Data Triangulation
27
Data Triangulation
description
Data Triangulation. Objectives:. At the end of the session, participants will be able to: Describe the role of data triangulation in program evaluation List data sources and approaches that can be used for triangulated analysis. Data Triangulation for M&E. - PowerPoint PPT Presentation
Transcript of Data Triangulation

Data Triangulation

Objectives:
At the end of the session, participants will be able to:
Describe the role of data triangulation in program evaluation
List data sources and approaches that can be used for triangulated analysis

Data Triangulation for M&E
Linking different information sources involving persons, place and time
Analysis of data from multiple sources can increase the validity and reliability of findings; it can corroborate findings and weakness of any one data source can be compensated for by the strengths of another
Analysis of program level data with outcome/impact level data can help substantiate the linkage between program interventions and population-level outcomes/impacts

Questions that data triangulation can help address:
Are interventions working and are they making a difference?
What changes in population-level outcome and impact indicators have been observed and what do they mean?
Can the observed changes in outcomes and impact indicators be attributed to program outputs?
Are the collective efforts being implemented on a large enough scale to impact the course of the epidemic?
Source: A framework for monitoring and evaluating HIV prevention programmes for most-at-risk populations. UNAIDS 2007

Source of data
Repeated HIV and/or STI prevalence surveys/surveillance
Repeated population surveys with behavioral data
Routine program or service delivery data
Quality of service assurance and quality improvement assessments
Qualitative studies (in-depth interviews, focus group discussions, key informant interviews, etc)
Source: A framework for monitoring and evaluating HIV prevention programmes for most-at-risk populations. UNAIDS 2007

When to do Data Triangulation
When interventions have been in place for a sufficient duration of time to reasonably expect that changes at the population level may be attributable to program interventions
When interventions have been implemented with sufficient intensity and with high enough coverage to reasonably expect effects to be observed in the target population.
When good program-level data (i.e outputs, coverage, quality of implementation are available) are available
When process evaluation indicates that program activities are being realized as planned.
Source: A framework for monitoring and evaluating HIV prevention programmes for most-at-risk populations. UNAIDS 2007

Considerations
Is there a culture of data sharing?
Are data from different sources representative of te population ofinterest?
Do the time frames of te data points match?

Example 1:
Female Sex Worker Program in Nepal
Family Health International

Logic of the program in Nepal Reach people with information to increase their
knowledge and awareness Provide services to allow them to act on that
knowledge Expand coverage of information and services so that
so that changes are observable at the population-level
Improve the quality of services while expanding coverage (e.g. STI treatment)
Information and good quality services for enough target group members will lead to service use, which will lead to safer behaviour and lower risk of exposure to HIV
Source: FHI Regional Office, Bangkok.

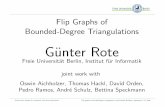
Number of sex workers reached and contacts by type of staff
02,0004,0006,0008,000
10,00012,00014,00016,000
2000 2001 2002 2003 2004
Year
Total Number Reached
Total Number of Contacts -Outreach WorkersTotal Number of Contacts -Peer Educators
FHI Nepal, 2005
Program records indicate the program is being delivered and reaching more of the target
population through more channels over time
Source: FHI Regional Office, Bangkok.

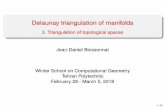
This increasing coverage is confirmed by FSWs in target areas
(exposure to NGO-related activities among FSWs, 1998 – 2002)
29 31
61.868.3
32.3 30
47.8
64.8
38.5
48
63
74
52
44.3
68
21.5 19.3
39.344.3
56.4
0
10
20
30
40
50
60
70
80
90
100
1998 1999 2000 2001 2002
Per
cent
age
(%)
Received condoms
Received brochures/booklets/pamphlets
Received other information about HIV/AIDS
Received items/information from all three sources
Source: FHI Regional Office, Bangkok.

There were signs of improved quality of services e.g. STI diagnosis and treatment
Quality Criteria Situation Prior to Dec. 2003 Current Situation
Treatment All STI patients receiving treatment as per the STI management guidelines. Drug quality needs to be standardized. Follow up visits are infrequent.
Compliance of the drug therapy cannot be assured with multi-dose drugs.
Drugs supply is of better quality. Drugs are mostly single dose and taken under direct observation, improving compliance
Clinic location & accessibility
Most static clinics placed centrally in the town and are easily accessible but mobile clinics are kept at DIC or government owned offices and changed from time to time
Static clinics which were not appropriately located have been changed and improved
Clinic setup Clinics have mostly 3 rooms one each for registration, consultation and laboratory test. Only some of the clinics have private rooms for consultation and examination
VCT now integrated into STI clinics, and a separate room for counseling has been added in most static clinics
Staffing Clinical teams consist of 3 persons: one medical officer, a staff nurse and a laboratory technician. Frequent turnover of the trained staff.
Addition of one trained VCT counselor in static clinics. Staff turnover rate has decreased.
Clinical Skill General history taking, general and genital examination are performed confidently, oral and anal examinations are not routinely conducted
Improved sexual history taking skills and clinical skills, but regular guidance still needed.
Source: FHI Regional Office, Bangkok.

