Date of Lecture 29-9-2018 · missing tooth. If we have the upper or lower canine we should consider...
13
Faculty of Dentistry Batch of 2018 Date of Lecture 29-9-2018 Sheet Number 3 Doctor Fuad Kathim Written By Alaa’ Nashwan Corrected by Ruba Halasa Reference sheets in 2013 (if present) 2
Transcript of Date of Lecture 29-9-2018 · missing tooth. If we have the upper or lower canine we should consider...

Faculty of Dentistry Batch of 2018
Date of Lecture 29-9-2018
Sheet Number 3
Doctor Fuad Kathim
Written By Alaa’ Nashwan
Corrected by Ruba Halasa
Reference sheets in 2013
(if present) 2

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 2 | 13
Let's continue what we started talking about last lecture..
We talked about replacement of single missing tooth, and usually what we do is a
three-unit bridge; this bridge has 2 retainers, the first one is the mesial abutment
and the second one is the distal abutment, and the pontic which replaces the
missing tooth. If we have the upper or lower canine we should consider two
abutments, or we can prepare two mesial teeth "the lateral and central”, also we
talked about the use of cantilever bridge in cases where the upper lateral is
missing.
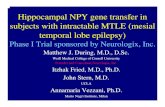
Problems associated with using the cantilever bridge are tipping, rotation and
drifting for the abutment, because in 3-unit bridge the forces are distributed on two
abutments rather than in one abutment in cantilever. "the figure below is from the book"
You must do proper assessment for the abutment before you start the preparation,
it's good idea to replace all previous amalgam or composite restoration on the
abutments, and after the removal of old restoration we decide if this tooth is
indicated for RCT or not. If a proper RCT was done for the abutment with proper
post and core the tooth can serve as abutment for the bridge.
We know that the walls for abutments should be parallel to each other, for
example if the 5 is missing the distal wall of the 4 should be parallel to mesial wall
of the 6 after preparation to have a proper path of insertion, but what if the

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 3 | 13
abutment is tilted? Here we may cut more from the tooth structure but if the tooth
is vital there is a risk of pulp exposure; so what are the options?
1- RCT then preparation.
2- Correction for the tilted tooth orthodontically.
3- Modify the preparation or the type of retainer used, instead of doing full
coverage for the tilted abutment do three quarter prep sparing the distal part of
tooth.
A student asked a question which I couldn't hear, but this is what the doctor
answered: in case of single tooth is missing we go for doing three unit bridge,
canine is large tooth subjected to heavy occlusion, the lateral is small so it will not
serve as good abutment so that's why we prepare two mesial abutments when the
canine is missing.
When I choose the abutment I think how the forces will be distributed? Forces
should distribute equally between the distal and mesial abutments.
Replacement of multiple missing teeth
Fixed prosthodontics becomes more difficult when several teeth are missing;
problems will be encountered when restoring a single long uninterrupted
edentulous area, or multiple edentulous areas with an intermediate pier abutment
especially when anterior and posterior teeth need to be replaced
with a single fixed prosthesis.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 4 | 13
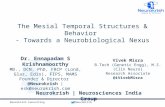
Here in this figure we have a tooth between
two edentulous areas and this tooth is called
"pier abutment".
The difficulty here is that I must prepare three
teeth; one of the requirements to get correct
preparation is that I have to prepare the three teeth in the figure above parallel to
each other and it's difficult to achieve this parallelism.
Under estimation of the problems involved in extensive or extended prosthesis can
lead to failure. to ensure a successful result we have to plan the prosthesis by
waxing the proposed or planned restoration on articulated diagnostic cast and then
study the case carefully.
One of the solutions for the case in figure above is to do 2 separate bridges, a 3
unit bridge on the 5, and 3 to replace the 4, fixed-movable retainer on 7 and
mobile retainer on 5, so now we have (1) fixed-fixed bridge, and (1) fixed-
movable bridge, and by this we avoid doing a long bridge.
Waxing up on the diagnostic cast is essential for the complex fixed prosthodontics
treatment, particularly where an irregular occlusal plane is to be corrected, the
vertical dimension of occlusion is to be altered and a planned supported prosthesis
is recommended or combination of fixed and removable prosthesis are to be used.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 5 | 13
look at this case, due to extraction and destruction of carious teeth , the patient had
such occlusion with low vertical dimension, so patient may have functional and
appearance problems so patient essentially needs to restore the vertical dimension
in order to provide space for placement of missing teeth.
To solve this problem you have to start by collecting data, doing a diagnostic
study model articulating the upper and lower casts after doing the wax pattern then
you can study the case (e.g. if you are considering veneers, discussing the wax up
with the patient is a good idea)
When you design a fixed bridge for multiple missing teeth you have to consider
these influencing factors;
A) Overloading of abutment teeth:
-The ability of the abutment teeth to accept applied forces without drifting or
becoming mobile must be estimated and has a direct influence on prosthodontics
treatment plan. These forces could be particularly severe during parafunctional
grinding, heavy occlusion and clenching, and the need to eliminate them becomes
obvious during restoration of such a damaged condition.
The first point you have to consider in order to avoid overloading abutment is the
direction of forces; whereas the magnitude of the forces is difficult to regulate, a
well fabricated FPD can distribute these forces in the most favorable way,
directing them in the long axis of abutment teeth. When we have multiple missing
teeth it's not always necessary to do full coverage, sometimes it's good to modify
the preparation. (in case of sound mesial and distal abutments, 2 or 3 quarter preps
may be a good option)

