
d'Annunzio 'School d'Annunzio · Physical Medicineand Rehabilitation of"G. D'Annunzio" University...
11
EUROPEAN JOURNAL OF INFLAMMATION CHRONIC ULCERS: TREATMENT WITH UNFOCUSED EXTRACORPOREAL SHOCK WAVES Vol. II, no. 2, 499-509 (2013) R. SAGGINI', P.FIORAMONTF, R.G. BELLOM03, A. DI STEFANO\ L. SCARCELLO\ L. DI PANCRAZI03, P. IODICE!, A. SAGGINP and N. SCUDERF 'Department ofNeuroscience and Imaging, "G. d'Annunzio" University, Chieti, Italy; 2Department of Plastic and Reconstructive Surgery, University of Rome "Sapienza", Rome, Italy; 3Department of Medicine and Science ofAging, "G. d'Annunzio" University, Chieti, Italy; 'School of Specialties in Physical Medicine and Rehabilitation, "G. d'Annunzio" University, Chieti, Italy; 'Department of Dermatology, University ofRome "Tor Vergata", Rome, Italy ReceivedJuly 31, 2012 - Accepted April 22, 2013 The aim of this study was to evaluate the efficacy of the treatment of chronic ulcers with unfocused shock waves. Between March 2009 and February 2012 we studied a group of 124 patients, aged between 28 and 80 years, with serious wounds arisen over three months and who met the inclusion criteria for treatment. The patients were randomly divided into groupsA and B, both treated with unfocused ESWT but with an average energy density for each impulse equal to 0.10 m.l/mm' in group A (total energy equal to 1.7 mJ for each shot) and an average energy density for each impulse equal to 0.04 m.I/mm- in group B (total energy equal to 3.3 mJ for each shot). The pulses were administered at a frequency of 4 Hz in both groups. Wounds were classified according to: location, width, length, percentage of granulation tissue, necrotic tissue, fibrous tissue, presence of bacterial exudation and pain (assessed by VAS). Their evolution was monitored by photo capture. The patients were treated with a frequency of 1 session every 7 days for 7 weeks. During the treatment period, the possible occurrence of side effects was monitored. Before treatment the wounds in group A had an average area equal to 3.85 em- and the average value of the VASpain scale was equal to 5.8 (range 2-9); the wounds in group B had an average area equal to 3.4 ern" and the average value ofthe VASpain scale was equal to 5.7 (range 3-9). At the end of the treatment protocol the mean area in group A decreased by 80% (final mean area 0.93 em"), and the average pain on VASscale dropped by 79%; the mean area in group B decreased by 67% (final mean area 1.2 ern") and the average score on VAS scale dropped by 48%. None of the treated patients experienced adverse reactions to treatment. None of the treated wounds developed infection during treatment. In conclusion, shock waves can act on difficult wounds, stimulating the reparative physiological process; therefore it represents an effective and safe procedure to accelerate the healing process, reducing the operating costs and avoiding more complex interventions. Chronic ulcers are complex wounds that do not heal spontaneously and are usually associated with local and systemic predisposing factors (1). Wound healing is a dynamic process influenced by homeostatic balance, inflammatory and matrix- synthesis process, and by an appropriate process Key words: chronic ulcers, unfocused shock waves, wound healing Mailing address: Prof. Raoul Saggini, Unit of Physical Medicine and Rehabilitation, "G. d'Annunzio" University, Viale Abruzzo 322, 66013 Chieti, Italia Tel.: +390871587107 e-mail: [email protected] 1721-727X (2013) Copyright © by BIOLIFE. s.a.s. This publication andlor article is for individual use only and may not be further reproduced without written permission from the copyright holder. Unauthorized reproduction may result in financial and other penalties 499 DISCLOSURE: ALL AUTHORS REPORT NO CONFLICTS OF INTEREST RELEVANT TO THIS ARTICLE.
Transcript of d'Annunzio 'School d'Annunzio · Physical Medicineand Rehabilitation of"G. D'Annunzio" University...

