Davin j Osteocondritis
5
Manual Therapy 11 (2006) 157–161 Case report Osteochondritis dessicans: A complex case of anterior knee pain John Davin a, , James Selfe b a Manchester United Football Club, Birch Road, Carrington, Manchester, M31 4BH, UK b Reader in Physiotherapy, Allied Health Professions Unit, University of Central Lancashire, Preston, PR1 2HE, UK Received 25 March 2004; received in revised form 4 February 2005; accepted 19 May 2005 1. Introd uction This case highlig hts the difficu lty in correc tly identify- ing osteochon dritis dessicans and alerts clinicians to the fac t that alth ough pre viousl y unr epo rted as such, the conditi on may be pr one to recurre nc e. Presenti ng symptoms and ear ly pos itiv e res pon ses to tre atme nt may be mis lea din g and indi cativ e of dysf unct ion in structures that are not responsible for the complaint. 2. The patie nt The patien t was a 17-y ear- old male, right leg domi- nant, full-time professional football player. He appeared to be in goo d hea lth and walked confide ntl y int o the treatment room. Movements of sitting to standing were completed effortlessly with no obvious visual cues as to the nat ure of the compl ain t. His past me dic al his tor y consisted of a previous arthroscopy to the left knee when the pati ent was 14. This sho wed oste och ond ritis dessi- cans, with a large flap of articular cartilage on the medial femora l co nd yl e. The me di al fe mora l co nd yl e was successfully rep air ed. In addit ion , the pat ien t had an asymptomatic spondylolisthesis of L5/S1. 3. Histor y of conditio n The patien t rec alle d a 6-mont h hist ory of lef t kne e pain. Initially, it had not prevented him from training but he felt it had altered his running style. He reported that his left leg felt considerably weaker than his right one and that this was more than the expected difference due to leg dominance. He had not sought help at the time of the initial pain as shortly thereafter he suffered from glandular fever and this had enforced a prolonged break from football. When the patient return ed to the club for pre-sea son training, initially his knee felt normal. Four weeks into the season he rec all ed exp eri enc ing sli ght kne e pai n. Thi s grad uall y wors ened over a 2-wee k perio d unti l the pain became so intense that he could not complete the warmup. 4. Subjec tive assessment The patient complained of a painful left knee as well as other symptoms (see Fig. 1). A Visual Analogue Scale (VAS) value of 7 was given by the patient for his knee pai n. His primar y complaint (P1) was descri bed as a diffuse dull ache around the anterior aspect of the knee, sometimes spr ead ing to the mid-th igh aft er 4–5 min of intense exercise includ ing accele ration, deceleratio n and change of direction exercises. P2 was a general tightness around th e k ne e, wh ich came on af te r 20 min of sustain ed flex ion. P3 was an occ asio nal shooti ng pai n along the lateral aspect of the calf from the knee to the Achilles tendon. He noted a link between P1 and P3 but stated that P1 could be felt at rest but not P3. 5. Objectiv e examinat ion The pain distribution suggested several possible structu res as the source of symptoms. A previous AR TIC LE IN PR ESS www.elsevier.com/locate/math 1356-68 9X/$ - see front matter r 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.math.2005.05.003 Corresponding author. E-mail address: john.dav in@manu td.co.u k (J. Davin).
-
Upload
diego-subiabre -
Category
Documents
-
view
216 -
download
0
Transcript of Davin j Osteocondritis

8/16/2019 Davin j Osteocondritis
http://slidepdf.com/reader/full/davin-j-osteocondritis 1/5
Manual Therapy 11 (2006) 157–161
Case report
Osteochondritis dessicans: A complex case of anterior knee pain
John Davina,, James Selfeb
aManchester United Football Club, Birch Road, Carrington, Manchester, M31 4BH, UK bReader in Physiotherapy, Allied Health Professions Unit, University of Central Lancashire, Preston, PR1 2HE, UK
Received 25 March 2004; received in revised form 4 February 2005; accepted 19 May 2005
1. Introduction
This case highlights the difficulty in correctly identify-
ing osteochondritis dessicans and alerts clinicians to the
fact that although previously unreported as such, the
condition may be prone to recurrence. Presenting
symptoms and early positive responses to treatment
may be misleading and indicative of dysfunction in
structures that are not responsible for the complaint.
