevent development of cardiovascular complications inpatients with chronic kidney disease and, conversely,strategies that allow successful treatment of acute orchronic heart failure without exacerbation of renaldysfunction, are awaited.
There is a complex anatomical and physiologicalinterplay between the heart and the kidney, withthe optimal functioning of either organ systembeing interdependent upon the other. When
organ function is disordered by disease this is greatlyemphasized. We have known for several decades thatpatients with chronic kidney disease (CKD) are atconsiderably increased risk of cardiovascular disease,and that the majority of patients with advanced CKDeventually die early, and from a cardiac death. Morerecently, there has been a clear recognition that in pa-tients with cardiac disease, intercurrent renal impair-
Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
Keywords: anemia; cardiorenal syndrome; chronic kidney disease; heartfailure; neurohormonal activationAddress for correspondence: Dr Paul R. Kalra, Department ofCardiology, Portsmouth Hospitals NHS Trust, Queen Alexandra Hospital,Southwick Hill Road, Cosham, Portsmouth PO6 3LY, UK ([email protected]); Professor Philip A. Kalra, Department ofNephrology, Salford Royal Foundation NHS Trust, Stott Lane, Salford M68HD, UK (e-mail: [email protected])Dialogues Cardiovasc Med. 2011;16:251-263
SELECTED ABBREVIATIONS AND ACRONYMS
AKI acute kidney injury
ARVD atherosclerotic renovascular disease
CAD coronary artery disease
CHF chronic heart failure
CKD chronic kidney disease
CRS cardiorenal syndrome
eGFR estimated glomerular filtration rate
ESA erythropoietin-stimulating agent
ESCAPE Effect of Strict blood pressure Control and ACE-inhibition on ProgrEssion of chronicrenal failure in pediatric patients
ESRD end-stage renal disease
GFR glomerular filtration rate
HOPE Heart Outcomes Prevention Evaluation
LVH left ventricular hypertrophy
LVMI left ventricular mass index
POSH Prospective Outcomes Study in Heart failure
RAAS renin-angiotensin-aldosterone system
SCD sudden cardiac death
WRF worsening renal function
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 251

ment has a major adverse effect upon outcome. Thisis now well established in the two preeminent cardiacconditions that cause disease in the Western world.Patients with coronary artery disease (CAD) fare worsewhen impaired glomerular filtration rate (GFR) is evi-dent, and the latter has a significant negative effectupon outcomes in those undergoing coronary revascu-larization procedures. Likewise, those patients withheart failure, whether acutely decompensated or chron-ic, have particularly bad outcomes if renal impairmentis either already present or if it supervenes during thecourse of treatment.
In this article we will be concentrating on the relation-ship between heart failure and renal dysfunction, acommonly occurring association described under theumbrella heading of “cardiorenal syndrome” (CRS). Wewill consider the definition/classification, epidemiology,pathogenesis, and outcomes of the condition, and alsothe currently available treatments to improve the prog-nosis of these high-risk patients. Specific and topicalaspects of the CRS, namely anemia, sudden cardiacdeath, and optimal pharmacotherapeutic management,will then be considered in more detail by our interna-tionally renowned contributors.
DEFINITION AND CLASSIFICATION OFTHE CARDIORENAL SYNDROME
A number of terms to address the coexistence of heartfailure and renal dysfunction have been proposed.CRS is now generally favored. Historically, this termhas typically been used to describe declining renalfunction in the setting of advanced or decompensatedheart failure.1,2 It has also been used to describe themore specific development of acute kidney injury (AKI)in response to heart failure treatment that then leadsto diuretic resistance, fluid overload, and worseningheart failure.3
In an attempt to differentiate between acute andchronic interactions and identify the “primary” drivingpathophysiological abnormality, Ronco and colleagueshave proposed a classification based around five typesof the CRS (Table I).4 Worsening or decompensatedheart failure as a cause or effect of AKI constitutestypes 1 and 3, respectively. Chronic heart failure (CHF)as a cause and effect of CKD is suggested as types 2and 4, respectively. Type 5 is classed as cardiovascularand renal damage from a common underlying pathol-ogy; acutely, this might be sepsis, whereas chronically,diabetes mellitus, atherosclerosis, and/or hyperten-sion are more likely. There are limitations to this clas-sification, particularly since the precise pathophysio-logical relationships in the different clinical scenariosare not fully (and often poorly) understood (see be-low). Furthermore, each type of CRS is more likely tooccur in the presence of another. For example, AKI ismore likely in a patient with decompensated heart fail-ure if the patient has underlying diabetes (underlyingsystemic condition) with associated CKD and CAD. Inaddition, it is plausible that a patient with CHF, forexample, will exhibit pathophysiological changes typ-ical of distinct subgroups at different stages of theirheart failure syndrome. While the precise mechanismsare not fully understood, it is apparent that dysfunc-tion of one organ system may cause or exacerbate dys-function of the other, and a spiral of decline can occur,with resultant adverse prognosis.
A brief mention of the definition of AKI is worthwhile.This term has now replaced “worsening renal failure"(this of course will be encountered in historic publica-tions), although debate around the precise definitioncontinues. While some (“RIFLE classification” = Risk;Injury; Failure; Loss of kidney function; End-stage kid-ney disease) have proposed an increase in serum cre-atinine of at least 50% from baseline (which may ofcourse not be known),5 many studies of heart failure
252
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
CRS Type Title Description
Type 1 Acute cardiorenal syndrome Rapid worsening of cardiac function leadingto acute kidney injury
Type II Chronic cardiorenal syndrome Chronic abnormalities of cardiac function leading to progressive CKD
Type III Acute renocardiac syndrome Acute and primary worsening of kidney
function leading to cardiac dysfunction
Type IV Chronic renocardiac syndrome Chronic and primary renal disease (CKD) leading to CHF
Type V Secondary cardiorenal syndrome Systemic conditions causing simultaneous cardiac and renal dysfunction, eg, sepsis
Table I. The 5 proposedsubtypes of the cardiore-nal syndrome (CRS).
Abbreviations: CHF, chronicheart failure, CKD, chronickidney disease; CRS, cardio-renal syndrome. Adapted from reference 4:Ronco et al. J Am CollCardiol. 2008;52:1527-1539.American College ofCardiology Foundation.
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 252

populations have used the “AKIN” (Acute Kidney InjuryNetwork) definition.6 In this report, AKI was suggestedas reflecting an abrupt (within 48 hours) reduction inkidney function manifest by:• An increase in serum creatinine �26.4 μmol/L (0.3mg/dL), or• An increase in serum creatinine of �50% (1.5-foldfrom baseline), or • Oliguria (< 0.5 mL/kg per hour for more than 6hours).
Formula for conversion of serum creatinine unitsSerum creatinine: 1 mg/dL = 88.4 μmol/L
EPIDEMIOLOGY OF CARDIORENAL SYNDROME
Although the previously described classification of theCRS may be an oversimplification of what is often amore complex pathophysiological interaction betweenthese two important and interdependent organ sys-tems, it does help in defining the clinical situations inwhich patients are at risk and enables a logical sepa-ration which aids further discussion. Acute decom-pensated heart failure complicated by AKI has a verypoor outcome, but even minor rises of creati-nine (eg, <10 μmol/L) have been shown to pro-long hospitalization and increase mortality in these patients.7 In a study of over 1000 pa-tients hospitalized for decompensated heartfailure, 25% had a rise in serum creatinine of>26.5 μmol/L (which fulfills the definition forAKI), with increased risk of this in those withdiabetes, hypertension, or prior CKD.8 Thisfinding is consistent across a number of stud-ies, with the development of AKI being associ-ated with worse outcomes not only in hospi-tal, but over the next 6 to 12 months as well.9
A recent meta-analysis of studies in patientswith heart failure (n=18 634) showed thataround 25% patients exhibited an increase inserum creatinine �0.2 mg/dL (>18 µmol/L) ora decrease in estimated glomerular filtrationrate (eGFR) �5 mL/min/1.73 m2; when present,this was associated with a higher risk for mor-tality (odds ratio [OR], 1.62; 95% confidenceinterval [CI], 1.45-1.82; P<0.001) and hospital-ization (OR, 1.30; 95% CI, 1.04-1.62; P=0.022).10
Additional associations of AKI in this situationare anemia, age, and the use of renin-angioten-sin blocking agents and diuretics, these latterdrugs presumably further reducing renal perfu-sion in patients with low cardiac output states.
Insight into the prevalence of CKD in patients withacute cardiac decompensation is provided by the AcuteDecompensated Heart Failure National Registry (AD-HERE), a database which includes over 100 000 pa-tients—one analysis showed that 64% of patients hadat least moderate CKD (<60 mL/min/1.73 m2) and only9% had normal eGFR.11 The epidemiology of renal im-pairment in patients with CHF is less clear becausemuch of the available data are derived from clinicaltrials or studies that have tended to exclude patientswith more advanced CKD. Age is strongly associatedwith both CHF and CKD and so it is no surprise thatthe majority of elderly patients with heart failure willhave some degree of CKD. A prospective cohort studyof all-comers to one heart failure clinic found that about80% had an abnormal creatinine clearance (previouslyused as a surrogate for eGFR, but having even greaterlimitations).12 Overall, over 50% of patients with CHFhave evidence of stages 3 to 5 CKD (GFR <60 mL/min),and increasing mortality is seen with reducing GFRwhen the latter is analyzed as a covariate.13 The degreeof renal impairment as estimated by serum creatinineis also associated with adverse prognosis (Figure 1).14
Indeed, advanced CKD is as prognostically important asleft ventricular systolic dysfunction in this population.12
253
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
60
50
40
30
20
10
0
80 100 120 140 160 180
Baseline serum creatinine (μmol/L)
Annual m
ort
ality
1.0 1.2 1.4 1.6 1.8 2.0Baseline serum creatinine (mg/dL)
Figure 1. Studies with patients with heart failure published during the period1985-2008 (including registries, clinical trials, and observational cohort studies).These include patients with acute as well as chronic heart failure and those with leftventricular dysfunction after myocardial infarction. The size of circles is proportionalto the study size. The solid line represents the fitted regression line, weighted for studysize. Dashed lines represent the 95% confidence intervals.
Adapted from reference 14: Damman et al. J Ren Care. 2010;36(suppl 1):18-26. © 2010, John Wiley & Sons, Inc.
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 253

254
So what about the reverse association, cardiac dys-function complicating acute or chronic kidney disease?The incidence of severe AKI varies between 50 and1000 cases/million/year, depending upon age group-ing15; 9% of all hospital admissions have AKI, and thelatter is found in 35% of all intensive care unit admis-sions. Fluid overload, which can be life-threatening ifleft untreated, frequently complicates AKI. Its mecha-nism is multifactorial and includes oliguria, cardiacdysfunction due to neurohormonal abnormalities, cap-illary leak syndrome due to multisystem illness (espe-cially sepsis), and hypoalbuminemia. Surprisingly,there is a paucity of data regarding the true incidenceof this “acute renocardiac failure,” and even less relat-ing to systematic study of structural and functionalcardiac changes occurring both during the episode andin the recovery period.
In patients with CKD, a plethora of interrelated car-diovascular risk factors exist, and some of these un-doubtedly contribute to the development of CHF.These will be considered more extensively in the sec-tion on pathophysiology, but nonetheless some areworthy of mention here. Structural myocardial disease,termed by some as “uremic cardiomyopathy,16” is im-portant and the prevalence of left ventricular hyper-trophy (LVH) increases with declining GFR,17 and itscause is both multifactorial and complex. LVH is asso-ciated with hypertension (present in >70% of patientswith stage 4 CKD and >90% of dialysis patients), vita-min D deficiency,18 volume status, anemia, and in-creased arterial stiffness, and the latter in turn is re-lated to endothelial dysfunction and medial vascularcalcification,19 which are now the subject of much re-search. When patients reach end-stage renal disease(ESRD), defined as eGFR <15 mL/min, up to threequarters of those starting renal replacement therapy(RRT) will have echocardiographic evidence of LVH;36% already have left ventricular dilatation, and 15%severe left ventricular (LV) dysfunction.20,21 In a Cana-dian cohort of 259 patients followed from dialysis in-ception, serial echocardiography showed that 70% hadan increase in LV mass index (LVMI) and 50% an in-crease in LV cavity volume compared with baseline,after the patients had been followed for a mean of 41months. A new diagnosis of heart failure was morelikely in those with greatest LVMI; 33% of patientshad CHF at the end of the study, and new onset CHFaccounted for half of the cases. The importance of hy-pertension was emphasized as each 10 mm Hg rise inmean arterial pressure predicted a 44% increased riskof de novo heart failure.22 The incidence of new-onsetheart failure in patients with earlier stage (ie, before
dialysis) CKD has not been well evaluated. Althoughthe risk of this association is accentuated by the patho-physiological factors described above, which may pro-gressively worsen as eGFR falls, it is also likely thatmany affected patients will have concomitant coronaryartery disease and/or diabetes. However, it is wellknown that LVH develops early in CKD; in a study of175 consecutive patients attending a predialysis clinic,LVMI increased as creatinine clearance fell and LVHwas independently associated with age and systolichypertension.17
Underpinning all of the cardiorenal associations de-scribed above is the fact that many common conditionscan lead to both cardiovascular and renal complicationsin parallel. Classic examples are diabetes and hyper-tension; diabetes is the primary disease in at least20% of UK patients with ESRD,23 and over 30% of pa-tients receiving dialysis are diabetic. The figures areconsiderably greater in the US, with around 60% ofthe dialysis population having diabetes.24 These pa-tients have a very high prevalence (>70%) of cardiacabnormalities, including coronary artery disease andheart failure. The association of hypertension with LVHand heart failure in ESRD has already been mentionedabove.
PATHOPHYSIOLOGY OF THE CARDIORENAL SYNDROME
CHF is characterized by the inability of the heart topreserve cardiac output. The net result is a reductionin perfusion to key peripheral organs. Typical symp-toms of dyspnea, peripheral edema, and weight gaintogether with the classic physical signs such as jugularvenous distension, rales, and edema relate in part tothe inability of the body to excrete sodium and sec-ondary water. While this excessive salt and water reten-tion is related to decreased GFR, it is vital to under-stand why GFR is reduced in CHF.
Cardiovascular and renal disease may both occur as a consequence of the same underlying disease. In addition, the presence of CKD is an independent riskfactor for developing cardiovascular disease, particu-larly CAD and LVH. Epidemiological studies suggestthat CAD is responsible for more than half of incidentcases of heart failure.25 Furthermore, arterial diseaseis a major cause of renal disease. As such, teasing outthe precise pathophysiology of the CRS is complex andfraught with difficulty. We will now briefly discuss someof the putative pathways and mechanisms involved(Figure 2).26
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 254

255
Hemodynamic abnormalities
Historically, the reduction in GFR in CHF was thoughtto be mainly attributable to a decrease in renal bloodflow.27 Circulatory integrity (preservation of mean ar-terial pressure) is the main determinant of renal sodi-um and water excretion.28,29 A reduction in cardiacoutput results in a series of systemic and intrarenalresponses that aim to retain fluid and restore cardiacoutput at an increased circulatory volume. With a fur-ther drop in cardiac output, renal blood flow becomesimpaired, which activates a number of complex re-sponses that further decrease renal function, but failto normalize cardiac output.30 A recent cross-section-al study that determined GFR and renal blood flow byradiolabeled tracer techniques in patients with CHFreceiving blockers of the renin-angiotensin-aldosterone
system (RAAS) has consolidated this belief.31 Block-ade of the RAAS is the cornerstone of evidence-basedheart failure management. However, drug-induced re-duction in renal perfusion may have a deleterious effectupon renal function under certain circumstances as aconsequence of actions on glomerular hemodynamics(these are beneficial when perfusion is preserved).
Yet, hypotension is not present in all patients whodevelop AKI. There is increasing interest in the relation-ship between renal venous congestion and associatedrenal dysfunction and AKI.14 Damman et al32 haveshown in a large cohort of patients with cardiovasculardisease that elevated higher central venous pressurewas associated with lower eGFR independent of car-diac output. Furthermore, a substudy of the ESCAPEtrial (Effect of Strict blood pressure Control and ACE-
inhibition on ProgrEssion of chronicrenal failure in pediatric patients)demonstrated that the single (inva-sively determined) parameter asso-ciated with reduced renal functionwas right atrial pressure.33
Common underlying disease
Hypertension and LVHElevated blood pressure is extremelycommon in patients with CKD andis associated with a high rate of denovo cardiac failure and CAD. Evenmodest elevations in blood pres-sure are associated with LVH andcardiomyopathy. Optimal control ofhypertension appears to be funda-mental to patients with either CKDor cardiovascular disease. However,in ESRD, mortality is strongly asso-ciated with low blood pressure.22
Advanced heart failure will often leadto a low blood pressure irrespectiveof renal function. As such, the useof antihypertensive therapy will needto be reevaluated in patients whodevelop heart failure.
AtherosclerosisAtherosclerosis is a multisystem dis-ease. Underlying CAD is the mostcommon cause of heart failure,25 andaround 40% of patients with CKDhave evidence of CAD.34 The pres-ence of CKD appears to be a proath-
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
Substrate for sudden cardiac death
Chronic activationof RAAS
Arterialhypoperfusion
Venous congestion
CKDand/or
AKI
Impairedcardiac function
(LVSD, LVH)
Anemia
Sharedetiological
risk factors,eg,
HypertensionAtherosclerosis
SmokingDiabetes
High cholesterol
Figure 2. Basic schematic overview of the pathophysiological abnormalities contributingto the cardiorenal syndrome (CRS). Shared etiological risk factors (in particular hypertension), at least in part, contribute to abnormalitiesin both cardiac and renal function. An abnormality of function in either organ system adversely impactson the other. As a consequence of cardiac dysfunction (as seen in chronic heart failure) a reductionin cardiac output results in reduced renal blood flow; associated venous congestion further impairsrenal function, leading to AKI and progression of CKD. A complex series of responses occur; the netresult is sodium and water retention and vasoconstriction mediated by neurohormonal activation.There is increasing interest in the adverse impact of anemia. Other factors such as inflammatory im-mune activation and abnormal calcium/phosphate metabolism result in endothelial dysfunction andarterial stiffness and are also implicated in disease progression. The figure is an oversimplification,since many of the abnormalities found impact on other pathways incriminated in disease progres-sion—for example, activation of the RAAS will impact on inflammatory immune activation andanemia (and vice versa). Resultant abnormalities of left ventricular function and structure form thesubstrate for sudden cardiac death.
Abbreviations: AKI, acute kidney injury; CKD, chronic kidney disease; LVH, left ventricular hyper-trophy; LVSD, left ventricular systolic dysfunction; RAAS, renin-angiotensin-aldosterone system. Adapted from reference 26: Zachariah et al. J Ren Care. 2009;35(1):2-10. © 2009, John Wiley& Sons, Inc.
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 255

256
erosclerotic condition and atherosclerosis itself canlead to and/or exacerbate CKD as a consequence ofmicrovascular damage. Traditional risk factors for ath-erosclerosis such as smoking are associated with thedevelopment and progression of cardiovascular diseaseand CKD. When present, it is thought that pathophys-iological abnormalities associated with CKD can ex-acerbate the atherosclerotic process (see below).
Diabetes mellitus and the metabolic syndromeDiabetes is a common comorbidity in patients withCHF and CKD. It is often encountered in conjunctionwith other established vascular risk factors in the meta-bolic syndrome (coexistent obesity, hypertension, hightriglycerides, and low-density lipoprotein (LDL) cho-
lesterol, and high circulating levels of prothrombotic/proinflammatory markers); this in part explains whythe presence of diabetes is associated with such a highcardiorenal morbidity and mortality.
Diabetic nephropathy accounts for around 20% of newdialysis cases in the UK23 and 40% in the US.35 Endo-thelial dysfunction secondary to insulin resistance andchronic hyperglycemia leads onto the development ofmacrovascular disease (CAD and CKD). Microvasculardisease and early endothelial disruption in the kidneysresults in albuminuria. The presence of even microal-buminuria (urine albumin-to-creatinine ratio of 30-299mg/g), an early marker of endothelial dysfunction, isassociated with a marked increased risk of progressionto established diabetic nephropathy.36 A large meta-analysis has confirmed that microalbuminuria is an
independent predictor of all-cause mortality and ad-verse cardiovascular outcomes.37 There appears to bean amplified risk when considering the presence of in-creasing degrees of microalbuminuria and deterioratingrenal function. The HOPE (Heart Outcomes PreventionEvaluation) trial showed that the presence of microal-buminuria was associated with an adjusted threefoldrelative risk of hospitalization for heart failure, whichwas similar for patients with and without diabetes.38
Neurohormonal activation
Activation of the RAAS is a protective physiologicalmechanism that attempts to prevent underperfusionof vital organs such as the kidney.39 While acutely this
may help preserve central aorticpressure, continued activation (asseen in CHF) leads to excess sodi-um and water retention and vaso-constriction with resultant adversehemodynamic effects such as leftventricular dilatation and increasedafterload. Angiotensin II and aldo-sterone also exert direct unfavorableeffects on the kidney (intraglomeru-lar hypertension and intrarenal fi-brosis) and heart (myocardial cellu-lar hypertrophy, progressive loss ofmyocardial function with myocytehypertrophy and interstitial fibro-sis) (Figure 3).
The neurohumoral hallmark of bothpatients with CKD or CHF is chronicoveractivation of the RAAS, and thissystem appears to play a prominent
pathophysiological role in worsening renal and car-diac function.40 Angiotensin II and aldosterone alsostimulate proinflammatory cytokines which may con-tribute to endothelial dysfunction, cardiac and renaldisease. (See in this issue the paper by Luis M. Ruilope:“What is the optimal pharmacotherapeutic approach tothe cardiorenal syndrome?”—page 277).
Inflammation
Inflammatory immune activation is found in patientswith CKD and/or CHF, and it is believed this contributesto disease progression. In CHF, inflammatory cytokinessuch as tumor necrosis factor and interleukin 6 areindependent predictors of adverse outcome.41 This isparticularly apparent in advanced or decompensatedheart failure; disordered gut wall function (eg, second-
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
Heartfailure
RAASactivation
Fibrosisand vaso-
constriction
Reduced renal
blood flow
Intrarenalhypertensionand scarring
Cardiacfibrosis and
LVH
CKD
Figure 3. Simplified schematic diagram showing the central role of RAAS activation inthe pathogenesis of the cardiorenal syndrome in patients with heart failure and CKD.Abbreviations: CKD, chronic kidney disease; RAAS, renin-angiotensin-aldosterone system.
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 256

257
ary to edema from elevated right atrial pressure) mayfacilitate translocation of bacterial endotoxin (lipo-polysaccharide), which in turn is a potent stimulus forinflammatory cytokine activation.
Renal disease as a cause of cardiovascular disease
Not only do patients with CKD exhibit an excess oftraditional vascular disease risk factors, but vascularcalcification and associated arterial stiffness are common and associated with excess mortality.42 Thepathophysiology of calcification is complex and islinked to hyperphosphatemia, hypercalcemia, hyper-parathyroidism, and a reduction in endogenous in-hibitors of calcification (eg, fetuin A). The net result isan increase in vascular stiffness, which is associatedwith LVH and may predispose to heart failure. Endothe-lial dysfunction, with an associated loss of endotheli-um-mediated vasodilatory response to nitric oxide(NO), is common in patients with CHF and linked tocardiovascular mortality. Activation of RAAS furtherexacerbates endothelial dysfunction. CKD is a majorcontributor to endothelial dysfunction, which in partrelates to circulating proinflammatory cytokines.43
Anemia
Patients with CHF commonly have low hemoglobin as a comorbid finding; when present it is an importantdeterminant of impaired exercise capacity44 and mor-tality.45 Silverberg et al highlighted its pathophysio-logical importance in patients with both CHF and CKD,introducing the term “cardio-renal-anemia syndrome.”46
The etiology of anemia in CHF is complex and not fullyunderstood. However, absolute and functional irondeficiency appears to be extremely common.47 Bluntederythropoietin production has also been demonstrat-ed. As such, there is much interest in the potentialuse of iron and erythropoietin-stimulating agents (ESA)in this area.
The use of intravenous iron and ESA has become anintegral part of the management of patients with ESRD.The need for large-scale studies assessing both effica-cy and safety prior to routine clinical use in patientswith CHF has been exemplified by a number of recentstudies of ESA in patients with CKD.48 Understandingwho might benefit, which therapy to use, and appro-priate targets (hemoglobin and iron parameters) isfundamental. (See in this issue the paper by Ewa A.Jankowska and Piotr Ponikowski: “Should anemia beactively treated in cardiorenal syndrome?”—page 284).
Atherosclerotic renovascular disease
Atherosclerotic renovascular disease (ARVD) is com-mon, and it is frequently seen in association with cardiovascular diseases. ARVD (here defined as renalartery stenosis >50%) is present in around one thirdof elderly patients presenting to hospital with heartfailure49 and just over 50% of outpatient cohorts withCHF.50 Heart failure is present in around two fifths ofelderly patients with ARVD and is associated with excessmortality when present (almost threefold).51 Renalrevascularization therapy may provide substantial clin-ical benefit, but this needs to be evaluated further.52
The above description of the interactions between theheart, kidneys, neurohormonal, immune, and othersystems represents a simplification; numerous inter-actions between systems occur via intricate feedbackloops.3 As such, a number of interrelating factors maycontribute to CRS and it is highly likely that for anyone patient a number of mechanisms may be at play.
Outcomes of patients with the cardiorenal syndrome
The presence or subsequent development of renalimpairment in patients with acute or chronic cardiacfailure confers an increased risk of adverse outcome.In acute decompensated heart failure, the degree ofincrease in creatinine appears to be of greater prog-nostic significance than the baseline value.53 In POSH(Prospective Outcomes Study in Heart failure), AKI wastermed “worsening renal function” (WRF—as with oth-er studies a 26.5 μmol/L or greater rise in creatinine).WRF was more likely to occur with a higher serumcreatinine value on admission (OR, 3.02) and in thosewith pulmonary edema (OR, 3.35). The presence of WRFincreased average length of hospital stay by 2 days, butin this study it did not influence readmission ratesand mortality.54 Interestingly, analysis of the ESCAPEtrial has shown that even an improvement in renalfunction is as poor an adverse prognostic marker asWRF in patients with decompensated heart failure.55
A suggested explanation for this counterintuitive find-ing is that patients who manifest altered renal functionhave more advanced disease than those who remainstable during the decompensation. The heterogeneouspathophysiology of acute heart failure must be of im-portance here, and its influence can be seen by thevariable response of patients to diuretic therapy. It iswell known that some patients manifest a deteriora-tion in renal function, presumed secondary to poor
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 257

258
renal perfusion, following diuretic-induced decrease incardiac filling pressure and cardiac output. However,some patients respond to diuretics with an increase inGFR, possibly achieved by an off-loading of intra-ab-dominal and renal venous pressure. Other patientshave no change in renal function, and these patientsmay have cardiac physiology that manifests the flatpart of the Starling curve, where changes in LV end-diastolic pressure have little effect upon cardiac out-put. An alteration in hemodynamics must play a centralrole in the above changes in renal function in acuteheart failure56 and this is emphasized by the improve-ments in GFR seen in patients treated with ventricularassist devices or cardiac resynchronization therapy.57
In CHF, the presence of renal impairment has a majordetrimental impact upon survival, and this has beenextensively studied. In a meta-analysis of 16 studiesthat included >80 000 patients with CHF, the annualmortality was 24% in patients with normal renal func-tion, 38% in those with mild renal impairment (GFR =53-89 mL/min) and 51% in the presence of moderateimpairment (defined here as GFR <53 mL/min).12 Theincreased risk of mortality was quantified as 15% forevery 10 mL/min decline in GFR. In the CHARM pro-gram (Candesartan in Heart failure–Assessment ofmoRtality and Morbidity), all-cause mortality risk was2.92 times greater for patients with GFR <45 mL/mincompared with those with GFR >75 mL/min, and thiswas independent of LV ejection fraction.58
Conversely, cardiovascular disease accounts for over50% of deaths in patients with CKD. Studies from theUS Medicare system highlight the accentuation of riskbrought about by various combinations of CKD (not atESRD), heart failure, and anemia according to claimsdata.59 In a 5% annual random cohort from the Medi-care database that included over 1.3 million subjectsaged >65 years, the annual mortality for patients withno history of anemia, CKD, or heart failure was 4%,for patients with CKD it was 8%, and for patients withall 3 comorbidities, 23% (Table II).59 As GFR declinesin CKD, mortality rises; in dialysis populations, the an-nual mortality risk is around 20%. Data from the UnitedStates Renal Data System indicate that cardiomyopa-thy, congestive heart failure, or pulmonary edema arethe predominant causes of mortality in dialysis patients,with a rate of 11.4 events per 1000 patient-years,60
which equates to around 6% of all deaths. One of themain mechanisms of death that occurs in patients withcardiac failure, and particularly those with ESRD treat-ed by dialysis, is sudden death, thought to be provokedby bradyarrhythmia or tachyarrhythmia—“sudden car-
diac death” (SCD).61 This is now an area of increasingresearch in dialysis patients, as up to 25% of all deathsare attributed to SCD. Although SCD will be coveredin one of the three reviews that follow this article, (seein this issue the paper by Robert N. Foley and Charles A.Herzog: “How can we reduce sudden cardiac death incardio-renal syndrome?”—page 267), it is worth empha-sizing the comparative epidemiology—SCD in the dial-ysis population occurs at 70 times the rate of that inthe general population.62 Predisposing factors includethe cardiac structural factors already discussed, myo-cardial changes (eg, myocardial stunning) that occurduring the dialysis procedure,63 as well as fluxes inelectrolytes and water balance that are prone to de-velop around the time of a hemodialysis session.
THE CLINICAL MANAGEMENT OF CARDIORENAL SYNDROME:
HOW CAN WE OPTIMIZE OUTCOMES?
When considering the clinical management of the CRS,we find limitations when trying to separate diseasestates according to the classification. As there is a com-plex interrelationship between the organ systems,some therapies are applicable to most or all clinicalpresentations. Hence, hypertension control is a genericrequirement and blockade of the RAAS would be con-sidered routine in all patients with acute and chronicheart failure. It is also applicable to the majority ofpatients with CKD with the aim of controlling hyper-tension, ameliorating proteinuria, slowing progressiveloss of renal function, and reducing cardiovascular risk.The treatment of anemia with intravenous iron and/orerythropoiesis-stimulating agents (ESA) has been em-bedded as a core part of CKD management for many
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
Risk factor Hazard ratio
No anemia, CHF, or CKD 1.00
Anemia only 1.60
CKD only 1.64
CHF only 2.25
CHF and CKD 3.30
Anemia, CHF, and CKD 3.63
Table II. Relative annual mortality figures for patients who havehad inpatient hospital visits relating to anemia, CKD, and heartfailure. The baseline annual mortality for patients with no history of anemia, CKDor heart failure is 4%.
Abbreviations: CHF, congestive heart failure; CKD, chronic kidney disease.Adapted from reference 59: Herzog et al. J Card Fail. 2004;10(6):467-472. © 2004, Elsevier Inc.
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 258

