
David W. Denning National Aspergillosis Centre University ...
46
Lethal pulmonary fungal disease – ‘think fungus’ early David W. Denning National Aspergillosis Centre University Hospital of South Manchester The University of Manchester Global Action Fund for Fungal Infections
Transcript of David W. Denning National Aspergillosis Centre University ...

Lethal pulmonary fungal disease – ‘think fungus’ early
David W. Denning
National Aspergillosis Centre
University Hospital of South Manchester
The University of Manchester
Global Action Fund for Fungal Infections

OUR VISION IS TO REDUCE ILLNESS AND DEATH ASSOCIATED WITH FUNGAL DISEASES WORLDWIDE.
GAFFI Global Action Fund for Fungal Infections
LEAVE NO ONE BEHIND: Too many people have no access to life-saving fungal diagnostics and antifungal medicine. This has to change!

Deaths from fungal infections need to fall
Fungal Infection TB (2015) Malaria (2015)
>1,660,000
1,800,000
(200,000
with HIV)
429,000
www.GAFFI.org

Fungal infections
• Mucosal i.e. oral or vulvovaginal thrush
• Cutaneous i.e. athlete’s foot, ringworm and onychomycosis
• Chronic fungal infections such as chronic pulmonary aspergillosis
• Allergic i.e. allergic fungal sinusitis and allergic bronchopulmonary aspergillosis (ABPA)
• Invasive and life-threatening i.e. candidaemia, invasive aspergillosis and cryptococcal meningitis

Fungal infections
• Mucosal i.e. oral or vulvovaginal thrush
• Cutaneous i.e. athlete’s foot, ringworm and onychomycosis
• Chronic fungal infections such as chronic pulmonary aspergillosis
• Allergic i.e. allergic fungal sinusitis and allergic bronchopulmonary aspergillosis (ABPA)
• Invasive and life-threatening i.e. candidaemia, invasive aspergillosis and cryptococcal meningitis

Pegorie et al, J Infect 2017;74:60

Simple (single) aspergilloma
Patient NM
Positive Aspergillus antibodies in blood
Lobectomy
Wythenshawe Hospital
August 2006 May 2009
Community acquired New cough pneumonia requiring
ICU care

Irregular cavity walls – very characteristic of fungal growth in the cavity

Chronic cavitary pulmonary aspergillosis
National Aspergillosis Centre

Early Aspergillus infection of a pulmonary cavity – ‘pre-aspergilloma’
Aspergillus growth on the surface of a pulmonary cavity
Severo on www.aspergillus.man.ac.uk
Orderly hyphal growth on the inside of the cavity

Chronic cavitary pulmonary aspergillosis (CCPA) – coughing up blood (haemoptysis)
Wythenshawe Hospital

Progression of CCPA to
chronic fibrosing pulmonary aspergillosis
1992 1994 on no Rx 1997 still on no Rx

Denning DW et al, Chronic pulmonary aspergillosis – Rationale and clinical guidelines for diagnosis and management. Eur Resp J
2016;47:45-68.

Denning DW et al, Chronic pulmonary aspergillosis – Rationale and clinical guidelines for diagnosis and management. Eur Resp J
2016;47:45-68
Clinical phenotypes of chronic Aspergillus spp diseases
Single/simple
aspergilloma
Aspergillus
nodule(s)
Chronic cavitary pulmonary
aspergillosis (CCPA)
Chronic fibrosing
pulmonary aspergillosis
(CFPA)
Subacute Invasive aspergillosis
(SAIA) or chronic necrotizing
pulmonary aspergillosis (CNPA)
Treat as for IA – 6 months

Radiological diagnosis of CPA Population Intention Intervention SoR QoE Reference Comment
Features of cavitation, fungal ball, pleural thickening and/or upper lobe fibrosis
Raise suspicion of CPA for physicians
Radiological report must mention possible CPA
A
II
Roberts, 1987; Kim, 2000; Franquet, 2001; Denning, 2003; Greene, 2005; Kobashi, 2006; Godet, 2014
CPA is often missed for years and patients mismanaged. Microbiological testing required for confirmation High quality CT with vessel visualisation
Denning et al, Eur Resp J 2016;47:45