EUROPEAN JOURNAL OF INFLAMMATION
CHRONIC ULCERS: TREATMENT WITH UNFOCUSEDEXTRACORPOREAL SHOCKWAVES
Vol. II, no. 2, 499-509 (2013)
R. SAGGINI', P. FIORAMONTF, R.G. BELLOM03, A. DI STEFANO\ L. SCARCELLO\L. DI PANCRAZI03, P. IODICE!, A. SAGGINP and N. SCUDERF
'Department ofNeuroscience and Imaging, "G. d'Annunzio" University, Chieti, Italy; 2DepartmentofPlastic and Reconstructive Surgery, University ofRome "Sapienza", Rome, Italy; 3DepartmentofMedicine and Science ofAging, "G. d'Annunzio" University, Chieti, Italy; 'School ofSpecialtiesin Physical Medicine and Rehabilitation, "G. d'Annunzio" University, Chieti, Italy; 'Department of
Dermatology, University ofRome "Tor Vergata", Rome, Italy
Received July 31, 2012 - AcceptedApril 22, 2013
The aim of this study was to evaluate the efficacy of the treatment of chronic ulcers with unfocusedshock waves. Between March 2009 and February 2012 we studied a group of 124 patients, aged between28 and 80 years, with serious wounds arisen over three months and who met the inclusion criteria fortreatment. The patients were randomly divided into groups A and B, both treated with unfocused ESWTbut with an average energy density for each impulse equal to 0.10 m.l/mm' in group A (total energy equalto 1.7 mJ for each shot) and an average energy density for each impulse equal to 0.04 m.I/mm- in groupB (total energy equal to 3.3 mJ for each shot). The pulses were administered at a frequency of 4 Hz inboth groups. Wounds were classified according to: location, width, length, percentage of granulationtissue, necrotic tissue, fibrous tissue, presence of bacterial exudation and pain (assessed by VAS). Theirevolution was monitored by photo capture. The patients were treated with a frequency of 1 session every7 days for 7 weeks. During the treatment period, the possible occurrence of side effects was monitored.Before treatment the wounds in group A had an average area equal to 3.85 em- and the average value ofthe VASpain scale was equal to 5.8 (range 2-9); the wounds in group B had an average area equal to 3.4ern"and the average value ofthe VASpain scale was equal to 5.7 (range 3-9).At the end of the treatmentprotocol the mean area in group A decreased by 80% (final mean area 0.93 em"), and the average painon VAS scale dropped by 79%; the mean area in group B decreased by 67% (final mean area 1.2 ern")and the average score on VAS scale dropped by 48%. None of the treated patients experienced adversereactions to treatment. None of the treated wounds developed infection during treatment. In conclusion,shock waves can act on difficult wounds, stimulating the reparative physiological process; therefore itrepresents an effective and safe procedure to accelerate the healing process, reducing the operating costsand avoiding more complex interventions.
Chronic ulcers are complex wounds that do notheal spontaneously and are usually associated withlocal and systemic predisposing factors (1).
Wound healing is a dynamic process influencedby homeostatic balance, inflammatory and matrix-synthesis process, and by an appropriate process
Key words: chronic ulcers, unfocused shock waves, wound healing
Mailing address: Prof. Raoul Saggini,Unit ofPhysical Medicine and Rehabilitation,"G. d'Annunzio" University,Viale Abruzzo 322,66013 Chieti, ItaliaTel.: +390871587107e-mail: [email protected]
1721-727X (2013)Copyright © by BIOLIFE. s.a.s.
This publication andlor article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties499 DISCLOSURE: ALL AUTHORS REPORT NO CONFLICTS OF
INTEREST RELEVANT TO THIS ARTICLE.

500 R. SAGGINI ET AL.
of tissue remodelling. From a histological point ofview, the healing process is divided into three mainstages: inflammatory stage, proliferative stage, andmaturation or remodelling stage (2-4).Inflammation occurs in the tissue as the first
immediate response to injury. In the inflammatoryphase, vasodilation causes an increased permeabilityof blood vessels, vasocongestion and loss of serousfluids into the surrounding tissue. When the acuteresponses ofhomeostasis and inflammation are over,the wound healing begins (5).During the proliferative phase, the recovery
processes consist of: angiogenesis, fibroplasiaand epithelisation. This second stage is defined bythe production of granulation tissue composed ofcapillary bed, fibroblasts, macrophages and a loosearrangement of collagen, fibronectin, hyaluronicacid and bacteria. The proliferative stage resultsin the wound filling up with connective tissue andcovered with epithelium.In the maturation stage the wound contracts
through the internal moving ofthe surrounding tissueand skin and is reduced in size. The alteration ofone of these physiological steps leads to the chronicwound.A chronic wound is histologically determined
by lack of organization in endothelial proliferation,presence of parakeratotic keratinocytes, connectivetissue disorganization, increasing in keratinocytesand granulocytes, disorders of proteins, electrolytesand cytokines (1-6).The main causes affecting the physiological
healing process are: pressure, slipping and shearingforces, reduced mobility, sensory-motor functionimpairment, poor nutrition, advanced age, changesin hematopoiesis and external factors such aspsychosocial problems, prolonged immobilizationand infections (5). Many studies have shown thatthe predisposing bacteriological factor has a directcorrelation between high levels of bacteria inpressure ulcers and lack of tissue repair (7,8).Previous studies showed that shock waves are