259
years, despite a rather limited evidence base, and it is now gaining a lot of attention in cardiology, partic-ularly in heart failure treatment. Further discussion ofthis topic is merited and is covered in the already citedreview by Ewa A. Jankowska and Piotr Ponikowski inthis issue.
Class 3 CRS, when acute pulmonary edema compli-cates AKI, is seen very frequently in oliguric AKI fromany cause and its management usually involves acutehemofiltration during dialytic therapy, which is outsidethe scope of this account. However, there are less com-mon, but specific, related clinical scenarios that areworthy of mention, one being flash pulmonary edemaassociated with severe renal artery stenosis. This ac-counts for around 5% of renovascular presentationsand refers to acute heart failure occurring in the ab-sence of significant myocardial ischemic injury; despitethe absence of randomized trial evidence, there is adefinite consensus that this presentation should betreated with renal revascularization therapy,64 which isnow via percutaneous intervention in 99% of cases.65
Limiting the development of cardiovascular complica-tions in patients with CKD is a fundamental tenet ofmanagement in renal clinics, with hypertension control,renin-angiotensin blockade, lipid management, ane-mia correction, and reduction of vascular calcificationrisk being central. This is a huge topic and detaileddiscussion falls outside the scope of this review. Theremainder of this section will provide a brief overviewof therapies available for patients primarily presentingwith heart failure, and having class 1 or 2 CRS.
Medical therapy
Blockade of the RAAS axis in the cardiorenal syndromeis covered by Luis M. Ruilope in this issue (cited above)and will not be discussed here. β-Blockade improvessurvival in patients with stage 3 CKD, CAD and heartfailure (OR 0.75),66 whereas dialysis patients with heartfailure also benefit, one study showing a 2-year all-cause mortality of 52% with carvedilol compared with73% for placebo.67 Preemptive treatment with a β-block-er can also reduce the likelihood of developing de novoheart failure.68 However, as is the case with most med-ical therapies in heart failure, there is underutilization inpatients with CKD compared with those without renalimpairment, despite absence of any adverse evidence.
The historic core of medical therapy for heart failureinvolves diuretics, but nephrotoxicity and decline inrenal function accompanying their use can cause a
therapeutic dilemma. Those patients with decompen-sated heart failure and either associated AKI or under-lying CKD are more prone to suffer further AKI due todiuretic drugs. Consequently, renin-angiotensin block-ers are often discontinued during an acute admissionbecause of AKI or hyperkalemia, but they should bereintroduced when the acute risk has passed. Patientswith AKI or CKD are less responsive to diuretics thanpatients with preserved renal function. Higher-dosediuretic therapy correlates with poor outcome in heartfailure, presumably because diuretic resistance reflectsmore severe CRS and more fragile hemodynamic sta-tus. Nesiritide, a B-type natriuretic peptide analog, doesnot reduce the need for diuretic or increase urine out-put in acute heart failure.69 Nitrates and hydralazineare useful alternatives to blockade of the RAAS whenheart failure exacerbations are complicated by AKI, al-though hypotension may preclude their use. If nitratesare unable to stabilize a patient with severe heart fail-ure who has AKI and diuretic resistance, the treatmentoptions are then rather limited, at which point mechan-ical ultrafiltration may need to be considered.
Inotropic agents were once often used for treating se-vere decompensated heart failure, but this practice hasnow fallen from favor. For decades, low-dose dopaminehas been used to encourage a diuresis in AKI basedupon the knowledge that a response of specific intra-renal receptors resulted in an increase in renal bloodflow (without significant inotropic effect), but in normalphysiological conditions. Some physicians still usedopamine with the belief that it improves diuretic re-sponsiveness and reduces the incidence and progres-sion of AKI,70 but sound evidence of benefit is lacking.
Dialysis and hemofiltration for cardiorenal syndrome
Off-loading the heart in type 1 CRS by rapid removalof fluid with either dialysis or hemofiltration is an in-teresting development that has been used sporadicallyin the past, but which is now undergoing more robustscientific evaluation. Hemofiltration is the ultrafiltra-tion of fluid via an extracorporeal machine, and hasadvantages over diuretic therapy in that rapid fluid andsodium removal can be achieved in the early phase ofan admission with decompensated heart failure, min-imizing the chance of deteriorating renal function orhypotension that frequently accompanies high-dosediuretic therapy. The hemofiltration process can becontrolled and can thus be beneficial for very unstablepatients who have labile blood pressure responses dur-ing treatment. Acute hemodialysis would be far more
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 259

risky in these unstable patients. Studies have shownshort-term benefits with hemofiltration compared withintravenous diuretics in acute admissions with heartfailure,71 but evidence regarding longer term outcomeis needed. The logistics and safety of inserting a peri-toneal dialysis catheter in an acutely unwell patientlimit the applicability of peritoneal dialysis for themanagement of acute heart failure. However, the pos-sibility of using peritoneal dialysis for refractory chronicheart failure in patients with and without advancedCKD is now gaining support. One small study of 17 pa-tients started on peritoneal dialysis for refractory heartfailure showed that it improved 1-year survival and re-sulted in fewer hospital admissions.72 Trials are nowbeing developed to assess the efficacy of the therapyin a more robust manner.
When considering chronic dialytic therapies for ESRD,there has been a trend toward offering peritonealdialysis rather than hemodialysis to patients with coexistent heart failure. This has been based on anassumption that patients with markedly impairedventricular function will benefit from gradual fluid removal and so be less likely to suffer hypotensivecollapse and/or serious arrhythmias that might resultfrom hemodialysis. The evidence to support this prac-tice is conflicting.
SUMMARY
Patients who develop the cardiorenal syndrome are atmajor risk of morbidity and mortality due to multipleand complex pathophysiological interactions. Standardmedical therapy, such as β-blockers and renin-angio-tensin blocking agents, is effective, but underused, inpatients with heart failure and renal impairment. Man-agement of heart failure in the setting of acute or CKDis made difficult by the potentially nephrotoxic effectof, or resistance to, standard therapies such as highdose-diuretics. Peritoneal dialysis and hemofiltrationare measures that may yet improve the outcome ofhemodynamically unstable patients with severe car-diorenal disease. As is the case with most areas ofmedicine, prevention is better than cure, and optimaltherapies that help prevent development of left ventric-ular dysfunction and other cardiovascular complica-tions in patients with CKD, and conversely, strategiesthat allow successful treatment of acute or chronicheart failure without exacerbation of renal dysfunction,are eagerly awaited.
REFERENCES
1. Francis G.
Acute decompensated heart failure: the cardiorenal syndrome.
Cleve Clin J Med. 2006;73(suppl 2):S8-S13.
2. Ronco C, House AA, Haapio M.
Cardiorenal syndrome: refining the definition of a complex symbiosisgone wrong.
Intensive Care Med. 2008;34(5):957-962.
3. Geisberg C, Butler J.
Addressing the challenges of cardiorenal syndrome.
Cleve Clin J Med. 2006;77(5):485-491.
4. Ronco C, Haapio M, Horoncouse AA, Anavekar N,Bellomo R.
Cardiorenal syndrome.
J Am Coll Cardiol. 2008;52:1527-1539.
5. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P;ADQI Workgroup.
Acute renal failure—definition, outcome measures, animal models,fluid therapy and information technology needs. The second inter-national consensus conference of Acute Dialysis Quality Initiative(ADQI) Group.
Crit Care. 2004;8:R204-R212.
6. Mehta RL, Kellum JA, Shah SV, et al; Acute KidneyInjury Network.
Acute Kidney Injury Network: report of an initiative to improveoutcomes in acute kidney injury.
Crit Care. 2007;11(2):R31.
7. Gottlieb S.
The prognostic importance of different definitions of worsening renalfunction in congestive heart failure.
J Card Fail. 2002;8(3):136-141.
8. Forman DE, Butler J, Wang Y, et al.
Incidence, predictors at admission, and impact of worsening renalfunction among patients hospitalized with heart failure.
J Am Coll Cardiol. 2004;43(1):61-67.
9. Borman NL, Kalra PA, Kalra PR.
Acute kidney injury in patients with decompensated heart failure.
Br J Hosp Med (Lond). 2010;71(5):269-275.
10. Damman K, Navis G, Voors AA, et al.
Worsening renal function and prognosis in heart failure: systematicreview and meta-analysis.
J Card Fail. 2007;13:599-608.
260
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 260

11. Heywood JT, Fonarow GC, Costanzo MR, Mathur VS,Wigneswaran JR, Wynne J; ADHERE Scientific AdvisoryCommittee and Investigators.
High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heartfailure: a report from the ADHERE database.
J Card Fail. 2007;13(6):422-430.
12. McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW.
Renal insufficiency and heart failure: prognostic and therapeuticimplications from a prospective cohort study.
Circulation. 2004;109(8):1004-1009.
13. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C.
Chronic kidney disease and the risks of death, cardiovascularevents, and hospitalization.
New Engl J Med. 2004;351(13):1296-1305.
14. Damman K, Kalra PR, Hillege H.
Pathophysiological mechanisms contributing to renal dysfunctionin chronic heart failure.
J Ren Care. 2010;36(suppl 1):18-26.
15. Chertow GM, Burdick E, Honour M, Bonventre JV,Bates DW.
Acute kidney injury, mortality, length of stay, and costs in hospital-ized patients.
J Am Soc Nephrol. 2005;16:3365-3370.
16. Mark PB, Johnston N, Groenning BA, et al.
Redefinition of uremic cardiomyopathy by contrast-enhanced cardiacmagnetic resonance imaging.
Kidney Int. 2006;69(10):1839-1845.
17. Levin A, Singer J, Thompson C, Ross H, Lewis M.
Prevalent left ventricular hypertrophy in the predialysis population:Identifying opportunities for intervention.
Am J Kidney Dis. 1996;27(3):347-354.
18. Nitta K, Akiba T, Uchida K, et al.
Left ventricular hypertrophy is associated with arterial stiffnessand vascular calcification in hemodialysis patients.
Hypertens Res. 2004;27(1):47-52.
19. London GM, Guérin AP, Marchais SJ, Métivier F,Pannier B, Adda H.
Arterial media calcification in end-stage renal disease: impact onall-cause and cardiovascular mortality.
Nephrol Dial Transplant. 2003;18(9):1731-1740.
20. Foley RN, Parfrey PS, Harnett JD, Kent GM.
The prognostic importance of left ventricular geometry in uremiccardiomyopathy.
J Am Coll Cardiol. 1995;5(12):2024-2031.
21. Parfrey PS, Foley RN.
The clinical epidemiology of cardiac disease in chronic renal failure.
J Am Soc Nephrol. 1999;(7):1606-1615.
22. Foley RN, Parfrey PS, Harnett JD, Kent GM, MurrayDC, Barrett PE.
Impact of hypertension on cardiomyopathy, morbidity and mortalityin end-stage renal disease.
Kidney Int. 1996;49(5):1379-1385.
23. Farrington K, Hodsman A, Casula A, Ansell D,Feehally J.
Chapter 4: ESRD prevalent rates in 2007 in the UK: national andcentre-specific analyses.
In: UK Renal Registry 11th Annual Report. 2007:43-68.
24. Foley RN, Collins AJ.
End stage renal disease in the United States: an update from theUnited States Renal Data System.
J Am Soc Nephrol. 2007;18:2644-2648.
25. Fox KF, Cowie MR, Wood DA, et al.
Coronary artery disease as the cause of incident heart failure inthe population.
Heart. 2001:22(3);228-236.
26. Zachariah D, Kalra PA, Kalra PR.
Optimal management of chronic heart failure in patients withchronic kidney disease.
J Ren Care. 2009;35(1):2-10.
27. Ljungman S, Laragh JH, Cody RJ.
Role of the kidney in congestive heart-failure—relationship ofcardiac index to kidney-function.
Drugs. 1990;39:10-21.
28. Schrier RW, Abraham WT.
Hormones and haemodynamics in heart failure.
N Engl J Med. 1999;341(8): 577-585.
29. Zannad F, Adamopoulos C, Mebazaa A,Gheorghiade M.
The challenge of acute decompensated heart failure.
Heart Fail Rev. 2006;11:135-139.
30. Stevenson LW, Nohria A, Mielniczuk L.
Torrent or torment from the tubules? Challenge of the cardiorenalconnections.
J Am Coll Cardiol. 2005;45(12):2004-2007.
31. Smilde TDJ, Damman K, van der Harst P, et al.
Differential associations between renal function and “modifiable”risk factors in patients with chronic heart failure.
Clin Res Cardiol. 2009;98:121-129.
261
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 261

32. Damman K, van Deursen VM, Navis G, et al.
Increased central venous pressure is associated with impaired renalfunction and mortality in a broad spectrum of patients with car-diovascular disease.
J Am Coll Cardiol. 2009;53:582-588.
33. Nohria A, Hasselblad V, Stebbins A, et al.
Cardiorenal interactions: insights from the ESCAPE trial.
J Am Coll Cardiol. 2008;51:1268-1274.
34. Stack AG, Bloembergen WE.
Prevalence and clinical correlates of coronary artery disease amongnew dialysis patients in the United States: a cross-sectional study.
J Am Soc Nephrol. 2001;12(7):1516-1523.
35. Ritz E, Rychlík I, Locatelli F, Halimi S.
End-stage renal failure in type 2 diabetes: a medical catastropheof worldwide dimensions.
Am J Kidney Dis. 1999;34(5):795-808.
36. Nelson RG, Knowler WC, Pettitt DJ, Saad MF,Charles MA, Bennett PH.
Assessment of risk of overt nephropathy in diabetic patients fromalbumin excretion in untimed urine specimen.
Arch Intern Med. 1991;151(9):1761-1765.
37. Chronic Kidney Disease Prognosis Consortium;Matsushita K, van der Velde M, Astor BC, et al.
Association of estimated glomerular filtration rate and albuminuriawith all-cause and cardiovascular mortality in general populationcohorts: a collaborative meta-analysis.
Lancet. 2010;375(9731):2073-2081.
38. Gerstein HC, Mann J, Yi Q, et al.
Albuminuria and risk of cardiovascular events, death, and heartfailure in diabetic and nondiabetic individuals.
JAMA. 2001;286(4):421-426.
39. Bongartz LG, Cramer MJ, Doevendans PA, Joles JA,Braam B.
The severe cardiorenal syndrome: “Guyton revisited.”
Eur Heart J. 2005;26(1):11-17.
40. Anker SD, Sharma R.
The syndrome of cardiac cachexia.
Int J Cardiol. 2002;85:51-66.
41. Niebauer J, Volk HD, Kemp M, et al.
Endotoxin and immune activation in chronic heart failure: a prospective cohort study.
Lancet. 1999;353(9167):1838-1842.
42. Wang M, Tsai W, Chen J, Cheng M, Huang J.
Arterial stiffness correlated with cardiac remodelling in patientswith chronic kidney disease.
Nephrology. 2007;12(6):591-597.
43. Tripepi G, Mallamaci F, Zoccali C.
Inflammation markers, adhesion molecules, and all-cause andcardiovascular mortality in patients with ESRD: searching for thebest risk marker by multivariate modeling.
J Am Soc Nephrol. 2005;16:s83-s88.
44. Kalra PR, Bolger AP, Francis DP, et al.
Effect of anemia on exercise tolerance in chronic heart failure in men.
Am J Cardiol. 2003;91:888-891.
45. Groenveld HF, Januzzi JL, Damman K, et al.
Anemia and mortality in heart failure patients a systematic reviewand meta-analysis.
J Am Coll Cardiol. 2008;52:818-827.
46. Silverberg DS, Wexler D, Blum M, Iaina A.
The cardio renal anemia syndrome: correcting anemia in patientswith resistant congestive heart failure can improve both cardiacand renal function and reduce hospitalizations.
Clin Nephrol. 2003;60(suppl 1):S93-S102.
47. Opasich C, Cazzola M, Scelsi L, et al.
Blunted erythropoietin production and defective iron supply forerythropoiesis as major causes of anaemia in patients with chronicheart failure.
Eur Heart J. 2005;26:2232-2237.
48. Pfeffer MA, Burdmann EA, Chen CY, et al; TREATInvestigators.
A trial of darbepoetin alfa in type 2 diabetes and chronic kidneydisease.
N Engl J Med. 2009;361:2019-2032.
49. MacDowall P, Kalra PA, O'Donoghue DJ, Waldek S,Mamtora H, Brown K.
Risk of morbidity from renovascular disease in elderly patientswith congestive cardiac failure.
Lancet. 1998; 352(9121):13-16.
50. de Silva R, Loh H, Rigby AS, et al.
Epidemiology, associated factors, and prognostic outcomes of renalartery stenosis in chronic heart failure assessed by magnetic reso-nance angiography.
Am J Cardiol. 2007;100(2):273-279.
51. Kalra PA, Guo H, Kausz AT, Gilbertson DT, Liu J,Chen S, et al.
Atherosclerotic renovascular disease in United States patients aged67 years or older: risk factors, revascularization, and prognosis.
Kidney Int. 2005; 68(1):293-301.
52. Kane GC, Xu N, Mistrik E, Roubicek T, Stanson AW,Garovic VD.
Renal artery revascularization improves heart failure control in patients with atherosclerotic renal artery stenosis.
Nephrol Dial Transplant. 2010;25(3):813-820.
262
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 262

263
53. Smith GL, Vaccarino V, Kosiborod M, et al.
Worsening renal function: what is a clinically meaningful changein creatinine during hospitalization with heart failure?
J Card Fail. 2003;9(1):13-25.
54. Cowie MR, Komajda M, Murray-Thomas T,Underwood J, Ticho B.
Prevalence and impact of worsening renal function in patients hos-pitalized with decompensated heart failure: results of the prospectiveoutcomes study in heart failure (POSH).
Eur Heart J. 2006;27(10):1216-1222.
55. Testani JM, McCauley BD, Kimmel SE, Shannon RP.
Characteristics of patients with improvement or worsening in renalfunction during treatment of acute decompensated heart failure.
Am J Cardiol. 2010;106(12):1763-1769.
56. Stampfer M, Epstein SE, Beiser GD, Braunwald E.
Hemodynamic effects of diuresis at rest and during intense uprightexercise in patients with impaired cardiac function.
Circulation. 1968;37(6):900-911.
57. Adelstein EC, Shalaby A, Saba S.
Response to cardiac resynchronization therapy in patients withheart failure and renal insufficiency.
Pacing Clin Electrophysiol. 2010;33(7):850-859.
58. Hillege HL, Nitsch D, Pfeffer MA, et al.
Candesartan in Heart Failure: Assessment of Reduction in Mortalityand Morbidity (CHARM) Investigators Renal function as a predictorof outcome in a broad spectrum of patients with heart failure.
Circulation. 2006;113:671-678.
59. Herzog C, Muster H, Li S, Collins A.
Impact of congestive heart failure, chronic kidney disease, andanemia on survival in the Medicare population.
J Card Fail. 2004;10(6):467-472.
60. No authors listed.
Section H—Mortality and causes of death.
In: USRDS 2008 Annual Data Report. 2008:619-670.
61. Green D, Roberts PR, New DI, Kalra PA.
Sudden cardiac death in hemodialysis patients: an in-depth review.
Am J Kidney Dis. 2011;57(6):921-929.
62. Rich A.
Morbidity and mortality.
In: USRDS 2008 Annual Data Report. National Institute ofHealth, National Institute of Diabetes and Digestive and RenalDiseases. 2008:129-146.
63. McIntyre CW.
Effects of hemodialysis on cardiac function.
Kidney Int. 2009;76(4):371-375.
64. Hirsch AT, Haskal ZJ, Hertzer NR, et al.
ACC/AHA 2005 guidelines for the management of patients withperipheral arterial disease (lower extremity, renal, mesenteric, andabdominal aortic): executive summary a collaborative report fromthe American Association for Vascular Surgery/Society for VascularSurgery, Society for Cardiovascular Angiography and Interventions,Society for Vascular Medicine and Biology, Society of InterventionalRadiology, and the ACC/AHA Task Force on Practice Guidelines(Writing Committee to Develop Guidelines for the Management ofPatients With Peripheral Arterial Disease).
J Am Coll Cardiol. 2006;47(6):1239-1312.
65. Kalra PA, Guo H, Gildertson DT, et al.
Atherosclerotic renovascular disease in the United States.
Kidney Int. 2010;77:37-43.
66. Ezekowitz J, McAlister FA, Humphries KH, et al.
The association among renal insufficiency, pharmacotherapy, andoutcomes in 6,427 patients with heart failure and coronary arterydisease.
J Am Coll Cardiol. 2004;44(8):1587-1592.
67. Cice G, Ferrara L, D'Andrea A, D’Isa S.
Carvedilol increases two-year survival in dialysis patients with dilated cardiomyopathy—a prospective, placebo-controlled trial.
J Am Coll Cardiol. 2003;43:1438-1444.
68. Abbott K, Trespalacios F, Agodoa L, Taylor A, Bakris G.
Beta-blocker use in long-term dialysis patients.
Arch Intern Med. 2004;164:2465-2471.
69. Dhar S, Pressman GS, Subramanian S, et al.
Natriuretic peptides and heart failure in the patient with chronickidney disease: a review of current evidence.
Postgrad Med J. 2009;85(1004):299-302.
70. Elkayam U, Ng TM, Hatamizadeh P, Janmohamed M,Mehra A.
Renal vasodilatory action of dopamine in patients with heart failure:magnitude of effect and site of action.
Circulation. 2008;117(2):200-205.
71. Bart BA, Boyle A, Bank AJ, et al.
Ultrafiltration versus usual care for hospitalized patients with heartfailure: the Relief for Acutely Fluid-Overloaded Patients WithDecompensated Congestive Heart Failure (RAPID-CHF) trial.
J Am Coll Cardiol. 2005;46(11):2043-2046.
72. Sánchez J, Ortega T, Rodríguez C, et al.
Efficacy of peritoneal ultrafiltration in the treatment of refractorycongestive heart failure.
Nephrol Dial Transplant. 2010;25(2):605-661.
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Cardiorenal syndrome: epidemiology, pathogenesis, and outcomes - Kalra and Kalra
DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 263

DCVM 62 Lead article:Mise en page 1 23/03/12 11:27 Page 264

265
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome?
E. A. Jankowska, P. Ponikowski
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome?
L. M. Ruilope
Expert Answers to Three Key Questions
How can we reduce sudden cardiac death in cardiorenal syndrome?
R. N. Foley, C. A. Herzog
1
2
3
Cardiorenal Syndrome
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:28 Page 265

DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:28 Page 266

theromatous coronary artery disease is a verycommon condition in latter-day dialysis popu-
lations. In the early days of mainte-nance dialysis, when clinically overtcoronary artery disease was a strictexclusion criterion for an extremelyscarce therapy, it soon became clearthat cardiovascular event rates wereorders of magnitude beyond expec-tations. A pivotal paper was pub-lished in 1974 describing the clini-cal experience of 39 patients whoreceived long-term hemodialysis in Seattle since 1960, with over 6.5years of treatment per patient.1
Mortality rates were unexpectedlyhigh for a population starting dialy-sis therapy with an average age of37 years: 23 deaths were observedand “14 of 23 deaths could be attrib-uted to arteriosclerotic complica-tions, myocardial infarction beingresponsible for 8, strokes for 3, andrefractory congestive heart failurefor 3 deaths.” By today’s standards,autopsies were performed in a high-ly impressive 91% of cases. Howev-er, as the study was retrospective,pathological criteria for assigningcause of death were not systemati-
cally applied, and it was telling thatthe terms “arteriosclerosis” and“atherosclerosis” appear to havebeen used interchangeably in thestudy report. Ultimately, the title ofthis study “Accelerated Atherosclerosisin Prolonged Maintenance Hemodial-ysis” became an accepted patho-genetic concept in the end-stagerenal disease community, one thatresonates to this day.
Laying aside the still unsubstanti-ated hypothesis of accelerated atherosclerosis, there is somethingdifferent about the uremic heart.For example, there is convincingexperimental evidence that uremialeads to pathological cardiac hyper-trophy, fibrosis, diastolic dysfunc-tion, vascular and valvular calcifica-tion, and arterial stiffening.2-7 Evenhemodialysis patients with pristinecoronary arteries are continuouslyexposed to varying conditions ofcardiac preload, afterload, ion flux-es, as well as repetitive myocardialischemia and localized ventricularstunning from hemodialysis.8 Indialysis patients, while the relativeproportions of atherosclerotic andnonatherosclerotic arteriosclerosis
A
267Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
How can we reduce sudden cardiac death in cardiorenal syndrome? Robert N. Foley, MB, FRCPC; Charles A. Herzog, MD
Chronic Disease Research Group - and Department of Medicine - University of Minnesota - Minneapolis - Minn - USA
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
SELECTED STUDY ACRONYMS
CAPRICORN CArvedilol Post infaRction survIval COntRol in left ventricular dysfunctioN
COPERNICUS CarvedilOl ProspEctive RaNdomIzed, CUmulative Survival
HEMO Hemodialysis Study
MADIT-II Multicenter Automatic Defibrillator Implantation Trial–II
Keywords: β-blocker; cardiovascular event;chronic kidney disease; hemodialysis; dysrhythmia; implanted cardiac defibrillator;prevention; risk factor/marker; sudden cardiac deathAddress for correspondence:Robert N. Foley, MB, Chronic DiseaseResearch Group, 914 South 8th Street,Suite S-406, Minneapolis, MN 55404, USA(e-mail: [email protected])Dialogues Cardiovasc Med. 2011;16:267-276
While sudden cardiac death ratesare inordinately high in advancedchronic kidney disease, evidence-based prevention algorithms arelacking. This article examines thedifficulties of case definition inobservational studies of intrinsi-cally unhealthy populations, asso-ciations between event rates anddeclining kidney function, poten-tially modifiable risk markers,and the lack of evidence-basedtherapies. On the basis of highevent rates, trials in the generalpopulation, and temporal patternsof event rates in dialysis patients,we argue that definitive trials ofimplanted cardioverter defibrilla-tors, �-blockers, and more fre-quent hemodialysis need urgentconsideration.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:28 Page 267