Trends in desirable outcomes are evident – Knowledge of condoms is high among FSWs and condom carrying
behavior is increasing over time, 1998 - 2002
94.5 98 98.3 99.392.8 95.8 97.9 96.9
92.285
28.334.7
39.3
54.858.4
0102030405060708090
100
1998 1999 2000 2001 2002
Per
cen
tag
e (%
)
Ever heard of condoms
Know using condom can prevent HIV transmission
Usually carry condoms with them
Source: FHI Regional Office, Bangkok.

Trends in Desirable Outcomes are evident – Condom use with clients among FSWs is increasing steadily over
time, 1998 - 2002
77.582.3
94 95
61.867
87.3 90.3
3340.3
51 54.3
19.826.5
36.3 40.2
93.386
44.8
38.7
0102030405060708090
100
1998 1999 2000 2001 2002
Per
cen
tag
e (%
)
Ever use of condoms
Use of condoms with last client
Consistent use of condoms with clients in the past year
Gave condom to client at last sex
Source: FHI Regional Office, Bangkok.

Those Reached by the Program Have Safer Behaviors: Exposure to various NGO-related activities in the past year impacts on
consistent condom use with clients among FSWs - 2002
64.8 65.7
36.7 37.3
61.5
38.4
0
10
20
30
40
50
60
70
80
90
100
Received condoms Received brochures &materials
Received IPC informationabout HIV/AIDS
Co
nsi
sten
t Co
nd
om
Use
(%)
Exposed Unexposed
Source: FHI Regional Office, Bangkok.

There is evidence of a favourable Dose-Response relationship:
Greater exposure to various NGO-related activities results in better condom use behavior - 2002
24.6
33.3
75.8
28.2
39.7 42.1
6869.276.2
83.9
91.9
48.2
0
10
20
30
40
50
60
70
80
90
100
None Any one* Any two* All three*
Per
cen
tag
e (%
)
Carrying condoms Consistent condom use with clients
Consistent condom use with regular clients
*1) Received condoms, 2) received brochures/materials, 3) received IPC information about HIV/AIDS
Source: FHI Regional Office, Bangkok.

Summary of Key Findings among FSWs
Program activities have expanded in scale and improved in quality
HIV and STI prevalence are decreasing over time
Knowledge of condoms is high and consistent condom use is increasing and high among clients and regular clients
Exposure to NGO-related information sources about HIV/AIDS and condoms is increasing and high
Exposure to various NGO-related activities is increasing and high
Exposure to NGO-related activities is strongly linked with condom carrying & consistent condom use in a dose-response manner
Source: FHI Regional Office, Bangkok.

Example 2: Botswana
Antiretroviral scale-up in Botswana
National AIDS Committee Botswana,
WHO, UCSF and UNAIDS (2006)

Overview of Botswana Triangulation
Objective:
To develop a model to measure the impacts of ART and PMTCT programs on adult and child mortality
Application:
Provide timely information on the impact of national scale-up of ART for policy and programmatic decision making
Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Approach Meetings with stakeholders to identify objectives of
analysis
Identification and compilation of data from many sources Vital statistics (morbidity and mortality)
Population survey data
Patient Management systems (HMIS)
Program data (i.e. HIV testing, ART)
Examination of trends in HIV prevalence and mortality in relation to ART and PMTCT availability and service uptake
Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Conclusions of Botswana Analysis Since the inception the ART programme,
Botswana has achieved reductions in mortality of adults aged 25–54 years
Reduced mortality is associated with early initiation of district ART programmes and with the overall rate of ART uptake in the district.
Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.
Source: Case Study. Country-enhanced monitoring and evaluation for antiretroviral therapy scale-up: analysis and use of strategic information in Botswana. WHO 2006.

Strengths and Limitations of Triangulation
Strengths
Pre-existing data sources are used
Can provide relatively rapid results
Limitations
Existing data may be insufficient
Institutional barriers to data sharing

Triangulation Resources
HIV Triangulation Resource Guide: Synthesis of Results from Multiple Data Sources for Evaluation and Decision-making (WHO 2009)
Data Triangulation for HIV Prevention Program Evaluation in Low and Conncetrated Epidemics (FHI 2010)

MEASURE Evaluation is a MEASURE project funded by the
U.S. Agency for International Development and implemented by
the Carolina Population Center at the University of North Carolina
at Chapel Hill in partnership with Futures Group International,
ICF Macro, John Snow, Inc., Management Sciences for Health,
and Tulane University. Views expressed in this presentation do not
necessarily reflect the views of USAID or the U.S. Government.
MEASURE Evaluation is the USAID Global Health Bureau's
primary vehicle for supporting improvements in monitoring and
evaluation in population, health and nutrition worldwide.