effective in stimulating several endogenous growthfactors such as EGF, IGF1, VEGF and nitric oxideproduction, inducing angiogenesis and promotingthe healing of fractures, ulcers and complex lesions(1, 9-16). In their 2005 studies Gerdesmeyer et al.showed the antibacterial effect of shock waves
mediated by cavitation (17); in 2009 Kuo et al.also showed that when administered properlyextra corporeal shock wave therapy (ESWT) isable to: reduce the inflammatory response withsubsequent reduction in the number of circulatingleukocytes and of oxygen free radicals; promote theproduction of fibroblasts and the vascularization ofthe compromised skin, thus reducing the number ofapoptotic cells (18). That study assessed whetherESW treatment rescues the compromised flap tissueby suppressing the apoptosis of ischemic tissue andstimulating tissue regeneration. A random-patternextended dorsal-skin-flap (10 x 3 em) rodent modelwas used: skin grafts distal to the treated area wereapplied on 36 rats randomly divided into 3 groups(each consisting of 12 rats): the first group did notreceive treatment with ESWT, the second group wastreated with a single session of ESWT immediatelyafter surgery, and the third group was treated with2 sessions of ESWT, one immediately after surgery,the other the next day. The assay of the above-mentioned elements showed positive results in thegroups treated with shock waves compared to theuntreated one and a most significant advantage in thegroup treated with a single session of shock wavescompared to the one treated with two consecutivesessions.Human ulcer histological analysis also showed
a statistically significant increase of von Willebrandfactor (vWF), vascular endothelial growth factor(VEGF), endothelial nitric oxide synthase (e-NOS),antigen nuclear proliferation (PCNA) and theexpression of epidermal growth factor (EGF) withreduction of the expression of TUNEL, which is asignal of the cellular apoptotic cascade (19, 20).These results allow to develop patterns of
treatment in order to reduce the inflammatoryprocess and the excessive protease activity and, atthe same time, promote angiogenesis, and fibroblastproliferation as well as keratinocytes migration,inducing a correct biological process of woundhealing.
MATERIALS AND METHODS
Thestudywasapproved by the localethicscommittee,and was performed in accordance with the 1964Declaration of Helsinki. Subjects were informed about

European Journal of Inflammation 501
the procedures and purposes of the research and gave theirwritten informed consent before participating.
A randomized blind assessment controlled trial wasdesigned to study the efficacy of shock wave treatmentproduced by the unfocused probe through the analysisof the percentage of wound healing (calculated as thereduction in wound area divided for the initial areapercentage).
The study was carried out by the Department ofPhysical Medicine and Rehabilitation of"G. D' Annunzio"University in Chieti, and the Department of Plastic andReconstructive Surgery of "Sapienza" University inRome.
The secondary outcome of the study was to assessthe antibacterial effect through the evaluation of specificbuffers and the search for possible occurrence of infectionduring therapy. Inclusion criteria were as follows: vascular(blood-based and/or venous), diabetic, pressure, bum,iatrogenic, post-traumatic ulcer or ulcer in autoimmunedisease. No wound healing progression or loss ofsubstancefor at least 3 months; age over 18 years; informed consentsignature.
Exclusion criteria were: arrhythmias; pacemaker;severe bleeding disorders; cancer close to the treatmentarea; pregnancy; presence of growing cartilage; localacute inflammation; bone exposure; wound area less than
I em- or greater than IOx20 em,One hundred and twenty-four patients (67 men, 57
women), aged between 28 and 80 years, meeting theinclusion criteria were treated between March 2009and February 2012. The selected patients had chroniculcers for at least 3 to 24 months before the beginning oftherapy (mean 10 months). They were randomly dividedinto 2 treatment groups A and B; all patients receivedunfocused ESWT treatment; patients in group A weretreated with Dermagold unfocused probe (MTS EuropeGmbH, Constance, Germany), patients in group B weretreated with Evotron unfocused probe (HMT, Lengwil,Switzerland). All patients were treated with a frequencyof I session every 7 days for 7 weeks. A medical recordwith personal data, main disease (responsible for ulcer),secondary diseases, time of onset, previous treatmentsand their costs, and previous medications was completedfor each patient.
Before and after the treatment period the ulcers wereclassified according to: localization, width (in em), length(in ern), percentage of granulation tissue, necrotic tissue,fibrous tissue, presence of bacterial exudate (classifiedas absent, minimal, moderate, high) and pain, whichwere assessed by Visual Analogic Scale (VAS). Themorphological evolution was monitored, taking photosbefore each session using digital cameras with resolution
144 subjects aged between 28 and 80 with chroniculcers
20 subjects excluded because they had ulcers forless than 3 months
124 patients with all the inclusion criteria
124 randomized subjects
62 subjectsDermagoldgroup
N" 2 withdrawn (lack of protocolcompliance)
60 subjectswith full data
Fig. 1. Flow chart ofpatients enrolled in the study.