are usually unknown, there seemslittle doubt that patients enter intostates of end-stage renal diseasewith disproportionately high bur-dens of clinically meaningful ather-osclerotic vascular disease. Finally,while autonomic neuropathy is aclassic feature of the untreated state,treated end-stage renal disease hasbeen more recently characterizedas a state of sympathetic nervoussystem overdrive.9
EPIDEMIOLOGY OF SUDDEN CARDIACDEATH IN END-STAGE
RENAL DISEASE
Event rates in dialysis patients
Some basic epidemiological obser-vations suggest that cardiovasculardisease event profiles are “different”in dialysis patients. For example,when reimbursement claims wereexamined in US dialysis patients,claims for cardiac failure, peripheralvascular disease, and sudden cardiacdeath far outstripped those for typ-ical coronary heart disease.10
Sudden cardiac death is often de-fined as unexpected death withinone hour of the onset of symptoms,or an unwitnessed, unexpecteddeath without obvious noncardiaccause in a patient who was known tobe well within the past 24 hours.11
If one assumes that well individu-als don’t usually reside in hospital,this definition requires nonhospi-talization for functionality in obser-vational studies. This proviso pos-es challenges in dialysis patients,given that they typically have highburdens of comorbidity, spend asubstantial amount of time in med-ical institutions, their deaths areusually unobserved, and precisetiming of death may be impossibleto determine. In addition, multiplecardiac and multiple noncardiac
causes of death may be applicablein a given situation. Fashion andusage issues may also be important:for example, in situations wheredeath is unwitnessed, sudden car-diac death may be a label of conven-ience in situations of indeterminatetiming and causation.
Regarding attribution of cause ofdeath, this is believed to be highlyinaccurate in dialysis populations,especially in the current era whereautopsy is rare. For example, in thewell-known Hemodialysis (HEMO)Study, cause of death on the stan-dard (in US patients) Death Notifi-cation Form (Form 2746) and deathclassified by the HEMO Study ad-judication committee were in pooragreement. Using the HEMO Studydesignation as gold standard, sen-sitivity values for cause of deathfrom the Death Notification Formwere 9% for congestive heart failure,38% for ischemic heart disease, and39% for dysrhythmias and conduc-tion disorders.12 To date, few if anystudies have attempted to quantifythe ability of predictor variables todiscriminate sudden cardiac deathfrom other deaths. If, as seems like-ly, one cannot reliably discriminatecardiac from noncardiac death, theepidemiological foundations ofsudden cardiac death may be un-sound. If these arguments turn outto be valid, it is a truism that theassociations of sudden cardiac arethe same as for all-cause mortality,and vice versa.
Another neglected issue concernsthe requirement for not being inhospital for case definition. Withusual case definitions, admittingall patients to hospital indefinitelywould completely eradicate the“disease,” at least in observationalstudies. In classic epidemiology,disease events can only be countedwhen they occur during a periodwhen subjects are considered to be
at risk. If one accepts this argument,it seems reasonable to propose thatcalculation of sudden cardiac deathrates should account for periods oftime in hospital in the calculationof the total time at risk. To date,these niceties have often been ig-nored and interim hospitalizationshave usually been ignored in thecalculation of exposure time. Someof these important theoretical issuesare illustrated in Figure 1. As a pre-amble, two basic types of analysisare considered. With typical survivalanalysis (such as Cox regression), allfollow-up ends at the first instantsubjects are not at risk, whether ornot they become at risk again in thefuture; returning to our scenario, ifsudden cardiac death is predicatedon occurrence outside of a hospi-talization, follow-up ends at thefirst hospitalization. In a scenario ofa period outside hospital, followedby a period in hospital, followed bya period outside hospital, only theinformation from the first of thesetime periods is used. With typicalrate-based analysis (such as Poissonregression), the first and third peri-ods would also contribute outcomeinformation. In Figure 1, cases Aand B are never hospitalized, andcontribute identical event rates andfollow-up time per person, and theissue of ignoring follow-up time ismoot; there is one sudden cardiacdeath (as the event occurred out-side hospital). Case C terminateswith a cardiac death and D exitsalive; as the cardiac death occurredin hospital neither case is classi-fied as a sudden cardiac death; thefollow-up time, however, dependson whether interim hospitalizationtime is considered (in which casethe denominator for calculation ofrates is 1 unit of time) or ignored(in which case the denominator is3 units of time). In case E, depend-ing on the analytic technique therate of sudden cardiac death is 1/3,0/1 or 1 /2; in case F, three answers
268
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:28 Page 268
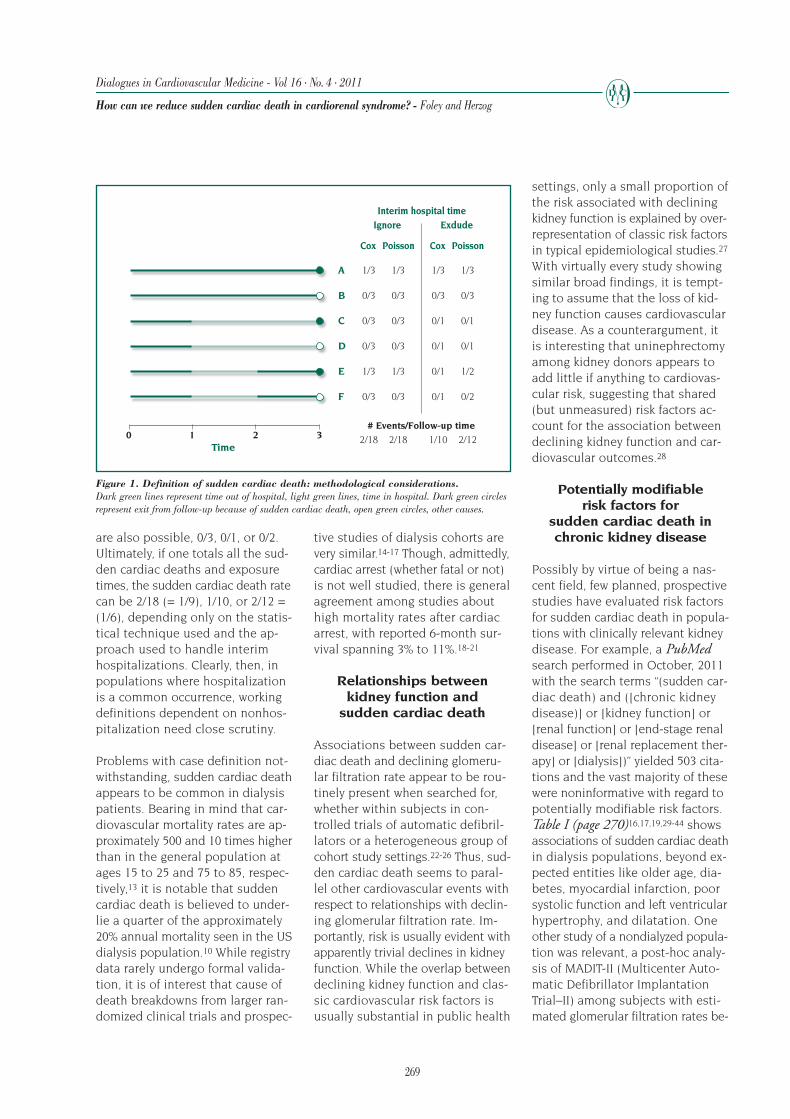
are also possible, 0/3, 0/1, or 0/2.Ultimately, if one totals all the sud-den cardiac deaths and exposuretimes, the sudden cardiac death ratecan be 2/18 (= 1/9), 1/10, or 2/12 =(1/6), depending only on the statis-tical technique used and the ap-proach used to handle interim hospitalizations. Clearly, then, inpopulations where hospitalizationis a common occurrence, workingdefinitions dependent on nonhos-pitalization need close scrutiny.
Problems with case definition not-withstanding, sudden cardiac deathappears to be common in dialysispatients. Bearing in mind that car-diovascular mortality rates are ap-proximately 500 and 10 times higherthan in the general population atages 15 to 25 and 75 to 85, respec-tively,13 it is notable that suddencardiac death is believed to under-lie a quarter of the approximately20% annual mortality seen in the USdialysis population.10 While registrydata rarely undergo formal valida-tion, it is of interest that cause ofdeath breakdowns from larger ran-domized clinical trials and prospec-
tive studies of dialysis cohorts arevery similar.14-17 Though, admittedly,cardiac arrest (whether fatal or not)is not well studied, there is generalagreement among studies abouthigh mortality rates after cardiacarrest, with reported 6-month sur-vival spanning 3% to 11%.18-21
Relationships between kidney function and
sudden cardiac death
Associations between sudden car-diac death and declining glomeru-lar filtration rate appear to be rou-tinely present when searched for,whether within subjects in con-trolled trials of automatic defibril-lators or a heterogeneous group ofcohort study settings.22-26 Thus, sud-den cardiac death seems to paral-lel other cardiovascular events withrespect to relationships with declin-ing glomerular filtration rate. Im-portantly, risk is usually evident withapparently trivial declines in kidneyfunction. While the overlap betweendeclining kidney function and clas-sic cardiovascular risk factors isusually substantial in public health
settings, only a small proportion ofthe risk associated with decliningkidney function is explained by over-representation of classic risk factorsin typical epidemiological studies.27
With virtually every study showingsimilar broad findings, it is tempt-ing to assume that the loss of kid-ney function causes cardiovasculardisease. As a counterargument, itis interesting that uninephrectomyamong kidney donors appears toadd little if anything to cardiovas-cular risk, suggesting that shared(but unmeasured) risk factors ac-count for the association betweendeclining kidney function and car-diovascular outcomes.28
Potentially modifiable risk factors for
sudden cardiac death in chronic kidney disease
Possibly by virtue of being a nas-cent field, few planned, prospectivestudies have evaluated risk factorsfor sudden cardiac death in popula-tions with clinically relevant kidneydisease. For example, a PubMedsearch performed in October, 2011with the search terms “(sudden car-diac death) and ([chronic kidneydisease)] or [kidney function] or[renal function] or [end-stage renaldisease] or [renal replacement ther-apy] or [dialysis])” yielded 503 cita-tions and the vast majority of thesewere noninformative with regard topotentially modifiable risk factors.Table I (page 270)16,17,19,29-44 showsassociations of sudden cardiac deathin dialysis populations, beyond ex-pected entities like older age, dia-betes, myocardial infarction, poorsystolic function and left ventricularhypertrophy, and dilatation. Oneother study of a nondialyzed popula-tion was relevant, a post-hoc analy-sis of MADIT-II (Multicenter Auto-matic Defibrillator ImplantationTrial–II) among subjects with esti-mated glomerular filtration rates be-
269
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
0 21 3# Events/Follow-up time
Time
Cox Poisson
A
B
C
D
E
F
1/3
0/3
0/3
0/3
1/3
0/3
1/3
0/3
0/3
0/3
1/3
0/3
Cox Poisson
IgnoreInterim hospital time
Exdude
1/3
0/3
0/1
0/1
0/1
0/1
1/3
0/3
0/1
0/1
1/2
0/2
2/18 2/18 1/10 2/12
Figure 1. Definition of sudden cardiac death: methodological considerations. Dark green lines represent time out of hospital, light green lines, time in hospital. Dark green circlesrepresent exit from follow-up because of sudden cardiac death, open green circles, other causes.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:28 Page 269

low 75 mL/min/1.73 m2 in patientsrandomly assigned to conventionalmedical therapy.45 Multivariate asso-ciations of sudden cardiac death inthe subgroup with lower glomerularfiltration rates included higher rest-ing heart rate, low diastolic bloodpressure, prolonged QRS duration,and nontreatment with a β-blocker.
Factors relating to delivery of dialy-sis are prominent in Table I. He-modialysis is usually delivered threetimes weekly, with two 1-day inter-vals and one 2-day interval betweendialysis sessions. As end-stage renaldisease severely limits the capacityto tolerate volume and potassium-related deviations from normality,
the 2-day interdialytic interval haslong been a source of concern.46
Two clinical trials of daily hemodial-ysis—demonstrating beneficial ef-fects on intermediate outcome likeleft ventricular mass and quality oflife—have reignited interest in theissues of timing and frequency ofhemodialysis session delivery.47,48
270
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
Design*
Comments Prospective Retrospective Case control
Related to HD Procedure
Interval between HD 29, 30
Low potassium dialysate 19, 31
Low calcium dialysate 31
High HD ultrafiltration 31
Catheter for HD 19
Electrocardiographic
Absence of sinus rhythm HD patients with diabetes, 32RCT of atorvastatin or placebo
Increased heart rate Holter monitoring 33
QT interval 34
Impaired baroreflex sensitivity Electrocardiogram and beat-to- 35beat BP recorded continuously
QT dispersion 36
Sympathetic hyperactivity Holter-based beat-to-beat variability 37
Blood levels
Predialysis K 30
Glycosylated hemoglobin HD with diabetes, RCT of atorvastatin 38
Vitamin D defiency HD with diabetes, RCT of atorvastatin 39
Copeptin Hypothesized as a surrogate for 40arginine-vasopressin. HD with diabetes, RCT of atorvastatin
Ca-P product 41
C-reactive protein HD with diabetes, RCT of atorvastatin 16, 30, 42,
Low serum albumin 16
Interleukin-6 16
Predialysis creatinine 31
P-selectin 43
Low urinary output 44
High systolic BP 17
Low diastolic BP 17
N-terminal pro-BNP 17
Table I. Associations of sudden death in dialysis populations. *Numbers are citation references.
Abbreviations: BNP, brain natriuretic peptide; BP, blood pressure; Ca, calcium; HD, hemodialysis; K, potassium; P, phosphorus; RCT, randomized con-trolled trial.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 270

To date, the observational studiesexamining the associations of thelong interdialytic interval have con-centrated on sudden cardiac deathand cardiac arrest. The landmarkstudy of Bleyer et al examined 7-day patterns of sudden death andcardiac death in US hemodialysispatients between 1977 and 1997.Sudden death and cardiac deathwere approximately 40% more like-ly than expected on Mondays andTuesdays.29 The same group exam-ined the timing of sudden death in hemodialysis patients in a retro-spective study including 228 patientdeaths, 35% of which were consid-ered to be “sudden.” The risk ofdeath increased by a factor of 1.7during the 12-hour period startingwith the dialysis procedure and bya factor of 3 in the 12-hour periodat the end of the long interdyaliticinterval.49 Another group examined400 cardiac arrests occurring indialysis units affiliated with a largedialysis chain, between 1998 and1999. The observed cardiac arrestrate was equivalent to 1.1 per 100person-years and cardiac arrest wasmuch more likely on Mondays; casefatality rates were 60% within 48hours following cardiac arrest.19
We have recently reexamined theclose-to-universal paradigm of threetimes weekly schedules in a nation-ally representative sample of US pa-tients receiving hemodialysis at theend of calendar years 2004 through2007, followed for 2.2 years.50 Ad-verse event rates were noticeablyhigher on the day after the 2-dayinterdialytic interval than on otherdays: all-cause mortality, 23% (high-er); mortality from cardiac causes,36%; mortality from cardiac arrest,30%; admissions for any cardiovas-cular event, 124% higher and admis-sions for dysrhythmia, 90% higherthan at other times during the dial-ysis week. When examined by daysof the dialysis week, adverse events
followed a downward-tilted saw-tooth pattern with the followingcharacteristics: highest rates on thedialysis day following the long in-terdialytic interval; higher rates on dialysis days than on ensuingnondialysis days; higher rates earlyin the week than later (Figure 2).50
Finally, when examined by subgroup,the finding of heightened risk afterthe long interval appeared to be aclose-to-universal phenomenon.
With most observational studies,one looks at a single outcome indifferent segments of the popula-tion. When differences are found, itis impossible to refute the argumentthat unmeasured differences in thepopulation segments are responsi-ble for differences in study out-comes. A different argument needsto be invoked when examining out-comes on different days of the week:thus, identical populations are be-ing considered when outcomes on
271
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
25
20
15
10
5
0HD1 HD1+1 HD2 HD2+1 HD3 HD3+1 HD3+2
Day of week
Annualized mortality rateAAll causes
Rate
per
100 p
ers
on-y
ear
Cardiac causesInfectious causesVascular causes
50
45
40
35
30
25
20
15
10
5
0HD1 HD1+1 HD2 HD2+1 HD3 HD3+1 HD3+2
Day of week
Annualized CVD-admission rateB
Any CVD
Rate
per
100 p
ers
on-y
ear
CHFDysrhythmiaMIStroke
Figure 2. Annualized mortality (A) and cardiovascular disease admission rates (B) ondifferent days of the hemodialysis (HD) week. After reference 50: Foley et al. N Engl J Med. 2011;365(12):1099-1107. © 2011, MassachusettsMedical Society.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 271

Mondays, for example, are beingcompared with outcomes on otherdays. Accordingly, if one finds dis-parities in outcome rates relatedto days of the hemodialysis week,the corresponding irrefutable ex-planatory hypothesis is that an un-measured temporal factor links theexcess mortality on certain days tothe scheduling of dialysis sessions.
RISK STRATIFICATION:GENERAL POPULATIONFACTORS THAT MAY BE
APPLICABLE IN CHRONICKIDNEY DISEASE
It is generally believed that mostsudden cardiac death cases in thegeneral population exhibit coro-nary artery disease on autopsy.50
Although, there is little reason tobelieve that uremia should protectagainst pathophysiological process-es of importance in the generalpopulation, the preceding discus-sion suggests that many other fac-tors specific to late-stage chronickidney disease may be important.
In the general population, left ven-tricular systolic dysfunction is animportant risk factor for suddencardiac death and a dominant evi-dence-based consideration for im-planted cardioverter defibrillatordevices. Even if one ignores the like-lihood that dialysis patients areexposed to many more risk factorsfor sudden cardiac death than theircounterparts in the general popula-tion, a nontrivial proportion haveready-made indications for thesedevices estimated at 6.3% in onecross-sectional study.52 While notnegligible, this figure appears topale into relative insignificancewhen compared with the incidenceof sudden cardiac death in this pop-ulation, suggesting that low ejec-tion fraction, alone, cannot accountfor the rates of sudden cardiac deathseen in dialysis patients.
Though likely to be very common,the true burden of coronary arterydisease is usually unclear in dialysispatients, as definitive diagnosticstudies are rarely applied system-atically. To date, there is little evi-dence to prove that coronary arterydisease is the dominant underlyingfactor, at least on a proportionatebasis, a hypothesis that appears tobe supported by the failure of statinsto confer benefit in dialysis popu-lations in well-designed clinical tri-als.15,53,54 Lack of autopsy data hasclearly retarded pathophysiologicalinsights, as, to date, only one studyhas reported autopsy findings indialysis patients who died sudden-ly.55 In the latter study, causes ofsudden death were investigated in113 Japanese patients who died be-tween 1979 and 1989. Autopsy wasperformed in 93 of the cases, and35 of these were considered to besudden deaths.
Dissecting aortic aneurysm was themost common cause of suddendeath (5), followed by cerebral hem-orrhage (3), acute subdural hema-toma (3), acute myocardial infarc-
tion (2), cerebral infarction (2), andsubarachnoid hemorrhage (1). Whilethe applicability of these findingsto latter-day populations is clearlyuncertain, and cerebrovascularevents are much more common inJapanese than Western populations,these findings are still noteworthy.
Left ventricular hypertrophy, whichis strongly associated with suddendeath in the general population, is typically present in about 4/5 ofmaintenance dialysis patients.56
Possibly because the issue of sud-den cardiac death has only recentlycome to prominence, associationsbetween left ventricular hypertrophyand sudden cardiac death have yetto be clearly defined.32,57
INTERVENTIONS TO PREVENT SUDDEN
CARDIAC DEATH
Sadly, there are no definitive ran-domized trials to guide preventivetherapy for sudden cardiac deathin patients with advanced chronickidney disease. When “trial” wasadded to the PubMed search termsdescribed above, only yielded 3 rel-evant citations (Table II)22,58,59 werefound (for implanted cardiac defib-rillators, nicorandil, and candesar-tan); none of these trials was bothspecific to a population with clini-cally meaningful chronic kidneydisease and designed with suddencardiac death as primary outcome.
While many candidate interventionscan be suggested, high incidencerates of sudden cardiac death andbeneficial effects in targeted mem-bers of the general population sug-gest that implanted cardiac defibril-lators deserve serious consideration.The enormous rates of sudden car-
272
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
Primary outcome Secondary outcome
CKD only Subgroup CKD only Subgroupwith CKD with CKD
Nicorandil D58
ICD ND22
Candesartan D59
Table II. Interventions to reduce sudden cardiac death in CKD: evidence base.Numbers are citation references.
Abbreviations: CKD, chronic kidney disease; D, dialysis; ICD, implanted cardiac defibrillator; ND,nondialysis.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 272

diac death in dialysis patients, com-bined with the inability to definephenotypic characteristics that couldreliably discriminate low- and high-risk subgroups, support the argu-ment that a trial of implanted car-diac defibrillators should be appliedto all dialysis patients where a pri-mary indication does not alreadyexist. In a less ideal world, one couldargue that patients with at leastmoderate systolic dysfunction orleft ventricular hypertrophy, overtcoronary artery disease, and dia-betic nephropathy might be candi-dates for this hypothetical trial.
A number of interesting observa-tional studies of dialysis patientshave been reported. Among themwas a retrospective cohort studywhose objectives were to examineimplanted cardiac defibrillator useand survival associations.60 A sub-set of approximately 6000 US dialy-sis patients who survived to dis-charge following hospitalization forventricular fibrillation or cardiacarrest was identified. Mortality as-sociations of implanted cardiac de-fibrillators placed within 30 days ofadmission were examined with botha comorbidity-adjusted Cox modeland a propensity model approach.Of these patients, 7.6% had an im-planted cardiac defibrillator andassociated 1-, 2-, 3-, 4-, and 5-yearsurvivals were 71%, 53%, 36%, 25%,and 22%, respectively; correspon-ding values were lower in the groupwithout an implanted cardiac de-fibrillator, at 49%, 33%, 23%, 16%,and 12%. Survival disparities per-sisted with standard comorbidityadjustment and with the propensity-adjusted approach. Similar issueswere examined in a more recentcohort of US dialysis patients overa longer time frame, 1994 to 2006,wherein mortality in implanted car-diac defibrillator recipients and oth-erwise similar nonimplanted cardiacdefibrillator patients were compared
with high-dimensional propensityscore matching.61 More than 88%of implanted cardiac defibrillatorswere placed after 2000, with implant-ed cardiac defibrillators in the 1990sexclusively used for secondary pre-vention, in contrast to the situationin 2006, when half the implantedcardiac defibrillators were used forprimary prevention. All-cause andcardiovascular mortality rates remained high in dialysis patientseven after implantation, and deviceinfections were not uncommon.Although implanted cardiac defib-rillator use in US dialysis patientsaccelerated from 2000 to 2005, datafor subsequent years suggest a pla-teau after 2005, possibly reflectingconcerns about long-term efficacy.
Considering their up-front cost, itseems clear that randomized con-trolled trials are needed to stream-line appropriate use of these devices.In this regard, the ICD2 (SecondImplantable Cardioverter Defibrilla-tors in Dialysis Patients) trial is ofgreat relevance.62 This trial plansto evaluate the effect of preventiveimplanted cardiac defibrillator ther-apy on sudden cardiac death ratesin dialysis patients aged 55 to 80years. The study plans to enroll atotal of 200 patients, with 4 yearsof follow-up. While the sample sizeof this study is likely to be beset byType II power issues, it should pro-vide invaluable information aboutthe feasibility of doing a largermore definitive study.
Among pharmacological therapies,β-blockers are an attractive optionfor a future randomized trial in ad-vanced chronic kidney disease. Inthis regard, the findings of a studyby Cice et al were noteworthy.63 In aplacebo-controlled trial of 114 dial-ysis patients with dilated cardiomy-opathy, carvedilol led to a favorableleft ventricular phenotype, lowermortality, lower cardiovascular mor-
tality, fewer all-cause and heart-fail-ure related admissions to hospitaland fewer fatal myocardial infarc-tions and strokes. Another groupassessed whether the subgroup ofsystolic heart failure patients withchronic kidney disease benefitedfrom carvedilol therapy by perform-ing a post-hoc analysis of pooledindividual patient data from theCAPRICORN (CArvedilol Post infaRc-tion survIval COntRol in left ven-tricular dysfunctioN) and COPER-NICUS (CarvedilOl ProspEctiveRaNdomIzed, CUmulative Survival)studies. Among the 60.8% of studysubjects with estimated glomerularfiltration rates below 60 mL/min/1.73 m2, treatment with carvediloldecreased the risks of death, firstheart failure hospitalization, and thecomposite of cardiovascular mor-tality or heart failure hospitalization.Interestingly, a clear effect on suddencardiac death was not discernible.Finally, based on observational evidence linking 2-day intervals toadverse outcomes in typical hemo-dialysis populations, trials of strate-gies that avoid these intervals needserious consideration.
REFERENCES
1. Lindner A, Charra B, Sherrard DJ,Scribner BH.
Accelerated atherosclerosis in prolongedmaintenance hemodialysis.
N Engl J Med. 1974;290(13):697-701.
2. Blacher J, London GM, Safar ME,Mourad JJ.
Influence of age and end-stage renal diseaseon the stiffness of carotid wall material inhypertension.
J Hypertens. 1999;17(2):237-244.
3. London GM, Fabiani F, MarchaisSJ, et al.
Uremic cardiomyopathy: an inadequate leftventricular hypertrophy.
Kidney Int. 1987;31(4):973-980.
273
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 273

4. Silberberg JS, Barre PE, PrichardSS, Sniderman AD.
Impact of left ventricular hypertrophy onsurvival in end-stage renal disease.
Kidney Int. 1989;36(2):286-290.
5. Foley RN, Parfrey PS, Harnett JD,et al.
Clinical and echocardiographic disease inpatients starting end-stage renal diseasetherapy.
Kidney Int. 1995;47(1):186-192.
6. Goodman WG, Goldin J, Kuizon BD,et al.
Coronary-artery calcification in youngadults with end-stage renal disease who areundergoing dialysis.
N Engl J Med. 2000;342(20):1478-1483.
7. Amann K, Wiest G, Zimmer G,Gretz N, Ritz E, Mall G.
Reduced capillary density in the myocardi-um of uremic rats—a stereological study.
Kidney Int. 1992;42(5):1079-1085.
8. McIntyre CW, Burton JO, Selby NM,et al.
Hemodialysis-induced cardiac dysfunctionis associated with an acute reduction inglobal and segmental myocardial blood flow.
Clin J Am Soc Nephrol. 2008;3(1):19-26.
9. Converse RLJ, Jacobsen TN, TotoRD, et al.
Sympathetic overactivity in patients withchronic renal failure.
N Engl J Med. 1992;327(27):1912-1918.
10. National Institutes of Health,National Institute of Diabetes andDigestive and Kidney Diseases.
U.S. Renal Data System, USRDS2010 Annual Data Report Atlas ofChronic Kidney Disease and End-Stage Renal Disease in the UnitedStates. Bethesda, MD, 2010.
11. Pratt CM, Greenway PS, Schoen-feld MH, Hibben ML, Reiffel JA.
Exploration of the precision of classifyingsudden cardiac death. Implications for theinterpretation of clinical trials.
Circulation. 1996;93(3):519-524.
12. Rocco MV, Yan G, Gassman J, et al.
Comparison of causes of death using HEMOStudy and HCFA end-stage renal diseasedeath notification classification systems.The National Institutes of Health-fundedHemodialysis. Health Care FinancingAdministration.
Am J Kidney Dis. 2002;39(1):146-153.
13. Foley RN, Parfrey PS, Sarnak MJ.
Epidemiology of cardiovascular disease inchronic renal disease.
J Am Soc Nephrol. 1998;9(12 suppl):S16-S23.
14. Eknoyan G, Beck GJ, Cheung AK,et al.
Effect of dialysis dose and membrane fluxin maintenance hemodialysis.
N Engl J Med. 2002;347(25):2010-2019.
15. Wanner C, Krane V, Marz W, et al.
Atorvastatin in patients with type 2 diabetesmellitus undergoing hemodialysis.
N Engl J Med. 2005;353(3):238-248.
16. Parekh RS, Plantinga LC, Kao WH,et al.
The association of sudden cardiac deathwith inflammation and other traditionalrisk factors.
Kidney Int. 2008;74(10):1335-1342.
17. Wang AY, Lam CW, Chan IH,Wang M, Lui SF, Sanderson JE.
Sudden cardiac death in end-stage renaldisease patients: a 5-year prospectiveanalysis.
Hypertension. 2010;56(2):210-216.
18. Pun PH, Lehrich RW, Smith SR,Middleton JP.
Predictors of survival after cardiac arrest inoutpatient hemodialysis clinics.
Clin J Am Soc Nephrol. 2007;2(3):491-500.
19. Karnik JA, Young BS, Lew NL, et al.
Cardiac arrest and sudden death in dialy-sis units.
Kidney Int. 2001;60(1):350-357.
20. Lai M, Hung K, Huang J, Tsai T.
Clinical findings and outcomes of intra-hemodialysis cardiopulmonary resuscitation.
Am J Nephrol. 1999;19(4):468-473.
21. Moss AH, Holley JL, Upton MB.
Outcomes of cardiopulmonary resuscitationin dialysis patients.
J Am Soc Nephrol. 1992;3(6):1238-1243.
22. Goldenberg I, Moss AJ, McNitt S,et al.
Relations among renal function, risk ofsudden cardiac death, and benefit of theimplanted cardiac defibrillator in patientswith ischemic left ventricular dysfunction.
Am J Cardiol. 2006;98(4):485-490.
23. Saxon LA, Bristow MR, BoehmerJ, et al.
Predictors of sudden cardiac death and ap-propriate shock in the Comparison of Med-ical Therapy, Pacing, and Defibrillation inHeart Failure (COMPANION) Trial.
Circulation. 2006;114(25):2766-2772.
24. Pun PH, Smarz TR, Honeycutt EF,Shaw LK, Al-Khatib SM, Middleton JP.
Chronic kidney disease is associated withincreased risk of sudden cardiac deathamong patients with coronary artery disease.
Kidney Int. 2009;76(6):652-658.
25. Deo R, Lin F, Vittinghoff E, Tseng ZH, Hulley SB, Shlipak MG.
Kidney dysfunction and sudden cardiacdeath among women with coronary heartdisease.
Hypertension. 2008;51(6):1578-1582.
26. Deo R, Sotoodehnia N, Katz R,et al.
Cystatin C and sudden cardiac death riskin the elderly.
Circ Cardiovasc Qual Outcomes. 2010;3(2):159-164.
27. Go AS, Chertow GM, Fan D,McCulloch CE, Hsu CY.
Chronic kidney disease and the risks of death,cardiovascular events, and hospitalization.
N Engl J Med. 2004;351(13):1296-1305.
28. Ibrahim HN, Foley R, Tan L, et al.
Long-term consequences of kidney donation.
N Engl J Med. 2009;360(5):459-469.
29. Bleyer AJ, Russell GB, Satko SG.
Sudden and cardiac death rates in hemodial-ysis patients.
Kidney Int. 1999;55(4):1553-1559.
274
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 274

