Danny McAuley Queen’s University of Belfast Scottish Combined Critical Care Conference September...
38
Danny McAuley Queen’s University of Belfast Scottish Combined Critical Care Conference September 2010 Statins in ARDS
-
Upload
gabriel-walsh -
Category
Documents
-
view
213 -
download
0
Transcript of Danny McAuley Queen’s University of Belfast Scottish Combined Critical Care Conference September...

Danny McAuleyQueen’s University of Belfast
Scottish Combined Critical Care ConferenceSeptember 2010
Statins in ARDS

Novel therapies for ARDS - What is on the horizon?Conclusions
• Beta agonists– Potential benefit in phase II study– Phase III multi-centre clinical trials awaited
• Potential therapeutic interventions in phase II trials– APC– Statins
• Novel potential future treatments– Modulation of renin-angiotensin system– Stem cell therapy
Scottish Critical Care Trials Group June 2007

Statins in ARDS
• Mechanism of action• Observational data• Statins and pulmonary inflammation• Phase 2 clinical trial (HARP)• HARP-2

Cecilia O’Kane
Ashbaugh et al. described using “a clinical trial of a variety of drugs, respirators and fluid regimens” with limited success
No pharmacological treatment for ALI
Ashbaugh et al. Lancet 1967

Step-wise approach to new therapies
McAuley et al. CCM (in press)

Cellular effects of statins

Simvastatin reduces thrombin-induced endothelial injury
Jacobson et al. AJRCMB 2004;30:662

Simvastatin attenuates LPS-induced experimental lung injury
Jacobson et al. AJP Lung 2005;288:L1026

Statinn = 24
No statinn = 164
34%
21%
10%
20%
30%
40%
Mor
talit
y (%
)
OR 0.27 (0.06-1.21)p=0.09
Observational data to support a role for novel therapies in ALI
Irish Critical Care Trials Group. Critical Care 2008;12:R30

Steiner et al. Circulation 2005; 111:1841
Pre-treatment with simvastatin attenuates systemic inflammation following LPS challenge
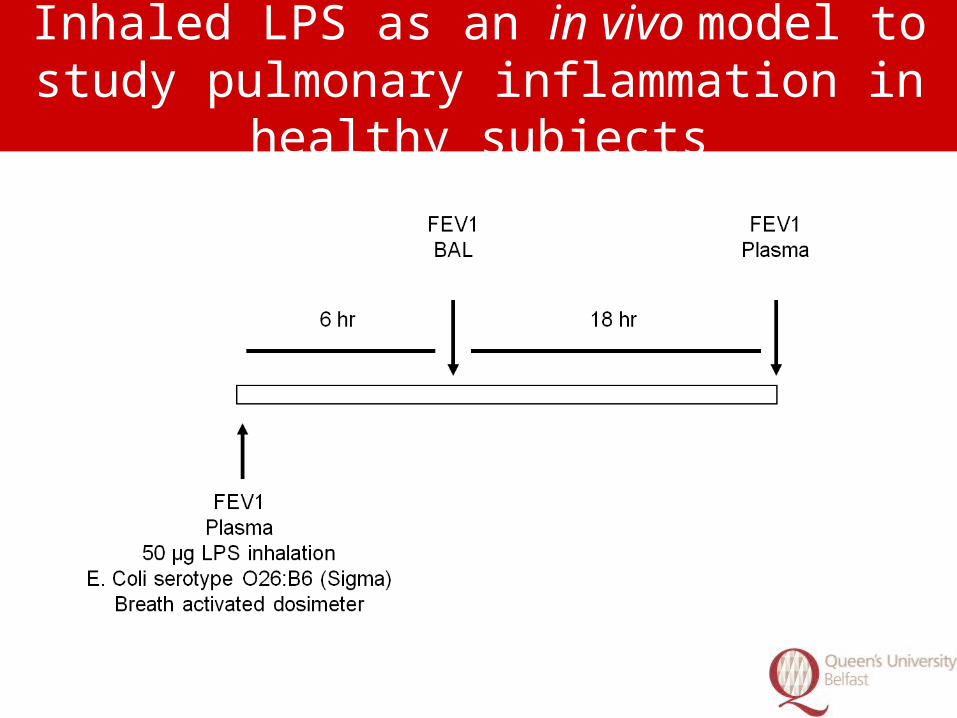
Inhaled LPS as an in vivo model to study pulmonary inflammation in healthy subjects

Cecilia O’Kane Inhaled LPS induces inflammatory
cytokines in pulmonary compartment

Simvastatin in the inhaled LPS model of ALI
Treatment with a clinically relevant dose of simvastatin will reduce pulmonary inflammation induced by LPS inhalation in humans
Shyamsundar et al. AJRCCM 2009 179:1107-1114

Schedule for patient safety monitoring

Simvastatin decreases pulmonary neutrophilia following LPS inhalation
Placebo(n=10)
Simvastatin(n=20)
P value
Total cells (x 105/ml)
15.2(10.3-49.8)
10.7(4.6-17.4)
0.2
Neutrophils8.5
(4.4-16.2)3.0
(1.8-8.1)0.05
Macrophages7.0
(3.1-19.1)5.1
(2.1-13.0)0.48
Lymphocytes1.1
(0.6-3.2)0.9
(0.2-1.6)0.37

Simvastatin increases neutrophil apoptosis following LPS inhalation
* p < 0.05 vs placebo