62 subjectsEvotrongroup
40 subjects withfull data
N" 22 withdrawn (lack ofprotocol compliance)

Table I. Relation between wound area and number ofshots administeredfor each session.
higher than 5 megapixels and macros function; all pictureswere taken at the shortest distance necessary to frame thelesion and the standardized squared.
After each session dressing with povidone-iodine andapplication of fat gauze, Connettivina (Fidia FarmaceuticiS.p.A, Italy) and semipermeable occlusive patches wascarried out. During the treatment period, the possibleoccurrence of side effects such as pain, petechiae andcutaneous adverse reactions related to therapy wasmonitored (21-22) (Fig. I).
Sixty-two subjects (39 men and 23 women) agedbetween 28 and 80 years (mean age 62 years), wereincluded in GroupA, two ofwhom dropped out ofthe studybecause of personal problems. Of the remaining patients,23 had diabetic ulcers, 10 pressure ulcers, 10 traumaticulcers, 19 vascular ulcers. All subjects were alwaystreated with ESWT unfocused probe with Dermagoldelectrohydraulic system (MTS Europe GmbH, Constance,Germany); the mean energy density applied for each pulsein Group A was equal to 0.1 m.l/rnrrr' (0.09/0.11 ml/mm-),with a total energy equal to 1.7 mJ for each shot.
Sixty-two subjects (28 men and 34 women) agedbetween 30 and 80 years, were included in Group B, 22ofwhom dropped out of the study after the first treatmentsession and were not included in the final evaluation.Of the remaining 40 patients (16 men and 24 women),aged between 33 and 77 years (mean age 61 years), 9had diabetic wounds, II post-trauma wounds, I patientpressure ulcer, 16 vascular wounds and 3 wounds incryoglobulinemia. All subjects were always treated withESWT unfocused probe with Evotron electrohydraulicsystem (HMT, Lengwil, Switzerland); the mean energy
502
Wound area (em") Number of shots
300
400
500
600
R. SAGGINI ET AL.
density applied in Group B was equal to 0.04 ml/rnm',with a total energy equal to 3.3 mJ for each shot.
In both Groups A and B, 300 to 600 shots wereadministered per session relating to the wound area, asshown in Table I, at a frequency of 4 Hz or 240 pulsesper minute.
All data are given as means ± SDs. Differencesbetween mean values before and after the treatmentperiod were tested for significance using Student's t-testfor paired observations. ANOYA with an interaction testwas used to compare the responses to the treatment in thetwo groups. Fischer's PLSD test for post hoc analysis wasemployed. The minimum level of statistical significancewas set at P<0.05. GraphPad Prism (version 5) software(Abacus Concepts GraphPad Software, San Diego, CA,USA) for statistical analysis was used.
RESULTS
Before treatment the average area of the 62wounds in Group A was equal to 3.85 em- As forthe location of ulcers, 21 patients had lesions on thelower limbs, 31 on the foot-ankle complex, lOin thepelvic region.At first, lesions were made of 56% granulation