30. Genovesi S, Valsecchi MG, RossiE, et al.
Sudden death and associated factors in ahistorical cohort of chronic haemodialysispatients.
Nephrol Dial Transplant. 2009;24(8):2529-2536.
31. Pun PH, Lehrich RW, HoneycuttEF, Herzog CA, Middleton JP.
Modifiable risk factors associated with suddencardiac arrest within hemodialysis clinics.
Kidney Int. 2011;79(2):218-227.
32. Krane V, Heinrich F, Meesmann M,et al.
Electrocardiography and outcome in patientswith diabetes mellitus on maintenance hemodialysis.
Clin J Am Soc Nephrol. 2009;4(2):394-400.
33. Cice G, Di Benedetto A,D’Andrea A, et al.
Heart rate as independent prognostic factorfor mortality in normotensive hemodialysedpatients.
J Nephrol. 2008;21(5):704-712.
34. Hage FG, de Mattos AM,Khamash H, Mehta S, Warnock D,Iskandrian AE.
QT prolongation is an independent predictorof mortality in end-stage renal disease.
Clin Cardiol. 2010;33(6):361-366.
35. Johansson M, Gao SA, Friberg P,et al.
Baroreflex effectiveness index and baroreflexsensitivity predict all-cause mortality andsudden death in hypertensive patients withchronic renal failure.
J Hypertens. 2007;25(1):163-168.
36. Beaubien ER, Pylypchuk GB,Akhtar J, Biem HJ.
Value of corrected QT interval dispersion inidentifying patients initiating dialysis atincreased risk of total and cardiovascularmortality.
Am J Kidney Dis. 2002;39(4):834-842.
37. Nishimura M, Tokoro T, Nishida M,et al.
Sympathetic overactivity and sudden car-diac death among hemodialysis patientswith left ventricular hypertrophy.
Int J Cardiol. 2010;142(1):80-86.
38. Drechsler C, Krane V, Ritz E,Marz W, Wanner C.
Glycemic control and cardiovascular eventsin diabetic hemodialysis patients.
Circulation. 2009;120(24):2421-2428.
39. Drechsler C, Pilz S, Obermayer-Pietsch B, et al.
Vitamin D deficiency is associated with sud-den cardiac death, combined cardiovascularevents, and mortality in haemodialysis patients.
Eur Heart J. 2010;31(18):2253-2261.
40. Fenske W, Wanner C, Allolio B,et al.
Copeptin levels associate with cardiovascularevents in patients with ESRD and type 2diabetes mellitus.
J Am Soc Nephrol. 2011;22(4):782-790.
41. Ganesh SK, Stack AG, Levin NW,Hulbert-Shearon T, Port FK.
Association of elevated serum PO(4), Ca xPO(4) product, and parathyroid hormonewith cardiac mortality risk in chronic he-modialysis patients.
J Am Soc Nephrol. 2001;12(10):2131-2138.
42. Krane V, Winkler K, Drechsler C,Lilienthal J, Marz W, Wanner C.
Association of LDL cholesterol and inflam-mation with cardiovascular events and mor-tality in hemodialysis patients with type 2diabetes mellitus.
Am J Kidney Dis. 2009;54(5):902-911.
43. Scialla JJ, Plantinga LC, Kao WH,Jaar B, Powe NR, Parekh RS.
Soluble P-selectin levels are associated withcardiovascular mortality and sudden car-diac death in male dialysis patients.
Am J Nephrol. 2011;33(3):224-230.
44. Szeto CC, Wong TY, Chow KM,Leung CB, Li PK.
Are peritoneal dialysis patients with andwithout residual renal function equivalentfor survival study? Insight from a retrospec-tive review of the cause of death.
Nephrol Dial Transplant. 2003;18(5):977-982.
45. Chonchol M, Goldenberg I, MossAJ, McNitt S, Cheung AK.
Risk factors for sudden cardiac death inpatients with chronic renal insufficiencyand left ventricular dysfunction.
Am J Nephrol. 2007;27(1):7-14.
46. Kjellstrand CM, Rosa AA,Shideman JR, Rodrigo F, Davin T,Lynch RE.
Optimal dialysis frequency and duration:the “unphysiology hypothesis.”
Kidney Int Suppl. 1978(8):S120-S124.
47. Culleton BF, Walsh M,Klarenbach SW, et al.
Effect of frequent nocturnal hemodialysis vsconventional hemodialysis on left ventricularmass and quality of life: a randomized controlled trial.
JAMA. 2007;298(11):1291-1299.
48. FHN Trial Group; Chertow GM,Levin NW, Beck GJ, et al.
In-center hemodialysis six times per week versus three times per week.
N Engl J Med. 2010;363(24):2287-2300.
49. Bleyer AJ, Hartman J, BrannonPC, Reeves-Daniel A, Satko SG,Russell G.
Characteristics of sudden death in hemodial-ysis patients.
Kidney Int. 2006;69(12):2268-2273.
50. Foley RN, Gilbertson DT, Murray T, Collins AJ.
Long interdialytic interval and mortalityamong patients receiving hemodialysis.
N Engl J Med. 2011;365(12):1099-1107.
51. Thomas AC, Knapman PA,Krikler DM, Davies MJ.
Community study of the causes of “natural”sudden death.
BMJ. 1988;297(6661):1453-1456.
52. Saravanan P, Freeman G,Davidson NC.
Risk assessment for sudden cardiac death indialysis patients: how relevant are conven-tional cardiac risk factors?
Int J Cardiol. 2010;144(3):431-432.
53. Fellstrom BC, Jardine AG,Schmieder RE, et al.
Rosuvastatin and cardiovascular events inpatients undergoing hemodialysis.
N Engl J Med. 2009;360(14):1395-1407.
275
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 275

54. Baigent C, Landray MJ, Reith C,et al.
The effects of lowering LDL cholesterol withsimvastatin plus ezetimibe in patients withchronic kidney disease (Study of Heart andRenal Protection): a randomised placebo-controlled trial.
Lancet. 2011;377(9784):2181-2192.
55. Takeda K, Harada A, Okuda S,et al.
Sudden death in chronic dialysis patients.
Nephrol Dial Transplant. 1997;12(5):952-955.
56. Foley RN, Parfrey PS, Harnett JD,Kent GM, Murray DC, Barre PE.
The prognostic importance of left ventriculargeometry in uremic cardiomyopathy.
J Am Soc Nephrol. 1995;5(12):2024-2031.
57. Paoletti E, Specchia C, Di Maio G,et al.
The worsening of left ventricular hypertro-phy is the strongest predictor of sudden car-diac death in haemodialysis patients: a 10year survey.
Nephrol Dial Transplant. 2004;19(7):1829-1834.
58. Nishimura M, Tokoro T, NishidaM, et al.
Oral nicorandil to reduce cardiac death aftercoronary revascularization in hemodialysispatients: a randomized trial.
Am J Kidney Dis. 2009;54(2):307-317.
59. Takahashi A, Takase H,Toriyama T, et al.
Candesartan, an angiotensin II type-1 re-ceptor blocker, reduces cardiovascular eventsin patients on chronic haemodialysis—a randomized study.
Nephrol Dial Transplant. 2006;21(9):2507-2512.
60. Herzog CA, Li S, Weinhandl ED,Strief JW, Collins AJ, Gilbertson DT.
Survival of dialysis patients after cardiacarrest and the impact of implantable car-dioverter defibrillators.
Kidney Int. 2005;68(2):818-825.
61. Charytan DM, Patrick AR, Liu J,et al.
Trends in the use and outcomes of implant-able cardioverter-defibrillators in patientsundergoing dialysis in the United States.
Am J Kidney Dis. 2011;58(3):409-417.
62. de Bie MK, Lekkerkerker JC, van Dam B, et al.
Prevention of sudden cardiac death: ration-ale and design of the Implantable Car-dioverter Defibrillators in Dialysis patients(ICD2) Trial—a prospective pilot study.
Curr Med Res Opin. 2008;24(8):2151-2157.
63. Cice G, Ferrara L, D’Andrea A, et al.
Carvedilol increases two-year survival indialysis patients with dilated cardiomyopa-thy: a prospective, placebo-controlled trial.
J Am Coll Cardiol. 2003;41(9):1438-1444.
276
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
How can we reduce sudden cardiac death in cardiorenal syndrome? - Foley and Herzog
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 276

277
he cardiovascular (CV) contin-uum as described by EugeneBraunwald and Victor Dzautwo decades ago1 and recent-
ly revisited2,3 is depicted in Figure 1,with a significant change in nameand content to take into accountthe high prevalence of the simulta-neous occurrence of CV and chronickidney (CKD) diseases. Thus, it isnow designated as the “cardiorenalcontinuum,” for which three mainstages may be distinguished:
• Stage 1 is characterized by thepresence of CV risk factors only,without any associated target organdamage (TOD). At this stage, ade-quate control of modifiable CV riskfactors (blood pressure [BP], smok-ing, lipids, metabolic syndrome,obesity, and diabetes) can prevent
the development of TOD and henceforestall cardiorenal morbidity (suchas microalbuminuria4,5 and left ven-tricular hypertrophy [LVH]6) andmortality. Pharmacotherapy in pa-tients with high-normal BP levelsis able to prevent the developmentof established hypertension (BP>140/90 mm Hg).7,8 But how effec-tive are these measures in prevent-ing future fatal and nonfatal CVevents and the progression of CKD?The answer is unknown and willprobably remain so forever becauseof the long duration and high costsof studies necessary to elucidatethis point. However, as far as dailyclinical practice is concerned, therecently demonstrated ability of anyof the four individual markers ofTOD (microalbuminuria, pulse wavevelocity, left ventricular mass and
What is the optimal pharmacotherapeutic approachto cardiorenal syndrome?Luis M. Ruilope, MD, PhD
Chief Hypertension Unit - Hospital 12 October - and Professor of Public Health and Preventive Medicine Autonomous University of Madrid - Madrid - SPAIN
T
Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Keywords: albuminuria; aldosterone block-er; angiotensin-converting enzyme inhibitor;angiotensin receptor blocker; cardiorenalcontinuum; chronic kidney disease;glomerular filtration rate; hyperkalemia;renin-angiotensin-aldosterone systemAddress for correspondence:Professor Luis M. Ruilope, MD, PhD,Unidad de Hipertensión, Hospital 12 deOctubre, Avda Córdoba s/n, 28041 Madrid,Spain (e-mail: [email protected])Dialogues Cardiovasc Med. 2011;16:277-283
“Cardiorenal syndrome” refers tothe different combinations of simul-taneous impairment in cardiac andrenal function. The presence of albuminuria and/or diminishedestimated glomerular filtration rate(eGFR) results in increased risk ofcardiovascular (CV) events and ofdeveloping end-stage renal disease.The high prevalence of chronic kid-ney disease along the CV continu-um is explained by the fact that theyshare common pathophysiologicalmechanisms. This also explains thesimilarities in pharmacologicaltreatment aimed at protecting theCV and renal systems. DecreasedeGFR can contraindicate dualblockade of the renin-angiotensin-aldosterone system with an angio-tensin-converting enzyme inhibitoror an angiotensin receptor blocker,in combination with an aldosteroneblocker.
Cardiorenal continuum
REGRESS
RETARD
PREV
ENT CKD
New risk factors
Risk factors ESRD Death
Target organ damageAsymptomatic
Target organ damage
Symp- tomatic
Atheroslerosis
Figure 1. Representation of cardiorenal continuum. Abbreviations: CKD, chronic kidney disease; ESRD, end-stage renal disease.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 277

carotid plaques) to predict CV mor-tality independently of SCORE (Sys-temic Coronary Risk Evaluation fromthe European Society of Cardiology[ESC] stratification),9 is an argumentin favor of preventing TOD. It is alsoimportant to take into account oth-er preventable types of TOD, suchas, for example, alterations in mi-crovascular function: thus, hyper-emic velocity has recently beenrecognized as an important param-eter for improving risk stratificationin apparently low-risk healthy men.10
Also, this is the stage where it isimportant to look for early markersof renal damage in an attempt todefine a pre-CKD stage, in a similarway as we define prehypertensionor prediabetes today.
• Stage 2 is characterized by thepresence of one or several types ofsubclinical TOD, such as the pres-ence of CKD. Adequate control ofBP and other risk factors can facili-tate the regression of TOD. Prelim-inary data indicate that regressionof albuminuria11,12 and LVH13,14 isassociated with a significant de-crease in number of CV events. Incontrast, increase in urinary albuminexcretion predicts the developmentof CV events or death.12 These find-ings suggest the usefulness of mon-itoring TOD in patients at this stageof the cardiorenal continuum andof including prevention of TOD asan end point in future trials, in par-ticular in hypertensive patients.
• Stage 3 is characterized by thepresence of clinically overt CV dis-ease and /or advanced renal failuredue to the progression of TOD andatherosclerosis. Both conditionsultimately result in CV mortality orend-stage renal disease (ESRD),which in the absence of dialysis isalso fatal. Active intervention onBP and associated cardiovascularrisk factors together with therapiesspecifically directed at overt CV and
renal disease in many cases unfor-tunately only delays the appearanceof new CV or renal events. Identifi-cation of patients at high risk ofdeveloping CV and renal events inthe first two stages described aboveis therefore of enormous importancebecause the great majority of CVand renal events take place in pa-tients belonging to those two stages.Age, clustering of CV and renal riskfactors, and presence of diverseforms of TOD together with theemerging role of genetics and new-er techniques such as proteomicswill greatly facilitate this task.
In summary, adequate managementof modifiable CV risk factors as soonas they are detected will greatly con-tribute to slowing the progressionof atherosclerosis and CKD, there-by ensuring long-term benefits.
The term cardiorenal syndrome de-scribes five situations in which theheart and the kidney interact: acutesituations where failure of the oneaffects the other (= 2); situations inwhich a chronic condition of oneaffects the other (= 2); and finallysystemic alterations that can affectheart and kidney simultaneously (= 1).15 In this paper I will exclusive-
ly refer to the cross-talk betweenheart and kidney in situations ofchronic kidney disease and how thelatter influences our therapeutic at-titude in patients with heart disease.
DETECTION OF CHRONIC KIDNEY DISEASE
The two relevant measures to de-tect the presence of CKD are thecalculation of glomerular filtrationrate (usually estimated using a for-mula = eGFR) and the finding ofalbumin in the urine. The CKD-EPI16
formula is the most widely usedone because it corrects for much ofthe overestimation of CKD, espe-cially among eGFR values between60 and 89 mL/min/1.73m2. Formu-las to estimate GFR rely on the accuracy of serum creatinine mea-surement, avoiding the presence ofchromogens, which can increase itsvalue by up to 20%.
Albuminuria can be determinedover the 24 h (mg/24 h) or overnight(μg/min), but the presence of albu-minuria is most frequently assessedby obtaining three early morningspot urine samples at different timesover 1 or 2 months. Two out of thethree with values above 30 mg/g of
278
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
SELECTED ABBREVIATIONS AND ACRONYMS
ARB angiotensin receptor blocker
BP blood pressure
CKD chronic kidney disease
CV cardiovascular
DRI direct renin inhibitor
eGFR estimated glomerular filtration rate
ESRD end-stage renal disease
GFR glomerular filtration rate
LVH left ventricular hypertrophy
RAAS renin-angiotensin-aldosterone system
SCORE Systemic Coronary Risk Evaluation
TOD target-organ damage
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 278

creatinine is enough to declare thepresence of microalbuminuria.17
Values above 300 mg/dL define thepresence of macroalbuminuria orproteinuria.
The definition and classification ofCKD18 is contained in Table I, wherefive stages can be seen, accordingto eGFR values. In the first two, CKDis only defined by the presence ofalbuminuria while in the other threeit is the level of eGFR that definesthe presence of CKD, rather thanalbuminuria.
Both an eGFR <60 mL/min/1.73m2
and the presence of microalbumin-uria are independent and additivepredictors of future CV morbidityand mortality. CKD is a commonprocess whose prevalence is over10% in the general population, with6% to 7% having only microalbumin-uria and 3% to 5% having a dimin-ished eGFR.19 Most of the perceivedprevalence of CKD is accounted forby individuals older than 60 years,and according to El Nahas20 such ahigh prevalence of CKD in peoplewith advanced age represents a sit-uation of diffuse and age-relatedcardiorenal damage that requirescareful evaluation and treatment.
WHY IS CKD SOPREVALENT IN CVDAND VICE VERSA?
The Framingham study showed thatestablished CV risk factors (age,body mass index, diabetes, smok-ing, hypertension, high-density lipo-protein (HDL)-cholesterol, and thelevel of eGFR) are associated withthe development of new-onset kid-ney disease.21 In many cases, thesame risk factors contribute to thesimultaneous development of CVand renal disease. Patients witheGFR <90 mL/min/1.73 m2 and es-tablished CV risk factors should bemonitored for the progression of
kidney disease.21 Their common ori-gin explains why CV and renal dis-ease are so frequently seen togeth-er and why the presence of CKDworsens the prognosis of estab-lished CV disease.
PHARMACOTHERAPY INCARDIORENAL DISEASE
Figure 2 (page 280) depicts thepathophysiological mechanisms un-derlying the cross-talk between CVand renal disease.19 The main fac-tors involved in injury to the CVsystem and the kidney include acti-vation of the renin-angiotensin-al-dosterone (RAAS) and sympatheticnervous systems (SNS) and alter-ation in renal sodium excretion(DNaU). Their action combines topromote the clinical manifestationsof CV disease (coronary artery dis-ease, heart failure, stroke, and pe-ripheral artery disease) as well asthe progression of CKD and theonset of albuminuria. Once renalfunction is altered, new risk factorsappear that hasten the progressionof CV and renal disease, such asanemia, calcium-phosphate disor-ders, and vitamin D deficiency,19
while the deleterious effect of thethree main factors—RAAS, SNS,and DNaU—further increases.
As can be seen in Figure 2, the op-timal therapy is similar for both CVand renal protection and includesappropriate lifestyle measures suchas physical activity and quittingsmoking, and achieving adequatecontrol of BP, blood lipids, HbA1c,and body weight. Pharmacotherapyconsists of an ACE inhibitor or anARB at the highest tolerated dose,usually in conjunction with otherantihypertensive drugs, in particularcalcium channel blockers and diuret-ics when BP is elevated, and anti-diabetic therapy in diabetics. Theuse of a statin is mandatory as isthe use of aspirin when CKD is pres-ent.22 New forms of therapy haveto be added when impairment inrenal function progresses, such asphosphate binders, vitamin D sup-plements (including vitamin D re-ceptor analogs), and erythropoietin.These new treatments also con-tribute to counteract the progres-sion of CV and renal damage.
RAAS AND SNS ASPRIMARY THERAPEUTICOBJECTIVE IN CARDIO-
RENAL DISEASE: ADVANTAGES AND RISKS
Chronic activation of the RAAS andSNS is implicated in a wide range
279
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
Stage Description GFR
At increased risk Risk factors for kidney disease >90(diabetes, high blood pressure familial history, older age, ethnic group)
Stage 1 Kidney damage (albuminuria) and normal >90 renal function
Stage 2 Kidney damage and mild decrease in GFR 60-89
Stage 3 Moderate decrease in GFR 30-59
Stage 4 Severe decrease in GFR 15-29
Stage 5 Kidney failure (dialysis needed soon) <1
Table I. The five stages of chronic kidney disease (CKD). Values of glomerular filtration rate (GFR) represent eGFR = estimated GFR.
Modidfied after reference 18: Levey et al. Kidney Int. 2011;80:17-28. © 2011, Nature PublishingGroup.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 279

of CV diseases, as described in Fig-ure 3. As can be seen, these twosystems promote the developmentand progression of TOD in the brain,vessels, kidney, and heart, leadingto the development of CV eventsand CKD, resulting in death. Thus,a series of mechanisms starting withendothelial dysfunction lead to thedevelopment and progression ofatherosclerosis, arteriosclerosis, hy-pertrophy and increased stiffnessof the vessels, decrease in eGFRand albuminuria, resulting in pro-gressive glomerulosclerosis, cardiachypertrophy, fibrosis and remodel-ing, and ultimately coronary arterydisease and heart failure.
Blocking the adverse effects of theRAAS has been a main goal in thetreatment of CV and renal diseasefor the past 30 years. Use of ACE
inhibitors, ARBs, and more recentlydirect renin inhibitors (DRIs) shouldbe started in clinical practice fromthe very first stages of the cardiore-nal continuum to prevent the de-velopment of TOD4-6 or regress itsmanifestations.11-14 Early RAAS sup-pression also prevents the develop-ment of established hypertension.7,8
Early RAAS suppression started tobe used following initial positiveresults obtained in heart failure,post myocardial infarction, and pa-tients with increased global CV riskor advanced renal failure. Initially,the benefits of these drugs weremostly attributed to the suppres-sion of the effects of angiotensin II,while the role of aldosterone andof the mineralocorticoid receptorreceived less attention because itwas initially assumed that treatment
with an ACE inhibitor would alsosuppress aldosterone. The mecha-nisms of angiotensin II binding tothe AT1 and AT2 receptors is depict-ed in Figure 4. The clinical interestin blocking aldosterone in patientsalready treated with an ACE inhibitoror ARB has been stimulated by re-cent trials in heart failure23 and re-sistant hypertension.24 In both cas-es, spironolactone and eplerenonewere found to be very effective.
However, RAAS suppression maygive rise to unwanted and deleteri-ous side effects. Hypotension, de-crease in eGFR, and hyperkalemiaare the main complications associ-ated with RAAS suppressors. Pre-existing sodium depletion and re-duced eGFR are the most importantfactors contributing to these com-plications. Aldosterone blockers, in
280
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
CVRFAge, Ethnicity
Diabetes/MetSyn/ObesityHypertension, hyperlipidemia
Smoking
Primary renal diseasesDeranged fetal programming with nephron underdosing
BP controlLipid controlHbA1C controlBody weight controlAntiplatelet therapyQuit smokingAdequate dietPhysical activity
Stage 3-5 CKDPhosphate controlAnemia controlVitamin D deficiency
RRF(stage 3-5 of CKD)
AlbuminuriaAnemia
Vitamin D deficiencyCalcium/phosphate
alterationsADMA
+
++ –
–
+
+ +
CKDeGFR <60 mL/min/1.73 m2
Albuminuria
CVDAtherosclerosis
Figure 2.Pathophysiologic-al mechanisms involved in thecross-talk betweenthe cardiovascu-lar system andthe kidney.
Abbreviations:ADMA, asymmetricdimethyl–L-arginine;BP, blood pressure;CVD, cardiovasculardisease; CKD, chron-ic kidney disease;CVRF, cardiovascu-lar risk factors;eGFR, estimatedglomerular filtra-tion rate, MetSyn,metabolic syndrome;RRF, renal risk factors. Modified afterreference 19:Ruilope and Bakris.Eur Heart J.2011;32:1599-1604Oxford UniversityPress © The Author.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 280

281
particular when added to an ACEinhibitor or an ARB should be usedwith caution when eGFR values arebelow 30 mL/min/1.73 m2. However,each case should be considered onan individual basis and the risk/benefit ratio carefully assessed. Thismeans that in patients with estab-lished CV disease in whom the en-hancement of CV risk due to thepresence of CKD is the highest, thepossibility of using RAAS blockadeobtained with an ACE inhibitor,ARB, or DRI in combination with an
aldosterone blocker may be limit-ed by the potential development of hyperkalemia, particularly in pa-tients with serum potassium levelsabove 5 mmol/dL before introduc-ing the aldosterone blocker.
Combination therapy with β-block-ers also contributes to increasingthe risk of hyperkalemia as does ahigh potassium intake or the useof nonsteroidal anti-inflammatorydrugs. Administration of higher dos-es of loop diuretics can increase
urinary potassium excretion. Finally,the usefulness of chronic treatmentwith potassium binders is currentlybeing evaluated.25
Evidence has accumulated over thepast three decades that SNS acti-vation is crucial in the developmentof CV disorders, most notably heartfailure and arterial hypertension,and that its activity is significantlyincreased in CKD, as reflected byhigh cardiac norepinephrine spill-over and reduced myocardial norep-inephrine stores.26 These pathophys-iological findings have translatedinto better treatment for heart fail-ure patients thanks to the introduc-tion of β-adrenergic blockers. How-ever, evidence of efficacy has beenestablished only for some β-adren-ergic blockers (bisoprolol, meto-prolol succinate, carvedilol, andnebivolol), and, therefore, patientsreceiving therapy for a comorbidcondition have to be switched toone of the above β-adrenergic block-ers. In the case of arterial hyperten-sion, it is now well established thatrenal sympathetic innervation playsa pivotal role in the pathogenesisof essential hypertension27 by in-fluencing renin release, GFR, and
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
Figure 3.Implications ofthe RAAS andSNS in cardio-vascular andrenal diseases.
Abbreviations:CKD, chronic kid-ney disease;RAAS, renin-an-giotensin-aldos-terone system;SNS, sympatheticnervous system.
AtherosclerosisVasoconstrictionVascular hypertrophyEndothelial dysfunction
Stroke
HypertensionArteriosclerosisStiffnessArteriolar remodelling
Glomerular filtration rateProteinuriaAldosterone releaseGlomerular sclerosis
CKD
HypertrophyFibrosisRemodellingCell death
Heart failureMyocardial infarction
BRAIN
VESSELS
KIDNEY
HEART
RAAS
SNS
DEATH
AldosteroneSecretion
Sodium retentionVasoconstriction
InflammationCell growth
HypertrophyAngiogenesis
AT1 receptor AT2 receptor
Modulation of cardiovascular and renal damage
VasodilationAntigrowth
Antihypertrophic effect (?)Apoptoais
Angiogenesis (?)
Figure 4. Cardiorenal consequences of the binding of angiotensin II to AT1 and AT2receptors.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 281

282
renal tubular sodium reabsorption.Antiadrenergic therapies includeaerobic exercise training, and calo-rie restriction,28 in addition to theuse of centrally acting sympatheticsuppressants, imidazoline-bindingagents such as moxonidine and ril-menidine. However, these drugs areunderused in the treatment of ar-terial hypertension.
Very recently, a new technique usingrenal artery catheter-based renaldenervation has been shown to con-trol the blood pressure in resistanthypertension,29 opening a new wayto improve the influence of sympa-thetic nervous activity in other sit-uations such as milder forms of hy-pertension and heart failure.
SUMMARY
The presence of CKD is very frequentthroughout the CV continuum. Theterm cardiorenal syndrome refersto the various combinations of si-multaneous impairment in cardiacand renal function. The presence ofalbuminuria and/or diminishedeGFR contribute to increasing therisk of CV events, mortality and pro-gression to end-stage renal disease.The high prevalence of CKD in theCV continuum is explained by thefact that they share similar patho-physiological mechanisms; this alsoexplains the similarity between phar-macological treatments to protectthe CV and renal systems. Advancedforms of renal failure require addi-tion of specific therapy to achievedual protection of the CV system andkidney. Diminished eGFR may con-traindicate dual RAAS blockade withan ACE inhibitor or an ARB togeth-er with an aldosterone blocker.
REFERENCES
1. Dzau V & Braunwald E.
Resolved and unresolved issues in the pre-vention and treatment of coronary arterydisease: a Workshops consensus statement.
Am Heart J. 1991;121:1244-1263.
2. Dzau V, Antman EM, Black HR, et al.
The cardiovascular disease continuum vali-dated: clinical evidence of improved patientoutcomes. Part I: Pathophysiology andclinical trial evidence (risk factors throughstable coronary disease).
Circulation. 2006;114:2850-2870.
3. Dzau V, Antman EM, Black HR, et al.
The cardiovascular disease continuum vali-dated: clinical evidence of improved patientoutcomes. Part II: Clinical trial evidence(acute coronary syndrome through renaldisease) and future directions.
Circulation. 2006;114:2871-2891.
4. Ruggenenti P, Fassi A, Ilieva AP, et al.
Preventing microalbuminuria in type 2 diabetes.
N Engl J Med. 2004;351:1941-1951.
5. Haller H, Ito S, Izzo JL Jr, et al.
Olmesartan for the delay or prevention ofmicroalbuminuria in type 2 diabetes.
N Engl J Med. 2011;364:907-917.
6. Ruggenenti P, Iliev I, Costa GM, et al.
Preventing left ventricular hypertrophy byACE inhibition in hypertensive patientswith type 2 diabetes: a prespecified analysisof the Bergamo Nephrologic DiabetesComplications Trial (BENEDICT).
Diabetes Care. 2008;31:1629-1634.
7. Julius S, Nesbitt SD, Egan BM, et al.
Feasibility of treating prehypertension withan angiotensin-receptor blocker.
N Eng J Med. 2006;354:1685-1697.
8. Lüders S, Schrader J, Berger J, et al.
The PHARAO study: prevention of hyperten-sion with the angiotensin-converting enzymeinhibitor ramipril in patients with high-nor-mal blood pressure: a prospective, randomizedcontrolled prevention trial of the GermanHypertension League.
J Hypertens. 2008;26:1487-1496.
9. Sehestedt T, Jeppesen J, HansenTW, et al.
Risk prediction is improved by adding mark-ers of subclinical organ damage to SCORE.
Eur Heart J. 2010;31:883-891.
10. Anderson TJ, Charbonneau F,Title LM, et al.
Microvascular function predicts cardiovas-cular events in primary prevention.
Circulation. 2011;123:163-169.
11. Ibsen H, Olsen MH, Wachtell K,Borch-Johnsen K, Lindholm LH,Mogensen CE.
Reduction in albuminuria translates to reduction in cardiovascular events in hyper-tensive patients with Leith ventricular hyper-trophy and diabetes.
J Nephrol. 2008;21:566-569.
12. Schmieder R, Mann JF,Schumacher H, et al.
Changes in albuminuria predict mortalityand morbidity in patients with cardiovascu-lar disease.
J Am Soc Nephrol. 2011;22:1353-1364.
13. Wachtell K, Okin PM, Olsen MH,et al.
Regression of electrocardiographic left ven-tricular hypertrophy during antihypertensivetherapy and reduction in sudden cardiacdeath.
Circulation. 2007;116:700-705.
14. Verdecchia P, Sleight P, Mancia G,et al.
Effects of telmisartan, ramipril, and theircombination on left ventricular hypertrophyin individuals at high vascular risk in theOngoing Telmisartan Alone and in Combi-nation With Ramipril Global End Point Trialand the Telmisartan Randomized AssessmentStudy in ACE Intolerant Subjects With Car-diovascular Disease.
Circulation. 2009;120:1380-1389.
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 282

15. Ronco C, Haapio M, House AA,Anavekar N, Bellomo R.
Cardiorenal syndrome.
J Am Coll Cardiol. 2008: 52: 1527-1539.
16. Levey AS, Stevens LA, SchmidCH, et al.
A new equation to estimate glomerular fil-tration rate.
Ann Intern Med. 2009;150:604-612.
17. De Jong P, Curhan GC.
Screening, monitoring, and treatment of albuminuria: public helth perspectives.
J Am Soc Nephrol. 2006;17:2120-2126.
18. Levey AS, de Jong PE, Coresh J,et al.
The definition, classification and prognosisof chronic kidney disease: a KDIGO contro-versies conference report.
Kidney Int. 2010;80:17-28.
19. Ruilope LM, Bakris GL.
Renal function and target organ damagein hypertension.
Eur Heart J. 2011;32:1599-1604.
20. El Nahas M.
Cardio-kidney damage: a unifying concept.
Kidney Int. 2010:78:14-18.
21. Fox CS, Larson MG, Leip EP,Culleton B, Wilson PF, Levy D.
Predictors of new onset kidney disease in acommunity-based population.
JAMA. 2004;291:844-850.
22. Wali RK.
Aspirin and the prevention of cardiovasculardisease in chronic kidney disease. Time tomove forward?
J Am Coll Cardiol. 2010;56:957-965.
23. Böhm M, Reil JC, Bramlage P,Pitt B, Zannad F.
Clinical efficacy of aldosterone blockingagents.
Eur Heart J. 2011;13(suppl B):B36-B39.
24. Sowers JR, Whaley-Connell A,Epstein M.
Narrative review: the emerging clinical impli-cations of the role of aldosterone in the meta-bolic syndrome and resistant hypertension.
Ann Intern Med. 2009;150:776-783.
25. Pitt B, Anker SD, Bushinsky DA,Kitzman DW, Zannad F, Huang IZ.
Evaluation of the efficacy and safety ofRLY5016, a polymeric potassium binder, ina double-blind, placebo controlled study inpatients with chronic heart failure (thePEARL-HF trial).
Eur Heart J. 2011;32:820-828.
26. Esler M.
The sympathetic nervous system throughthe ages: from Thomas Willis to resistanthypertension.
Exp Physiol. 2011;96:611-622.
283
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
What is the optimal pharmacotherapeutic approach to cardiorenal syndrome? - Ruilope
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 283

