Dari eBook
34
Neural tube defects: failure of the embryonic process of neurulation Failure of neural tube closure results in malformations termed neural tube defects (Copp, 1999). In craniorachischisis (Figure 8.4a), the most severe type of neural tube defect, the neural tube fails to close along most of the body axis, although the forebrain usually closes normally. If the neural tube fails to close specifically in the future brain, exencephaly results (i.e. exteriorization of the brain folds), which is converted to anencephaly (i.e. absence of brain) owing to neurodegeneration in later gestation. In contrast, if the low spine is primarily affected, this leads to open spina bifida (myelomeningocele; Figure 8.4b). Related to these open CNS defects are a series of ‘closed’ defects, in which the neural tube and/or meninges herniate through an opening in the skull or in the neural arches of the vertebral column. Brain herniation yields a defect called encephalocele, while herniation of the spinal cord is termed meningocele. A further category of neural tube defects are so-called ‘occult’ spina bifida (also called spinal dysraphism), which mainly affect the low spinal region and are skin-covered lesions in which the spinal cord may be split or tethered to the surrounding tissues, often in association with a bony spur or a fatty mass (lipoma). While covered lesions are protected from the potentially toxic amniotic environment, open neural tube defect lesions undergo erosion of the exposed neuroepithelium so that, by the late stages of gestation, the region of affected nervous system is largely degenerate, leading to severe disability or death after birth. Surgery on the human fetus during pregnancy, with the
-
Upload
marta-tata-salember -
Category
Documents
-
view
202 -
download
4
Transcript of Dari eBook

Neural tube defects: failure of the embryonic process of neurulationFailure of neural tube closure results in malformations termed neural tube defects(Copp, 1999). In craniorachischisis (Figure 8.4a), the most severe type of neural tube defect, the neural tube fails to close along most of the body axis, although the forebrain usually closes normally. If the neural tube fails to close specifically in the future brain, exencephaly results (i.e. exteriorization of the brain folds), which is converted to anencephaly (i.e. absence of brain) owing to neurodegeneration in later gestation. In contrast, if the low spine is primarily affected, this leads to open spina
bifida (myelomeningocele; Figure 8.4b).Related to these open CNS defects are a series of ‘closed’ defects, in which theneural tube and/or meninges herniate through an opening in the skull or in theneural arches of the vertebral column. Brain herniation yields a defect calledencephalocele, while herniation of the spinal cord is termed meningocele. A furthercategory of neural tube defects are so-called ‘occult’ spina bifida (also called spinaldysraphism), which mainly affect the low spinal region and are skin-covered lesions in which the spinal cord may be split or tethered to the surrounding tissues, often inassociation with a bony spur or a fatty mass (lipoma). While covered lesions areprotected from the potentially toxic amniotic environment, open neural tube defectlesions undergo erosion of the exposed neuroepithelium so that, by the late stages ofgestation, the region of affected nervous system is largely degenerate, leading to severedisability or death after birth. Surgery on the human fetus during pregnancy, with theaim of covering the neural tube defect lesion with muscle and skin, has shown thatthis process of degeneration can be halted (Johnson et al., 2003), minimizing damageto the exposed CNS but not recovering function.
Neural tube cacat: kegagalan proses embrio NeurulasiKegagalan hasil penutupan tabung saraf malformasi disebut cacat tabung saraf(Copp, 1999). Dalam craniorachischisis (Gambar 8.4a), jenis yang paling parah cacat neural tube, tabung saraf gagal menutup sebagian sepanjang sumbu tubuh, meskipun otak depan biasanya menutup normal. Jika tabung saraf gagal menutup khusus di otak depan, hasil eksensefali (exteriorization yaitu lipatan otak), yang dikonversi menjadi anencephaly (yaitu tidak adanya otak) karena neurodegeneration dalam kehamilan nanti. Sebaliknya, jika tulang belakang rendah terutama dipengaruhi, ini mengarah untuk membuka bifidabifida (myelomeningocele; Gambar 8.4b).Terkait dengan ini cacat SSP terbuka adalah serangkaian 'tertutup' cacat, di manatabung saraf dan / atau meninges herniate melalui lubang pada tengkorak atau dilengkungan saraf tulang belakang dari kolom. Herniasi otak menghasilkan cacat yang disebutencephalocele, sementara herniasi dari sumsum tulang belakang disebut Meningosel. A lebih lanjutkategori cacat tabung saraf yang disebut 'okultisme' spina bifida (juga disebut tulang belakangdysraphism), yang terutama mempengaruhi daerah tulang belakang rendah dan lesi kulit yang tertutup di mana sumsum tulang belakang mungkin akan dipecah atau ditambatkan ke jaringan sekitarnya, sering kali dalamasosiasi dengan sebuah bertulang memacu atau massa lemak (lipoma). Sementara lesi yang dibahas adalah

dilindungi dari lingkungan ketuban berpotensi beracun, neural tube defect bukalesi mengalami erosi neuroepithelium terkena sehingga, dengan tahap akhirkehamilan, wilayah sistem saraf yang terkena sebagian besar merosot, yang mengarah ke parahcacat atau meninggal setelah lahir. Operasi pada janin manusia selama kehamilan, dengantujuan untuk menutup lesi cacat tabung saraf dengan otot dan kulit, telah menunjukkan bahwaproses degenerasi dapat dihentikan (Johnson et al, 2003.), meminimalkan kerusakanke SSP disinari tetapi tidak memulihkan fungsi.
Genetic basis of neural tube defects The high recurrence risk in siblings and inclose relatives of individuals with neural tube defects suggests a strong genetic basis,although there is a marked lack of large families with neural tube defects, arguingagainst causation based on single genes. It has been suggested, therefore, that neuraltube defects have a multifactorial causation, with many genetic variants interacting todetermine individual risk of neural tube defect, and with a marked contribution ofenvironmental factors, both exacerbating and preventive. Since neural tube defectsare relatively common malformations (Table 8.1), the predisposing genetic variantsthemselves seem likely to be relatively common, or else there may be many differentcombinations of rare genetic variants that can predispose to neural tube defect. Inmice, more than 80 different mutant genes cause non-closure of the mouse neuraltube, with different mutations affecting different rostro-caudal levels of the body axis,thereby mimicking the human situation (Copp et al., 2003b). In contrast, only a fewof the mouse mutants exhibit closed neural tube defects, for example resemblingencephalocele. Despite the many genetic loci that have been implicated in mouseneural tube defects, few human genes have so far been definitively shown topredispose to human neural tube defects. The best known of these is the geneencoding 5,10-methylene tetrahydrofolate reductase (MTHFR), an enzyme of folicacid metabolism. MTHFR catalyses the reaction that produces 5-methyl tetrahydrofolate,a methyl donor for homocysteine during its conversion to methionine. Apolymorphic, thermolabile variant of the MTHFR gene (the C677T variant) exhibits ahigher frequency among neural tube defect cases and their families than amongnormal controls in several populations (Van der Put et al., 1997) and seemsresponsible for imparting an increased risk of neural tube defect, especially incombination with a low folate and/or vitamin B12 level during pregnancy.
Genetik dasar cacat tabung saraf Resiko rekurensi tinggi dalam saudara dan di kerabat dekat dari perorangan dengan cacat tabung saraf menunjukkan dasar genetik yang kuat, walaupun ada kekurangan ditandai keluarga besar dengan cacat tabung saraf, berdebat terhadap penyebab berdasarkan gen tunggal. Ia telah mengemukakan, karena itu, bahwa saraf cacat tabung memiliki penyebab multifaktorial, dengan banyak varian genetik berinteraksi untuk menentukan risiko individual neural tube defect, dan dengan kontribusi ditandai faktor lingkungan, baik memperburuk dan preventif. Sejak cacat tabung saraf adalah malformasi relatif umum (Tabel 8.1), varian genetik predisposisi sendiri tampaknya mungkin relatif umum, atau yang lain mungkin ada banyak berbeda kombinasi varian genetik langka yang dapat mempengaruhi terhadap cacat tabung saraf. Dalam tikus, lebih dari 80 gen mutan yang berbeda ini menyebabkan non-penutupan saraf mouse tabung, dengan mutasi yang berbeda mempengaruhi tingkat rostro-ekor yang berbeda dari sumbu