tissue, 37% fibrous tissue, and 7% necrotic tissue; 29subjects showed complete autonomy in the ordinarydaily activities, 23 showed reduced autonomy, 10showed autonomy with wheelchair; pain assessmentin the early phase showed a mean VAS of 5.8, range2-9.Before treatment, the mean wound area In Group
B was equal to 3.4 cm-; as for the location of ulcers,28 were on the foot-ankle complex, 14 on lowerlimbs, in particular 2 patients had lesions on bothlower limbs.At first lesions were represented by an average
of 55% of granulation tissue; 35% of fibrous tissueand 10% of necrotic tissue; among the 40 selectedpatients, 25 had complete autonomy, 14 reducedautonomy, I patient had autonomy with a wheelchair;pain assessment in the initial phase in this Groupshowed a mean VAS of5.7, range 3-9. No patient inany group underwent antibiotic therapy during thewhole treatment period.Improvement in vascularization is quantitatively
difficult to assess, therefore the surrounding skin,being a valid indicator of tissue distress, wasmonitored to determine the successful closure orreduction in size of the lesions in both groups during
GROUP AWOUND AREA
European Journal of Inflammation
GROUP A
503
Meanwound area
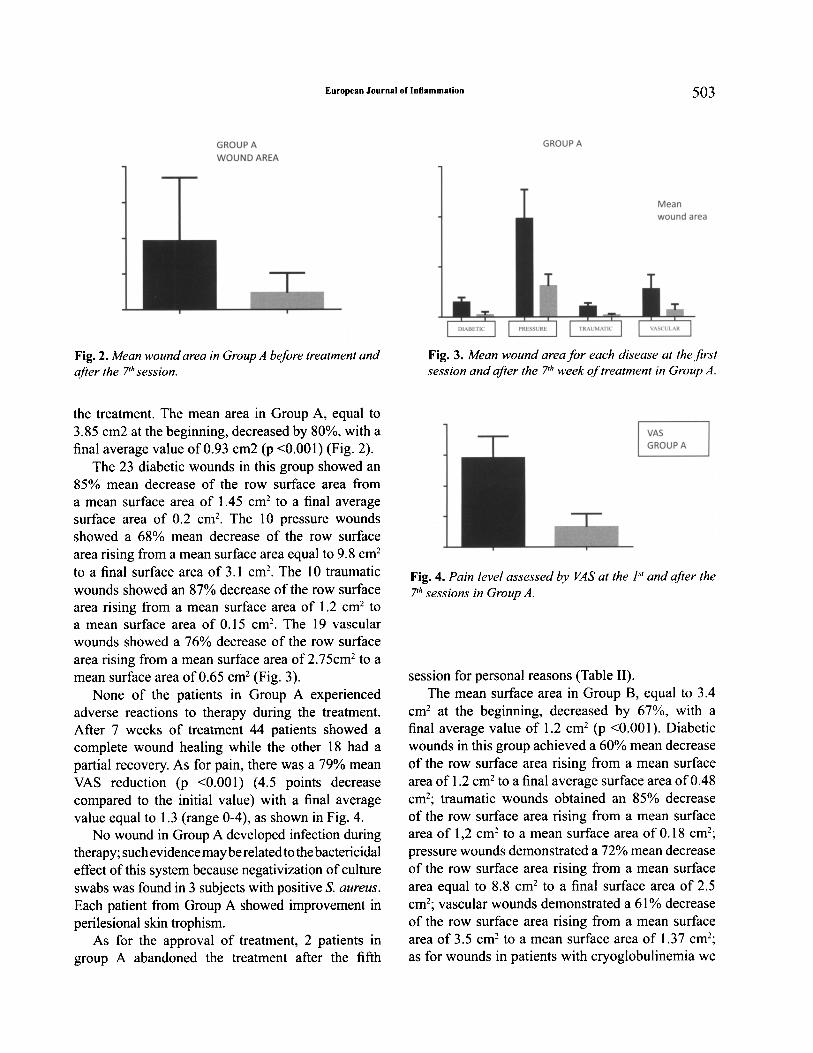
Fig. 2. Mean wound area in Group A bef ore treatment andafter the 7th session.
the treatment. The mean area in Group A, equal to3.85 cm2 at the beginning, decreased by 80%, with afinal average value of 0.93 cm2 (p <0.001) (Fig. 2).The 23 diabetic wounds in this group showed an
85% mean decrease of the row surface area froma mean surface area of 1.45 em' to a final averagesurface area of 0.2 em' . The 10 pressure woundsshowed a 68% mean decrease of the row surfacearea rising from a mean surface area equal to 9.8 ern'to a final surface area of 3.1 em' . The 10 traumaticwounds showed an 87% decrease of the row surfacearea rising from a mean surface area of 1.2 em' toa mean surface area of 0.15 cm/. The 19 vascularwounds showed a 76% decrease of the row surfacearea rising from a mean surface area of 2.75cm2 to amean surface area of 0.65 em' (Fig. 3).None of the patients in Group A experienced
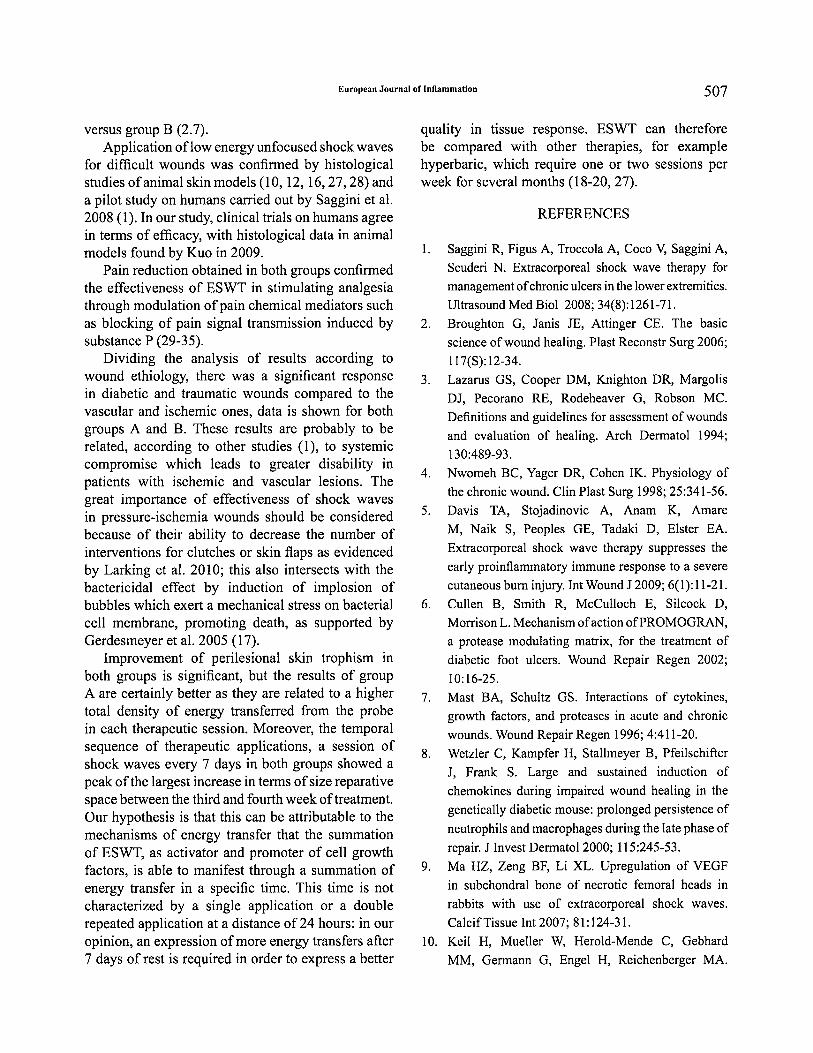
adverse reactions to therapy during the treatment.After 7 weeks of treatment 44 patients showed acomplete wound healing while the other 18 had apartial recovery. As for pain, there was a 79% meanVAS reduction (p <0.001) (4.5 points decreasecompared to the initial value) with a final averagevalue equal to 1.3 (range 0-4), as shown in Fig. 4.No wound in Group A developed infection during
therapy;such evidencemayberelated tothebactericidaleffect of this system because negativization of cultureswabs was found in 3 subjects with positive S. aureus.Each patient from Group A showed improvement inperilesional skin trophism.As for the approval of treatment, 2 patients in
group A abandoned the treatment after the fifth