2. The patient
The patient was a 17-year-old male, right leg domi-
nant, full-time professional football player. He appeared
to be in good health and walked confidently into the
treatment room. Movements of sitting to standing were
completed effortlessly with no obvious visual cues as to
the nature of the complaint. His past medical history
consisted of a previous arthroscopy to the left knee when
the patient was 14. This showed osteochondritis dessi-
cans, with a large flap of articular cartilage on the medial
femoral condyle. The medial femoral condyle was
successfully repaired. In addition, the patient had an
asymptomatic spondylolisthesis of L5/S1.
3. History of condition
The patient recalled a 6-month history of left knee
pain. Initially, it had not prevented him from training
but he felt it had altered his running style. He reported
that his left leg felt considerably weaker than his rightone and that this was more than the expected difference
due to leg dominance. He had not sought help at the
time of the initial pain as shortly thereafter he suffered
from glandular fever and this had enforced a prolonged
break from football.
When the patient returned to the club for pre-season
training, initially his knee felt normal. Four weeks into the
season he recalled experiencing slight knee pain. This
gradually worsened over a 2-week period until the pain
became so intense that he could not complete the warmup.
4. Subjective assessment
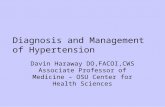
The patient complained of a painful left knee as well
as other symptoms (see Fig. 1). A Visual Analogue Scale
(VAS) value of 7 was given by the patient for his knee
pain. His primary complaint (P1) was described as a
diffuse dull ache around the anterior aspect of the knee,
sometimes spreading to the mid-thigh after 4–5 min of
intense exercise including acceleration, deceleration and
change of direction exercises. P2 was a general tightness
around the knee, which came on after 20 min of
sustained flexion. P3 was an occasional shooting pain
along the lateral aspect of the calf from the knee to the
Achilles tendon. He noted a link between P1 and P3 but
stated that P1 could be felt at rest but not P3.
5. Objective examination
The pain distribution suggested several possible
structures as the source of symptoms. A previous
ARTICLE IN PRESS
www.elsevier.com/locate/math
1356-689X/$ - see front matterr 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.math.2005.05.003
Corresponding author.
E-mail address: [email protected] (J. Davin).

8/16/2019 Davin j Osteocondritis
http://slidepdf.com/reader/full/davin-j-osteocondritis 2/5
history of an L5/S1 spondylolisthesis is a red flag
(Clinical Standards Advisory Group (CSAG), 1994).
Although the previous history suggested that the
spondylolisthesis was stable (concurrent X-rays taken
at yearly intervals for 4 years) an objective assessment of
the lumbar spine was undertaken. This was not only to
rule out a possible source of symptoms but also to allay
the patient’s fear in terms of diagnosis. The patient’s
brother was also a professional footballer whose career
had halted early due to a congenital active spondylo-
listhesis. The patient had expressed concern at this and
any undue anxiety, as Main and Watson (1999) argue,
may influence pain mechanisms.
The only significant finding was related to posture.
Postural assessment revealed a thoracic kyphosis,
lumbar lordosis and anteriorly tilted pelvis. However,
footballers often present with this altered posture due to
repeated activity of the hip flexor and knee extensor
muscles combined with relative inactivity of the
antagonistic muscle groups.
Maitland (1991) notes that knee pain can be provoked
from a painless hip. Although, pain referral patterns of
the hip as described by Sims (1999) bore some relation
to those experienced by the patient no significant hip
abnormalities were found on objective examination.
In this case long-standing symptoms around the knee
combined with previous trauma, surgery and the
subject’s occupation (four seasons of professional foot-
ball since surgery) meant that the knee became the
primary focus of the clinical assessment.
Objective assessment of the tibiofemoral joint
consisted of palpation, active and passive movements
for flexion, extension, medial and lateral rotation
and flexion extension quadrants with and without
ARTICLE IN PRESS
Fig. 1. Patient notes linkage between P1 and P3.