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 6 | 13
The second point you must consider avoiding overloading abutment is the root
surface area; Ante's law suggested in 1926 that it was unwise to provide a fixed
partial denture when the root surface area of the abutment was less than the root
surface area of the teeth being replaced.
- Surface area of the root of the abutments should be equal or more than
the surface area of the root of the missing teeth.
Imagine if we have missing first molar, and the surface areas of second premolar
and second molar are more than surface area of first molar. which is a good case.
But in case of two teeth missing (second premolar and first molar), compare their
surface area to the surface area of first premolar and second molar. the root surface
area for the 7 & 4 should be equal or more than the surface area of the teeth to be
replaced (5 & 6 so you have to study the case carefully you may need to do
preparation on canine and premolar)

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 7 | 13
This
table is from the book showing the root surface area for each tooth, not to
memorize of course but to understand the idea.
Third point you need to consider is Root shape and angulations, also an
important factor; When the tooth support is borderline, the shape of the roots and
their angulations should be considered. A molar with divergent root will provide
better support than molar with conical root and little or no inter-radicular bone. So
when the tooth has more than one root and the inter-radicular bone between roots
is more, it will serve as good abutment. Imagine a tree with only one root and
other one with multiple divergent roots, surely the second one is more strongly
attached to the ground same principle is applied to the teeth.
Periodontal disease should be considered; after horizontal bone loss from a
periodontal disease the periodontal ligament tissue supported root surface area can
be reduced because of conical shape of most roots when one third of root length
has been exposed half of the supporting area is lost.
so when a third of periodontal ligament of root are loss and bone loss occur, it will
cause loss of about half of a root support because it’s a conical shape root.
Ex. when we calculate the surface area of this third it's about a half of the surface
area of the whole root.
In addition, the forces applied to the supporting bone are magnified, because of
greater leverage associated with length of the clinical crown plus potentially
abutment need to be carefully assessed where significant bone loss has occurred.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 8 | 13
B) Length of edentulous span:
All fixed partial denture flex slightly when subjected to load, the longer the span
the greater the flexion, the relationship between deflection and length of the span
is not simply linear but varies with cube of length of the span.
So, when we have long span even if we did good preparation the patient will keep
visiting us complaining from de-cementation of the prosthesis and we need to re-
cement; why? Any type of bridges tends to deflect upon function; this deflection is
not simply linear. When I had one pontic in my prosthesis let’s suppose that the
deflection would be “X” when I had two pontics the cube of 2 is 8, so the amount
of deflection would be “8X”, when I had three pontics the amount of deflection
would be “27X” . This large deflection would present clinically by de-
cementation or fracturing of porcelain.
Excessive flexing under occlusal load may cause failure of long span fixed partial
denture it can lead to fracture of porcelain veneer, breakage in connector area of
the retainer or unfavorable tissue response, this renders the prosthesis prognosis
poor.
Replacement of multiple anterior teeth:
-Special consideration in this situation includes problems with appearance and the
need to resist laterally directed tipping forces.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 9 | 13
-The 4 mandibular incisors can usually be replaced by simple fixed partial denture
with a retainer on each canine, in the lower it's not usually necessary to include the
premolar; Final restoration is 6 unit bridge replace 4 lower anterior teeth.
-If a single incisor remains, it should be extracted because its retention will
unnecessarily complicate the design and fabrication of FPD, and can jeopardize
the long term results.
- the Mandibular incisors because of their small size teeth generally make poor
abutment, it is particularly important not to have over-contoured restorations on
these teeth because plaque control will be nearly impossible.
Thus the clinician may have a choice between a compromised esthetic (too thin
ceramic veneer) or pulp exposure during tooth preparation and elective Endo.
Sometimes when two centrals are missing we can do preparation on laterals they
will be good abutments, but the problem is the difficulty of having acceptable
esthetic restoration, always they become over contoured because these laterals are
too small also if we make over reduction we will end up with pulp exposure
because we need room for porcelain and we need more cutting.
Replacement of missing maxillary incisors:
The loss of several maxillary incisors is a much greater problem in term of esthetic
and providing support because of the curvature of arch, the forces directed against
the maxillary incisors which tends to tip of the abutment teeth (the canine is not
enough because there will be drifting in preparation, so you have to involve the
first premolar in preparation, so the missing upper incisors need two abutments
(canine and first premolar) at each end of a long span FPD (replacing all 4
maxillary incisors).
If anterior bone loss has been severe as can happen when teeth are lost due to
trauma or periodontal disease they may have a ridge defect. In those patient
(removable partial denture) should be considered especially when the patient has
high smile line since a fixed partial denture generally replace only the missing
tooth structure and not the supporting tissue. Sometimes we can use pink porcelain
to imitate the color of gingiva, but this is in limited scenarios.
Sequences of treatment plan:
when a patient needs have been identified and the appropriate corrected measures
have been determine, a logical sequence of steps must be decided on including the