tubuh, dengan demikian meniru situasi manusia (Copp et al, 2003b.). Sebaliknya, hanya beberapa dari mouse mutan pameran ditutup cacat tabung saraf, misalnya menyerupai encephalocele. Meskipun banyak lokus genetik yang telah terlibat di mouse cacat tabung saraf, gen manusia hanya sedikit yang sejauh ini telah secara definitif terbukti predisposisi manusia cacat tabung saraf. Yang paling terkenal di antaranya adalah gen 5,10 encoding-metilen tetrahydrofolate reduktase (MTHFR), sebuah enzim folat metabolisme asam. MTHFR mengkatalisis reaksi yang menghasilkan tetrahydrofolate 5-metil, donor metil untuk homosistein selama konversi kepada metionin. A polimorfik varian, termolabil gen MTHFR (varian C677T) menunjukkan suatu frekuensi yang lebih tinggi di antara kasus cacat neural tube dan keluarga mereka dari antara kontrol normal dalam beberapa populasi (Van der Put et al, 1997.) dan tampaknya bertanggung jawab untuk menyampaikan peningkatan risiko neural tube defect, terutama di kombinasi dengan folat rendah dan / atau tingkat vitamin B12 selama kehamilan.
Environmental effects on occurrence of neural tube defects Many environmentalfactors have been demonstrated, in mice, to interact with the genotype to eitherincrease or decrease the risk of neural tube defect (Copp et al., 1990). Teratogenic (i.e.malformation increasing) influences range from physical factors such as hyperthermiato biologically active molecules such as retinoids (vitamin A derivatives). Inhumans, several of these agents are also suspected of increasing neural tube defect riskand the anti-epileptic drug sodium valproate, taken early in pregnancy, has conclusivelybeen demonstrated to predispose to spina bifida (Lammer et al., 1987). In180 EMBRYOS, GENES AND BIRTH DEFECTScontrast to these teratogenic influences, folic acid is well known to diminish the riskof neural tube defects in a proportion of predisposed human pregnancies (Wald et al.,1991) and in several mouse mutants with neural tube defect. While studies in micehave demonstrated that folic acid acts directly on the developing embryo, its precisemode of action remains elusive. Genetic predisposition to neural tube defect via theC677T variant of MTHFR leads to elevated levels of homocysteine, a trend that isreversed by administration of exogenous folic acid. Homocysteine has not beenfound to directly cause neural tube defects in experimental animals, however,suggesting that other embryonic defects, such as diminished embryonic cell proliferationor excessive cell death, may be the primary target of folic acid in preventingneural tube defects. A proportion of neural tube defects in both humans and mice donot respond to folic acid therapy. In one folate-resistant mouse mutant, curly tail,administration of the vitamin-like molecule inositol can prevent the great majority ofcases of spina bifida, through a molecular mechanism involving activation of specificisoforms of the enzyme family protein kinase C (Cogram et al., 2004). It remains tobe determined whether inositol will also prove to exert a preventive effect againsthuman neural tube defects.
Lingkungan efek pada terjadinya cacat tabung saraf Banyak lingkungan faktor telah ditunjukkan, pada tikus, untuk berinteraksi dengan genotipe baik meningkatkan atau mengurangi risiko neural tube defect (Copp et al, 1990.). Teratogenik (yakni

kelainan meningkat) berkisar pengaruh dari faktor-faktor fisik seperti hipertermia untuk biologis molekul aktif seperti retinoid (vitamin A derivatif). Dalam manusia, beberapa agen ini juga diduga meningkatkan resiko cacat tabung neural dan obat anti-epilepsi natrium valproate, diminum pada awal kehamilan, telah meyakinkan telah ditunjukkan untuk mempengaruhi untuk spina bifida (Lammer et al, 1987.). Dalam 180 embrio, GEN DAN CACAT LAHIR Berbeda dengan pengaruh teratogenik, asam folat dikenal untuk mengurangi risiko cacat tabung saraf dalam proporsi kehamilan manusia cenderung (Wald et al., 1991) dan di beberapa tikus mutan dengan cacat tabung saraf. Sementara penelitian pada tikus telah menunjukkan bahwa asam folat bekerja langsung pada embrio yang berkembang, tepat nya cara kerja tetap sukar ditangkap. Genetik predisposisi terhadap cacat neural tube melalui varian C677T dari MTHFR menyebabkan peningkatan kadar homosistein, sebuah tren yang terbalik dengan pemberian asam folat eksogen. Homosistein belum ditemukan langsung menyebabkan cacat tabung saraf pada hewan percobaan, bagaimanapun, menunjukkan bahwa cacat embrio lain, seperti proliferasi sel embrio berkurang atau kematian sel yang berlebihan, mungkin menjadi sasaran utama asam folat dalam mencegah cacat tabung saraf. Sebuah proporsi cacat tabung saraf di kedua manusia dan tikus melakukan tidak menanggapi terapi asam folat. Dalam satu tikus mutan tahan folat, ekor keriting, administrasi inositol molekul seperti vitamin dapat mencegah sebagian besar kasus spina bifida, melalui mekanisme molekuler yang melibatkan aktivasi khusus isoform dari keluarga enzim protein kinase C (Cogram et al, 2004.). Hal ini tetap ditentukan apakah inositol juga akan membuktikan mengerahkan efek pencegahan terhadap manusia cacat tabung saraf.
Embryonic mechanisms of neural tube defects In mice, the great majority ofneural tube defects arise from non-closure of the neural tube during neurulation.Analysis of the types of mutant gene (especially gene knock-outs) that lead to mouseneural tube defects has highlighted several embryonic mechanisms that appearessential for closure of the neural tube. In some cases, experimental studies haveconfirmed the importance of these developmental mechanisms in neurulation.Craniorachischisis. In this most severe neural tube defect, both cranial and spinalregions of the neural tube remain open (Figure 8.4a). The defect arises when theinitial event of neural tube closure (‘closure 1’) fails at the hindbrain–cervicalboundary. A small group of mouse mutant genes give rise to this neural tube defectand recent work has implicated these genes in the so-called ‘planar cell polarity’signalling pathway, in which Wnt/frizzled signals are transduced by a _-cateninindependentmechanism (Copp et al., 2003a). Hence, loss of function of Vangl2 (alsocalled strabismus), Celsr1, Scrb1, Ptk7 and double mutants for dishevelled-1 and -2,produce craniorachischisis in homozygous form. The planar cell polarity pathway isrequired for ‘convergent extension’, a net medially-directed movement of cells, withintercalation and rostro-caudal extension in the midline. Convergent extension failsin mice with planar cell polarity mutations, leading to short, broad embryos in whichthe neural folds are spaced widely apart. This wide spacing of the neural foldsprevents closure 1 and causes craniorachischisis (Greene et al., 1998).