Aspergillus nodule
Muldoon E. BMC Pulm Med 2016 In press
Patients may have 1, 2 or more nodules
Cough and dyspnoea are common, 30% weight loss,
occcasional haemoptysis.
57% had positive IgG antibody

Figure 13 - Nodule of the right upper lobe with irregular and slightly spiculated borders that was surgically resected and
proven to be an Aspergillus nodule.
Spiculated nodule - aspergillosis
Denning et al, Eur Resp J 2016;47:45

Aspergillosis in COPD
www.GAFFI.org
• There is an overlap between COPD and asthma, now referred to as ‘asthma-COPD overlap syndrome (ACOS)’
• Many COPD patients are ‘colonised’ by Aspergillus - ~30% by high volume culture
• Aspergillus IgG antibody may be positive in COPD patients (~50%) – of uncertain clinical significance
• The commonest underlying disease for CPA in high income countries includes COPD
• Invasive aspergillosis complicates COPD in 1.3-3.9% of hospital admissions

Figure 6 – Aspergillus nodules of variable size and borders and fungus ball filling a cavity with a wall of variable thickness in a
patient with preexisting bronchiectasis and cicatricial atelectasis of the middle lobe. Successive axial views with lung windows.
Multiple Aspergillus nodules
Denning et al, Eur Resp J 2016;47:45

Differential diagnosis of patients with upper lobe disease, usually with
cavitation
• Pulmonary TB • Non-tuberculous mycobacterial infection (NTM) • Chronic pulmonary aspergillosis • Allergic bronchopulmonary aspergillosis (asthma) • Lung cancer (adeno, small cell or large cell) • Cavitating pneumonia – Pseudomonas,
Staphylococcus, Rhodococcus, Nocardia etc • Actinomycosis
• Chronic cavitary pulmonary histoplasmosis • Pulmonary coccidioidomycosis • Pulmonary paracoccidioidomycosis

Interaction of Aspergillus with the host
A unique microbial-host interaction
Immune dysfunction
Fre
quency of aspergillosis
Immune hyperactivity
Fre
quen
cy o
f as
perg
illo
sis
Acute IA
Subacute IA
Aspergillus keratitis Aspergillus bronchitis
Chronic pulmonary Otitis externa Onychomycosis
ABPA SAFS
Allergic sinusitis
. After Casadevall & Pirofski, Infect Immun 1999;67:3703
Lung/tissue damage

Important airborne fungi
Alternaria
Aspergillus
Cladosporium
Rhizopus

Common allergen exposures by month
Twaroch et al, Allergy Asthma Immunol Res 2015:7:205