J. Davin, J. Selfe / Manual Therapy 11 (2006) 157–161158

8/16/2019 Davin j Osteocondritis
http://slidepdf.com/reader/full/davin-j-osteocondritis 3/5
compression. All supporting ligaments were passively
stressed and gave a strong end feel. There were no other
comparable signs apart from a low-grade effusion.
Spencer et al. (1984) reported that 20 ml of saline could
inhibit the vastus medialis (VM) and 50 ml of saline
could inhibit both rectus femoris and vastus lateralis.
The presence of an extensor lag was noted which couldimplicate either the tibiofemoral joint or the patellofe-
moral joint (Maitland, 1991).
The absence of any comparable signs in the lumbar
spine, hip and tibiofemoral joint suggested that patello-
femoral joint dysfunction might be the source of the
symptoms. Objective assessment revealed a patella that
was laterally shifted, laterally tilted and externally
rotated, and tightness in the lateral retinaculum was
also noted. Altered patella positioning may adversely
affect patellofemoral biomechanics. However, it is
acknowledged that the reliability of measurements of
patella alignment abnormalities has been reported to be
poor (Fitzgerald and McClure, 1995; Tomsich et al.,
1996; Watson et al., 1999). Accessory movements of
medial glide and medial rotation to the patella gave
comparable signs.
Neural screening showed a deficit in the L3 myotome.
The lateral leg pain (P3) was further assessed in the
slump position. Left leg dorsiflexion/inversion brought
on P3 at 451 of knee flexion.
Multidirectional functional running tests provoked P1
to a level of 8 out of 10 when running backwards and
when cutting sideways from left to right. However,
similar to the extensor lag noted previously, this finding
does not discriminate between tibiofemoral or patellofe-moral dysfunction. Corrective taping was applied to the
patella and multidirectional running testing was repeated,
and this time reported pain levels were 1 out of 10.
6. Treatment
Subjective questioning and objective assessment pre-
sented a strong case for patellofemoral joint dysfunction
and the following treatment regime was instigated. It
consisted of 6 treatment sessions which included 10 min
of manual therapy and 20 min of active control work.
The patient was also instructed in a home exercise
programme. This consisted of rectus femoris and
gastrocnemius stretching (15 s 4), 10 min of plie work
using a biofeedback machine, and sliders 30 s 4 per
night.
Accessory movements to the patella gave comparable
signs and so were used as the first treatment choice.
Grade III medial glides (5 30 s) with a rest between
sets were used. After treatment 2 this was progressed to
Grade IV (5 30 s) with a rest between sets. These were
performed to the patella to mobilize the joint through a
more elastic phase and to increase joint nutrition. The
movement helps to ‘‘stir the inflammatory soup’’
(Butler, 2000, p. 53) increasing the fluid pH and
decreasing acidity. This elevates the threshold at which
nociceptors fire; a greater stimulus is therefore required
to elicit a response (Butler, 2000). Severity, Irritability
and Nature (SIN) factors (Maitland, 1991) allowed
quick progression to grade IV to stretch tightenedlateral structures.
Patellar taping (see Figs. 2–4) in this case was used to
maintain a stretch on the lateral tissues achieved in
treatment. It was applied at the end of treatment two
after it was established that medial glides (grade IV)
were beneficial in reducing pain. Although effective in
this case at significantly reducing pain, the decision to
use patellar taping is controversial as it is unclear how
the tape actually works (Harrison and Magee, 2001).
Mini squats in the plie position were instructed to
exercise the VM and complement the medial glide
mobilisation, the aim being for the patient to gain active
motor control around the patellofemoral joint. The
function of the VM is to re-align the patella medially
during extension of the knee. Any insufficiency of this
muscle will increase the lateral drift of the patella, which
may lead to patellofemoral pain (McConnell, 1986). A
portable biofeedback machine was used in treatment
sessions to ensure that the exercises were targeting the
VM. The machine was then used for the home exercises,
ensuring correct technique.