Embrio mekanisme cacat tabung saraf Pada tikus, sebagian besarcacat tabung saraf timbul dari non-penutupan tabung saraf selama Neurulasi.Analisis jenis gen mutan (khususnya gen knock-out) yang mengarah pada tikuscacat tabung saraf telah menyoroti mekanisme beberapa embrio yang munculpenting untuk penutupan tabung saraf. Dalam beberapa kasus, peneliti jugamenegaskan pentingnya mekanisme ini perkembangan pada Neurulasi.Craniorachischisis. Dalam hal ini cacat tabung saraf yang paling parah, baik tengkorak dan tulang belakangdaerah dari tabung saraf tetap terbuka (Gambar 8.4a). Cacat muncul ketikaacara awal penutupan tabung saraf ('penutupan 1') gagal di-otak belakang leher rahimbatas. Sekelompok kecil dari mouse gen mutan ini menimbulkan neural tube defectdan pekerjaan terakhir telah terlibat gen tersebut dalam 'polaritas sel planar' yang disebutsinyal jalur, di mana Wnt / sinyal frizzled adalah transduced oleh cateninindependent-_mekanisme (Copp et al, 2003a.). Oleh karena itu, hilangnya fungsi Vangl2 (jugadisebut strabismus), Celsr1, Scrb1, Ptk7 dan mutan ganda untuk kusut-1 dan -2,menghasilkan craniorachischisis dalam bentuk homozigot. Jalur sel planar polaritas adalahdiperlukan 'ekstensi konvergen' untuk, gerakan medial-diarahkan bersih sel, denganinterkalasi dan penyuluhan rostro-ekor di garis tengah. Konvergen ekstensi gagalpada tikus dengan mutasi polaritas sel planar, yang mengarah ke pendek, embrio yang luas di manalipatan saraf berjarak luas terpisah. Ini jarak luas saraf lipatanmencegah craniorachischisis penutupan 1 dan menyebabkan (Greene et al, 1998.).
Exencephaly and anencephaly. Many mutant genes and a large number of teratogenscause cranial neural tube defects in the mouse, with the neural tube failing toclose in the future brain (Figure 8.4b). Analysis of the genetic models has revealedseveral critical events in cranial neurulation that are required for successful brainCH 08 BRAIN AND SPINAL CORD 181closure (Copp et al., 2003b). The initial elevation of the cranial neural folds requiresexpansion of the cranial mesenchyme, as a result of cell proliferation and increase inextracellular space. This causes the elevating neural folds to adopt a bi-convexappearance, particularly in the midbrain. Mice with loss of function of the Twist orCart1 genes have cranial neural tube defects in which the principal defect is areduction in the proliferation and expansion of the cranial mesenchyme (Chen andBehringer, 1995; Zhao et al., 1996).
Eksensefali dan anencephaly. Banyak mutan gen dan sejumlah besar teratogenmenyebabkan cacat tabung saraf kranial dalam mouse, dengan tabung saraf gagaldekat di otak masa depan (Gambar 8.4b). Analisis model genetik telah mengungkapkankritis beberapa peristiwa di Neurulasi tengkorak yang diperlukan untuk sukses otakCH 08 OTAK DAN sumsum tulang belakang 181penutupan (Copp et al, 2003b.). Elevasi awal dari lipatan saraf kranial membutuhkanperluasan mesenkim tengkorak, sebagai akibat dari proliferasi sel dan peningkatanruang ekstraselular. Hal ini menyebabkan neural mengangkat lipatan untuk mengadopsi bi-cembung