Fig. 3. Mean wound area for each disease at the fi rstsession and after the Z'" week oftreatment in Group A.
VASGROUP A
Fig. 4. Pain level assessed by VAS at the / " and after the7th sessions in Group A.
session for personal reasons (Table 11).The mean surface area in Group B, equal to 3.4
em? at the beginning, decreased by 67%, with afinal average value of 1.2 ern- (p <0.00 I). Diabeticwounds in this group achieved a 60% mean decreaseof the row surface area rising from a mean surfacearea of 1.2 em' to a final average surface area of0.48cm-; traumatic wounds obtained an 85% decreaseof the row surface area rising from a mean surfacearea of 1,2 em? to a mean surface area of 0.18 ern";pressure wounds demonstrated a 72% mean decreaseof the row surface area rising from a mean surfacearea equal to 8.8 em- to a final surface area of 2.5em'; vascular wounds demonstrated a 61% decreaseof the row surface area rising from a mean surfacearea of 3.5 ern? to a mean surface area of 1.37 cm-;as for wounds in patients with cryoglobulinemia we

504 R. SAGG I:'III ET AL.
Table II. Compliance to therapy in group A where 2 patients abandoned the protocol.
WOUND AREA WOUNDAREA VAS VAS REASOl'i FOR
GROUPA AGE 1STsession 5THsession 1sTsession 5THsession WITHDRAWAL
I 73 11.5 1.7 5 4 CHANGE OF RESID ENCE
., 78 7 4.5 4 3 CHANGE OF RESID ENCE
GROUP BWOUND AREA
VASGROUP B
Fig. S.Mean wound area in Group B before treatment andafter the 7th session.
GROUP B
Meanwound area
Fig. 6. Mean wound area f or each disease at the fir stsession and after the 7th week of treatment in Group B.
found a 33% decrease of the row surface area (Figs .5 and 6).None of patients in Group B experienced adverse
reactions to treatment (bleeding, petechiae) apartfrom IS patients who withdrew from the studybecause of pain .At the end of therapy, 16 patients achieved
Fig. 7. Pain level assessed by VAS at the I" and after the7th session in Group B.
complete healing, 15 obta ined partial recovery, 9wounds (5 from vascular insufficiency, 2 in diabeti cmicroangiopathy, 2 in cryoglobulinemia) showedno improvement. As for pain, in Group B, there wasa 48% mean VAS reduction (2.7 reduction pointscompared to the initial value) with a final meanvalue equal to 3 (range 1-6) (Fig. 7).As for the approval of treatment, 22 patients
withdrew from the study after the first session forpersonal reasons as described in Table III.No wound in Group B developed infect ion
during therapy ; such evidence may be related to thebactericidal effect ofthis system because dejection ofStaphylococcus aureus in culture swabs was found.Each patient from Group B showed improvement inperilesional skin trophism.Both groups A and B showed a good response
to treatment with a sign ificant reduction in woundareas after 7 weeks and a peak of increase in termsof wound size reduction, between the third and thefourth week of treatment. During the last evaluationGroup A showed a greater area reduction than GroupB (Fig. 8 and 9).