284
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
lthough in recent yearsthere has been an enor-mous progress in themanagement of patients
with heart failure (HF), both qualityof life and prognosis remain poorin this clinical syndrome, and HFstill constitutes a serious economicburden in modern societies. There-fore, there is an urgent need for theimplementation of novel therapies.
There is no doubt that myocardialdamage is the very first event in thecomplex pathophysiology of HF,and that this precipitates the sub-sequent changes occurring in mostbody organs and tissues, includingrenal and hematopoietic systems.1
Importantly, there is increasing evi-dence that these triggered peripher-al pathophysiological mechanismsand comorbidities (such as renalfailure and/or anemia), which aredirectly related to augmented symp-toms and poor outcomes, are poten-tial therapeutic targets in patientswith HF.
Impairment of renal function is arelatively common and ominous dis-order occurring in the course of HF,and the combination of these twoentities forms the so-called cardio-renal syndrome.2 The combinationof chronic kidney disease (CKD) andHF is of particular importance, be-cause each disorder can acceleratethe progression of the other andnegatively affect outcomes. It has re-cently been recognized that due tocommon pathophysiological mecha-
nisms and etiological and risk fac-tors, these disorders frequently coexist with anemia and/or irondeficiency (ID), prompting the fol-lowing designations, cardiorenal-anemia syndrome [CRAS] and cardiorenal-anemia-ID syndrome[CRAIDS], respectively, to be pro-posed.3
It was more than 50 years ago thatanemia and ID were first reportedto further worsen the compromisedhemodynamics in HF, but surpris-ingly these intriguing observationsremained neglected. Recently, ane-mia and ID have been receivinggrowing interest among both scien-tists and clinicians as potential nov-el therapeutic targets in patientswith HF.4-6
PATHOPHYSIOLOGICALMECHANISMS LEADING TO ANEMIA AND IRON DEFICIENCY IN HEART
FAILURE
The pathophysiology of anemia and/or ID in patients with HF is complex,multifactorial, and still unclear.4-8
Several pathophysiological mecha-nisms are presumed to contributeto the development of anemia inthe course of HF (Table I).4,7 Angio-tensin II diminishes renal perfusionand as a consequence increaseserythropoietin (EPO) secretion bythe kidneys, hence inhibition of an-giotensin II production (due to treat-ment with angiotensin-convertingenzyme [ACE] inhibitors) or signal-
Should anemia be actively treated in cardiorenal syndrome?Ewa A. Jankowska, MD, PhD, FESC; Piotr Ponikowski, MD, PhD, FESC
Department of Heart Diseases - Wroclaw Medical University - and Center for Heart Diseases - Military Hospital - Wroclaw - POLAND
Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
Anemia and/or iron deficiency (ID)is a frequent comorbidity in patientswith cardiorenal syndrome, andtogether with heart failure (HF)and chronic kidney disease (CKD)constitutes the cardio-renal-anemiasyndrome. There are substantialdifferences in the pathogenesis ofanemia as well as in the effect oftreatment with erythropoietin (EPO)or its analogs (with or withoutiron), depending on whether ane-mic patients have primary HF orprimary CKD. Studies with EPOor its analogs in anemic patientswith HF are still inconclusive, andshow evidence of EPO resistance, inmost cases associated with inflam-mation and/or ID. IV iron improvesfunctional status, quality of life,and exercise capacity in ID patientswith HF and may potentially be-come a novel therapeutic approachin anemic HF patients in the nearfuture.
Keywords: anemia; cardiorenal syndrome;chronic kidney disease; erythropoietin;heart failure; iron deficiencyAddress for correspondence:Associate Professor Ewa J. Jankowska, MD,PhD, FESC, Department of Heart Diseases,Wroclaw Medical University, Center forHeart Diseases, Military Hospital, ul. Weigla 5, 50-981 Wroclaw, Poland(e-mail: [email protected])Dialogues Cardiovasc Med. 2011;16:284-293
A
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 284

285
ing (due to treatment with angio-tensin receptor blockers [ARBs])may reduce circulating EPO in pa-tients with HF.9 ACE inhibition alsoblocks the disintegration of N-acetyl-seryl-aspartyl-lysyl-proline (a sup-pressor of hematopoietic stem cellproliferation)10 and inhibits brady-kinin degradation (which inducesmigration and homing of endothelialprogenitor cells and endothelialrepair).11
Augmented generalized inflamma-tion with high circulating proin-flammatory mediators and their in-creased expression in myocardiumand peripheral tissues constitutesa crucial element of the complexpathophysiology of HF. In most cas-es, anemia occurring in patients withHF is an anemia of chronic disease(ACD), of immunologic origin,12
or/and an anemia due to ID, wherethe involvement of immune mech-anisms has also been postulated,but not been definitively proven.6
In the study of Opasich et al, 20%of anemic patients with systolic HFhad microcytic anemia (accompa-nied by absolute ID), and 57% ofthem had ACD (accompanied main-ly by functional ID).13 It is suggestedthat in patients with HF, proinflam-matory mediators (such as inter-leukin 6 [IL-6]) also impair the func-tioning of the hematopoietic system.Namely, they contribute to the re-duced EPO production by the kid-neys, decrease bone marrow re-sponsiveness to EPO, induce EPOresistance within extrahematopoi-etic tissues, and restrict iron avail-ability for hematopoiesis and othermetabolic needs.8,12 Patients withHF have high circulating EPO levels,which increase proportionally tothe severity of heart disease.14,15
Among patients with HF (but not
in healthy subjects), there is only aweak negative correlation betweencirculating EPO and hemoglobin lev-els, which may reflect the impairedresponse of bone marrow to EPOstimulus (resistance to EPO).14,15
In addition to augmented general-ized inflammation, there are otherpotential causes of EPO resistancein HF, such as: ID, infections, malig-nancy, secondary hyperparathy-roidism, vitamin B12 or folic aciddeficiencies, intrinsic bone marrowdysfunction, hemolysis, and druginteractions.4,8
Pathophysiological mechanisms oc-curring in the course of HF also favorthe development of both absoluteand functional ID, which, when pro-found, leads to ID-associated ane-mia.6 Absolute ID reflects depleted
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
SELECTED ABBREVIATIONS AND ACRONYMS
(hs)CRP (high-sensitivity) C-reactive protein
ACD anemia of chronic disease
CHOIR Correction of Hemoglobin and Outcomes In Renal insufficiency
CKD chronic kidney disease
CREATE Cardiovascular Risk Reduction by Early Anemia Treatmentwith Epoetin Beta
EPO erythropoietin
ESA erythropoietin-stimulating agent
FAIR-HF Ferinject® Assessment in patients with IRon deficiency and chronic Heart Failure
FERRIC-HF FERRIC iron sucrose in Heart Failure
HF heart failure
ID iron deficiency
MCV mean corpuscular volume
NT-proBNP N-terminal prohormone of brain natriuretic peptide
RDW red cell distribution width
RED-HF Reduction of Events with Darbepoetin alfa in Heart Failure
STAMINA–HeFT Study of Anemia in Heart Failure Trial
TIBC total iron binding capacity
TREAT Trial to Reduce cardiovascular Events with Aranesp Therapy
TSAT transferrin saturation
• Inflammation
• Diminished EPO production
• EPO resistance
• ID (absolute and functional)
• Vitamin B12 deficiency
• Folic acid deficiency
• CKD (and associated metabolicabnormalities)
• Insulin resistance and/or dia-betes mellitus
• Hemodilution
• Gastrointestinal blood loss(also occult) due to impaired in-tegrity of intestinal mucosaand/or antiplatelet/anticoagulanttreatment
• ACE-inhibitor or/and ARB therapy
Table I. Major potential pathophysiologi-cal mechanisms favoring the developmentof anemia in heart failure.
Abbreviations: ACE, angiotensin-convertingenzyme; ARB, angiotensin receptor blocker;CKD, chronic kidney disease; EPO, erythropoi-etin; ID, iron deficiency.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 285

iron stores in the organism, where-as functional ID is diagnosed whenthere is an inadequate iron supplyto meet actual metabolic demanddespite normal or even abundantbody iron stores, and presence ofiron within the reticuloendothelialcells.6,16 In case of both absoluteand functional ID, iron remains un-available to cellular metabolism.The potential causes of absolute IDseen in HF are: poor nutrition lack-ing sufficient iron supply, reducedgastrointestinal absorption (due to,eg, mucosal edema), drug interac-tions, and gastrointestinal bloodloss (also occult), excessive men-strual bleeding, medications favor-ing bleeding.6,16
Functional ID is thought to be driv-en mainly by inflammatory stimuli(eg, IL-6), which induce the liversynthesis of hepcidin. Hepcidin isthe major regulator of iron metab-olism, and when released into thecirculation, blocks intestinal ironabsorption, traps iron in the reticu-loendothelial cells, and as a conse-quence results in a blockade of ironinflux to iron metabolizing cells.17,18
Importantly, this pathophysiologicalmechanism, although seen in CKDpatients and cancer, has not beenevidenced to date in the clinical set-ting of HF.
It should be emphasized that al-though there are many similaritiesin the pathophysiological mecha-nisms leading to anemia in pa-tients with HF and CKD, there arealso some differences.19 Most im-portantly, patients with CKD usual-ly exhibit absolute EPO deficiency,although circulating EPO levels arealso increased, but are inappropri-ately low in relation to hemoglobinlevels. In contrast, patients withHF have very high circulating EPO,and EPO resistance is the promi-nent feature of anemia associatedwith HF.19 These pathophysiological
differences may at least partiallyexplain the discrepancies observedin the effects of erythropoiesis stim-ulating agents (ESA) in patientswith HF and those with CKD (seecomment below).
DEFINITION AND PREVA-LENCE OF ANEMIA AND
IRON DEFICIENCY INHEART FAILURE
According to the World Health Or-ganization, anemia is diagnosedwhen hemoglobin is <13 g/dL inmen and <12 g/dL in postmeno-pausal women. According to theNational Kidney Foundation, anemiais diagnosed when hemoglobin is<12 g/dL in both men and post-menopausal women.
Anemia occurs relatively frequentlyin HF, with a prevalence varying fromapproximately 10% to 55%, due todifferences in the severity of heartdisease in studied HF populationsand in definitions of anemia.4,5,20
Anemia is more prevalent in patientsat advanced stages of HF, in olderand female subjects, in those withmultiple comorbidities (eg, renalfailure), and in patients with cardiaccachexia.5
Whereas the diagnosis of anemia,based only on hemoglobin level, isstraightforward, on the contrary, thediagnosis of ID is more complex,particularly in patients with chronicinflammatory diseases. Direct as-sessment of iron stores in bone mar-row biopsy is the gold standard forthe diagnosis of ID, but in the ma-jority of cases this procedure is replaced by parameters measuredin peripheral blood, such as: serumferritin; transferrin saturation (TSAT),the ratio of serum iron and total ironbinding capacity (TIBC) by transfer-rin, multiplied by 10021-23; serumsoluble transferrin receptor (sTfR)24;or indices of iron-restricted erythro-
poiesis, such as: mean corpuscularvolume (MCV); red cell distributionwidth (RDW); percentage of hypo-chromic red cells (PHRC); or con-tent of hemoglobin in reticulocytes(CHR).22
The diagnosis of absolute ID, de-fined as insufficient iron stores, isbased on circulating ferritin, whichis secreted from iron-storing cells.In the general population, absoluteID is diagnosed when serum ferritinis <30 μg/L,21-23 but in patients withinflammatory chronic diseases (suchas HF) higher cutoffs of serum fer-ritin (<100 μg/L) are used, becauseinflammatory stimuli, regardless ofiron status, can induce ferritin se-cretion. Reduced TSAT (<20%) is acommonly accepted surrogate ofinsufficient iron available for metab-olizing cells. When serum ferritin isbetween 100-300 µg/L (ie, when ironstores are normal/slightly increased),TSAT <20% allows diagnosis of func-tional ID.21-23 Therefore, a defini-tion of ID combining absolute andfunctional ID, could be applied inpatients with HF, as it was done infew clinical trials, eg, FERRIC-HF(FERRIC Iron Sucrose in Heart Fail-ure)25 and FAIR-HF (Ferinject® As-sessment in patients with IRon defi-ciency and chronic Heart Failure).26
There is scarce evidence on theprevalence of ID in anemic and non-anemic patients with HF. In thestudy by Ezekowitz et al, who ana-lyzed the data from national andhealth care insurance systems, ane-mia was found in 17% of patientshospitalized for HF, and ID was con-firmed in 21% of anemia cases.27
In the observational study of Opa-sich et al, the presence of ID wasdemonstrated in 36% of all anemicpatients with systolic HF and in 64%of subjects with ACD.13 Nanas et alconfirmed the presence of ID basedon depleted iron stores in bonemarrow in 73% of anemic patients
286
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 286

with decompensated advanced HFin New York Heart Association(NYHA) class IV.28 Adlbrecht et alshowed the presence of ID (serumferritin <30 µg/L or TSAT <15%) in26%, 16%, and 54% of all patientswith systolic HF, nonanemics, andanemics, respectively.29 We haveshown that ID (serum ferritin <100μg/L or serum ferritin 100-300 μg/Lwith TSAT <20%) was present in37%, 32%, and 57% of all patientswith systolic HF, nonanemics, andanemics, respectively.30 In our study,ID was more prevalent in patientsin advanced NYHA class, women,those with high plasma N-terminalprohormone of brain natriuretic pep-tide (NT-proBNP) and high serumhigh-sensitivity C-reactive protein(hsCRP) (Figure 1).30 (In the studyby Okonko et al, ID (serum ferritin<100 μg/L or serum ferritin 100-300μg/L with TSAT <20%) was moreprevalent, being present in 69%, 78%,and 65% of all, anemic, and nonane-mic patients with HF, respectively.31
CLINICAL AND PROGNOSTIC CONSE-QUENCES OF ANEMIA AND IRON DEFICIENCY
IN HEART FAILURE
In patients with HF, reduced hemo-globin is associated with impairedexercise capacity (expressed as re-duced 6-minute walking distanceand diminished peak oxygen con-sumption), poor quality of life, andmore advanced depressive symp-toms,4,20,32,33 The presence of ID isaccompanied by reduced peak oxy-gen consumption and increasedventilatory response to exercise,31,34
as well as by more severe depressivesymptoms,35 irrespective of theseverity of HF. These associationsbetween iron status and exercisecapacity and depressive symptomsare present in both nonanemic andanemic patients with systolic HF(Figure 2).34,35
Anemia is a strong and independ-ent predictor of high hospitalizationrates and increased cardiovascularand all-cause mortality in patientswith HF.4,20,31,36 Anemia also predictspoor outcome in patients with de-compensated HF.37 Moreover, thereduction in hemoglobin levels inHF is related to the increased mor-bidity and mortality in this group ofpatients.33,36 Finally, high circulatingEPO (an indirect measure of EPO
resistance), irrespective of hemo-globin and other clinical prognosti-cators, is also related to poor out-come in patients with HF,14,15 andanemic patients with HF with cir-culating EPO higher than expected(which may suggest the presenceof EPO resistance) have increasedmortality compared with those withserum EPO equal to or lower thanexpected, even after adjustment forclinical prognosticators.38
287
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 6
ID absentID present
Numbers at risk
12 18 3024
Patients without ID;Survival: 66.7%95% CI; 61.0-72.4%
Patients with ID;Survival: 53.6%95% CI; 46.2-61.0%
36
347199
331167
306145
240117
15974
20399
10156
P=0.0002
Follow-up (months)
Cum
ula
tive
eve
nt-
free s
urv
ival
Figure 1. Kaplan-Meier curves reflecting 3-year event-free survival rates in patientswith systolic chronic heart failure with vs without iron deficiency (ID).
After reference 30: Jankowska et al. Eur Heart J. 2010;31:1872-1880. © Published on behalf ofthe European Society of Cardiology (ESC) © 2011, The Author.
Iron deficiency (ID)AnemiaInteractions
F=12.72F=2.13F=0.01
P<0.001P=0.15P=0.94
Pea
k V
O2
(mL/
min
/kg)
17
16
15
14
13
12ID (–)
Anemia (–)ID (–)
Anemia (+)ID (+)
Anemia (–)ID (+)
Anemia (+)
Figure 2. Peak VO2 vsanemia and iron deficiency(ID). Peak oxygen consumption(VO2) (means ± standard error) in patients with systolicchronic heart failure, with vswithout ID, and with vs with-out anemia. ID was definedas serum ferritin <100 µg/L,or serum ferritin �100 µg/Land 100 to 300 µg/L whentransferrin saturation <20%.Anemia was defined as hemo-globin level <12 g/dL inwomen and <13 g/L in men.
After reference 34:Jankowska et al. J Card Fail.2011;17:899-906. © 2011,Elsevier Inc.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 287

288
So far only three observational stud-ies have evidenced a link betweeniron status and prognosis in patientswith systolic dysfunction39 and sys-tolic HF.30,31 In the study of Varmaet al in patients with systolic dys-function, ID-associated anemia wasrelated to high cardiac mortality,whereas malignancy-related anemiapredicted increased noncardiac mor-tality.39 In our study, the presenceof ID in patients with systolic HF, ir-respective of hemoglobin and otherclinical prognosticators, was a strongand independent predictor of deathand heart transplantation duringthe 3-year follow-up.30 In the studyby Okonko et al, ID defined as TSAT<20% was associated with increasedmortality in patients with HF.31
EFFECTS OF ERYTHROPOIETIN
THERAPY IN PATIENTSWITH HEART FAILURE
The relatively high prevalence ofanemia in patients with HF—partic-ularly those with advanced stages ofheart disease—and the unfavorableclinical and prognostic consequencesof this comorbidity, provided astrong rationale to study whetherthis group of patients would benefitfrom the correction of hemoglobinlevels using EPO or its analogs.
Several studies (mainly small, un-controlled studies) evidenced thefollowing advantageous effects ofEPO or its analogs in patients withHF: (i) reduction in HF symptomsand improvement in exercise capac-ity (reduced NYHA class, increasedpeak oxygen consumption); (ii) im-provement in quality of life; (iii) reduction in circulating natriureticpeptides; (iv) reduction in daily diuretic dose; (v) improvement insystolic and diastolic left ventricularfunction ventricle, assessed usingechocardiography; (vi) attenuationof certain peripheral pathophysio-
logical mechanisms (reduction incirculating markers of apoptosis andinflammation) (reviewed in 4,5,40).
However, the results of availablesmall randomized clinical trials withEPO analogs in anemic patientswith HF appeared to be inconclusiveand partially disappointing regard-ing both the nonsatisfactory im-provement in exercise capacity andprognosis. For example, in STAMI-NA-HeFT (Study of Anemia in HeartFailure Trial), Ghali et al found onlya trend toward reduced rates ofdeath or HF hospitalization after 1year in patients treated with darbe-poietin vs those receiving placebo.41
Interesting information was provid-ed by the meta-analysis by Kotechaet al, which included 11 random-ized controlled trials (nine studieswere placebo controlled and fivestudies were double blind; a total794 anemic patients with sympto-matic systolic HF were included)comparing patients treated witherythropoiesis-stimulating agents(ESA) with controls during up to 12months of follow-up.42 In this meta-analysis, ESA therapy significantlyextended exercise duration, pro-longed 6-minute walking distance,increased peak oxygen consumption,reduced NYHA class, increased leftventricular ejection fraction, reducedplasma BNP, improved quality oflife, and, importantly, reduced HFhospitalization rate.42 There wasonly a marginally significant reduc-tion in all-cause mortality in onegroup receiving ESA, but in the sub-groups with different lengths of fol-low-up the statistical significanceof this effect was lost.42 Importantly,ESA therapy did not increase therisk of potential adverse events, suchas hypertension, stroke, and myo-cardial infarction or other thrombo-embolic events.42 Similar resultswere provided by another meta-analysis by Lawler et al.43 However,the reader should be aware that
evidence on the safety of ESA inpatients with HF with various de-grees of renal function impairmentcomes only from small studies and these meta-analyses, which isfraught with obvious weaknessesand limitations.
Findings from studies on ESA inpatients with CKD and accompany-ing cardiovascular disease arerather discouraging. Therapy withESAs in patients with CKD (and incancer patients as well) is associat-ed with adverse effects, especiallywhen high doses are used, such asimpaired blood viscosity, derangednitric oxide metabolism, uncon-trolled hypertension, thromboem-bolic events, and, as a conse-quence, increased mortality rates.
The results of the CHOIR trial(Correction of Hemoglobin andOutcomes In Renal insufficiency)showed that patients with CKDwho achieved higher target hemo-globin levels (13.5 g/L) on ESAtherapy had increased rates of car-diovascular events (eg, myocardialinfarction, stroke, HF hospitaliza-tion, and death) as compared withthose who achieved lower hemo-globin levels (11.3 g/dL).44 Similarunfavorable effects of ESA therapyaiming to achieve normal hemo-globin/hematocrit values in pa-tients with CKD were seen in otherstudies, eg, the CREATE trial (Car-diovascular Risk Reduction by EarlyAnemia Treatment with EpoetinBeta)45 and the Normal Hematocrittreatment trial.46 The results of theseopen-label trials were strengthenedby evidence from the multicenter,double-blind, placebo-controlledrandomized TREAT trial (Trial toReduce cardiovascular Events withAranesp Therapy).47 In this trial car-ried out in 4038 patients with dia-betes, CKD (defined as estimatedglomerular filtration rate of 20 to60 mL/min/1.73m2 not requiring
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 288

hemodialysis) and anemia (baselinehemoglobin �11 g/dL), treatmentwith darbepoetin α with a hemo-globin target of 13 g/dL vs placebo(with the rescue therapy with dar-bepoetin α only if hemoglobin <9.0g/dL), did not reduce the risk of ei-ther death or a cardiovascular event(nonfatal myocardial infarction, HF,stroke, or hospitalization for myo-cardial ischemia), or death or end-stage renal disease (need for long-term renal replacement therapy), butwas associated with a significantlyincreased risk of stroke.47
At issue in these trials is whetheradverse effects in anemic patientswith CKD are due to inappropriate-ly high target hemoglobin levels orthe high EPO doses that had to beused in order to achieve these he-moglobin levels. Indeed, additionalanalyses from the CHOIR trial re-vealed that the worse outcome inCKD patients treated with ESA wasassociated with an ineffective re-sponse in terms of hemoglobin lev-els during increasing ESA doses.48
In the TREAT trial, anemic patientswith CKD and diabetes with a poorresponse to darbepoetin α (definedas the lowest quartile of percentchange in hemoglobin level (<2%)after the first two standardized dos-es of the drug) compared with thosewith a better hemoglobin response,received higher doses of darbepo-etin α, and had increased rates ofcardiovascular events and death.49
Moreover, ESA treatment consumesiron stores, hence when not sub-stantial the induced negative ironbalance may also negatively affectthe myocardium and erythron, andinduce EPO resistance. Finally, dueto the slightly different pathophys-iological background of anemia in patients with HF and CKD, it isdoubtful whether the results of tri-als with ESA in CKD populationscould also be implemented in HFcohorts.
Meta-analyses of small randomizedcontrolled trials (RCTs) suggest thatESA treatment may be safe, well-tolerated, and can improve exercisetolerance, reduce symptoms, andhave beneficial effects on someclinical outcomes in at least someanemic patients with HF. However,the evidence of at least partial fu-tility of EPO therapy cannot be ig-nored. The insufficient effectivenessof ESA therapy in patients with CKDand/or HF may be a consequenceof EPO resistance, which in mostcases results from inflammation it-self and/or associated ID (absoluteor functional), the latter not beingproperly recognized and, conse-quently, corrected.
Indeed, in patients with CKD re-quiring dialysis, TSAT and ferritinlevels identified patients with CKDwith poor response to EPO thera-py, and in this group of patients, IV iron therapy allowed reduction inthe EPO doses needed to achievetarget hemoglobin levels.50,51
There is much current debate on thedosage of EPO, the need for con-comitant iron therapy (oral versusintravenous), and which hemoglobinlevel should be achieved. It is hopedthat the ongoing RED-HF (Reduc-tion of Events with Darbepoetinalfa in Heart Failure) trial,52 a mul-ticenter placebo-controlled double-blind study of darbepoetin α in 3400anemic patients with HF, will beable to confirm the results of thesemeta-analyses.50 This trial was de-signed to evaluate the effect of dar-bepoetin α (dosed to achieve a hemoglobin level between 13 and14.5 g/dL) on mortality, morbidity(primary end point: time to deathfrom any cause or first hospital ad-mission for worsening HF, whicheveroccurs first), and quality of life inpatients with symptomatic systolicHF and anemia (baseline hemoglo-bin level between 9 to 12 g/dL).52
EFFECTS OF IRON SUPPLEMENTATION
THERAPY IN PATIENTSWITH HEART FAILURE
ID is a common and alarming co-morbidity in patients with HF. ID isnow recognized not only as a causalfactor leading to or aggravating ane-mia in HF, but also as a distinctcomorbidity independent of con-comitant anemia, with serious nega-tive consequences for hematopoiet-ic and extrahematopoietic tissues.6
In fact, ID is more prevalent thananemia itself in patients with HF,and the role of ID as the most com-mon etiological factor of anemia isunquestionable. Similarly, in HF,the effects of impaired EPO signal-ing (due to reduced EPO and/orimpaired responsiveness of targetcells to EPO) are evidenced both inhematopoietic and in extrahemato-poietic tissues.53 This prompted in-vestigation of the effects of IV irontherapy in six small studies andone trial in iron-deficient patientswith HF. Two of these includedboth anemic and nonanemic sub-jects25,26 (for details see reference 6)(Figure 3, page 290).26
So far, seven studies have been published (three open-label uncon-trolled studies, two randomizedopen-label studies, and two ran-domized double-blind placebo-con-trolled trials). They showed the fol-lowing advantageous effects ofintravenous iron therapy in pa-tients with systolic HF: reductionin HF symptoms; improvement inexercise capacity (reduced NYHAclass and increase in 6-minutewalking distance and peak oxygenconsumption); improvement inquality of life; reduction in plasmaNT-proBNP; reduction in daily di-uretic dosage; improvement in leftventricular systolic and diastolicfunction assessed using echocar-diography; increase in creatinine
289
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 289

290
clearance; trend toward reductionin circulating cystatin C and CRP(reviewed in reference 6).
To date, the FAIR-HF trial is thelargest randomized double-blindplacebo-controlled multicenter trial,in which 24-week IV iron therapy(or placebo) was administered to459 iron-deficient anemic and non-
anemic patients with systolic HF.26
Intravenous iron supplementationreduced NYHA class and improvedpatient global assessment, and thesebeneficial effects were evidenced in several clinical subgroups (eg,regardless of baseline hemoglobinand serum ferritin or presence ofrenal dysfunction and anemia),without any increased risk of side
effects.26 There was also a trend to-ward a reduced rate of first cardio-vascular hospitalization in patientsreceiving IV iron.26 As excess of irongenerates oxidative stress and canbe toxic, safety issues need to beaddressed and optimal serum fer-ritin and TSAT determined before IViron can be recommended in iron-deficient patients with HF. Furtherlarge and longer-running trials aretherefore needed to assess the safe-ty effects of IV iron therapy on mor-bidity and mortality in ID patientswith HF, both with and without ac-companying anemia.
CONCLUSIONS
Anemia is a frequent comorbidityin patients with HF, and togetherwith renal failure forms the cardio-renal-anemia syndrome. Its patho-physiology is complex and not fullyelucidated. The anemia is usually ofthe ACD type and/or is associatedwith ID.
Both anemia and ID remain under-recognized in the cardiovascular set-ting. Patients with HF, particularlythose with concomitant CKD, shouldbe screened for the presence of ane-mia and ID. Basic hematologicalfindings, including low hemoglobinlevels with reduced MCV and in-creased RDW, suggest the existenceof iron-restricted compromisederythropoiesis. Standard laboratoryscreening for iron status should in-clude serum ferritin and TSAT, cal-culated as the ratio of serum iron toTIBC or the ratio of serum iron toserum transferrin. Although not yet
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
8.0
4.0
2.0
1.0
0.5
0.00 4
FCMPlacebo
No. of patients
8 12 2016 24
304155
287147
294150
294150
Weeks since randomization
NYHA functional classA
Od
ds
rati
o (
95%
CI)
Pla
ceb
ob
ett
er
FC
Mb
ett
er
P<0.001 P<0.001 P<0.001
14
12
10
8
6
4
2
0
–20 4
No. of patientsMean score
FCM
8 12 2016 24
29554±1
27460±1
28362±1
28563±1
No. of patientsMean score
Placebo152
54±1140
54±2145
56±2146
57±2
Mean study-treatment effect
6±1 6±2 7±2
Weeks since randomization
EQ-5D visual analog scaleB
Change in s
core
P<0.001 P<0.001 P<0.001
Placebo
FCM
Figure 3. Effect of IV iron on NHYA func-tional class (Panel A) and quality of life(Panel B).Abbreviations: EQ-5D, standardized measure ofhealth status (EuroQol Group); FCM, ferric car-boxymaltose; NYHA, New York Heart Association.After reference 26: Anker et al. N Engl J Med.2009;361:2436-2448. © 2009, MassachusettsMedical Society.
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 290