penampilan, khususnya di otak tengah. Tikus dengan hilangnya fungsi Twist atauGen Cart1 memiliki cacat tabung saraf kranial dimana cacat utama adalahpengurangan proliferasi dan perluasan mesenkim tengkorak (Chen danBehringer, 1995; Zhao et al, 1996)..
Once the bi-convex neural folds have formed, a second phase of cranial neurulationoccurs in which the dorsolateral aspects of the neural fold bend medially,allowing the folds to adopt a bi-concave morphology and approach the dorsalmidline for fusion. This second phase is highly dependent on the actin cytoskeleton,as illustrated by mice mutant for shroom, a gene involved in generating actinmicrofilaments, which fail to close their brains (Hildebrand and Soriano, 1999).The initiation of cranial neural crest emigration from the neural fold apices is alsorequired, as shown by mice overexpressing connexin 43, which exhibit defects ofcranial neural crest emigration and exencephaly (Ewart et al., 1997). A thirdrequirement for cranial closure is precise regulation of programmed cell death(apoptosis). Knock-out mice with either increased (e.g. AP-2_, bcl10 and Tulp1)or decreased (e.g. Apaf-1, caspase 9 and p53) apoptosis exhibit cranial neural tubedefects (Copp et al., 2003b). Apoptosis appears to synergize with neural crest cellemigration, to enable the conversion from bi-convex to bi-concave morphology. Inaddition, apoptosis at the neural fold tips may be necessary for midline epithelialremodelling, once the neural folds have met in the midline, since inhibition ofapoptosis in the chick embryo prevents midline remodelling (Weil et al., 1997).Cranial closure also requires precisely coordinated cell proliferation in the neuraltube: mice mutant for RBP-J_, Hes1 and Numb show premature differentiation of theneuroepithelium and failure of brain closure (Copp et al., 2003b).
Setelah lipatan saraf bi-cembung telah membentuk, fase kedua Neurulasi tengkorak terjadi di mana aspek dorsolateral dari lipatan neural tikungan medial, memungkinkan lipatan untuk mengadopsi morfologi bi-cekung dan pendekatan punggung yang midline untuk fusi. Tahap kedua ini sangat tergantung pada sitoskeleton aktin, seperti yang digambarkan oleh tikus mutan untuk shroom, sebuah gen yang terlibat dalam menghasilkan aktin mikrofilamen, yang gagal menutup otak mereka (Hildebrand dan Soriano, 1999). Inisiasi emigrasi puncak tengkorak syaraf dari Apeks flip saraf juga diperlukan, seperti yang ditunjukkan oleh tikus overexpressing connexin 43, cacat pameran mana
emigrasi cranial neural crest dan eksensefali (Ewart et al, 1997.). Sepertiga persyaratan untuk penutupan tengkorak adalah peraturan yang tepat dari kematian sel terprogram
(Apoptosis). Knock-out tikus dengan baik meningkat (misalnya AP,-2_ bcl10 dan Tulp1) atau dikurangi (misalnya Apaf-1, caspase 9 dan p53) tabung menunjukkan apoptosis saraf kranial cacat (Copp et al, 2003b.). Apoptosis muncul untuk bersinergi dengan sel puncak neural emigrasi, untuk mengaktifkan konversi dari bi-cembung untuk morfologi bi-cekung. Dalam Selain itu, apoptosis di ujung saraf lipat mungkin diperlukan untuk epitel garis tengah renovasi, setelah lipatan saraf telah bertemu di garis tengah, karena penghambatan

apoptosis dalam embrio ayam mencegah remodeling garis tengah (Weil et al, 1997.). penutupan cranial juga membutuhkan tepat terkoordinasi proliferasi sel dalam saraf tube: tikus mutan untuk RBP-J_, Hes1 dan Numb menunjukkan diferensiasi dini neuroepithelium dan kegagalan penutupan otak (Copp et al, 2003b.).
Open spina bifida. A number of mouse mutants exhibit low spinal neurulationdefects leading to open spina bifida (Figure 8.4b). Here, the critical event appears tobe regulation of dorsolateral bending of the neural plate. In contrast to the cranialregion, dorsolateral bending in the spine does not require emigration of the neuralcrest (which begins after neurulation in the spine) or function of the actincytoskeleton (Ybot-Gonzalez and Copp, 1999). Instead, sonic hedgehog (Shh)signalling appears critical for regulation of dorsolateral bending. Shh is producedby the notochord underlying the ventral neural plate and inhibits dorsolateralbending (Ybot-Gonzalez et al., 2002). In the absence of Shh, for example in theShh mutant mouse, dorsolateral bending occurs as a default mechanism that ensuresspinal closure. Overstimulation of the Shh signalling pathway, on the other hand, isincompatible with spinal closure. Hence in the Ptc1 and Opb mouse mutants,dorsolateral bending is absent and homozygotes fail to close their low spinal neuraltube (Eggenschwiler and Anderson, 2000; Goodrich et al., 1997). In contrast, the curlytail mutant does not lack dorsolateral bending but apposition of the neural folds ishampered, owing to ventral curvature of the caudal body axis (Brook et al., 1991),182 EMBRYOS, GENES AND BIRTH DEFECTSsecondary to an underproliferation of ventral cell types (Copp et al., 1988), so that aproportion of homozygotes exhibit open spina bifida.
Buka spina bifida. Sejumlah tikus mutan menunjukkan Neurulasi tulang belakang rendah cacat terkemuka untuk membuka spina bifida (Gambar 8.4b). Di sini, peristiwa penting tampaknya menjadi peraturan dorsolateral lentur dari pelat saraf. Berbeda dengan tengkorak wilayah, dorsolateral membungkuk di tulang belakang tidak memerlukan emigrasi dari saraf puncak (yang dimulai setelah Neurulasi di tulang belakang) atau fungsi actin yang sitoskeleton (Ybot-Gonzalez dan Copp, 1999). Sebaliknya, sonic hedgehog (Shh) muncul sinyal penting untuk peraturan dorsolateral lentur. Shh diproduksi oleh notochord mendasari piring saraf ventral dan menghambat dorsolateral membungkuk (Ybot-Gonzalez et al, 2002.). Dengan tidak adanya Sst, misalnya di Shh mouse mutan, dorsolateral membungkuk terjadi sebagai mekanisme default yang memastikan penutupan tulang belakang. Overstimulation dari jalur Sst sinyal, di sisi lain, tidak kompatibel dengan penutupan tulang belakang. Maka pada tikus mutan Ptc1 dan OPB, dorsolateral bending tidak ada dan homozigot gagal untuk menutup saraf tulang belakang mereka yang rendah tabung (Eggenschwiler dan Anderson, 2000; Goodrich et al, 1997.). Sebaliknya, keriting ekor mutan tidak kekurangan tapi lentur dorsolateral aposisi dari lipatan saraf tiruan adalah

terhambat, karena kelengkungan ventral sumbu tubuh ekor (Brook et al, 1991.), 182 embrio, GEN DAN CACAT LAHIR sekunder ke underproliferation jenis sel ventral (Copp et al, 1988.), sehingga menunjukkan proporsi homozigot spina bifida terbuka.
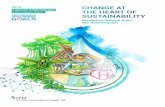
Figure 8.4 Neural tube defects and neuronal migration disorders. (a,b) Mouse fetuses at E15.5 toillustrate the appearance of craniorachischisis, in a Celsr1 mutant (a) and exencephaly and openspina bifida, in a curly tail mutant (b). In craniorachischisis, the neural tube is open from midbrainto low spine (between the thin arrows in A). Exencephaly in the curly tail fetus is restricted to themidbrain (thin arrow in b), while the spina bifida affects the lumbosacral region (arrowhead in b).Note the presence of a curled tail in both fetuses (thick arrows in a and b). (c) The various types ofneuronal migration disorder displayed diagrammatically on a coronal section of a postnatal human