European Journal of Inflammation
Table III. Compliance to therapy in group B where 22 patients abandoned the protocol.
505
WOUND WOUND AREA VAS VAS REASON FORGROUPB AGE AREA 2nd session I" session 2nd session WITHDRAWALI" sessionDIFFICULTY INI 68 2 1.7 7 7 MOVING and PAINCHANGE OF2 77 1.5 1.5 4 5 RESIDENCE and PAINCHANGE OF3 28 3 2.7 7 4 RESIDENCE and PAINDIFFICULTY IN4 80 3.4 3 5 4 MOVINGCHANGE OF5 77 13 12.5 7 6 RESIDENCE and PAINDIFFICULTY IN6 45 2 1.5 8 7 MOVINGDIFFICULTY IN7 71 1.7 1.6 7 7 MOVING and PAINCHANGE OF8 71 2 1.7 4 4 RESIDENCE and PAINDIFFICULTY IN9 45 10.3 9.5 8 7 MOVINGCHANGE OF10 45 5 4.7 9 9 RESIDENCE and PAINCHANGE OFII 52 4 3.4 4 3 RESIDENCE and PAINCHANGE OF12 54 2.5 2.2 4 4 RESIDENCE and PAINCHANGE OF13 28 2 2 5 4 RESIDENCE and PAINDIFFICULTY IN14 80 2.7 2.5 5 7 MOVING and PAINDIFFICULTY IN15 72 3 3 6 7 MOVINGCHANGE OF16 70 3.5 3.2 8 7 RESIDENCE and PAINDIFFICULTY IN17 55 4.4 4.3 5 7 MOVINGDIFFICULTY IN18 45 3 2.7 5 5 MOVING and PAINDIFFICULTY IN19 47 2 1.7 7 6 MOVING and PAINCHANGE OF20 73 3.5 3.2 6 4 RESIDENCECHANGE OF21 38 3 2.5 4 I RESIDENCE and PAINDIFFICULTY IN22 73 2 1.4 7 5 MOVING

506 R. SAGGINI ET AL.
Two-way ANOVAwith RM by columns5
4
3
2
1
...... GROUPA
... GROUP B
O......."T"""-"T"""--r---r--r--r--r-
Fig. 8. Comparison ofthe responses to treatment between group A and group B.
Fig. 9. Evolution in tissue regeneration in a patient (male, 77 y, 90kg, 1.70h) with pressure wound in gluteal region.Before (a), after (b) treatment and at 5-monthfollow-up (c).
DISCUSSION
Chronic wound treatment is becoming animportant economic and social issue related to theincrease in the average population age because ofthe necessary costs for management, not only infinancial terms but also in human resources (1, 23),patients quality of life and psychological impact onthem (24).Therefore, it would be interesting to find
therapeutic solutions able to aid the healing processby reducing, at the same time, the amount ofdressings applied, the need for assistance in woundcare and the need for surgery.
Nowadays, chronic wound treatment is based onmechanical debridement, use of flaps or skin grafts,advanced dressings and, in an experimental way,application of a particular type of acoustic wave,defined shock wave. ESWT basically representsa cellular activator because of its ability to induceangiogenesis, to stimulate the increase in growthfactors and promote cell differentiation (25-26).The results showed that in both groups there was
a significant decrease in the percentage (p <0.001)of the row surface area with a greater value in GroupA compared to Group B, respectively equal to80% and 67%. Moreover, pain reduction, assessedby VAS, was statistically significant (p <0.001) inboth groups, but with a larger value in group A (4.5)
European Journal of Inflammation 507
versus group B (2.7).Application oflow energy unfocused shock waves
for difficult wounds was confirmed by histologicalstudies ofanimal skin models (10, 12, 16,27,28) anda pilot study on humans carried out by Saggini et al.2008 (1). In our study, clinical trials on humans agreein terms of efficacy, with histological data in animalmodels found by Kuo in 2009.Pain reduction obtained in both groups confirmed
the effectiveness of ESWT in stimulating analgesiathrough modulation ofpain chemical mediators suchas blocking of pain signal transmission induced bysubstance P (29-35).Dividing the analysis of results according to
wound ethiology, there was a significant responsein diabetic and traumatic wounds compared to thevascular and ischemic ones, data is shown for bothgroups A and B. These results are probably to berelated, according to other studies (1), to systemiccompromise which leads to greater disability inpatients with ischemic and vascular lesions. Thegreat importance of effectiveness of shock wavesin pressure-ischemia wounds should be consideredbecause of their ability to decrease the number ofinterventions for clutches or skin flaps as evidencedby Larking et al. 2010; this also intersects with thebactericidal effect by induction of implosion ofbubbles which exert a mechanical stress on bacterialcell membrane, promoting death, as supported byGerdesmeyer et al. 2005 (17).Improvement of perilesional skin trophism in
both groups is significant, but the results of groupA are certainly better as they are related to a highertotal density of energy transferred from the probein each therapeutic session. Moreover, the temporalsequence of therapeutic applications, a session ofshock waves every 7 days in both groups showed apeak ofthe largest increase in terms ofsize reparativespace between the third and fourth week oftreatment.Our hypothesis is that this can be attributable to themechanisms of energy transfer that the summationof ESWT, as activator and promoter of cell growthfactors, is able to manifest through a summation ofenergy transfer in a specific time. This time is notcharacterized by a single application or a doublerepeated application at a distance of 24 hours: in ouropinion, an expression ofmore energy transfers after7 days of rest is required in order to express a better
quality in tissue response. ESWT can thereforebe compared with other therapies, for examplehyperbaric, which require one or two sessions perweek for several months (18-20, 27).