O’Driscoll, unpublished
Skin prick testing for fungal asthma
Cladosporium +ve
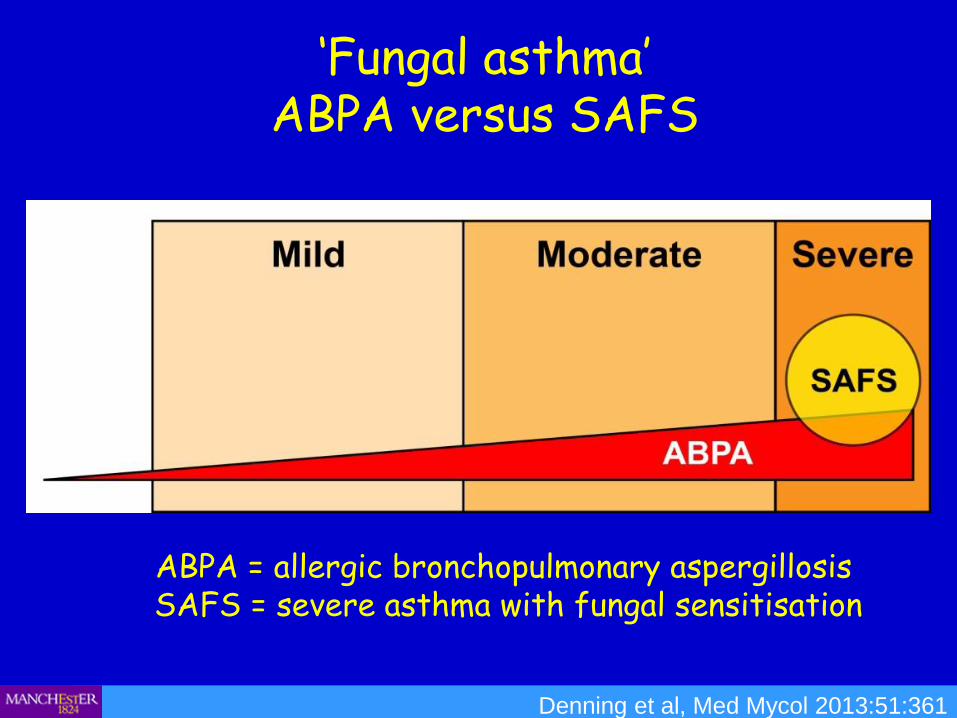
‘Fungal asthma’
ABPA versus SAFS
Denning et al, Med Mycol 2013:51:361
ABPA = allergic bronchopulmonary aspergillosis SAFS = severe asthma with fungal sensitisation

66% sensitised to one or more fungus:
45% to Aspergillus fumigatus
O’Driscoll R et al, Clin Exp All 2009;39:1677

Fraczek et al, J Allergy Clin Immunol 2017;in press
The mycobiome of fungal asthma
Oral corticosteroid is strongly associated with higher Aspergillus fungal loads (p < 0.01)

‘Fungal asthma’ in the UK
Pegorie et al, J Infect 2017;74:60

www.GAFFI.org
Fungal disease of the lungs in outside the hospital
~200 million adult asthmatics

Norback D, Occup Environ Med 2013;70:325-31.
7,104 young adults in 13 countries (11 Europe) Questionnaires, sensitisation to Alternaria and
Cladosporium, assessment of homes, asthma evaluation (metacholine challenge).
New onset asthma (n=355) Correlation with water damage and mould in the house Follow up 8.7 (5.9-11.7) years. Risk ratio for new asthma = 1.46 (water damage) and
1.3 (indoor moulds).

Retrospective comparison of itraconazole antifungal treatment of SAFS with ABPA
Pasquallotto et al, Respirology 2009;14:1121
22 patients with SAFS
were compared
with 11 with ABPA

Proof of concept RCT of itraconazole in SAFS – outcomes at 32 weeks
Quality of life outcome
Mean (95% CI) or % (n) P-value
Itraconazole Placebo
Change in AQLQ score +0.85 (0.28, 1.41)
-0.01 (-0.43, 0.42)
0.014
Improvement in AQLQ score of >0.75
54% (14) 18% (5) 0.013
Percentage change in total IgE (IU/L)
-27% (-14%, -38%)
+12% (-5%, +31%)
0.001
Change in FEV1 (L/min) -0.22 (-0.56, 0.11)
-0.02 (-0.16, 0.11)
NS
Change in FEV1 (% predicted) -3.66 (-9.39, 2.08)
0.13 (-3.67, 3.93)
NS
Change in average PEFR (am) 20.8 (3.5, 38.1)
-5.5 (-21.6, 10.7)
0.028
Change in average PEFR (pm) 16.8 (1.5, 35.2)
8.9 (-33.9, 51.8)
NS
Number needed to treat = 3.22
Denning et al, Am J Resp Crit Care Med 2009; 179:11

Risk groups and frequencies of invasive aspergillosis – different test performances
Herbrecht, Ann NY Acad Sci 2012;1271:23

Invasive aspergillosis by finished consultant episodes - UK
www.aspergillus.org.uk

IA in immunocompromised patients
Pegorie et al, J Infect 2017;74:60

COPD admissions (rate per 40+ years old)
www.GAFFI.org
OECD Health Statistics 2013, ttp://dx.doi.org/10.1787/health-data-en.