brain. The left side shows large-scale defects, while the right side shows typical focal lesions. Seetext for description of the different types of neuronal migration disorder. Parts (a) and (b) arereproduced with permission from Copp et al. (2003b) and part (c) from Copp and Harding (1999) Gambar 8.4 cacat tabung syaraf dan gangguan migrasi neuronal. (a, b) Mouse janin di E15.5 untukmenggambarkan munculnya craniorachischisis, dalam Celsr1 mutan (a) dan eksensefali dan terbukaspina bifida, dalam ekor keriting mutan (b). Dalam craniorachischisis, tabung saraf terbuka dari otak tengahuntuk tulang belakang rendah (di antara anak panah tipis di A). Eksensefali pada janin ekor keriting adalah terbatas padaotak tengah (panah tipis dalam b), sedangkan spina bifida mempengaruhi daerah lumbosakral (panah di b).Perhatikan adanya meringkuk ekor di kedua janin (panah tebal dalam a dan b). (c) berbagai jenisgangguan migrasi neuronal ditampilkan diagram di bagian koronal manusia pascakelahiranotak. Sisi kiri menunjukkan cacat besar-besaran, sementara sisi kanan menunjukkan lesi fokal khas. Lihatteks untuk deskripsi dari berbagai jenis gangguan migrasi neuronal. Bagian (a) dan (b) adalahdireproduksi dengan izin dari Copp et al. (2003b) dan bagian (c) dari Copp dan Harding (1999)
Dysraphism, or Rachischisis(Encephaloceles and Spina Bifida)Included under this heading are the large number of disorders offusion of dorsal midline structures of the primitive neural tube, aprocess that takes place during the first 3 weeks of postconceptuallife. Exogenous factors are presumed to be operative in most cases.The entire cranium may be missing at birth, and the undevelopedbrain lies in the base of the skull, a small vascular mass withoutrecognizable nervous structures. This state, anencephaly, has beendiscussed earlier, under “Disturbances of Neuronal Migration,” andit is the most frequent of the rachischises. It has many associationswith other conditions in which the vertebral laminae fail to fuse.An eventration of brain tissue and its coverings through anunfused midline defect in the skull is called an encephalocele.

Frontal encephaloceles may deform the forehead or remain occult.Associated defects of the frontal cortex, anterior corpus callosum,and optic-hypothalamic structures as well as CSF leakage into frontalor ethmoid sinuses pose a risk of meningitis. Some of thesechildren are relatively normal mentally. Far more severe are theposterior encephaloceles, some of which are enormous and are attendedby grave neurologic deficits. However, lesser degrees of thedefect are well known and may be small or hidden, such as a meningoencephaloceleconnected with the rest of the brain through asmall opening in the skull. Small nasal encephaloceles may causeno neurologic signs, but if they are mistaken for nasal polyps andsnipped off, CSF fistulae may result. The larger occipital ones areassociated with blindness, ataxia, and mental retardation.
Dysraphism, atau Rachischisis (Encephaloceles dan spina bifida) Termasuk dalam pos ini adalah jumlah besar gangguan fusi struktur garis tengah dorsal tabung saraf primitif, proses yang berlangsung selama 3 minggu pertama postconceptual hidup. faktor eksogen yang diduga operasi dalam kebanyakan kasus. Seluruh tengkorak mungkin hilang pada saat kelahiran, dan berkembang otak terletak di dasar tengkorak, massa pembuluh darah kecil tanpa dikenali gugup struktur. Keadaan ini, anencephaly, telah dibahas sebelumnya, di bawah "Gangguan saraf Migrasi," dan ini adalah yang paling sering dari rachischises. Ini telah banyak asosiasi dengan kondisi lain di mana lamina vertebra gagal sekering. Sebuah eventration dari jaringan otak dan penutup melalui sebuah cacat garis tengah tidak disatukan dalam tengkorak disebut encephalocele sebuah. encephaloceles Frontal mungkin cacad dahi atau tetap tersembunyi. Asosiasi cacat dari korteks frontal, corpus callosum anterior, optik-hipotalamus dan struktur serta kebocoran CSF ke frontal atau sinus ethmoid menimbulkan risiko meningitis. Beberapa anak-anak relatif normal mental. Jauh lebih parah adalah posterior encephaloceles, beberapa di antaranya sangat besar dan dihadiri oleh defisit neurologis kuburan. Namun, lebih rendah derajat dari cacat sudah dikenal dan mungkin kecil atau tersembunyi, seperti meningoencephalocele dihubungkan dengan sisa otak melalui kecil membuka dalam tengkorak. encephaloceles hidung kecil dapat menyebabkan tidak ada tanda-tanda neurologis, tetapi jika mereka keliru untuk polip hidung dan dipotong off, fistula CSF akan terjadi. Yang oksipital yang lebih besar terkait dengan kebutaan, ataksia, dan keterbelakangan mental.
A failure of development of the midline portion of the cerebellum,referred to earlier, forms the basis of the Dandy-Walkersyndrome (Fig. 38-2). A cyst-like structure, representing the greatly

dilated fourth ventricle, expands in the midline, causing the occipitalbone to bulge posteriorly and displace the tentorium and torculaupward. In addition, the cerebellar vermis is aplastic, the corpuscallosum may be deficient or absent, and there is dilatation of theaqueduct as well as the third and lateral ventricles.Even more frequent are abnormalities of closure of the vertebralarches. These take the form of a spina bifida occulta, meningocele,and meningomyelocele of the lumbosacral or otherregions. In spina bifida occulta, the cord remains inside the canal andthere is no external sac, although a subcutaneous lipoma or a dimpleor wisp of hair on the overlying skin may mark the site of thelesion. In meningocele, there is a protrusion of only the dura andarachnoid through the defect in the vertebral laminae, forming acystic swelling usually in the lumbosacral region; the cord remainsin the canal, however. In meningomyelocele, which is 10 times asfrequent as meningocele, the cord (more often the cauda equina) isextruded also and is closely applied to the fundus of the cysticswelling.
Sebuah kegagalan pengembangan bagian garis tengah otak kecil,disebut sebelumnya, membentuk dasar dari Dandy-Walkersindrom (Gbr. 38-2). Struktur kista seperti, mewakili sangatdilatasi ventrikel keempat, memperluas di garis tengah, menyebabkan oksipitaltulang untuk tonjolan posterior dan menggantikan tentorium dan torculake atas. Selain itu, vermis cerebellum adalah aplastik, korpuscallosum mungkin kekurangan atau tidak ada, dan ada dilatasi darisaluran air serta ventrikel ketiga dan lateral.Bahkan lebih sering adalah kelainan dari penutupan tulang belakanglengkungan. Ini mengambil bentuk spina bifida occulta, Meningosel,dan meningomyelocele dari lumbosakral atau lainnyadaerah. Pada spina bifida occulta, kabel tetap di dalam kanal dantidak ada kantung eksternal, meskipun lipoma subkutan atau sebuah lesung pipiatau gumpalan rambut di kulit di atasnya dapat menandai lokasilesi. Dalam Meningosel, ada tonjolan hanya dura danarakhnoid melalui cacat dalam lamina vertebra, membentukpembengkakan kistik biasanya di daerah lumbosakral, kabel tetapdi kanal, namun. Dalam meningomyelocele, yang 10 kalisering sebagai Meningosel, kabel (lebih sering bagian cauda equina) adalahdiekstrusi juga dan erat diterapkan pada fundus dari kistikpembengkakan.
The incidence of spinal dysraphism (myeloschisis), like thatof anencephaly, varies widely from one locale to another, and thedisorder is more likely to occur in a second child if one child hasalready been affected (the incidence then rises from 1 per 1000 to