291
tested in HF patients, soluble trans-ferrin receptor has been found to beuseful in the diagnosis of iron sta-tus in patients with hematologicaldisorders or with chronic diseases
Although the rationale for anemia(with/without ID) correction in pa-tients with HF and accompanyingCKD is strong, at the moment thereis huge uncertainty about the opti-mal hemoglobin level and how thislevel should be achieved. The guide-lines of the European Society ofCardiology for the management ofpatients with HF acknowledge ane-mia as a relatively common andalarming comorbidity, but its correc-tion is still not considered as partof standard therapy.
Reduced EPO signaling and deplet-ed tissue iron are serious negativeeffects for both hematopoietic andextrahematopoietic tissues, whileEPO and/or iron activate cardio-protective pathways. Studies withEPO or its analogs in anemic pa-tients with HF are still inconclusive.The partial futility of EPO therapy isexplained by EPO resistance, whichin most cases is the consequenceof inflammation and/or ID. Clinicalevidence suggests that IV iron im-proves functional status, quality oflife, and exercise capacity in ID pa-tients with HF. Treatment with EPOand/or iron is a novel and promis-ing therapeutic approach in anemicHF patients, but reliable evidencefrom multicenter trials on the effectsof ESA or iron therapy on morbidityand mortality end points is neededbefore it can be recommended inanemic and/or ID patients with HFas well as for determining the opti-mal effective and safe levels of hemoglobin, ferritin, and TSAT thatshould be achieved in this particu-lar group of patients.
REFERENCES
1. Jankowska EA, Ponikowski P,Piepoli MF, Banasiak W, Anker SD,Poole-Wilson PA.
Autonomic imbalance and immune activa-tion in chronic heart failure—pathophysio-logical links.
Cardiovasc Res. 2006;70:434-445.
2. Silverberg DS, Wexler D, Iaina A,Schwartz D.
The interaction between heart failure and oth-er heart diseases, renal failure, and anemia.
Semin Nephrol. 2006;26:296-306.
3. Palazzuoli A, Gallotta M, Iovine F,Nuti R, Silverberg DS.
Anaemia in heart failure: a common inter-action with renal insufficiency called thecardio-renal anaemia syndrome.
Int J Clin Pract. 2008;62:281-286.
4. Silverberg DS, Wexler D, Iaina A,Schwartz D.
The role of correction of anemia in patientswith congestive heart failure: a short review.
Eur J Heart Fail. 2008;10:819-823.
5. Von Haehling S, Jankowska EA,Ponikowski P, Anker SD.
Anemia in heart failure: an overview of current concepts.
Future Cardiol. 2011;7:119-129.
6. Jankowska EA, Von Haehling S,Anker SD, McDoughall I, Ponikowski P.
Iron deficiency and heart failure: diagnosticdilemmas and therapeutic perspectives.
Eur Heart J. 2011. In press.
7. Anand IS.
Heart failure and anemia: mechanisms andpathophysiology.
Heart Fail Rev. 2008;13:379-386.
8. Manolis AS, Tzeis S, Triantafyllou K,et al.
Erythropoietin in heart failure and othercardiovascular diseases: hematopoietic andpleiotropic effects.
Curr Drug Targets CardiovascHaematol Disord. 2005;5:355-375.
9. Ishani A, Weinhandl E, Zhao Z, et al.
Angiotensin-converting enzyme inhibitors asa risk factor for the development of anemia,and the impact of incident anemia on mortality in patients with left ventriculardysfunction.
J Am Coll Cardiol. 2005;45:391-399.
10. Van der Meer P, Lipsic E,Westenbrink BD, et al.
Levels of hematopoiesis inhibitor N-acetyl-seryl-aspartyl-lysyl-proline partially explainthe occurrence of anemia in heart failure.
Circulation. 2005;112:1743–1747.
11. Kränkel N, Katare RG, Siragusa M,et al.
Role of kinin B2 receptor signaling in therecruitment of circulating progenitor cellswith neovascularization potential.
Circulation. 2008;103:1335-1343.
12. Weiss G.
Iron metabolism in the anemia of chronicdisease.
Biochim Biophys Acta. 2009;1790:682-693.
13. Opasich C, Cazzola M, Scelsi L,et al.
Blunted erythropoietin production and de-fective iron supply for erythropoiesis as majorcauses of anaemia in patients with chronicheart failure.
Eur Heart J. 2005;26:2232-2237.
14. van der Meer P, Voors AA, Lipsic E,Smilde TD, van Gilst WH, vanVeldhuisen DJ.
Prognostic value of plasma erythropoietinon mortality in patients with chronic heartfailure.
J Am Coll Cardiol. 2004;44:63-67.
15. George J, Patal S, Wexler D, et al.
Circulating erythropoietin levels and prognosis in patients with congestive heart failure: comparison with neurohormonaland inflammatory markers.
Arch Intern Med. 2005;165:1304-1309.
16. Hentze MW, Muckenthaler MU,Galy B, Camaschella C.
Two to tango: regulation of Mammalianiron metabolism.
Cell. 2010;9;142:24-38.
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 291

17. Nemeth E, Ganz T.
The role of hepcidin in iron metabolism.
Acta Haematol. 2009;122:78-86.
18. Kemna EH, Tjalsma H, Willems HL,Swinkels DW.
Hepcidin: from discovery to differential diagnosis.
Haematologica. 2008;93:90-97.
19. Kazory A, Ross EA.
Anemia: the point of convergence or diver-gence for kidney disease and heart failure?
J Am Coll Cardiol. 2009;53:639-647.
20. Tang YD, Katz SD.
The prevalence of anemia in chronic heartfailure and its impact on the clinical out-comes.
Heart Fail Rev. 2008;13:387-392.
21. Wish JB.
Assessing iron status: beyond serum ferritinand transferrin saturation.
Clin J Am Soc Nephrol. 2006;1(suppl 1):S4-S8.
22. Goodnough LT, Nemeth E, Ganz T.
Detection, evaluation, and management ofiron-restricted erythropoiesis.
Blood. 2010;116:4754-4761.
23. Pasricha SR, Flecknoe-Brown SC,et al.
Diagnosis and management of iron deficiencyanaemia: a clinical update.
Med J Aust. 2010;1;193:525-532.
24. Koulaouzidis A, Said E, Cottier R,Saeed AA.
Soluble transferrin receptors and iron defi-ciency, a step beyond ferritin. A systematicreview.
J Gastrointestin Liver Dis. 2009;18:345-352.
25. Okonko DO, Grzeslo A,Witkowski T, et al.
Effect of intravenous iron sucrose on exercisetolerance in anemic and nonanemic patientswith symptomatic chronic heart failure andiron deficiency FERRIC-HF: a randomized,controlled, observer-blinded trial.
J Am Coll Cardiol. 2008;51:103-112.
26. Anker SD, Colet JC, Filippatos G,et al; FAIR-HF Trial Investigators.
Ferric carboxymaltose in patients withheart failure and iron deficiency.
N Engl J Med. 2009;361:2436-2434.
27. Ezekowitz JA, McAlister FA,Armstrong PW.
Anemia is common in heart failure and isassociated with poor outcomes: insightsfrom a cohort of 12,065 patients with new-onset heart failure.
Circulation. 2003;107:223-225.
28. Nanas JN, Matsouka C,Karageorgopoulos D, et al.
Etiology of anemia in patients with advancedheart failure.
J Am Coll Cardiol. 2006;48:2485-2489.
29. Adlbrecht C, Kommata S,Hülsmann M, et al.
Chronic heart failure leads to an expandedplasma volume and pseudoanaemia, but doesnot lead to a reduction in the body’s red cellvolume.
Eur Heart J. 2008;29:2343-2350.
30. Jankowska EA, Rozentryt P,Witkowska A, et al.
Iron deficiency: an ominous sign in patientswith systolic chronic heart failure.
Eur Heart J. 2010;31:1872-1880.
31. Okonko DO, Mandal AK,Missouris CG, Poole-Wilson PA.
Disordered iron homeostasis in chronic heartfailure: prevalence, predictors, and relationto anemia, exercise capacity, and survival.
J Am Coll Cardiol. 2011;58:1241-1251.
32. Jankowska EA, Drohomirecka A,Ponikowska B, et al.
Deficiencies in circulating testosterone anddehydroepiandrosterone sulphate, and de-pression in men with systolic chronic heartfailure.
Eur J Heart Fail. 2010;12:966-973.
33. Anand IS, Kuskowski MA, RectorTS, et al.
Anemia and change in hemoglobin overtime related to mortality and morbidity inpatients with chronic heart failure: resultsfrom Val-HeFT.
Circulation. 2005;112:1121-1127.
34. Jankowska EA, Rozentryt P,Witkowska A, et al.
Iron deficiency predicts impaired exercisecapacity in patients with systolic chronicheart failure.
J Card Fail. 2011;17:899-906.
35. Jankowska EA, Witkowska A,Drohomirecka A, et al.
Iron deficiency predisposes to depression inmen with systolic heart failure.
Eur J Heart Fail. 2012. In press.
36. Tang WH, Tong W, Jain A, et al.
Evaluation and long-term prognosis of new-onset, transient, and persistent anemia in am-bulatory patients with chronic heart failure.
J Am Coll Cardiol. 2008;51:569-576.
37. von Haehling S, Schefold JC,Hodoscek LM, et al.
Anaemia is an independent predictor of deathin patients hospitalized for acute heart failure.
Clin Res Cardiol. 2010;99:107-113.
38. van der Meer P, Lok DJ, Januzzi JL,et al.
Adequacy of endogenous erythropoietin levelsand mortality in anaemic heart failure patients.
Eur Heart J. 2008;29:1510-1515.
39. Varma A, Appleton DL, Nusca A,et al.
Iron deficiency anemia and cardiac mortalityin patients with left ventricular systolic dysfunction undergoing coronary stenting.
Minerva Cardioangiol. 2010;58:1-10.
40. Stamos TD, Silver MA.
Management of anemia in heart failure.
Curr Opin Cardiol. 2010;25:148-154.
41. Ghali JK, Anand IS, Abraham WT,et al; Study of Anemia in Heart FailureTrial (STAMINA-HeFT) Group.
Randomized double-blind trial of darbepoetinalfa in patients with symptomatic heartfailure and anemia.
Circulation. 2008;117:526-535.
42. Kotecha D, Ngo K, Walters JA,Manzano L, Palazzuoli A, Flather MD.
Erythropoietin as a treatment of anemia inheart failure: systematic review of random-ized trials.
Am Heart J. 2011;161:822-831.
292
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 292

43. Lawler PR, Filion KB, EisenbergMJ.
Correcting anemia in heart failure: the effi-cacy and safety of erythropoiesis-stimulatingagents.
J Card Fail. 2010;16:649-58.
44. Singh AK, Szczech L, Tang KL, et al; CHOIR Investigators.
Correction of anemia with epoetin alfa inchronic kidney disease.
N Engl J Med. 2006;355:2085-2098.
45. Drüeke TB, Locatelli F, Clyne N,et al; CREATE Investigators.
Normalization of hemoglobin level in patientswith chronic kidney disease and anemia.
N Engl J Med. 2006;355:2071-2084.
46. Besarab A, Bolton WK, Browne JK,et al.
The effects of normal as compared with lowhematocrit values in patients with cardiacdisease who are receiving hemodialysis andepoetin.
N Engl J Med. 1998;339:584-590.
47. Pfeffer MA, Burdmann EA, Chen CY, Cooper ME, et al; TREATInvestigators.
A trial of darbepoetin alfa in type 2 diabetesand chronic kidney disease.
N Engl J Med. 2009;361:2019-2032.
48. Szczech LA, Barnhart HX, Inrig JK,et al.
Secondary analysis of the CHOIR trial epoetin-alpha dose and achieved hemoglobinoutcomes.
Kidney Int. 2008;74:791-798.
49. Solomon SD, Uno H, Lewis EF, et al; Trial to Reduce CardiovascularEvents with Aranesp Therapy (TREAT)Investigators.
Erythropoietic response and outcomes inkidney disease and type 2 diabetes.
N Engl J Med. 2010;363:1146-1155.
50. Coyne DW, Kapoian T, Suki W, et al; DRIVE Study Group.
Ferric gluconate is highly efficacious inanemic hemodialysis patients with highserum ferritin and low transferrin saturation:results of the Dialysis Patients’ Response toIV Iron with Elevated Ferritin (DRIVE) Study.
J Am Soc Nephrol. 2007;18:975-984.
51. Kapoian T, O'Mara NB, Singh AK,et al.
Ferric gluconate reduces epoetin requirementsin hemodialysis patients with elevated ferritin.
J Am Soc Nephrol. 2008;19:372-379.
52. McMurray JJ, Anand IS, Diaz R,et al; RED-HF Committees andInvestigators.
Design of the Reduction of Events with Dar-bepoetin alfa in Heart Failure (RED-HF):a Phase III, anaemia correction, morbidity-mortality trial.
Eur J Heart Fail. 2009;11:795-801.
53. Jankowska EA, Ponikowski P.
Molecular changes in myocardium in thecourse of anemia or iron deficiency.
Heart Fail Clin. 2010;6:295-304.
293
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Should anemia be actively treated in cardiorenal syndrome? - Jankowska and Ponikowski
DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 293

DCVM 62 Three Expert Answer:Mise en page 1 23/03/12 11:29 Page 294

Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
295
n this “Lexicon of the Heart” Fas-cinoma article, we look at letter“H” for the heart and “K” for thekidney. And first, as with any prop-
er lexicon or dictionary, a few wordsabout etymology. Of course, there areno Latin or Greek roots in Chinese,one must go all the way back to thelate Shang Dynasty (1200-1050 BCE)and the earliest characters found onritual bronze vessels and the so-called“oracle bones” (often ox shoulderblades) used for divination purposes.Actually, the character for heart (xin,心) has hardly evolved at all since itsfirst appearance. Figure 1 shows theancient form of the character (left),and the form as painted with a brush(right), which is quasi identical to theprinted form (心).
According to Léon Wieger’s “ChineseCharacters” published in 1915,1 whichis based on ancient Chinese etymo-logical treatises and is to this day oneof the best sources for etymology in aEuropean language, the early form“represents the heart with, on top, thepericardium opened; in the middle,the organ; at the bottom, a summarydelineation of the aorta.”
The character for kidney (shen, 腎) isin three parts; the bottom part is the“classifier” or “radical” for “flesh,” “meat”(rou, 肉, 月), which represents piecesof smoke-dried meat (the two invert-ed “Vs”) gathered in a bundle (theround “envelope” around them). 肉 isthe character occurring independent-ly, 月 is the form used in compoundcharacters, as in “kidney,” consideredas belonging in the general categoryof “meaty” objects (see Figure 2 below,left panel: left, the ancient characters,right the brush scripts). The middlepanel represents “chen” (臣), a “minis-ter, attendant on a prince; the charac-ter, which is straightened in modernwriting (top), represents the ministerprostrate before his master (left, bot-tom). To this character is added a hand(shown in the right panel in the an-cient form with three fingers [top], andas又 in brush script [bottom]): hencethe meaning becomes: to have a hold(the hand) on one’s ministers/vas-sals/men. This meaning then evolvedto signify “firm, solid” (right panel). In total, if we now look at the com-plete character composed of the threeparts described above, the meaning is“a fleshy organ that is very firm”—I’msure you will admit that it’s quite anadequate description of a kidney!
The following is just a brief foray intohow the ancient Chinese understoodthe function of the heart and kidneys,by means of three examples from threedifferent medical works from the 17th-18th centuries, although “real dates”of first authorship are very difficult toascertain, as is often the case in China,since successive generations of authorskept building upon earlier editions.
THE HEART
Sancai Tuhui (三才圖會) or CollectedIllustrations of the Three Realms, byMing dynasty (1368-1644) author WangSiyi (王思義),2 was an encyclopediapublished in 1609. “Sancai” refers tothe three realms of heaven (天), earth(土), and man (人), in other words “ev-erything,” and “Tuhui” (圖會) means“collection of illustrations.”
Figure 3 (page 296) shows the formand position of the heart, and the ac-companying text states that it is situ-ated beside the 5th vertebra, belowthe lung, above the diaphragm. Theheart (xin, 心) is fed by the aorta, (thelarge vertical conduit), and from theheart issue four other smaller arteriesto the lung (fei, 肺), spleen (pi, 脾),kidneys (shen, 腎), and liver (gan, 肝).
I
A Lexicon of the HeartHeart and kidney in early Chinese medicine
Frederick Scheffler, MDRamsey County Lane - St Paul - Minnesota - USA
Address for correspondence:Frederick Scheffler, MD, Ramsey County Lane,St Paul, Minnesota, USA (e-mail: [email protected])Dialogues Cardiovasc Med. 2011;16:295-298
Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
Figure 1.
Figure 2.
DCVM 62 Fascinoma:DCVM n°48, Fascinoma 23/03/12 11:32 Page 295

These five organs constitute the “vis-cera,” (zang, 臟), over which the heart“rules,” thus being so to speak a “primusinter pares.” Traditional Chinese Med-icine (TCM) divides the body’s organsinto two categories, the five “zang,” aslisted above, which are “yin” (陰) innature, and whose main function is tostore “energy” or “Qi” (氣) and blood(xie, 血).
The other category is that of the six“entrails,” receptacles,” or “bowels”(fu, 腑), which are considered to be“yang” (陽) in nature, and which arethe small intestine (xiaochang, 小腸),large intestine (dachang, 大腸), gall-
bladder (dan, 膽), urinary bladder(pangguang, 膀胱), stomach (wei, 胃),and “triple warmer,” “sanjiao” (三焦),thought by some to refer to the para-sympathetic nervous system.
THE KIDNEY
“Problem 36” (Figure 4, from Tu ZhuBa Shi Yi Nan Jing Bian Zhen (圖註八十一難經辨真) or Corrected Editionof the Canon of 81 Problems, Illustra-ted and Annotated, published in theWan Li reign period of the Ming Dy-nasty (1573-1620) by Zhang Shixian(張世賢),3 illustrates the distinct phys-iological functions of the left and right
kidneys in Chinese medical theory.The left kidney (shen, 腎), partakes ofthe nature of water (shui, 水), whilethe right kidney, (mingmen, 命門), ie,Portal of Life) partakes of the natureof fire (huo, 火). The “mingmen” is cru-cial to life; it is the place where innateQi (氣) is stored, the origin of life pro-cesses, the very root of existence. Thefire in “mingmen” is expressed in theyang (陽) functions of the kidneys (inmodern times, taken to include thefunction of the adrenal gland). Therewere two views of the “mingmen” inancient Chinese medicine. Accordingto one theory, it corresponded to theright kidney; according to the other, it
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Heart and kidney in early Chinese medicine - Scheffler
296
Figure 3. Woodcut illustration from the Collected Illustrations of the Three Realms (1609). Library of the China Academy of Traditional Medicine, Beijing. © Wellcome Library.
Figure 4. Woodcut depicting the kidneys; illustration of “Problem36” from the Corrected Edition of the Canon of 81 ProblemsIllustrated and Annotated. This edition is dated 1573 to 1620. Libraryof the China Academy of Traditional Chinese Medicine. © Wellcome Library.
DCVM 62 Fascinoma:DCVM n°48, Fascinoma 23/03/12 11:32 Page 296

corresponded to both kidneys, as em-bodied in the dynamic interchange ofQi between them. The first theory isrepresented in this diagram.
“CARDIORENAL”?
The Shang Han Lun (傷寒論) or ShangHan Za Bing Lun (傷寒雜病論),known in English as the Treatise onCold Damage Disorders or the Treatiseon Cold Injury,4 is a Chinese medicaltreatise that was compiled by ZhangZhongjing (張仲景) sometime beforethe year 220 BC, at the end of the Handynasty. It is the oldest complete clini-cal textbook in the world. Composedof 12 volumes, the book has 397 sec-tions with 112 herbal prescriptions. Itorganizes all the diseases into the sixdivisions called "six channels," basedon the ways treatment can be appliedaccordingly.
Of all of China’s early medical classics,the Shang Han Lun is undoubtedlythe one with the greatest relevance tothe modern practice of Chinese medi-cine, and the one most deserving ofWestern attention. It was the first bookto attempt to incorporate medicinaltherapy into the medicine of system-atic correspondences and channelsand network vessels. Far ahead of itstime in both theory and practice, it isnot surprising that the prescriptionsit contains comprise an importantpart of today's medicinal formulary.
Figure 5 illustrates the ways in whichpathologies of the three “yin” (陰) chan-nels of the hand and foot are mani-fested in the inner areas of the body.
The hand “greater yin” (taiyin, 太陰)channel is related to disorders of thelungs; the hand “absolute yin” (jueyin,絶陰) channel is related to disordersof the heart envelope; the foot “taiyin”channel is related to disorders of thespleen; the foot “jueyin” channel isrelated to disorders of the liver; thefoot “lesser yin” (shaoyin, 少陰) chan-
nel is related to disorders of the kid-neys, etc, ie, each channel governs aparticular internal pathology.
CONCLUSION
To talk about a pathophysiologicalentity such as “cardiorenal syndrome”in early Chinese medicine—the termin modern Chinese is “xinshenzonghe-bing” (心腎綜合病, where you nowrecognize the first two characters as“heart” and “kidney”)—would be prom-ising more than one can deliver.
And yet, one of the central tenets ofChinese medicine since its incep-tion—as described in one of the ear-liest treatises, the Huangdi Neijing(黃帝內經) the “Yellow Emperor’sClassic of Medicine,5,6” dated between475 BCE and 221 CE—was the beliefthat all the body’s organs were physi-ologically and pathophysiologicallyinterrelated. For them, the organs were
ruled by the cyclic concepts of “yin”(陰) (= female, dark, wet, cold, moon)and “yang” (陽) (= male, bright, dry,warm, sun), influenced each other’sfunctions, and produced and received“energy” (Qi, 氣) from one another,which circulated in “canals,” the “merid-ians” familiar to those who know athing or two about acupuncture. “Qi”and the concepts of “yin” and “yang”constituted a far more sophisticatedand realistic theory than that of the“four humors” of ancient Greece, cham-pioned by Hippocrates (ca 460 BC toca 370 BC), and which remained theprevailing view of the (patho)physiol-ogy of the human body in Westernmedicine, only to finally die out in the19th century. In fact, traditional Chi-nese physiology anticipated by morethan two millennia the discovery of the“milieu intérieur” by Claude Bernard(1813-1878), renamed “homeostasis” byAmerican physiologist Walter Cannon(1871-1945).
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Heart and kidney in early Chinese medicine - Scheffler
297
Figure 5.Depicted inred (coloradded) arethe heart(心), abovethe twokidneys (腎).Woodcutillustrationfrom an editionof 1724 (QingDynasty).Library of theChina Academyof TraditionalChineseMedicine. © WellcomeLibrary.
•••
DCVM 62 Fascinoma:DCVM n°48, Fascinoma 23/03/12 11:32 Page 297

REFERENCES
1. Wieger L (SJ).
Chinese Characters: Their Origin, Etymology,History, Classification, and Signification. AThorough Study From Chinese Documents.
2nd ed. New York, NY: Paragon ReprintCorp/Dover Publications. 1927.
2. Wang Siyi.
Collected Illustrations of the Three Realms.(明)王圻王思義輯. 三才圖會 (一).
China-America Digital Academic Library(CADAL). 北京大學圖書館. UniversalLibrary. www.archive.org/details/02098268.cn.
3. Zhang Shixian.
Corrected Edition of the Canon of 81Problems, Illustrated and Annotated.(明)張世賢撰. 圖注八十一難經辨真 (一).
China-America Digital Academic Library(CADAL). 北京大學圖書館. UniversalLibrary. www.archive.org/details/02092757.cn.
4. Zhang Zhongjing, Zhang Chen.
Treatise on Cold Damage Disorders. (清) 張辰注. 傷寒論 (一).
China-America Digital Academic Library(CADAL). 北京大學圖書館. UniversalLibrary. www.archive.org/details/02092808.cn.
5. Wu Kun.
Yellow Emperor’s Classic of Medicine. Basic Questions. (明) 吳崑注.皇帝內經素問 (一).
China-America Digital Academic Library(CADAL). 北京大學圖書館. UniversalLibrary. www.archive.org/details/02092694.cn.
6. Maoshing Ni.
The Yellow Emperor’s Classic of Medicine.A New Translation of the Neijing SuwenWith Commentary.
Boston, MA: Shambhala; 1995:1-316.
298
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Heart and kidney in early Chinese medicine - Scheffler
DCVM 62 Fascinoma:DCVM n°48, Fascinoma 23/03/12 11:32 Page 298

299Copyright © 2011 LLS SAS. All rights reserved
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
1 6
Hormones and hemodynamics in heart failureR. W. Schrier, W. T. Abraham. N Engl J Med. 1999
2
Renal function as a predictor of outcome in a broad spectrum of patients
with heart failure H. L. Hillege et al. Circulation. 2006
8
Summaries of Ten Seminal PapersPaul R. Kalra, MD, FRCP; Philip A. Kalra, MD, FRCP
Department of Cardiology - Portsmouth Hospitals NHS Trust - Porstmouth - UK ([email protected]) Department of Nephrology - Salford Royal Foundation NHS Trust - Salford - UK ([email protected]
Dialogues Cardiovasc Med. 2011;16:299-310
4Albuminuria and risk of cardiovascular events,
death, and heart failure in diabetic and nondiabetic individuals
H. C. Gerstein. JAMA. 2001
9Cardiorenal syndrome
C. Ronco et al. J Am Coll Cardiol. 2008
Ferric carboxymaltose in patients with heart failure and iron deficiency
S. D. Anker et al. N Engl J Med. 2009
10
The severe cardiorenal syndrome: “Guyton revisited”
L. G. Bongartz et al. Eur Heart J. 2005
7
5
The use of subcutaneous erythropoietin and intravenous iron for the treatment
of the anemia…D. S. Silverberg et al. J Am Coll Cardiol. 2000
3
Selection of seminal papers by Paul R. Kalra, MD, FRCP; Philip A. Kalra, MD, FRCP
[email protected] - [email protected]
www.dialogues-cvm.org
Arterial media calcification in end-stage renal disease: impact on all-cause and
cardiovascular mortalityG. M. London et al. Nephrol Dial Transplant. 2003
Cardiorenal Syndrome
The clinical epidemiology of cardiac disease in chronic renal failure
P. S. Parfrey, R. N. Foley. J Am Soc Nephrol. 1999
Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization
A. S. Go et al. N Engl J Med. 2004
Highlights of the years by Ian Mudway, MDLung Biology - Division of Life Sciences Franklin Williams Building
150 Stamford Street - London SE1 9NN - UK
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 299

John F. Kennedy Jr and his wife are killed whentheir plane crashes off the coast of Martha’s
Vineyard; Lance Armstrong wins his first Tour deFrance; and Moroccan middle distance runner
Hicham El Guerrouj breaks the world mile recordin a time of 3:43:13 minutes
1999
300
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
n the 1990s, these two authors forged a strong research partnership in St John’s, Newfoundland,Canada, one which focused on the nature and epi-demiology of cardiovascular disease that occurs inpatients with advanced chronic renal disease. They
had been involved in several important original studiesincluding a seminal investigation of the evolution of echo-cardiographic changes in over 250 patients commencingdialysis, and then followed for over 2 years. They are cur-rently both heralded as leading experts in this field; Dr Foleynow works in Minneapolis, Minn, USA. Although this par-ticular article was a review and not an original study, itwas very important in comprehensively summarizing thelatest evidence of the time relating to the heterogeneouscardiovascular diseases suffered by patients receivingdialysis. Prior to this period, the majority of nephrologistswould more often direct their clinical attention to dialysis-related complications, dialysis membranes and process,and acute renal failure (now known as acute kidney injury)or their research interests to the pathophysiology of therelatively rare, but intellectually stimulating, glomerulardiseases, rather than to the cardiovascular disease, whichwas by far the biggest killer of their patients.
The review stressed the high relative mortality of dialysispatients—stark data from the United States Renal DataSystem (USRDS), which showed young dialysis patients (eg,25-30 years old), male or female, having a 100-200-fold in-creased death risk compared with similar aged normal in-dividuals, a mortality risk close to that experienced by 85-year-old individuals in the general population, which is anincredible statistic. Of these deaths, 50% are thought tobe due to cardiac causes, and the authors described thepathophysiological changes contributing to cardiovasculardisease in advanced kidney disease. The review empha-sized the importance of “nontraditional” risk factors—ie,not the usual diabetes, smoking, coronary artery atheromaand family history—with abnormalities such as left ven-tricular hypertrophy and dilatation, arterial stiffness andvascular calcification, inflammation, and especially heartfailure being cited as risk factors of major importance indialysis patients. Comparative epidemiology of cardiac
changes in hemodialysis and peritoneal dialysis patientsshowed that the former was more likely to lead to progres-sive increases in left ventricular muscle mass and ventricu-lar volume, forerunners of cardiac failure, which itself wasappearing as one of the major risk factors for death in dial-ysis populations. On the other hand, evidence from certainstudies that renal transplantation could improve these car-diac changes was cited, and was welcome relief from therather depressing data summarized throughout the review.At the time, topics such as vascular calcification, hypovi-taminosis D, and sudden cardiac death (now thought toaccount for a quarter of all dialysis deaths) were only justemerging in the renal literature, and hence were given littlemention in the article. Now it would be difficult to attend aconference without finding at least one session devotedto each of these topics. Another limitation was that inter-ventional strategies to ameliorate the cardiovascularchanges were only given minimal consideration in the pa-per, but this more reflected that randomized clinical trialsand other studies of therapeutic interventions for patientswith advanced renal failure had been overlooked by therenal community, especially in comparison with the trialportfolio that was appearing in cardiology and diabetology.Nevertheless, the manuscript provided the nephrologistwith a comprehensive summary of the epidemiology andpathogenesis of the cardiovascular disease burden sufferedby dialysis patients, bringing this to the fore as a subjectfor future research and of great importance in patient man-agement. Subsequently, there has been a major prolifera-tion of interest in this area, which is ever increasing.
Philip Kalra
I
The clinical epidemiology of cardiac disease in chronic renal failure
P. S. Parfrey, R. N. Foley
J Am Soc Nephrol. 1999;10:1606-1615
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 300