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 10 | 13
treatment of symptoms, stabilization of deteriorating conditions(dental caries and
periodontal disease), the definitive therapy (prosthodontics) and then a program of
follow up care .
1- Treatment of symptoms:
The relief of this discomfort accompanying an acute condition is a priority items
in planned treatment, this discomfort can be due to one or more of the following
items: Fractured tooth, acute pulpitis, acute exacerbation of chronic pulpitis, dental
abscess, acute pericoronitis or gingivitis and myofacial pain dysfunction.
Fortunately most patients candidate for fixed prosthodontics do not seek treatment
for acute conditions, the patient who comes to you for bridge construction ,does
not come with acute pulpitis or pain, his chief complaint is replacement of missing
teeth (esthetic problem).
However, they may have a specific problem which should receive immediate
attention such as anterior cracks or broken porcelain veneer or fractured
removable partial prosthesis.
2- Stabilization of deteriorating conditions:
The second step of treatment plan is stabilization of deteriorating conditions such
as dental caries and periodontal disease by removing the etiological factor,
increasing patient resistance or doing both.
Dental caries treatment is approached by a conservative manner and teeth are
restored with a proper contoured plastic material.
Periodontal disease; chronic periodontitis, with continued irreversible bone loss
should be treated as early as possible. Proper removal of plaque is possible only if
Question:
If a patient come with fractured porcelain crack , how could you deal with this case?
By adding Composite by using special bonding agent after doing etching for porcelain using
hydrofluoric acid not phosphoric acid which is weaker acid.
Question: why we do not use phosphoric acid? And why we use it on enamel and dentine?
1- Phosphoric acid reacts with hydroxyapatite crystals, the byproduct of this reaction is
washable.
2- The hydroxyapatite(Ca10(PO4)6(OH)2) have H3PO4 or phosphate which is also part of
phosphoric acid so it's not considered a foreign material and they share the same
compositions.
3- Phosphoric acid has a high molecular weight so we do not expect a more occurrence of
penetration of this acid into the dentinal tubules.
4- The PKa of phosphoric acid is weak so we do not expect the formation of hydrogen ions.
So all these are reasons for using phosphoric acid on enamel and dentine.
2013 sheet…