40 to 50 per 1000). Exogenous factors (e.g., potato blight in Ireland)have been implicated in the genesis of both myeloschisis andanencephaly. Folic acid, given before the 28th day of pregnancy,can be protective; vitamin A may also have slight protective benefit.As with anencephaly, the diagnosis can often be inferred fromthe presence of _-fetoprotein in the amniotic fluid (sampled at 15to 16 weeks of pregnancy) and the deformity confirmed by ultrasoundin utero, as mentioned earlier in this chapter. Blood contaminationis a source of error in the fetoprotein test (Milunsky). Acetylcholinesteraseimmunoassay, done on amniotic fluid, is anotherreliable means of confirming the presence of neural tube defects.
Insiden dysraphism tulang belakang (myeloschisis), seperti itudari anencephaly, sangat bervariasi dari satu lokal ke yang lain, dangangguan yang lebih mungkin terjadi pada anak kedua jika seorang anak telahsudah terpengaruh (kejadian kemudian naik dari 1 per 1000 untuk40 sampai 50 per 1000). Faktor eksogen (misalnya, kentang hawar di Irlandia)telah terlibat dalam asal-usul myeloschisis baik dananencephaly. Asam folat, diberikan sebelum hari ke 28 kehamilan,dapat menjadi pelindung; vitamin A juga mungkin memiliki manfaat perlindungan sedikit.Seperti anencephaly, diagnosis seringkali dapat disimpulkan darikehadiran _-fetoprotein dalam cairan ketuban (sampel di 15sampai 16 minggu kehamilan) dan deformitas dikonfirmasikan dengan ultrasounddi dalam rahim, seperti yang disebutkan sebelumnya dalam bab ini. Darah kontaminasimerupakan sumber kesalahan dalam uji fetoprotein (Milunsky). Acetylcholinesteraseimmunoassay, dilakukan pada cairan ketuban, yang lainberarti dapat diandalkan untuk mengkonfirmasi kehadiran cacat tabung saraf....
Some parents, on receiving this information, request abortion.In the case of meningomyelocele, the child is born with a largeexternalized lumbosacral sac covered by delicate, weeping skin. Itmay have ruptured in utero or during birth, but more often thecovering is intact. There is severe dysfunction of the cauda equinaroots or conus medullaris contained in the sac. Stroking of the sacmay elicit involuntary movements of the legs. As a rule the legsare motionless; urine dribbles, keeping the patient constantly wet;there is no response to pinprick over the lumbosacral zones; andthe tendon reflexes are absent. In contrast, craniocervical structuresare normal unless a Chiari malformation is associated (see furtheron). Differences are noted in the neurologic picture depending onthe level of the lesion. If it is entirely sacral, bladder and bowelsphincters are affected but legs escape; if lower lumbar and sacral,the buttocks, legs, and feet are more impaired than hip flexors andquadriceps; if upper lumbar, the feet and legs are sometimes sparedand ankle reflexes retained, and there may be Babinski signs. Thetwo dreaded complications of these severe spinal defects are meningitis

and progressive hydrocephalus from a Chiari malformation,which is often associated (see below). The subject of neural tubedefects has been reviewed by Botto and colleagues.
Beberapa orang tua, pada menerima informasi ini, permintaan aborsi.Dalam kasus meningomyelocele, anak lahir dengan besarexternalized sac lumbosakral tertutup oleh halus, kulit menangis. Inimungkin telah pecah dalam rahim atau selama melahirkan, tetapi lebih seringmeliputi utuh. Ada disfungsi berat dari bagian cauda equinaakar atau medullaris konus yang terkandung dalam kantung. Membelai dari kantungmungkin menimbulkan gerakan tak terkendali dari kaki. Sebagai aturan kakiyang bergerak; urin menggiring, menjaga agar pasien tetap selalu basah;tidak ada respon untuk cocokan peniti atas zona lumbosakral danrefleks tendon tidak hadir. Sebaliknya, struktur craniocervicaladalah normal kecuali malformasi Chiari berhubungan (lihat lebih lanjutaktif). Perbedaan dicatat dalam gambar neurologis tergantung padatingkat lesi. Jika seluruhnya sakral, kandung kemih dan usussphincters yang terpengaruh tapi kaki melarikan diri, jika lumbal lebih rendah dan sakral,pantat, kaki, dan kaki lebih terganggu dari fleksor pinggul danquadriceps, jika lumbal atas, kaki dan kaki kadang-kadang diselamatkandan refleks pergelangan kaki dipertahankan, dan mungkin ada tanda-tanda Babinski. Thedua komplikasi ditakuti dari cacat tulang belakang parah meningitisdan progresif hidrosefalus dari malformasi Chiari,yang sering diasosiasikan (lihat di bawah). Subyek tabung sarafcacat telah ditinjau oleh Botto dan rekan.
Treatment Opinions as to proper management vary considerably.Excision and closure of the coverings of the meningomyelocele inthe first few days of life is advised if the objective is to prevent afatal meningitis. After a few weeks or months, as hydrocephalusreveals its presence by rapid increase in head size and enlargementof the ventricles on the CT scan, a ventriculoatrial or ventriculoperitonealshunt is required. Patients with high spinal lesions andtotal paraplegia, kyphosis, hydrocephalus, and other major congenitalanomalies are usually not accepted for treatment. Less than 30percent of such patients survive beyond 1 year, and the long-termresults of treating these patients have not been encouraging. Lorberand others report that 80 to 90 percent of their surviving patientsare mentally retarded to some degree and are paraplegic—thustotally dependent on others for their care. The decision to undertakerather formidable surgical procedures is being questioned more andmore frequently. Exceptionally, the patient with meningomyelocele,and most of those with lumbar meningocele, are mentallynormal. Clinical differentiation of this mental state is obviouslyimportant.