A muscle-stretching regime was instructed as part of
the home exercise programme to enhance the general
condition of the knee joint. The influence of surrounding
musculature is open to debate. Rouse (1996) questionsthe relevance of the iliotibial band (ITB) and its
relationship with patellar problems. Mercer et al.
(1999) state that the ITB is firmly attached to the linear
aspera of the femur via the lateral inter-muscular
septum. Therefore, clinical procedures for assessing/
ARTICLE IN PRESS
Fig. 2. Hypafix taping in a lateral–medial direction.
J. Davin, J. Selfe / Manual Therapy 11 (2006) 157–161 159

8/16/2019 Davin j Osteocondritis
http://slidepdf.com/reader/full/davin-j-osteocondritis 4/5
stretching the ITB should be re-examined. In this case
no stretch was instructed for the ITB in the home
exercises. However, exercises for rectus femoris and
gastrocnemius were instructed due to their influence on
the knee joint (McConnell, 1986).
Home exercises were prescribed for the nervous
system to maintain improvements achieved in treatment
sessions. Sliders (a means of moving the nervous system
without causing tension) were used to continue nour-
ishment of the nervous system and induce mobilization
in a non-sensitive way. Sliders were used in the slump
position. As the ankle is dorsiflexed the cervical spine is
simultaneously extended. This is then reversed so that as
the ankle is plantar flexed the cervical spine is
simultaneously flexed. This aids vascular dynamics and
axonal transport along the nerve, Butler (2000).
The treatment regime allowed the patient to return to
football training. He successfully completed two con-
secutive training sessions pain free before being dis-
charged. Unfortunately, it so happened that the
patellofemoral problem the patient had been treated
for was not the primary cause of his complaint. Shortly
after his apparent recovery the symptoms returned and a
decision was made to scan the joint. This showed a
circular articular defect, 2.5 cm in diameter on the
medial femoral condyle.
7. Discussion
Osteochondritis dessicans is a common disorder,
affecting adolescents, Tatum (2000). According to Brier
(1999), the medial femoral condyle, particularly the
lateral portion, is the most common site for osteochon-
dritis dessicans. It occurs more regularly in boys and
patients who develop the condition tend to be very
athletically active. The disease is characterized by a
fragment of articular cartilage and subchondral bone
that becomes separated from the underlying bone.
Treatment of the condition is aimed at preservation of
the articular cartilage.
The patient’s age, sex and occupation clearly suggest
that he could be a candidate for developing osteochon-
dritis dessicans, yet, his patellofemoral joint became the
primary focus for treatment. From a clinical-reasoning
perspective combining the information gained from the
patient’s past medical history, the objective assessment
and the evidence available from the literature were very
important; the key points were as follows:
successful reparative surgery at the age of 14;
significant pain relief following patellar taping duringthe assessment; and
a literature search failed to find any previous reports
of osteochondritis dessicans recurrence.
Following the decision to treat the patellofemoral
joint, the treatment administered had a very positive
effect on the symptoms and the patient successfully
completed two consecutive training sessions pain free;
this reinforced the consideration that the patellofemoral
joint was the source of the symptoms.
It is interesting to speculate as to whether there was
any additional clinical testing that could have been
performed to indicate that osteochondritis dessicans was
a problem. Objective assessment of the tibiofemoral
joint gave no comparable signs. Currently, using clinical
testing it is not possible to differentiate between femoral
condyle and meniscal dysfunction. Testing at the knee
predominantly tests the meniscal structures. Even with
compression or active loading it is difficult to attribute
signs specifically to the femoral condyle.
It is also interesting to consider why there was such an
apparent improvement in symptoms to the level where
the patient was able to complete football training, at a
professional level, pain free when the problem was the
ARTICLE IN PRESS
Fig. 3. Hypafix re-enforced with strappal in identical lateral/medial
direction.
Fig. 4. Strappal applied in a lateral supero-medial direction to rotate
patella.