301
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
o why does a review article make into the top 10,when there are so many excellent scientific papersaround the cardiorenal syndrome? Well this is anabsolute belter, an all-time favorite of mine! Schrierand Abraham present a clear and succinct over-
view of what was understood at the time regarding thepathophysiology of chronic heart failure, with a focus onabnormal hemodynamics and neurohormonal activation.From a personal perspective it has been highly influential;as a callow youth I remember reading this at the time ofpublication (1999) and suddenly becoming excited aboutheart failure, which until then I had thought of (quite in-correctly) as a “Cinderella specialty.” Furthermore, largeamounts of the original scientific data referenced in thisreview are the work of the two authors and this article high-lights the crucial role they have played in understandingthe pathophysiology of heart failure, and the subsequentcontribution to improved patient outcomes. Although thisarticle is now over a decade old, if you have any input intothe clinical management of patients with chronic heartfailure (or chronic kidney disease) it is still most worthy ofa bedtime read. All of this is achieved in just 7 pages oftext and figures—for this in itself the authors should bewholeheartedly congratulated.
The review focuses on fluid and electrolyte metabolism inheart failure and therefore inevitably brings the heart andthe kidney together. The article is accompanied by a num-ber of relatively simple, but extremely useful, figures, whichadd to the clarity of explanation. The hemodynamic focusis on arterial underfilling and includes discussion aroundthe afferent sensing mechanisms and the subsequent neu-rohormonal activation. A key innate response to any threator disease process is to maintain arterial integrity. Thesame afferent and efferent systems come into play irrespec-tive of the threat to the circulation and thereby this formsa unifying hypothesis of the regulation of body fluid statusin edematous states (ie, this is applicable to disordersother that heart failure, for example, cirrhosis).
Subsequent sections detailing activation of the sympatheticnervous system, renin-angiotensin-aldosterone system,
and other hormones (eg, nonosmotic release of vasopressin)capture the crucial link between an abnormality in cardiacfunction and the subsequent impact on the function ofthe kidney and its various responses. Schrier and Abrahamhighlight the adverse impact of neurohormonal activationon sodium and water retention (performed by the kidney)and hemodynamics (such as arterial vasoconstriction andincreased afterload). In addition, they introduce the con-cept that angiotensin II and aldosterone in particular havefurther direct detrimental effects on heart and kidney struc-ture and function. Understanding these abnormalities isfundamental to understanding the mainstay of the con-temporary management of chronic heart failure (that is, howangiotensin-converting enzyme inhibitors or angiotensinreceptor blockers, β-blockers, and aldosterone antagonistsexert their benefits). Ever since this publication we havemore data supporting the beneficial use of these agentsfor nearly all stages of chronic heart failure secondary toleft ventricular systolic dysfunction. In many respects it isremarkable to see just how far we have come in improvingthe outcomes for patients with chronic heart failure overthe last 2 to 3 decades. This is one of the major successstories in modern medicine, although of course there ismuch more to discover and hopefully this will lead ontonovel treatments that will further advance care. However, I don’t believe this would have been achieved without aclear understanding of the basic pathophysiological prin-ciples of hormones and hemodynamics in heart failure!
Paul Kalra
S
A total solar eclipse occurs in Europe and Asia;more than 17 000 are killed and 44 000 injured
when a 7.4-magnitude earthquake strikes Istanbul and northwestern Turkey; and
a brief war is triggered when Chechen guerrillas invade the Russian republic of Dagestan
1999
Hormones and hemodynamics in heart failure
R. W. Schrier, W. T. Abraham
N Engl J Med. 1999;341(8):577-585
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 301

his paper was instrumental in igniting the cur-rent interest in the area of anemia and heartfailure. Despite the obvious limitations of aretrospective cohort study and a small unblind-ed intervention study (n=26) that was not place-
bo controlled, the results captured the enthusiasm of theheart failure community worldwide. The rest as they say ishistory! A second study by the same group published sev-eral months later in the same journal reinforced these find-ings (Silverberg et al. J Am Coll Cardiol 2001;37(7):1775-1780). Up until this stage it had been recognized that lowhemoglobin was seen in patients with chronic heart failure,but there had been scant attention paid to the possibleimpact on outcomes and potential correction. Indeed, bythe very fact that mild anemia was so common it appearedto have become accepted as the “norm” in clinical practice.
The authors evaluated patients attending a specialized heartfailure clinic (n=142) and detailed that 56% were anemic(hemoglobin <12 g/dL). Low hemoglobin was more preva-lent in highly symptomatic individuals (New York HeartAssociation [NYHA] Class II 19%; Class III 53%; and Class IV79%). Twenty-six highly symptomatic patients (NYHA Classof III or more) despite maximal tolerated standard therapywith hemoglobin <12 g/dL entered the intervention study(essentially a proof of concept or feasibility study). Theywere truly sick and were receiving high doses of oral or in-travenous loop diuretics and had required frequent recenthospitalizations. Treatment consisted of intravenous ironand subcutaneous erythropoietin for a mean of 7.2±5.5months. Intravenous iron sucrose was given in a dose of200 mg every week until serum ferritin reached 400 μg/Lor iron saturation reached 40%. Erythropoietin was givensubcutaneously on a weekly basis at a dose that attemptedto maintain a target hemoglobin of 12 g/dL. During thestudy, drugs used for treatment of heart failure were unal-tered, except diuretics, which were adjusted according toclinical status.
Treatment was feasible and tolerated, resulting in an in-crease in hemoglobin from 10.16±0.95 g/dL at baseline to12.20±1.21 g/dL at the end of the study (P<0.001). This
was associated with a remarkable reduction in diuretic re-quirement and hospitalizations (91%reduction as comparedwith a similar time period prior to the study). Left ventricularejection fraction and NYHA class were both seen to sig-nificantly improve. The authors concluded that mild ane-mia was extremely common and its correction may be animportant addition to the treatment in chronic heart failure.
Despite the limitations in design, as already mentioned,this landmark study paved the way for a number of smallrandomized studies evaluating the use of erythropoietin-stimulating agents (ESA) and/or intravenous iron. Larger-scale studies have subsequently been initiated: see FAIR-HF(Ferinject Assessment in patients with IRon deficiency andchronic Heart Failure) evaluating intravenous iron therapy,is discussed by Ewa A. Jankowska and Piotr Ponikowski inthis issue. The result of RED-HF (Reduction of Events withDarbepoetin alfa in Heart Failure), which is evaluating theimpact of ESA in patients with chronic heart failure is ea-gerly awaited.
Don Silverberg and colleagues from the departments ofnephrology and cardiology at the Tel Aviv Medical Centerwere instrumental in highlighting the importance of anemiaand iron deficiency in chronic heart failure. They identifiedpotential benefits of this therapeutic approach and alsonoted the relation between heart failure, anemia, and chron-ic kidney disease, introducing the concept of “cardio-renal-anemia syndrome” or CRAS. The investigators have alsohighlighted the achievements that can be made when car-diologists and nephrologists actually develop a symbioticrelationship!
Paul Kalra
302
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestiveheart failure improves cardiac and renal function and functionalcardiac class, and markedly reduces hospitalizationsD. S. Silverberg, D. Wexler, M. Blum, G. Keren, D. Sheps, E. Leibovitch, D. Brosh, S. Laniado, D. Schwartz, T. Yachnin, et alJ Am Coll Cardiol. 2000;35(7):1737-1744
T
A preliminary draft of the Human Genome is published; South Korean President Kim
Dae Jung visits North Korea; and Tiger Woods wins the US Open by a record 15 shots
2000
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 302

303
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
tatisticians and methodologists usually scoff at theimportance and results of post-hoc analyses, forprotean reasons including lack of power for theanalysis, ascertainment bias, and because the analy-ses were not preconsidered in the study design.
Having had some experience in the design of large trials,observing the flimsy initial data upon which the primaryoutcome measure might sometimes be based, the guess-work that can be involved in arriving at the effect size of onetreatment versus another, and the way in which secondaryoutcome measures can be selected, I would take an oppos-ing view. All studies are expensive to run, especially ran-domized control trials (RCT) whose costs can run into tensof millions, but most importantly, patients willingly givetheir consent and time to participate and without themthere would be no clinical research. For the latter two rea-sons I believe that the output from RCT should be maxi-mized. Most of all, we owe it to the patients to find out allwe can from a study to help guide their appropriate treat-ment in the future.
To move away from this particular soapbox it then natu-rally follows that this paper, a post-hoc analysis of HOPE(Heart Outcomes Prevention Evaluation), provides signifi-cant clinical insights that have changed our thinking withregard to the importance of microalbuminuria in relation tohard clinical outcomes in both high-risk nondiabetics anddiabetics. The HOPE study randomized 9000 individualswithout diabetes, but with cardiovascular disease, or withhigher-risk diabetes (cardiovascular disease, high choles-terol, smoking, or other risk factors) to treatment with ei-ther ramipril or placebo, to examine the effects upon all-cause mortality, myocardial infarction or stroke, and heartfailure hospitalization. The main trial result showed thatall patients were benefited by ramipril. Subsequent analy-ses showed that the diabetic subgroup (MICRO-HOPE)had reduced cardiovascular events and progression tonephropathy when treated with the active agent, whereasan analysis of baseline albuminuria (only in or below themicroalbuminuric range, as patients with dipstick-positiveproteinuria, ie, likely macroproteinuria, were excluded)demonstrated the negative effects of microalbuminuria
upon outcomes in all patients, including nondiabetics. Morespecifically, this post-hoc analysis showed that all end-points were more likely to occur in both nondiabetics anddiabetics, and there was a clear relationship between riskand increasing quantity of microalbuminuria. The hazardratios relating albuminuria to risk were greatest for hospi-talization for heart failure. Most strikingly, when patientswere divided into quartiles dependent upon their baselinelevel of microalbuminuria, it was clear that there was acontinuum of increasing risk related to increasing albumin-uria even when this was well below the cutoff value usedfor diagnosis of early diabetic nephropathy (a urinary al-bumin creatinine ratio (uACR) of >2 mg/mmol)—ie, belowthe conventional microalbuminuric range. Hence, diabeticsand nondiabetics with a uACR of >0.5 mg/mmol (crudelyequating to only 5 mg/L) had a significantly increased riskof death or cardiovascular events compared with thosewith negligible albuminuria. There were major limitationswithin the paper; the authors acknowledged that there hadbeen only one baseline uACR available for study, and thehypothesis linking microalbuminuria to increased risk wasrather weakly stated, suggesting this was likely to repre-sent generalized vascular permeability and “endothelialdysfunction.” Nevertheless, the study really did change ourmind-set regarding the importance of albuminuria as anindependent adverse risk factor in the higher-risk generaland diabetic populations, and the fact that it confers acontinuum of risk even below the microalbuminuric range.
Philip Kalra
S
Albuminuria and risk of cardiovascular events, death, and heartfailure in diabetic and nondiabetic individuals
H. C. Gerstein, J. Mann, Q. Yi, B. Zinman, S. F. Dinneen, B. Hoogwerf, J. P. Hallé, J. Young, A. Rashkow, C. Joyce, et al; Hope Study Investigators
JAMA. 2001;286(4):421-426
Simeon Saxe-Coburg-Gotha, the last Tsar ofBulgaria, is sworn in as Prime Minister followingthe election; novelist Jeffrey Archer is sentenced
to four years in prison for perjury; and the London Stock Exchange goes public
2001
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 303

304
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
ith the dawn of the new millennium itwas becoming increasingly recognizedthat arterial and valvular calcificationswere frequently present in dialysis pa-tients, and possibly related to the quan-
tity of calcium imbibed by patients in phosphate binders.French renal research groups were leaders in this field,and Gerard London, together with his former colleaguesBlacher and Safar, had previously demonstrated the rela-tionship between the extent of vascular calcification andmortality in end-stage renal disease. They had been pio-neers in changing our thinking about the importance of thestate of the arterial wall in renal patients, and had helpedintroduce noninvasive measurement of arterial stiffnessas a parameter that could quantitate the “hardening” ofthe vessel wall. Hence, their studies had found a close relationship between pulse wave velocity and mortality indialysis patients, which provided a plausible mechanismby which vascular calcification could lead to cardiac dam-age and then mortality.
The study reported in this article was led by London at adialysis center in Fleury-Merogis, France, and it focused onthe precise location of the calcification within vessel walls.Two hundred and two hemodialysis patients were includ-ed in what was a simple investigative and analytical studydesign. All patients had undergone a plain radiograph ofthe pelvis and/or thigh, and the type of calcification wasqualitatively classed as being intimal (arterial intimal calcification, AIC) or medial (arterial medial calcification,AMC) by two observers. The presence or absence of vas-cular calcification, and particularly the differing type ofvessel calcification, was then considered in relation to arange of basic clinical parameters and to long-term mor-tality. However, it was not clear within the paper whetherpatients had undergone baseline (at dialysis commence-ment) radiographs in protocolled fashion, or more likely,if patients who had previously undergone x-ray study weresimply a “convenience sample,” ripe for study. The key find-ings of the study were that any calcification was associatedwith a higher risk of mortality than no calcification, andthat any calcification was associated with increased dose
of oral calcium-containing phosphate binder and durationof time receiving dialysis.
A crucial observation was that there were major differencesbetween the two patterns of calcification. AIC was associ-ated with older age, prior cardiovascular disease at timeof commencing dialysis, and with diabetes or atheroscle-rotic etiologies of the renal disease. In contrast, AMC wasassociated with younger patients, who typically had noconventional cardiovascular risk factors, longer durationof dialysis, and greater calcium dosage in terms of calciumcarbonate. The mortality was high with both calcificationpatterns, although patients with AMC lived longer thanAIC, which was partly explained by age. The authors con-cluded that AIC tended to develop in patients prone toatheroma, the calcification being present on the surface ofintimal plaques. In contrast, all dialysis patients would beat risk of developing AMC due to perturbations of calcium-phosphate balance, calcium dose in binders, and otherfactors. Although this study used basic techniques to as-sess calcification, now superseded by quantitative tech-niques such as CT calcification score, it was fundamentalin changing our thinking with regard to the epidemiologyof vascular disease in dialysis patients.
Philip Kalra
Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality
G. M. London, A. P. Guerin, S. J. Marchais, F. Metivier, B. Pannier, H. Adda
Nephrol Dial Transplant. 2003;18(9):1731-1740
W
The foreign minister of Sweden, Anna Lindh, is fatally stabbed while shopping;Sweden rejects adopting the euro
in a referendum; and American singer-songwriterJohnny Cash dies at the age of 71
2003
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 304

305
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
ertainly, the sheer scale of the numbers ofsubjects in this study gets it into the top 10!The message is also crucial and this paper hashelped highlight the adverse and independ-ent impact of chronic kidney disease (CKD)—
even when mild—on adverse cardiovascular outcomes.The data are derived from a registry of a large integratedhealth care system (insured) within the San Francisco BayArea. The authors acknowledge that the data therefore maynot be representative of other cohorts/regions (do Califor-nians see themselves as anything other than normal?).While there are always limitations in such data sets, thishad huge advantages not just in terms of numbers, butalso the extent of other data related to cardiovascular riskand lifestyle that were available.
1 120 295 adults with an estimated glomerular filtrationrare (eGFR) were included in the analysis. Previous data haddocumented that patients with end-stage renal failure ex-perienced extraordinarily high cardiovascular event rates.However, until this megastudy was published there wererelatively limited data suggesting that mild impairment ofrenal function might be associated with adverse cardiovas-cular outcomes, and it was uncertain as to whether anyrelation was independent of conventional cardiovascularrisk factors.
The median follow up was 2.84 years giving over 3.1 millionsubject-years of follow-up! During follow-up, 3171 subjectsbegan dialysis. In contrast, there were 51 424 deaths and138 291 cardiovascular events. Subjects were grouped according to their eGFR. A value of �60 mL/min/1.73m2
formed the reference (and lowest-risk) group. The impactof a reduction in renal function (eGFR) on outcomes in-cluding all-cause mortality and (separately) cardiovascularevents (hospitalization for coronary heart disease, heartfailure, ischemic stroke, or peripheral vascular disease)was assessed. Multivariable statistical models correctedfor a multitude of sociodemographic (eg, age, sex, income,education) factors and clinical variables (eg, history of is-chemic heart disease, heart failure, diabetes, hypertension,dyslipidemia, etc).
The key finding was that a consistent independent pro-gressive worsening of risk was seen as renal function de-teriorated. While an excess risk was present in those sub-jects with even a mild reduction in eGFR (45-59 mL/min/1.73m2), a particular step-up in risk was seen for thosesubjects in CKD stage 3B or worse. For example, when con-sidering cardiovascular events a doubling of risk was seenfor subjects in stage 3B (eGFR 30-44 mL/min/1.73m2) ascompared with the reference group. This study firmly es-tablished impaired renal function (ie, CKD) as a risk factorfor all-cause death and the development of adverse cardio-vascular events. Enhanced risk was seen in subjects witheven mild renal impairment, with values of serum creatinineor eGFR that perhaps would have previously been clinicallyoverlooked. While this study has been unable to distin-guish whether CKD is merely a marker of advanced risk ora modifiable risk factor, it has I believe stimulated a majorsea change in clinical practice. Much greater attention isapplied to assessment of renal function and its implica-tions. Subsequent studies have replicated the results acrossa range of subjects with various underlying conditions.
Another key finding from this study is that it is only a mi-nority of subjects with CKD who progress on to end-stagerenal failure; in contrast they are far more likely to die pre-maturely or suffer an adverse cardiovascular event. Reduc-ing the risk in this massive cohort of patients remains amajor health care challenge. While not always the case inlife, this study certainly showed that bigger is better!
Paul Kalra
C
Chronic kidney disease and the risks of death, cardiovascularevents, and hospitalization
A. S. Go, G. M. Chertow, D. Fan, C. E. McCulloch, C. Y. Hsu
N Engl J Med. 2004;351(13):1296-1305
Terrorists seize a school in North Ossetia, killing335 hostages, including 156 children; the first
direct image of a planetary system outside our solarsystem is captured at the Yepun telescope in Chile;
and Greek Orthodox Patriarch of Alexandria Peter VII is killed in a helicopter crash
2004
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 305

s discussed elsewhere in this issue of Dia-logues in Cardiovascular Medicine, the car-diorenal syndrome is frequently encounteredin clinical practice, yet there has been scantattention given to the potential pathophysi-
ological mechanisms that underlie it. In this manuscriptthe authors concentrate on “severe cardiorenal syndrome”and return to the basic renal and cardiac physiologicalmechanisms as extolled by the famous American physiol-ogist Arthur Clifton Guyton (1919-2003), in trying to explainwhy patients with heart and kidney failure of-ten develop a rapidly downhill clinical course.Their basic hypothesis involves four interrelatedphysiological responses, which, when activated,interact to trigger worsening fluid retention,sympathetic overactivity, declining cardiac andrenal function, and increased inflammation.They term this pathophysiological reaction the“cardiorenal connection.” The main componentsof the proposed cardiorenal connection can beconsidered in turn (activation of the renin-an-
giotensin system [RAS]), imbalance in endothelial func-tion, inflammation, and activation of the sympathetic nerv-ous system [SNS]), although it does not follow that thesequence of events is stepwise, but more likely they occurin parallel with progressive perturbation and ever-worsen-ing consequences. Low renal perfusion leads to activationof the RAS, which not only increases salt and water reten-tion, so worsening cardiac failure, but reactive oxygenspecies (ROS) are also generated. Angiotensin II is alsoknown to stimulate vascular inflammation via nuclear fac-
A
The severe cardiorenal syndrome: “Guyton revisited”
L. G. Bongartz, M. J. Cramer, P. A. Doevendans, J. A. Joles, B. Braam
Eur Heart J. 2005;26(1):11-17
306
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
Renin-angiotensin system
SNS activation by failing kidneys
ROS production viaNADPH-oxidase
NF-κB–mediated inflammation
NO-ROS imbalance
Sympathetic activation by ROS
Inflammation induced by oxidatively modified
proteins, carbohydrates, and lipids
Renin release by afferent
vasoconstriction
Inflammation
Renin release as part of systemic
stress response
Cytokines stimulate NE release
ROS release by activated
macrophages
Sympathetic activation
ROS production: proliferation,
apoptosis
Renin release by renal
sympathetic neurons
NE/NPY-mediated macrophage activation
and cytokine release
A
B
C
D
Figure. (A) Angiotensin II affects the other cardiorenalconnectors: SNS activation in kidney failure, generation of
ROS, and NF-kB–mediated proinflammatory gene expression.(B) Imbalance between NO and ROS is a central event in
cardiovascular diseases. In the cardiorenal connection, thisbalance may influence sympathetic nervous activity, release
of renin and angiotensin, and promote inflammation byoxidative modification of substances. (C) Persistent
inflammation has been found in both renal and heart fail-ure. By altering ROS functioning, and promoting ROS and
norepinephrine (NE) formation, inflammation contributesto the positive feedback loops in the cardiorenal connection.(D) Sympathetic nervous activity is increased in both renal
and heart failure. By affecting the other cardiorenalconnectors it can play a significant role in the severe
cardiorenal syndrome. It stimulates renin release from thekidneys, generates ROS, and induces inflammation.
Abbreviations: NADPH, reduced nicotinamide adeninedinucleotide phosphate; NE, norepinephrine; NF-κB, nuclear
factor-κB; NO, nitric oxide; NPY, neuropeptide Y; ROS,reactive oxygen species; SNS, sympathetic nervous system.
From: Bongartz LG, Cramer MJ, Doevendans PA,Joles JA, Braam B. The severe cardiorenal syndrome:
“Guyton revisited.” © 2004, Eur Heart J. 2005;26: 11-17.The European Society of Cardiology.
•••
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 306

307
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
tor kappa B (NF-κB) pathway, and to lead to activation ofthe SNS, leading to vasoconstriction and further organ ischemia. The balance between nitric oxide and ROS isthought to be important in the control of blood pressureand extracellular fluid volume by regulation of vasodilata-tion, natriuresis, and desensitization of tubuloglomerularfeedback. In the severe cardiorenal syndrome, there is im-balance in this system due to excess production of ROS,diminished levels of native ROS scavengers, and lowerlevels of nitric oxide (due to reaction with ROS and theinhibitory effects of asymmetric dimethylarginine [ADMA]).Vasoconstriction results, with further renin release as aconsequence; ROS also lead to tissue damage, with pro-duction of oxidatively altered lipids, carbohydrates, andproteins, which then induce further inflammation; thereare stimuli that also trigger SNS activation.
By now the suggested complex interplay should be gettingclearer! It so happens that there is evidence that both in-flammation and SNS activation can have stimulatory ef-fects upon each other, and also mutual interactions withRAS activation and nitric oxide/ROS imbalance. Hence, in-flammation stimulates renin release as part of the systemicstress response, ROS are produced by activated macro-phages, and cytokines released by inflammatory cells trig-ger SNS activation. As you now would anticipate, the lattercan itself upregulate the RAS by renin release from renalsympathetic neurons, and prolonged stimulation can re-sult in cardiomyocyte hypertrophy, apoptosis, and focalnecrosis, in part caused by ROS induction. Norepinephrinecan stimulate cytokine release, again exacerbating inflam-mation. For good measure, SNS activation results in releaseof the neurohormone neuropeptide Y, which is thought totrigger inflammation, RAS activity by vasoconstriction, andneointimal hyperplasia, an important step in acceleratedatherosclerosis.
To summarize: the authors suggest that disturbances ofthe underlying physiological systems in the kidney, heart,and blood vessels lead to parallel, interrelated, and mutualactivation of four important hormonal and mediator path-ways, resulting in a progressively deleterious “cardiorenal
connection” that would explain the serious outcome of thesevere cardiorenal syndrome. Although there is plausibilityin their suggestion, as ever, it is likely that the interactionswill turn out to be even more complex, with subtleties inthe purported interdependencies.
I had hoped to be able to summarize the manuscript suc-cinctly and without a diagram, but having re-read my cri-tique, I now feel that the latter is necessary; Figure 2 fromthe review should suffice!
Philip Kalra
2005
Italy introduces a ban on smoking in public places;Zhao Ziyang, former Premier of the People’s
Republic of China and General Secretary of theCommunist Party of China, dies aged 85; andBill Gates donates $750 million to the Global
Alliance for Vaccines and Immunization to providevaccines to children in poor countries
•••
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 307

308
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
hile it had been previously recognizedthat impaired renal function was an inde-pendent predictor of adverse prognosisin patients with heart failure, data fromthe CHARM (Candesartan in Heart failure:
Assessment of Reduction in Mortality and morbidity) stud-ies permitted analysis in patients with impaired and pre-served systolic function, and in those intolerant of angio-tensin-converting enzyme (ACE) inhibition. A number ofthe authors originate from the University of Groningen,Netherlands, where researchers have been instrumental inhighlighting the close and important association betweenthe heart and kidneys.
The CHARM program consisted of three separate, but con-current, studies of candesartan versus placebo: (i) CHARM-Preserved, in patients with left ventricular ejection fraction(LVEF) greater than 40%; (ii) CHARM-Added, in patientswith LVEF of 40% or less already receiving an ACE inhib-itor; (iii) CHARM-Alternative, in patients with LVEF of 40%or less already with a documented intolerance of an ACEinhibitor. The data in this analysis are derived from 2680patients from these studies in whom there were sufficientdata, including renal function (estimated glomerular filtra-tion rate, eGFR).
eGRF was calculated by the Modified Diet in Renal Diseaseequation. Major outcomes assessed included cardiovascu-lar death and hospitalization for heart failure and all-causemortality. Chronic kidney disease (CKD) was common: 36%of subjects had eGFR �60 mL/min/1.73 m2. In comparisonto “real life” practice this is likely to underestimate the trueburden of CKD, since clinical studies in general excludethe very elderly and patients with major comorbidity. In-deed, the mean age in this analysis was around 65 years,which is over a decade lower than the median age of pres-entation with heart failure in the United Kingdom.
During a median follow-up of just under 3 years, cardio-vascular death or hospitalization for heart failure occurredin 950 subjects. A number of parameters, including eGFRand LVEF, were entered into multivariable analysis. Both
reduced renal function (eGFR) and left ventricular func-tion (LVEF) remained independent predictors of adverseoutcome. This was consistently seen across the three dif-ferent study populations, irrespective of whether the pa-tients were receiving blockers of the angiotensin system.
A stepwise reduction in prognosis was seen with reducingrenal function (or worse categories of CKD). As comparedto subjects with an eGFR of > 60 mL/min/1.73 m2, thosewith eGFR of 45 to 60 mL/min per 1.73 m2 (CKD stage 3A)had an adjusted hazard ratio of 1.54 for the primary endpoint (P<0.001) and 1.50 for all-cause mortality (P=0.006).For patients with eGFR <45 mL/min per 1.73 m2 (CKDstage 3B or worse), the respective adjusted hazard ratioswere 1.86 (P<0.001) and 1.91 (P=0.001).
So what are the key take home clinical messages from thisanalysis? Firstly, impaired renal function is common inpatients with chronic heart failure. Secondly, when present,even a modest reduction in renal function is a marker ofhigher absolute risk of an adverse event (including death).Thirdly, there is no evidence that the beneficial effect ofcandesartan (ie, inhibition of the angiotensin system) wasmodified by baseline eGFR. Drugs such as angiotensin-converting enzyme inhibitors and aldosterone blockers aregenerally underutilized in patients with impaired renal func-tion. Yet, these data would suggest that such patients areat high risk of an event and therefore have potentially muchto gain. When these drugs are used, careful monitoring ofclinical and biochemical status is required.
Paul Kalra
Renal function as a predictor of outcome in a broad spectrum of patients with heart failure
H. L. Hillege, D. Nitsch, M. A. Pfeffer, K. Swedberg, J. J. McMurray, S. Yusuf, C. B. Granger, E. L. Michelson, J. Ostergren, J. H. Cornel, et al; Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Investigators
Circulation. 2006;113(5):671-678
W
The 2006 Winter Olympics open in Turin, Italy;Facebook makes its debut and goes viral; and
an intact pharaonic tomb is discovered the Valley of the Kings, the first since the discovery
of the tomb of Tutankhamen in 1922
2006
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 308

309
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
his paper is the “marmite” of articles—you ei-ther love it or hate it! The authors’ justificationof this “state of the art” paper is to provide adefinition of the cardiorenal syndrome (CRS)that in turn helps the identification and full
characterization of the chronology of the pathophysiologi-cal interactions that typify a specific type of combined heart/kidney disorder. This paper, together with its subsequentcitations, associated editorials, and reviews has certainlyhelped raise awareness of this important clinical relation-ship and has inspired constructive debate. Prior to thispaper a number of proposed definitions and hypothesesfor CRS were in circulation. The authors highlight many of the limitations seen with these, including the fact thatmany were too simplistic. Although they do also acknowl-edge that “a more articulated definition of the CRS hasbeen advocated”—interestingly this is a publication by 3of the 4 authors of this manuscript!
Ronco and colleagues propose a classification based aroundfive types of the CRS. This results from the need to differ-entiate between acute and chronic interactions and identi-fy the “primary” driving pathophysiological abnormality ineach clinical scenario. Each subtype is described in turnand supported by very detailed figures with multiple arrowsshowing the pathophysiological abnormalities that charac-terize the differing scenarios. The reader would be mistakenif they were to assume that we have clear understandingof what the arrows really mean (one respected nephrolo-gist described the arrows as representing potential causalrelations with liberal sprinkling of magic pixie dust).
The 5 subtypes of CRS can be summarized as worsening ordecompensated heart failure as a cause or effect of acutekidney injury (AKI, constituting types 1 and 3, respectively),chronic heart failure (CHF) as a cause and effect of chron-ic kidney disease (CKD, types 2 and 4, respectively), andcardiovascular and renal damage from a common under-lying pathology (type 5, eg, acute sepsis, or chronic condi-tions such as diabetes mellitus, atherosclerosis, and/orhypertension). The classification is logical in separatingdifferent clinical presentations of heart/kidney disease.
Previously there was no or little distinction between, eg,acute heart failure resulting in acute kidney injury, as op-posed to CHF leading onto CKD. Moreover, it has certainlyhelped the clinician to realize the high risk associated withparticular clinical situations.
There are, however, major limitations to this classificationparticularly since as already mentioned the precise patho-physiological relationships in the different clinical scenar-ios are not fully understood. Each type of CRS may occur in the presence of another. For example, AKI is more likelyin a patient with decompensated heart failure if the patienthas diabetes (underlying systemic condition) with associ-ated CKD and coronary artery disease (CAD). In addition,it is plausible that a patient with CHF will exhibit patho-physiological changes typical of distinct subgroups at dif-ferent stages of their heart failure syndrome. While theprecise pathophysiological mechanisms are not fully under-stood, it is apparent that dysfunction of one organ systemmay cause or exacerbate dysfunction of the other and aspiral of decline can occur, with resultant adverse prognosis.In many respects, the major attribute of this paper, in myopinion, is how it highlights just how poorly we under-stand CRS. It emphasizes that we cannot sit on our laurelsand expect an improvement in clinical outcomes withoutcoordinating top quality research into this area. However,it probably adds little to the understanding of the patho-physiology. Cardiologists and nephrologists must work onCRS, which is currently seen through a glass, darkly.
Paul Kalra
Cardiorenal syndrome
C. Ronco, M. Haapio, A. A. House, N. Anavekar, R. Bellomo
J Am Coll Cardiol. 2008;52(19):1527-1539
T
Lewis Hamilton becomes the youngest and first black Formula One World Champion;
Democrat Barack Obama defeats Republican John McCain to win the 2008 US presidential
election; and India sends 10 satellites into orbit in a single launch
2008
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 309