Opini Perawatan untuk pengelolaan yang baik sangat bervariasi.Eksisi dan penutupan penutup dari meningomyelocele dibeberapa hari pertama kehidupan dianjurkan jika tujuannya adalah untuk mencegahfatal meningitis. Setelah beberapa minggu atau bulan, seperti hidrosefalusmengungkapkan kehadirannya dengan peningkatan pesat dalam ukuran kepala dan pembesarandari ventrikel pada CT scan, sebuah ventriculoatrial atau ventriculoperitonealshunt diperlukan. Pasien dengan lesi tulang belakang tinggi dantotal paraplegia, kyphosis, hydrocephalus, dan besar lainnya bawaananomali biasanya tidak diterima untuk pengobatan. Kurang dari 30persen pasien tersebut bertahan lebih 1 tahun, dan jangka panjanghasil mengobati pasien ini belum menggembirakan. Lorberdan lain-lain melaporkan bahwa 80 hingga 90 persen pasien mereka yang masih hidupsecara mental terbelakang untuk beberapa derajat dan lumpuh-sehinggasepenuhnya tergantung pada orang lain untuk perawatan mereka. Keputusan untuk melakukanprosedur pembedahan lebih tangguh sedang dipertanyakan lebih danlebih sering. Selain itu, pada pasien dengan meningomyelocele,dan kebanyakan dari mereka dengan Meningosel lumbal, secara mentalnormal. Diferensiasi klinis kondisi mental ini jelaspenting.
Other Developmental Spinal Defects and Delayed Effects ofFailure of Midline Fusion, Including Tethered Cord Theproblems of meningomyelocele and its complications are so strictlypediatric and surgical that the neurologist seldom becomes involved—except perhaps in the initial evaluation of the patient—in the treatment of meningeal infection, or in the case of shuntfailure with decompensation of hydrocephalus. Of greater interestto the neurologist are a series of closely related abnormalities thatproduce symptoms for the first time in late childhood, adolescence,or even adult life. These include sinus tracts with recurrent meningealinfections, lumbosacral lipomas with low tethering of the spinalcord (“tethered cord”), and a delayed radicular or spinal cordsyndrome; diastematomyelia, cysts, or tumors with spina bifida anda progressive myeloradiculopathy; and a Chiari malformation andsyringomyelia that first present in adolescence or adult life. Theseabnormalities are described below.
Lain Spinal Defects Pembangunan dan Efek PenundaanKegagalan Fusion garis tengah, termasuk kabel tertambat Themasalah meningomyelocele dan komplikasi yang sangat ketatpediatrik dan bedah yang ahli saraf jarang terlibat-kecuali mungkin dalam evaluasi awal pasien-dalam pengobatan infeksi meningeal, atau dalam kasus shuntkegagalan dengan dekompensasi dari hydrocephalus. Dari kepentingan yang lebih besar

untuk ahli saraf adalah serangkaian kelainan erat terkait yangmenghasilkan gejala-gejala untuk pertama kalinya pada akhir masa kanak-kanak, remaja,atau kehidupan bahkan dewasa. Ini termasuk saluran sinus dengan meningeal berulanginfeksi, lipoma lumbosakral dengan penarikan rendah dari tulang belakangkabel ("kabel ditambatkan"), dan tali radikuler atau tulang belakang tertundasindrom; diastematomyelia, kista, atau tumor dengan spina bifida dansebuah myeloradiculopathy progresif, dan cacat Chiari dansyringomyelia yang hadir pertama dalam kehidupan remaja atau dewasa. Inikelainan dijelaskan di bawah ini.Another class of disorders involves an occult lumbosacral dysraphismthat is not inherited but is due to faulty development ofthe cell mass that lies caudal to the posterior neuropore (normallythis undergoes closure by the 28th day of embryonic life). Occultspinal dysraphism of this type is also associated with meningoceles,lipomas, and sacrococcygeal teratomas. Another well-recognizedanomaly is agenesis of the sacrum and sometimes the lower lumbarvertebrae (caudal regression syndrome). Interestingly, in 15 percentof such cases, the mother is diabetic (Lyon and Evrard). Herethere is flaccid paralysis of legs, often with arthrogrypotic contracturesand urinary incontinence. Sensory loss is less prominent,mental function develops normally, and there is no hydrocephalus.Sinus tracts in the lumbosacral or occipital regions are of importance,for they may be a source of bacterial meningitis at anyage. They are often betrayed by a small dimple in the skin or by atuft of hair along the posterior surface of the body in the midline.(The pilonidal sinus should not be included in this group.) Thesinus tract may lead to a terminal myelocystocele and be associatedwith dermoid cysts or fibrolipomas in the central part of the tract.Cloacal defects (no abdominal wall and no partition between bladderand rectum) may be combined with anterior meningoceles. Evidenceof sinus tracts should be sought in every instance of unexplainedmeningitis, especially when there has been recurrentinfection or the cultured organism is of nosocomial dermal origin.There are, in addition, other congenital cysts and tumors, particularlylipoma and dermoid, that arise in the filum terminale andattach (tether) the cord to the sacrum; progressive symptoms andsigns are produced as the spine elongates during development,stretching the caudally fixed cord (Fig. 38-3). Some of these childrenhave bladder and leg weakness soon after birth. Others deteriorateneurologically at a later age (generally between 2 and 16years, sometimes later—see below). According to Chapman andDavis, it is not the myelolipoma but the tethering of the cord thatgives rise to symptoms; removal of the tumor is of little benefitunless the cord is untethered (detached from the sacrum) at thesame time. This may be difficult, for the lipoma may be fused withthe dorsal surface of the spinal cord.

Diastematomyelia is another unusual abnormality of the spinalcord often associated with spina bifida. Here a bony spicule orfibrous band protrudes into the spinal canal from the body of oneof the thoracic or upper lumbar vertebrae and divides the spinalcord in two halves for a variable vertical extent. Or the division ofthe cord may be complete, each half with its own dural sac andcomplete set of nerve roots. This longitudinal fissuring and doublingof the cord are spoken of as diplomyelia. With body growth,it leads to a traction myelopathy, presenting with pain and progressivesensory, motor, and bladder symptoms, sometimes as lateas adult life. Removal of the fibrous-bony spicule and untetheringof the spinal cord have been beneficial in some cases.Several clinical syndromes of delayed progressive disease (inadolescents or adults), due mainly to a tethered cord, have beendelineated:1. Progressive cauda equina syndrome with lesions in the lumbosacralregion. In our experience this has been the mostcommon presentation of the tethered cord syndrome, with orwithout a lipoma or dermoid. Complex disturbances of bladderfunction that produce urgency and incontinence beginningin the second or third decade may be the only manifestation,or the bladder symptoms may be combined withimpotence (in the male) and numbness of the feet and legs orfoot drop (Pang and Wilberger). Several of our adult patientshave had unusual visceral reflex reactions, such as involuntarydefecation or priapism with stimulation of the abdomenor perineum.2. Progressive spastic weakness in some of the weak musclesof the legs in a patient known to have had a meningocele ormeningomyelocele. Presumably the spinal cord, which is securelyattached to the lumbar vertebrae, is stretched duringthe period of rapid lengthening of the vertebral column.3. An acute cauda equina syndrome, following some unusualactivity or accident (e.g., rowing or a fall in a sitting position),in patients who have had an asymptomatic or symptomaticspina bifida or meningocele. The implicated sensory andmotor roots are believed to be injured by sudden or repeatedstretching.4. Syringomyelia (page 1082). This is a developmental cavitywithin the cervical cord, extending a variable distance caudallyor rostrally, associated with an Arnold-Chiari malformation(see below). Also, there are a variety of neurologicproblems associated with spinal abnormalities in the highcervical region [fusion of atlas and occiput or of cervicalvertebrae (Klippel-Feil syndrome), congenital dislocation ofthe odontoid process and atlas, platybasia and basilar impression].