Simvastatin decreases pulmonary neutrophilic activity following LPS inhalation
* p < 0.05 vs placebo

Simvastatin decreases pulmonary TNF following LPS inhalation
* p < 0.05 vs placebo

Simvastatin pre-treatment reduces systemic inflammation following LPS inhalation
0
20
40
60
80
Plasma CRP(mg/L)
*
PlaceboSimvastatin
* p < 0.05 vs placebo

Simvastatin decreases pulmonary MMP secretion following LPS inhalation
* p < 0.05 vs placebo

Simvastatin pretreatment reduces nuclear NFκB translocation in monocyte-derived macrophages
p = 0.0001 for control vs. placebo BALF; ** p=0.03 for placebo BALF vs. simvastatin BALF; # p=0.03 for placebo BALF vs. simvastatin + placebo BALF

Lovastatin decreases pulmonary inflammation measured by FDG PET following LPS instillation
Chen et al. AJRCCM 2009 180:533-539

FDG PET can detect pulmonary inflammation in patients with ALI
Bellani et al. Critical Care Medicine 2009 37:2216-2222

HMGCoA reductase inhibition in ALI to Reduce Pulmonary oedema (HARP)
• Proof of concept single centre trial• Prospective double blind • Within 48 hours of onset of ALI• Randomised to simvastatin 80mg or placebo for up
to 14 days• Outcomes:
– Extra-vascular lung water– Pulmonary function and systemic organ failure– Safety– Biological markers in plasma and BAL
Craig et al. AJRCCM 2010 (in press)

Cecilia O’Kane
• Age < 18 years• Pregnancy • Drug interactions• Declined consent• Participation in a
clinical trial within 30 days
• Current treatment with statins
• Creatinine kinase (CK) > 10 times upper limit
• Transaminases > 3 times upper limit
Exclusion criteria

Patient demographics
Simvastatinn=30
Placebon=30
p value
Age (years) 52.5 (17.1) 52.8 (20.0) 0.95
Gender (% male) 73 73 1.00
APACHE II 25.1 (6.5) 23.3 (6.8) 0.30
APACHE IIpredicted mortality (%) 45.6 (25.0) 46.1 (24.7) 0.93
SAPS II 53.4 (14.4) 54.2 (14.3) 0.83
SAPS IIpredicted mortality (%) 51.2 (25.2) 53.6 (24.9) 0.72
Sepsis n (%) 15 (50) 15 (50) 1.00

Cecilia O’KaneSimvastatin improves oxygenation index
n =30 n=30 n=10 n=9

Cecilia O’KaneSimvastatin reduces plateau pressure
n=30 n=30 n=10 n=9

Cecilia O’Kane
Simvastatin improves sequential organ failure assessment (SOFA) score
n=30 n=30 n=10 n=9

Cecilia O’KaneSafety profile
Simvastatin Placebop value
CK > 10 times ULN (%) 4.5 8.7 0.58
ALT > 3 times ULN (%) 4.4 8 0.60
AST > 3 times ULN (%) 8.3 16.7 0.34
Adverse events (%) 47 43 0.79
Serious adverseevents (%) 20 23 0.75
• No serious adverse events due to study drug occurred

Cecilia O’Kane
Simvastatin Placebo p value
Ventilator free days 8.2 (8.1) 9.1 (8.7) 0.7
ICU free days 7.20(7.47) 8.4 (8.4) 0.6
ICU survival n (%) 21 (70%) 21 (70%) 1.0
Hospital LOS (days) 51.2 (39.3) 48.0 (37.4) 0.8
Hospital survival (days) 19 (63%) 19 (63%) 1.0
Outcome data

Cecilia O’Kane
Simvastatin decreasesbronchoalveolar lavage IL-8
0
2000
4000
6000
8000
10000PlaceboSimvastatin
p = NS *p = 0.05
IL-8(pg/ml)
D0 D3 D0 D3
p=0.89
n=17 n=10 n=23 n=17

0
1000
2000
3000
4000
5000PlaceboSimvastatin
p = NS p = 0.07
IL-6(pg/ml)
D0 D3 D0 D3
Simvastatin decreasesbronchoalveolar lavage IL-6
p=0.43
n=17 n=10 n=23 n=17

Cecilia O’Kane
Simvastatin decreases systemic inflammation as measured by plasma CRP
0
100
200
300
400PlaceboSimvastatin
p = NS *p = 0.0004CRP
(mg/L)
D0 D14 D0 D14
p=0.06
n=30 n=9 n=29 n=8

Conclusions
• In a human LPS model of ALI simvastatin reduces pulmonary and systemic inflammation
• In patients with ALI simvastatin– Improves pulmonary and non-pulmonary organ
dysfunction– Well tolerated– Reduces inflammation
• Study now needed to determine if simvastatin improves clinical outcome in large clinical trials

Cecilia O’KaneHARP-2

Acknowledgements

HMGCoA reductase inhibition in prevention of ALI (HARP-prevention)
(http://www.controlled-trials.com/ISRCTN56543987)
• Proof of concept, double blind, placebo controlled, single centre study
• Study population– Patients undergoing oesphagectomy– N=30 of planned sample size 36
• Simvastatin 80mg or placebo • Endpoints:
– Pulmonary dead space– Respiratory compliance, oxygenation index – Biological markers in plasma and EBC