Aspergillus, IPA and COPD
~ 22% of
Aspergillus in
COPD = invasive
aspergillosis
~ 1.3% of COPD
admissions have
invasive
aspergillosis by
culture
www.GAFFI.org
Guinea et al. Clin Microbiol Infect 2010;16:870.
72% mortality of IPA

IA in COPD
www.GAFFI.org
Xu H et al. Clin Microbiol Infect 2012;18:403.
58 of the 298 COPD admissions with a lower respiratory
tract sample processed grew Aspergillus spp.
39 (3.9%) had probable IA.
Only 13% had oral corticosteroids
43% died

IA in lung disease patients - most probably being missed
Pegorie et al, J Infect 2017;74:60

Missed diagnoses in multiple intensive care units (31 studies, 5863 autopsies)
Winters et al, BMJ Qual Saf doi:10.1136/bmjqs-2012-000803
Most common serious infectious diagnostic errors were pneumonia and invasive aspergillosis

Invasive aspergillosis linked to influenza
Schauwvlieghe et al, TIMM 2017
Literature review – 68 cases of influenza-associated IA – 47% mortality.
Severe influenza admitted to 8 tertiary ICUs in
Netherlands Dec 2015 to April 2016
144 patients with influenza 23 (16%) had IA 14/23 (61%) died

Diagnostic tests – GM = aspergillus antigen; G = glucan
Immune compromised
Fre
quency of aspergillosis
Allergy - atopy
Fre
quen
cy o
f as
perg
illo
sis
Acute invasive
Subacute IA
Aspergilloma Chronic pulmonary
Aspergillus bronchitis
ABPA Severe asthma with fungal sensitisation
Allergic sinusitis
. After Casadevall & Pirofski, Infect Immun 1999;67:3703
Lung damage
GM test G test
IgG antibody test G test
IgE antibody test IgG antibody test
GM and Aspergillus PCR in BAL & respiratory samples

Pneumocystis pneumonia in the UK – all underlying diseases
Maini et al, Emerg Infect Dis 2013;10:386

Serious fungal disease in the UK
Pegorie et al, J Infect 2017;74:60

Conclusions
All forms of aspergillosis of the lungs are underdiagnosed, untreated and probably contribute to unnecessary morbidity, death and inappropriate antibiotic use.
In some populations, fungal disease is common, notably
severe asthma, CF, COPD in hospital with an infiltrate, influenza and complex patients
Early diagnosis is ideal, and may necessary for survival
We have good diagnostic tools and drugs – they need to be utilised
The global problem of fungal disease is huge

www.aspergillus.org.uk
17 years
Over 1M pages read monthly in >125 countries
Supported by the Fungal Infection Trust – 20 year anniversary in 2011
New section on drug interactions which you can search very quickly
+ app for iphones and android (search antifungal interaction)
691 interactions were rated as minor, 919 moderate and 381 severe,
= 2216 recorded interactions
![Aspergillosis - Youngstown State Universitypeople.ysu.edu/~crcooper01/Aspergillosis[1]- Katie Jacquie Qazi.pdf•People with Aspergillosis are in three distinct groups •Healthy immune](https://static.fdocuments.in/doc/165x107/5e3883b0e2f2970b7b1c24ad/aspergillosis-youngstown-state-crcooper01aspergillosis1-katie-jacquie-qazipdf.jpg)

![Clinical failure and its management David W. Denning Director, National Aspergillosis Centre University Hospital South Manchester [Wythenshawe Hospital]](https://static.fdocuments.in/doc/165x107/551796265503463e368b57c0/clinical-failure-and-its-management-david-w-denning-director-national-aspergillosis-centre-university-hospital-south-manchester-wythenshawe-hospital.jpg)