310
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Summaries of Ten Seminal Papers - Kalra and Kalra
he FAIR-HF study (Ferinject Assessment in pa-tients with IRon deficiency and chronic HeartFailure) is the largest published trial of IV irontreatment in patients with chronic heart failure(CHF). It produced notable results, and the
only criticism regarding its value and impact on clinicalcare is as a consequence of relatively short duration andslightly weak end points. The study design highlighted a number of difficulties within this area, such as how to truly double-blind a study in which the IV preparation (ie,iron) looks like Coca-Cola (!) and how to define iron defi-ciency in CHF. Patients received the drug into a cannulaplaced with their arm through a makeshift curtain and studypersonnel included a blinded and unblinded group. In lightof the fact that ferritin levels are influenced by coexistentinflammation, a normal value does not exclude iron defi-ciency in CHF and hence arbitrary (but sensible) cutoffswere chosen.
A total of 459 patients with left ventricular (LV) systolic dys-function and New York Heart Association (NYHA) class IIor III and ejection fraction (LVEF) �45% were recruited. It is important to note that patients did not need to beanemic to enter the study, merely iron deficient. Iron defi-ciency was defined as serum ferritin of <100 μg/L or be-tween 100-299 μg/L and a transferring saturation (TSAT)of <20%. Patients were randomized 2:1 to IV 200 mg ferriccarboxymaltose or placebo. A correction (therapy every 2weeks) and then maintenance phase (therapy every 4 weeks)were incorporated into the protocol. The primary endpoints were the self-reported Patient Global Assessment(PGA) and NYHA Class at 24 weeks. Safety of IV iron ther-apy was assessed at 26 weeks.
Treatment was associated with significant improvementsin the primary end point: 50% of patients receiving IV ironreported being much or moderately improved accordingto the PGA as compared with 28% patients receiving place-bo. An odds ratio for improving one of more NYHA classesof 2.40 (95% CI, 1.55-3.71) was seen with active treatmentversus placebo. Secondary end points such as 6-minutewalk distance were similarly improved. Findings were con-
sistent irrespective of whether patients were anemic or not,ie, iron deficiency is the key. Benefits appeared as early as4 weeks from starting treatment, suggesting that benefi-cial mechanisms extend beyond impact on hemoglobin.
Treatment with IV iron was safe, with no severe allergic re-actions reported. It is of note that during the maintenancephase treatment interruption only occurred if hemoglobinexceeded 16.0 g/dL or serum ferritin >800 µg/L or serumferritin >500 μg/L, if TSAT >50%. These ferritin values mightseem extremely high to “non-nephrologists.” However, theirincorporation into the protocol has provided further reas-surance of the safety of treating iron deficiency.
How is FAIR-HF likely to impact on clinical practice? Thedata suggest that correcting iron deficiency in patients withCHF is safe in the short term and associated with improvedfunctioning and quality of life. However, heart failure spe-cialists are used to megastudies with hard clinical endpoints such as mortality and hospitalization. To impactwhole scale changes in clinical practice, a larger study withlong-term follow-up and such end points is required.
Paul Kalra
Ferric carboxymaltose in patients with heart failure and iron deficiency
S. D. Anker, J. Comin Colet, G. Filippatos, R. Willenheimer, K. Dickstein, H. Drexler, T. F. Lüscher, B. Bart, W. Banasiak, J. Niegowska, et al; FAIR-HF Trial Investigators
N Engl J Med. 2009;361(25):2436-2448
T
The body of billionaire Friedrich Karl Flick, stolen from the family mausoleum in 2008
and held for ransom, is returned to his family;the 25th anniversary of the industrial disaster in
Bhopal in which 3787 were killed is marked in India; and the discovery of a new Triassic
theropod dinosaur genus, Tawa, is announced
2009
DCVM 62 Ten Seminal Paper:Mise en page 1 23/03/12 11:33 Page 310

311Copyright © 2011 LLS SAS. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Abe S, Yazawa T, Sloman G. Electrocardiographic abnormalities in patients receiving hemodialysis.
Am Heart J. 1991;(56):1137-1144.
Al-Ahmad A, Rand WM, Manjunath G, Konstam MA, Reduced kidney function and anemia as risk factors for mortality Salem DN, Levey AS, Sarnak MJ. in patients with left ventricular dysfunction.
J Am Coll Cardiol. 2001;38:955-962.
Anand IS, Chandrashekhar Y, Ferrari R, Poole-Wilson PA, Pathogenesis of oedema in chronic anaemic: studies of body water Harris PC. and sodium, renal function, haemodynamics and plasma hormones.
Br Heart J. 1993;70:357-362.
Anand IS, Ferrari R, Kalra GS, Wahi PL, Poole-Wilson PA, Edema of cardiac origin. Studies of body water and sodium, renal Harris PC. function, hemodynamic indexes, and plasma hormones in untreated
congestive cardiac failure.
Circulation. 1989;80:299-305.
Androne A, Katz S, Lund L, LaManca J, Hudaihed A, Hemodilution is common in patients with advanced heart failure. Hryniewicz K, Mancini D. Circulation. 2003;107:226-229.
Bolger AP, Bartlett FR, Penston HS, et al. Intravenous iron alone for the treatment of anemia in patients withchronic heart failure.
J Am Coll Cardiol. 2006;48:1225-1227.
Braun J, Oldendor FM, Moshage W, Heidler R, Zeitler E, Electron beam computed tomography in the evaluation of cardiac Luft F. calcification in chronic dialysis patients.
Am J Kidney Dis. 1996;27(3):394-401.
Burton JO, Korsheed S, Grundy BJ, McIntyre CW. Hemodialysis-induced left ventricular dysfunction is associated withan increase in ventricular arrhythmias.
Ren Fail. 2008;30(7):701-709.
Cannella G, Paoletti E, Delfino R, Peloso G, Molinari S, Regression of left ventricular hypertrophy in hypertensive dialyzed Traverso GB. uremic patients on long-term antihypertensive therapy.
Kidney Int. 1993;44(4):881-886.
Chertow GM, Normand SL, Silva LR, et al. Survival after acute myocardial infarction in patients with end-stagerenal disease: results from the cooperative cardiovascular project.
Am J Kidney Dis. 2000;35:1044-1051.
Cheung AK, Sarnak MJ, Yan G, et al. Cardiac diseases in maintenance hemodialysis patients: results of the HEMO Study.
Kidney Int. 2004;65(6):2380-2389.
Bibliography of One Hundred Key Papersselected by Paul R. Kalra, MD, FRCP
Department of Cardiology - Portsmouth Hospitals NHS Trust - Portsmouth - UK (e-mail: [email protected]) and Philip A. Kalra MD, FRCP
Department of Nephrology - Salford Royal Foundation NHS Trust - Salford - UK (e-mail: [email protected])
Cardiorenal Syndrome
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 311

Chugh SS, Jui J, Gunson K, et al. Current burden of sudden cardiac death: multiple source surveillanceversus retrospective death certificate-based review in a large U.S. community.
J Am Coll Cardiol. 2004;44(6);1268-1275.
Cowie MR, Wood DA, Coats AJ, et al. Incidence and aetiology of heart failure; a population-based study.
Eur Heart J. 1999;20:421-428.
Cowie MR, Wood DA, Coats AJ, et al. Survival of patients with a new diagnosis of heart failure: a population based study.
Heart. 2000;83:505-510.
Cromie N, Lee C, Struthers AD. Anaemia in chronic heart failure: what is its frequency in the UK and its underlying causes?
Heart. 2002;87:377-378.
Cuculich PS, Kerzner R, Greenberg SL, et al. Poor prognosis for patients with chronic kidney disease despite ICDtherapy for the primary prevention of sudden death.
PACE. 2007;30:207-213.
de Lima JJ, Vieira ML, Lopes HF, et al. Blood pressure and the risk of complex arrhythmia in renal insuffi-ciency, hemodialysis, and renal transplant patients.
Am J Hyperstens. 1999;12(2 pt 1):204-208.
Di Iorio BR, Bortone S, Piscopo C, et al. Cardiac vascular calcification and QT interval in ESRD patients: is there a link?
Blood Purif. 2006;24(5-6):451-459.
Dzau VJ. Renal and circulatory mechanisms in heart failure.
Kidney Int. 1987;31:1402-1416.
Eckart RE, Gula LJ, Reynolds MR, et al. Mortality following defibrillator implantation in patients with renalinsufficiency.
J Cardiovasc Electrophysiol. 2006;9:940-943.
Eschbach JW. The anemia of chronic renal failure: pathophysiology and the effects of recombinant erythropoietin.
Kidney Int. 1989;35:134-148.
Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare popu-lation, 1998 to 1999.
J Am Soc Nephrol. 2005;16(2):489-495.
Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease.
Am J Kidney Dis. 1998;32:S112-S119.
Formiga F, Chivite D, Castañer O, Manito N, Ramón JM, Anemia in new-onset congestive heart failure inpatients admitted for acute decompensation.
Eur J Intern Med. 2006;17:179-184.
Fox KF, Cowie MR, Wood DA, et al. Coronary artery disease as the cause of incident heart failure in the population.
Eur Heart J. 2001;22:228-236.
312
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 312

Garg AX, Clark WF, Haynes RB, et al. Moderate renal insufficiency and the risk of cardiovascular mortality:results from the NHANES I.
Kidney Int. 2002;61:1486-1494.
Gehi AK, Stein RH, Metz LD, Gomes JA. Microvolt T-wave alternans for the risk stratification of ventricular tachyarrhythmic events.
J Am Coll Cardiol. 2005;46:75-82.
Genovesi S, Rivera R, Fabbrini P, et al. Dynamic QT interval analysis in uraemic patients receiving chronichaemodialysis.
J Hypertens. 2003;21(10):1921-1926.
Genovesi S, Valsecchi MG, Rossi E, et al. Sudden death and associated factors in a historical cohort of chronic haemodialysis patients.
Nephrol Dial Transplant. 2009;24(8):2529-2536.
Gill GV, Woodward A, Casson IF, Weston PJ. Cardiac arrhythmia and nocturnal hypoglycaemia in type 1 diabetes—the “dead in bed” syndrome revisited.
Diabetologia. 2009;52:42-45.
Gilmore JP. Contribution of baroreceptors to the control of renal function.
Circ Res. 1964;14:301-317.
Gossmann J, Thurmann P, Bachmann T, et al. Mechanism of angiotensin converting enzyme inhibitor-related anemia in renal transplant recipients.
Kidney Int. 1996;50:973-978.
Haider AW, Larson MG, Benjamin EJ, Levy D. Increased left ventricular mass and hypertrophy are associated withincreased risk for sudden death.
J Am Coll Cardiol. 1998;32(5):1454-1459.
Haigney MC, Zareba W, Gentlesk PJ, et al. QT interval variability and spontaneous ventricular tachycardia or fibrillation in the Multicenter Automatic Defibrillator Implantation Trial (MADIT) II patients.
J Am Coll Cardiol. 2004;44(7):1481-1487.
Harris P. Role of arterial pressure in the oedema of heart disease.
Lancet. 1988;1:1036-1038.
Hasselblad V, Gattis Stough W, Shah MR, et al. Relation between dose of loop diuretics and outcomes in a heart failure population: results of the ESCAPE trial.
Eur J Heart Fail. 2007;9(10):1064-1069.
Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis.
N Engl J Med. 1998;339(12):799-805.
Hillege HL, Girbes AR, de Kam PJ, et al. Renal function, neurohormonal activation, and survival in patientswith chronic heart failure.
Circulation. 2000;102:203-210.
Hobson A, Kalra PA, Kalra PR. Cardiology and nephrology: time for a more integrated approach to patient care?
Eur Heart J. 2005;26(16):1576-1578.
313
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 313

Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Anemia is associated with worse symptoms, greater impairment inBorenstein J. functional capacity and a significant increase in mortality in patients
with advanced heart failure.
J Am Coll Cardiol. 2002;39:1780-1786.
Hujairi NM, Afzali B, Goldsmith DJ. Cardiac calcification in renal patients: what we do and don’t know.
Am J Kidney Dis. 2003;43(2):234-243.
Kalra PR, Anagnostopoulos C, Bolger A, Coats AJS, The regulation and measurement of plasma volume in heart failure.Anker SD. J Am Coll Cardiol. 2002;39:1901-1908.
Kalra PR, Anker SD, Coats AJS. Water and sodium regulation in chronic heart failure: the role of natriuretic peptides and vasopressin.
Cardiovasc Res. 2001;51:495-509.
Kalra PR, Collier C, Cowie MR, et al. Haemoglobin concentration does not predict prognosis in incident (new) cases of heart failure.
Lancet. 2003;362:211-212.
Kalra PR, Ponikowski P, Anker SD. Sympathetic activation and malignant ventricular arrhythmias: a molecular link?
Eur Heart J. 2002;23:1078-1080.
Kane GC, Xu N, Mistrik E, Roubicek T, Stanson AW, Renal artery revascularization improves heart failure control in Garovic VD. patients with atherosclerotic renal artery stenosis.
Nephrol Dial Transplant. 2010;25(3):813-820.
Kitano Y, Kasuga H, Watanabe M, et al. Severe coronary stenosis is an important factor for induction and lengthy persistence of ventricular arrhythmias during and after hemodialysis.
Am J Kidney Dis. 2004;44(2):328-326.
Kovesdy C, Regidor D, Mehrotra R, Jing J. Serum and dialysate potassium concentrations and survival in hemodialysis patients.
Clin J Am Soc Nephrol. 2004;2:999-1007.
Krumholz HM, Chen YT, Vaccarino V, et al. Correlates and impact on outcomes of worsening renal function in patients �65 years of age with heart failure.
Am J Cardiol. 2000;85(9):1110-1113.
Kuller LH. Sudden death—definition and epidemiological considerations.
Prog Cardiovasc Dis. 1980;23(1):1-12.
Lafrance JP, Nolin L, Senécal L, Leblanc M. Predictors and outcome of cardiopulmonary resuscitation (CPR) calls in a large haemodialysis unit over a seven-year period.
Nephrol Dial Transplant. 2006;21(4):1006-1012.
Lang CC, Choy AMJ, Henderson IS, Coutie WJ, Struthers AD. Effect of haemodialysis on plasma levels of brain natriuretic peptidein patients with chronic renal failure.
Clin Sci. 1992;82:127-131.
Leach IH, Blundell JW, Rowleyf JM, Turner DR. Acute ischaemic lesions in death due to ischaemic heart disease.
Eur Heart J. 1995;16:1181-1185.
Levin ER, Gardner DG, Samson WK. Natriuretic peptides.
N Engl J Med. 1998;339:321-328.
314
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 314

Levine B, Kalman J, Mayer L, Fillit HM, Packer M. Elevated circulating levels of tumor necrosis factor in severe chronicheart failure.
N Engl J Med. 1990;323:236-241.
Levy R, Dellavalle A, Atav S, Sklar AH, Stamato NJ. The relationship between glomerular filtration rate and survival in patients treated with an implantable cardioverter defibrillator.
Clin Cardiol. 2008;269:265-269.
Liang KV, Williams AW, Greene EL, et al. Acute decompensated heart failure and the cardio-renal syndrome.
Crit Care Med. 2008;36(suppl):S75-S88.
Logeart D, Tabet JY, Hittinger L, et al. Transient worsening of renal function during hospitalization for acute heart failure alters outcome.
Int J Cardiol. 2008;127(2):228-232.
Lown B, Wolf M. Approaches to sudden death from coronary heart disease.
Circulation. 1971;44:130-142.
Mahon NG, Blackstone EH, Francis GS, et al. The prognostic value of estimated creatinine clearance alongside functional capacity in ambulatory patients with chronic congestive heart failure.
J Am Coll Cardiol. 2002;40(6):1106-1113.
Mancia G. Sympathetic activation in congestive heart failure.
Eur Heart J. 1990;11(suppl A):3-11.
Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Effect of erythropoietin on exercise capacity in patients with Androne AS. moderate to severe chronic heart failure.
Circulation. 2003;107:294-299.
Martin PY, Schrier RW. Sodium and water retention in heart failure: pathogenesis and treatment.
Kidney Int. 1997;51(suppl 59):S57-S61.
McCullough PA. Cardiovascular disease in chronic kidney disease from a cardiologist’sperspective.
Curr Opin Nephrol Hypertens. 2004;13(6):591-600.
McCullough PA, Jurkovitz CT, Pergola PE, et al. Independent components of chronic kidney disease as a cardiovas-cular risk state: results from the Kidney Early Evaluation Program (KEEP).
Arch Intern Med. 2007;167(11):1122-1129.
McCullough PA, Sandberg KR. Chronic kidney disease and sudden death: strategies for prevention.
Blood Purif. 2004;22:136-142.
Means RT Jr. Advances in the anemia of chronic disease.
Int J Hematol. 1999;70:7-12.
Metra M, Nodari S, Parrinello G, et al. Worsening renal function in patients hospitalised for acute heart failure: clinical implications and prognostic significance.
Eur J Heart Fail. 2008;10(2):188-195.
Moe SM, O'Neill KD, Reslerova M, et al. Natural history of vascular calcification in dialysis and transplant patients.
Nephrol Dial Transplant. 2004;19(9):2387-2393.
315
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 315

Nakano T, Ninomiya T, Sumiyoshi S, et al. Association of kidney function with coronary atherosclerosis and calcification in autopsy samples from Japanese elders: the Hisayamastudy.
Am J Kidney Dis. 2010;55(1):21-30.
Näppi SE, Virtanen VK, Saha HH, Mustonen JT, QTc dispersion increases during hemodialysis with low-calcium Pasternack AI. dialysate.
Kidney Int. 2000;57(5):2117-2122.
Narula AS, Jha V, Bali HK, et al. Cardiac arrhythmias and silent myocardial ischaemia during hemodialysis.
Ren Fail. 2000;22(3):355-368.
Nearing BD, Verrier RL. Modified moving average analysis of T-wave alternans to predict ventricular fibrillation with high accuracy.
J Appl Physiol. 2002;92:541-549.
Newton JD, Squire IB. Glucose and haemoglobin in the assessment of prognosis after first hospitalisation for heart failure.
Heart. 2006;92:1441-1446.
Odden MC, Whooley MA, Shlipak MG. Association of chronic kidney disease and anemia with physical capacity: the heart and soul study.
J Am Soc Nephrol. 2004;15:2908-2915.
Oikawa K, Ishihara R, Maeda T, et al. Prognostic value of heart rate variability in patients with renal failureon hemodialysis.
Int J Cardiol. 2009;131(3):370-377.
Okonko DO, Grzeslo A, Witkowski T, et al. Effect of intravenous iron sucrose on exercise tolerance in anemic and nonanemic patients with symptomatic chronic heart failure andiron deficiency FERRIC-HF: a randomized, controlled, observer-blinded trial.
J Am Coll Cardiol. 2008;51:103-112.
Packer M. The neurohormonal hypothesis: a theory to explain the mechanism of disease progression in heart failure.
J Am Coll Cardiol. 1992;20:248-254.
Ponikowski P, Anker SD, Szachniewicz J, et al. Effect of darbepoetin alfa on exercise tolerance in anemic patients with symptomatic chronic heart failure: a randomized, double-blind,placebo-controlled trial.
J Am Coll Cardiol. 2007;49:753-762.
Priori SG, Aliot E, Bossaert L, et al. Task Force Report Task Force on Sudden Cardiac Death of the European Society of Cardiology.
Eur Heart J. 2001;22:1374-1450.
Radaelli B, Cavalli A, Latini R, Maggioni A. Multicentre cross-sectional study of ventricular arrhythmias in chronically haemodialysed patients.
Lancet. 1988;332(8606):305-309.
Reeder GS. Atrial natriuretic peptide elevation in congestive heart failure in the human.
Science. 1986;231:1145-1147.
316
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 316

Remme WJ, Swedberg K; Task Force for the Diagnosis Guidelines for the diagnosis and treatment of chronic heart failure. and Treatment of Chronic Heart Failure, European Society of Cardiology. Eur Heart J. 2001;22:1527-1560.
Robin J, Weinberg K, Tiongson J, et al. Renal dialysis as a risk factor for appropriate therapies and mor-tality in implantable cardioverter-defibrillator recipients.
Heart Rhythm. 2006;3(10);1197-1201.
Sakhuja R, Keebler M, Lai TS, et al. Meta-analysis of mortality in dialysis patients with an implantablecardioverter defibrillator.
Am J Cardiol. 2009;103(5):735-741.
Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research,Clinical Cardiology, and Epidemiology and Prevention.
Hypertension. 2003;42:1050-1065.
Schrier RW. Pathogenesis of sodium and water retention in high-output and low-output cardiac failure, nephrotic syndrome, cirrhosis and pregnancy.
N Engl J Med. 1988;319:1065-1072.
Schrier RW. Cardiorenal versus reno-cardiac syndrome: is there a difference?
Nat Clin Pract Nephrol. 2007;3:637.
Selby NM, McIntyre CW. The acute cardiac effects of dialysis.
Semin Dial. 2007:220-228.
Sforzini S, Latini R, Vincenti A, Redaelli B. Ventricular arrhythmias and four-year mortality in haemodialysis patients.
Lancet. 1992;339:212-213.
Shapira OM, Bar-Khayim Y. ECG changes and cardiac arrhythmias in chronic renal failure patients on hemodialysis.
J Electrocardiol. 1992;25(4):273-279.
Sharma R, Francis DP, Pitt B, Poole-Wilson PA, Haemoglobin predicts survival in patients with chronic heart failure: Anker SD. a substudy of the ELITE II trial.
Eur Heart J. 2004;25:1021-1028.
Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiacclass, and markedly reduces hospitalizations.
J Am Coll Cardiol. 2000;35:1737-1744.
Silverberg DS, Wexler D, Sheps D, et al. The effect of correction of mild anemia in severe, resistant conges-tive heart failure using subcutaneous erythropoietin and intra-venous iron: a randomized controlled study.
J Am Coll Cardiol. 2001;37:1775-1780.
Suarez GA, Clark VM, Norell JE, Kottke TE. Sudden cardiac death in diabetes mellitus: risk factors in the Rochester diabetic neuropathy study.
J Neurol Neurosurg Psychiatry. 2005;76:240-245.
317
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 317

Suzuki R, Tsumura K, Inoue T, Kishimoto H, Morii H. QT interval prolongation in the patients receiving maintenance hemodialysis.
Clin Nephrol. 1998;49(4):240-244.
Szachniewicz J, Petruk-Kowalczyk J, Majda J, et al. Anaemia is an independent predictor of poor outcome in patients with chronic heart failure.
Int J Cardiol. 2003;90:303-308.
Tanner H, Moschovitis G, Kuster GM, et al. The prevalence of anemia in chronic heart failure.
Int J Cardiol. 2002;86:115-121.
Toblli JE, Lombraña A, Duarte P, Di Gennaro F. Intravenous iron reduces NT-pro-brain natriuretic peptide in anemicpatients with chronic heart failure and renal insufficiency.
J Am Coll Cardiol. 2007;50:1657-1665.
Vander AJ. Control of renin release.
Physiol Rev. 1967;47:359-382.
Verma A, Anavekar NS, Meris A, et al. The relationship between renal function and cardiac structure, function, and prognosis after myocardial infarction: the VALIANT Echo Study.
J Am Coll Cardiol. 2007;50(13):1238-1245.
Verrier RL, Nearing BD, Teresa M, et al. Ambulatory electrocardiogram-based tracking of T wave alternansin postmyocardial infarction patients to assess risk of cardiac arrestor arrhythmic death.
J Cardiovasc Electrophysiol. 2003;14(4):705-711.
Weber KT. Extracellular matrix remodeling in heart failure: a role for de novo angiotensin II generation.
Circulation. 1997;96:4065-4082.
Witte KK, Desilva R, Chattopadhyay S, Ghosh J, Are hematinic deficiencies the cause of anemia in chronic heart Cleland JG, Clark AL. failure?
Am Heart J. 2004;147:924-930.
Wright JR, Shurrab AE, Cooper A, Kalra PR, Foley RN, Left ventricular morphology and function in patients with athero-Kalra PA. sclerotic renovascular disease.
J Am Soc Nephrol. 2005;16(9):2746-2753.
Wright JR, Shurrab AE, Cooper A, Kalra PR, Foley RN, Progression of cardiac dysfunction in patients with atheroscleroticKalra PA. renovascular disease.
QJM. 2009;102(10): 695-704.
Zachariah D, Kalra PA, Kalra PR. Optimal management of chronic heart failure in patients with chronic kidney disease.
J Ren Care. 2009;35(1):2-10.
Zimmerman RS, Edwards BS, Schwab TR, Cardiorenal-endocrine dynamics during and following volume Heublein DM, Burnett JC Jr. expansion.
Am J Physiol. 1987;252:R336-R340.
Zipes DP, Camm AJ, Borggrefe M, Buxton AE. ACC/AHA/ESC 2006 Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death.
Circulation. 2006;114:e385-e484.
318
Dialogues in Cardiovascular Medicine - Vol 16 . No. 4 . 2011
Bibliography of One Hundred Key Papers
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 318

GENERAL INSTRUCTIONS
• Manuscripts should be provided onword-processor disks (3.5-in, for IBM,IBM-compatible, or Apple computers)with three hard copies (text and fig-ures) printed on one side of standard-sized white bond paper, double-spaced, with 2.5-cm margins. Pagesmust be numbered. Standard typedpage = 25 lines of 75 characters (including spaces) double-spaced, 2.5-cm margins = a total of 275words per page.
• All texts should be submitted inEnglish. In the case of translations, the text in the original language shouldbe included.
• On the title page, provide title ofmanuscript (title should be concise,not exceeding 120 characters, includingspaces), short running title, keywords,and acknowledgments, as well as fullnames (first name, middle name(s),and last name) with highest academicdegrees (in country-of-origin language),affiliations/address, telephone No., fax No., and E-mail address.
• Illustrations (photographs, tables, graphs,figures–high-quality printouts, glossyprints, and/or high-quality scans asjpg files) should be of good quality orprofessionally prepared, numbered according to their order, with properorientation indicated (eg, “top,” or“left”), and SHORT legends provided,not repetitive of text. As figures and graphs may need to bereduced or enlarged, all absolute valuesand statistics should be provided. All illustrations should be cited in thetext, with distinct numbering for fig-ures and tables. Illustrations will bereproduced in full color only whenclearly necessary, eg, images from nu-clear medicine or histology.
• Include HEADINGS using a consistentstyle for the various levels of headings,to highlight key points and facilitatecomprehension of the text. The Publisher reserves the right to addor delete headings when necessary.
• Abbreviations should be used sparinglyand expanded at first mention.
• Use Système International (SI) units.
• Use generic names of drugs.
• All references should be cited in thetext and numbered consecutively us-ing superscript arabic numerals. Theauthor-date system of citation is NOTacceptable. “In press” references are tobe avoided. In the bibliography, titlesof journals should be abbreviated ac-cording to the Index Medicus. All au-thors should be listed up to six; if thereare more, only the first three shouldbe listed, followed by “et al” (Uniformrequirements for manuscripts sub mitted tobiomedical journals: see www.icmje.org ).Where necessary, references will bestyled to Dialogues in CardiovascularMedicine copyediting requirements.Authors bear total responsibility forthe accuracy and completeness of allreferences and for correct text citation.Example of style for references:
1. Ouriel K, Geary K, Green RM, Geary JE,DeWeese JA. Factors determining survival afterruptured abdominal aneurysm. J Vasc Surg.1990;11:493-496.
2. Darling RC, Brewster DC, Ottinger LW. Autopsy study of unoperated abdominal aorticaneurysms: the case for early resection.Circulation. 1977;56(suppl II):II161-II164.
3. Schulman JL. Immunology of influenza. In:Kilbourne ED, Alfade RT, eds. The InfluenzaViruses and Influenza. Orlando, Fla: AcademicPress Inc; 1975:373-393.
• Copyediting: all contributions toDialogues in Cardiovascular Medicine willbe styled by the Publisher’s editorialdepartment according to the specifica -tions of the current edition of theAmerican Medical Association Manual ofStyle, Williams & Wilkins. Page proofswill be sent to authors for approval andshould be returned within 5 days. If thistime is exceeded, changes made by theeditorial department will be assumedto be accepted by the author. Authorsare responsible for all statements madein their work, including changes madeby the editorial department and au-thorized by the author. The Publisherwill edit Editorials, Abstracts, andSeminal Paper Summaries to requiredsize if their length does not complywith specific requirements.
• Copyright of articles will be transferredto the Publisher of Dialogues inCardiovascular Medicine. For reproduction
of existing work, it is the author’s re-sponsibility to obtain copyright fromthe author(s) (including self) and thepublisher(s) and provide copies of theseauthorizations with the manuscript.
LEAD ARTICLE
The lead article should not exceed 30 standard typed pages (7000 to 8000 words), including an abstract of no more than 200 words, no more than50 references, and a minimum of 5 -maximum of 10 illustrations (figures and/or tables). A maximum of 5-10 keywordsshould be included. The 3 questions forthe respondents should be introducedin or after the conclusion. A separate listof “10 references of seminal papers”as well as a separate list of “100 KeyReferences” should be provided.
RESPONDENT ARTICLES
Respondent articles should not exceed15 standard typed pages (3000 to 4000 words), including an abstract of no more than 125 words, no more than10 references, and a mimimun of 3 -maximum of 5 illustrations (figures andtables). A maximum of 5-10 keywordsshould be included.
SEMINAL PAPER SUMMARIES
Seminal paper summaries take up onepage of Dialogues in Cardiovascular Medicine:the length of each summary should IM-PERATIVELY be comprised between500 and 600 words, ie, not exceed3000 characters. Summaries that aretoo short or too long will be returned tothe author or edited by the Publisher.No figures, tables or references shouldbe included in seminal paper summaries.
FASCINOMA CARDIOLOGICAARTICLES
Fascinoma Cardiologica articles (A Lexiconof the Heart; Icons of Cardiology; Plants andthe Heart; Trails of Discovery, etc) should notexceed 2000 words (8 standard typedpages), should include 3 to 5 illustra-tions (figures and tables), and cite nomore than 15 references. A maximum of5-10 keywords should be included. No abstract.
Instructions for authors
DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 319

DCVM 62 100 Key References:Mise en page 1 23/03/12 11:34 Page 320






![3 cras jf[1]](https://static.fdocuments.in/doc/165x107/55a464381a28ab5d4b8b4758/3-cras-jf1.jpg)