These abnormalities are reviewed in Chap. 44, withother diseases of the spinal cord.Chiari MalformationEncompassed by this term are a number of congenital anomaliesat the base of the brain, the most consistent of which are (1) extensionof a tongue of cerebellar tissue, posterior to the medullaand spinal cord, into the cervical canal and (2) displacement of themedulla into the cervical canal, along with the inferior part of thefourth ventricle. These and associated anomalies were first clearlydescribed by Chiari (1891, 1896). Arnold’s name is often attachedto the syndrome, but his contribution to our understanding of thesemalformations was relatively insignificant. Use of the double eponymArnold-Chiari malformation is so entrenched that a disputeover its propriety will not alter its usage. Chiari recognized fourtypes of abnormality. In recent years the term has come to be restrictedto Chiari’s types I and II—i.e., to the cerebellomedullarymalformation without and with a meningomyelocele, respectively.Type III Chiari malformation is no more than a high cervical oroccipitocervical meningomyelocele with cerebellar herniation, andtype IV consists only of cerebellar hypoplasia. It should be emphasizedthat a proportion of normal individuals have a smalltongue of the posterior cerebellum protruding below the openingof the foramen magnum by a few millimeters; this is usually of nosignificance and does not justify inclusion as a Chiari malformation.Several other morphologic features are characteristic of thetrue anomaly. The medulla and pons are elongated and the aqueductis narrowed. The displaced tissue (medulla and cerebellum) occludesthe foramen magnum; the remainder of the cerebellum,which is small, is also displaced so as to obliterate the cisternamagna. The foramina of Luschka and Magendie open into the cervicalcanal, and the arachnoidal tissue around the herniated brainstemand cerebellum is fibrotic. All these factors are probably operativein the production of hydrocephalus, which is alwaysassociated. Just below the herniated tail of cerebellar tissue thereis a kink or spur in the spinal cord, pushed posteriorly by the lowerend of the fourth ventricle. In this type of malformation, a meningomyeloceleis nearly always found. It should also be emphasized that hydromyelia or syringomyelia of the cervical cord arecommonly associated findings.Developmental abnormalities of the cerebrum (particularlypolymicrogyria) may coexist, and the lower end of the spinal cord(i.e., filum terminale) may extend as low as the sacrum. There areusually cranial bony abnormalities as well. The posterior fossa issmall; the foramen magnum is enlarged and grooved posteriorly.Nishikawa et al have suggested that smallness of the posteriorfossa, with overcrowding, is the primary abnormality leading to the

brain malformation. Often the base of the skull is flattened or infoldedby the cervical spine (basilar impression).Clinical Manifestations In type II Chiari malformation (withmeningomyelocele), the problem becomes one of progressive hydrocephalus.Cerebellar signs cannot be discerned in the first fewmonths of life. However, lower cranial nerve abnormalities—laryngeal stridor, fasciculations of the tongue, sternomastoid paralysis(causing head lag when the child is pulled from lying tositting), facial weakness, deafness, bilateral abducens palsies—may be present in varying combinations. If the patient survives tolater childhood or adolescence, one of the syndromes that occurswith the type I malformation may become manifest.In the more common type I Chiari malformation (withoutmeningocele or other signs of dysraphism), neurologic symptomsmay not develop until adolescence or adult life. The symptoms maybe those of (1) increased intracranial pressure, mainly headache,(2) progressive cerebellar ataxia, (3) progressive spastic quadriparesis,(4) downbeating nystagmus, or (5) cervical syringomyelia(segmental amyotrophy and sensory loss, with or without pain). Orthe patient may show a combination of disorders of the lower cranialnerves, cerebellum, medulla, and spinal cord (sensory and motortract disorders), usually in conjunction with headache that ismainly occipital. This combination of symptoms is often mistakenfor multiple sclerosis or a foramen magnum tumor. The symptomsmay have an acute onset after sustained extension of the neck, as,for example, after a long session of dental work, hairdressing inwomen, or chiropractic manipulation. The physical habitus of suchpatients may be normal, but about 25 percent have signs of anarrested hydrocephalus or a short “bull neck.” When basilar impression(a congenital abnormality of the occipital bone that invaginatesthe posterior atlas into the cranial cavity) and a Chiarimalformation coexist, it may be impossible to decide which of thetwo is responsible for the clinical findings.The tongue of cerebellar tissue and the kinked cervical cordobstruct the upward flow of dye and give a highly characteristicradiologic profile, particularly on sagittal MRI (Fig. 38-4). Inspectionof the axial sections of CT scans at the level of the foramenmagnum also demonstrates crowding of the upper cervical canalby inferiorly displaced cerebellar tissue, but one must be aware ofthe variations in the normal position of the cerebellar tonsils at thislevel. The low-pressure CSF syndrome may also lead to a slightdescent of the cerebellar tonsils that is reversible and in our experiencenot indicative of a Chiari malformation. The CSF is usuallynormal but may show an elevated pressure and protein levelin some cases.Treatment The treatment of Chiari malformation (and basilar

impression) is far from satisfactory. If clinical progression is slightor uncertain, it is probably best to do nothing. If progression iscertain and disability is increasing, upper cervical laminectomy andenlargement of the foramen magnum are indicated. Often this procedurehalts the progress of the neurologic illness, arrests the hydrocephalus,or results in some improvement. The outcome, in ourexperience, has been less satisfactory when decompression wasperformed mainly for intractable headache. The surgical proceduremust be done cautiously. Opening of the dura and extensive manipulationof the malformation or excision of herniated cerebellummay aggravate the symptoms or even cause death. The treatmentof an associated syringomyelia and other developmental abnormalitiesin this region is discussed further on page 1082. We areunable to comment on the use by a limited number of neurosurgeonsof posterior fossa decompression for the treatment of chronicfatigue syndrome except to say that it is illogical, even when aChiari malformation is detected.
Figure 38-4. Chiari-type malformation and developmental syringomyelia.T1-weighted MRI of the low-lying cerebellar tonsils below the foramenmagnum and behind the upper cervical cord (upper arrow) and the syrinxcavity in the upper cord (lower arrow).