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 11 | 13
the teeth are smooth and their contours allow unimpeded access to the gingival
sulci.
- So, the following are essential for stabilizing the condition:
Replacements of defective restoration, removal of carious lesion, recontouring of
Over-contoured crowns (especially in the furcation area) and oral hygiene
instructions and then start the definitive treatment.
Several therapeutic proposal may be applicable for a single patient and may range
in complexity from minimum restoration treatment with regular maintenance to
full mouth prosthodontic reconstruction proceeded by orthognathic surgery or
orthodontic treatment.
So first we control the acute condition, then stabilization then we start the
definitive treatment (removable or fixed). It's very important to start with making
wax pattern in order to study the case, predict the treatment outcome, show the
patient what's the final result would be and study how much space you have for
the prosthesis (could the space accommodate two teeth or a single tooth?), and
study it on the articulator.
Usually surgical procedures are scheduled first, followed by periodontics,
endodontics, orthodontics, fixed prosthodontics, (from restoration of a single tooth
to rehabilitation of the entire mouth), and finally removable prosthodontics.
Fixed Prosthodontics is only initiated after the preceding modalities have been
completed, this will permit modification of the original plan if unforeseen
difficulties surface during treatment.
for example; a tooth is indicated for RCT, porcelain core and then it will serve as
abutment, but after caries removal we find that it's non-restorable so now we have
to change treatment plan.
Occlusal adjustment are often necessary before the initiation of the fixed
prosthdontics, where extensive prosthodontics are to be provided, an accurate and
well tolerated occlusal relationship may be obtainable only if the discrepancy
between intercuspal position and centric relation is eliminated first.
The correct sequence of Tx is to start with correction of occlusion, followed by
anterior restorations, then posterior restorations, complex restorations then follow
up.
Further explanation; if a patient came complaining from missing anterior teeth and
posterior teeth also she has occlusal problems (deflection while attempting
maximum intercuspation position) the correct treatment steps are the above
mentioned, the doctor just repeated them.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 12 | 13
If both anterior and posterior teeth are to be restored, anterior teeth are usually
done first because they influence the border movement of the mandible and thus
the shape of occlusal surface of the posterior teeth.
We must start with anterior in order to create the anterior guidance as we said and
then go back for posterior restoration.
If the posterior teeth are restored first a subsequent change in the lingual contour
of the anterior teeth could require considerable adjustment of the posterior
restoration.
Restoring the opposing posterior segment at the same time is often advantageous,
this permits the development of efficient occlusal scheme through the application
of an additive wax technique, so one side of the mouth should be completed before
the other side treatment.
If I have lower and upper segment need bridges at the same side we create the
bridges at the same time so do impressions, put the models on the articulator then
make a wax pattern,
So we will have a proper occlusal relation, and a good space for what will be
added of restorative materials and we can do a proper marginal ridge to cuspal
relationship.
Restoring all four posterior segments at the same time might lead to considerably
more complications for the patient and the dentist including fracture of breaking of
the provisional restorations, discomfort with bilateral local anesthesia and
difficulties in confirming the accuracy of jaw relationship recordings.
Complex prosthodontics:
Carefully planned treatment sequencing is particularly important when complex
prosthodontic treatments involving alteration of the vertical dimension or a
combination of fixed and removable prostheses are required.
When patient has many missing teeth, loss of vertical dimension, wearing in teeth,
so how to treat this step by step?
Proper examination, vitality testing, periodontal chart, diagnostic casts and wax
pattern, ask the patients about their expectations, then think and evaluate the
abutments and how the force distribution would be, think about the periodontal
condition how much bone do you have, the oral hygiene is important it will
determine if the patient motivated or not.
So, consider all these when you're going to put your treatment plan.

University of Jordan Cons 5 Sheet #3 Faculty of Dentistry
P a g e 13 | 13
The doctor showed a case of a patient who has wearing of the teeth, loss in the
vertical dimension; how do we know that VOD has lost? By looking to patient
profile, we need to restore the vertical dimension by using night guard and
occlusal splint and creating a space and then start our restorations; crowning for
anterior teeth (upper and lower) and then the posterior restorations.
Always follow these steps for any case and don't forget the regular follow up
visits.
Follow up
A specific program of follow up care and regular recall is an essential part of the
treatment plan, The aim is to monitor dental health, identify the signs of disease
early, and initiate prompt corrective measures as necessary. The first lecture done Take a breath