J. Davin, J. Selfe / Manual Therapy 11 (2006) 157–161160

8/16/2019 Davin j Osteocondritis
http://slidepdf.com/reader/full/davin-j-osteocondritis 5/5
femoral condyle and yet the treatment was directed at
the patellofemoral joint. It may be that altered
mechanics at the tibiofemoral joint led to poor
patellofemoral integrity, which in turn led to repeated
micro trauma, which subsequently induced pain. One of
the difficulties in trying to interpret this is that the
treatment package consisted of a number of componentsany of which in isolation or combination could have had
an effect.
A recent report by Hinman et al. (2003) may shed
some light on one of the components of the treatment
package taping. These authors report the results of a
blinded randomised-controlled trial of patellar taping in
the management of osteoarthritic knees. In this report
patellar taping was significantly more effective than
placebo and no tape in a group of patients that included
some patients who only had tibiofemoral joint disease.
Although the report suggests that patellar taping can
improve symptoms in patients who have only tibiofe-
moral problems, no explanation is provided as to how
or why this occurs. It would seem that this patient’s
condition provides another example of a femoral
condition that initially responded to patellar taping.
Further research is required to understand the mechan-
isms behind this pain-relieving effect.
8. Conclusion
In sport the role of the first contact practitioner is
already well established. In other, areas of musculoske-letal physiotherapy therapists are finding that they are
becoming first contact/advanced practitioners with
increasing levels of clinical autonomy, e.g. clinical
specialists, extended scope practitioners and consultant
therapists. It is vital that advanced practitioners wher-
ever they are based, have the skills and knowledge to
identify serious and/or unusual pathology when it
presents. This case has highlighted the need for
clinicians to remain vigilant even when patients appear
to be responding well to treatment.
References
Brier SR. Primary care orthopedics. USA: Mosby; 1999. p. 352.
Butler DS. The sensitive nervous system, 1st ed. Australia: Noi GroupPublications; 2000.
Clinical Standards Advisory Group (CSAG). Back pain: report of a
clinical standards advisory group on back pain, HMSO, 1994.
Fitzgerald G, McClure P. Reliability of measurements obtained with
four tests for patellofemoral alignment. Physical Therapy
1995;75(2):84–92.
Harrison E, Magee D. Patellofemoral pain syndrome: the ongoing
challenges in etiology diagnosis and management. Critical Reviews
in Physical and Rehabilitation Medicine 2001;13(2&3):105–29.
Hinman RS, Crossley KM, McConnell J, Bennell KL. Efficacy of knee
tape in the management of osteoarthritis of the knee: blinded
randomized controlled trial. British Medical Journal 2003;327:
135–41.
Main CJ, Watson PJ. Psychological aspects of pain. Manual Therapy
1999;4(4):203–15.Maitland GD. Peripheral manipulation. 3rd ed. Oxford: Butterworth
Heinemann; 1991.
McConnell J. The management chondromalacia patellae: a long term
solution. The Australian Journal of Physiotherapy 1986;32(4):
215–23.
Mercer SJ, Rivett DA, Nelson RA. Stretching the iliotibial band: an
anatomical perspective. New Zealand Journal of Physiotherapy
1999;August:5–7.
Rouse SJ. The role of iliotibial tract in patellofemoral pain and
iliotibial band friction syndromes. Physiotherapy 1996;82(3):
199–202.
Sims K. Assessment and treatment of hip osteoarthritis. Manual
Therapy 1999;4(3):136–44.
Spencer J, Hayes K, Alexander I. Knee joint effusion and quadriceps
inhibition in man. Archives of Physical Medicine 1984;65:171–7.Tatum R. Ostechondritis dessicans of the knee: a radiological case
report. Journal of Manipulative and Physiological Therapeutics
2000;23(5):347–51.
Tomsich DA, Nitz JA, Threlkeld AG, Shapiro R. Patellofemoral
alignment reliability. Journal of Orthopaedic and Sports Physical
Therapy 1996;23(3):200–8.
Watson CW, Propps MM, Galt W, Dobbs D, Redding A. Reliability
of the McConnell classification system of static patellar orientation.
Journal of Sports Physical Therapy 1999;29(1):A-42.
ARTICLE IN PRESS
J. Davin, J. Selfe / Manual Therapy 11 (2006) 157–161 161