REFERENCES
I. Saggini R, Figus A, Troccola A, Coco V, Saggini A,Scuderi N. Extracorporeal shock wave therapy formanagement ofchronic ulcers in the lower extremities.Ultrasound Med Bioi 2008; 34(8):1261-71.
2. Broughton G, Janis JE, Attinger CEo The basicscience ofwound healing. Plast Reconstr Surg 2006;117(S):12-34.
3. Lazarus GS, Cooper DM, Knighton DR, MargolisDJ, Pecorano RE, Rodeheaver G, Robson Me.Definitions and guidelines for assessment ofwoundsand evaluation of healing. Arch Dermatol 1994;130:489-93.
4. Nwomeh BC, Yager DR, Cohen IK. Physiology ofthe chronic wound. Clin Plast Surg 1998; 25:341-56.
5. Davis TA, Stojadinovic A, Anam K, AmareM, Naik S, Peoples GE, Tadaki D, Elster EA.Extracorporeal shock wave therapy suppresses theearly proinflammatory immune response to a severecutaneous burn injury. Int Wound J 2009; 6(1):11-21.
6. Cullen B, Smith R, McCulloch E, Silcock D,Morrison L. Mechanism ofaction ofPROMOGRAN,a protease modulating matrix, for the treatment ofdiabetic foot ulcers. Wound Repair Regen 2002;10:16-25.
7. Mast BA, Schultz GS. Interactions of cytokines,growth factors, and proteases in acute and chronicwounds. Wound Repair Regen 1996; 4:411-20.
8. Wetzler C, Kampfer H, Stallmeyer B, PfeilschifterJ, Frank S. Large and sustained induction ofchemokines during impaired wound healing in thegenetically diabetic mouse: prolonged persistence ofneutrophils and macrophages during the late phase ofrepair. J Invest Dermatol2000; 115:245-53.
9. Ma HZ, Zeng BF, Li XL. Upregulation of VEGFin subchondral bone of necrotic femoral heads inrabbits with use of extracorporeal shock waves.CalcifTissue Int 2007; 81:124-31.
10. Keil H, Mueller W, Herold-Mende C, GebhardMM, Germann G, Engel H, Reichenberger MA.

508 R. SAGGINI ET AL.
Preoperative shock wave treatment enhancesischemic tissue survival, blood flow and angiogenesisin a rat skin flap model. Int J Surg 20 II; 9(4):292-6
II. Zins SR, Amare MF, Tadaki DK, Elster EA, DavisTA. Comparative analysis of angiogenic geneexpression in normal and impaired wound healing indiabetic mice: effects of extracorporeal shock wavetherapy. Angiogenesis 2010; 13(4):293-304.
12. Stojadinovic A, Elster EA, Anam K, Tadaki D,Amare M, Zins S, Davis TA. Angiogenic response toextracorporeal shock wave treatment in murine skinisografts. Angiogenesis 2008; 11(4):369-80.
13. Silveira A, Koenig 18, Arroyo LG, Trout D, MoensNM, LaMarre J, Brooks A. Effects of unfocusedextracorporeal shock wave therapy on healing ofwounds ofthe distal portion ofthe forelimb in horses.Am J Vet Res 2010; 71(2):229-34.
14. Morgan DD, McClure S, Yaeger MJ, SchumacherJ, Evans RB. Effects of extracorporeal shock wavetherapy on wounds of the distal portion of the limbs inhorses. J Am VetMed Assoc 2009; 234(9): 1154-61.
15. Tinazzi E, Amelio E, Marangoni E, et al. Effectsof shock wave therapy in the skin of patientswith progressive systemic sclerosis: a pilot study.Rheumatol Int 20 II; 31(5):651-6
16. YanX, Zeng B, Chai Y,Luo C, Li X. Improvement ofblood flow, expression of nitric oxide, and vascularendothelial growth factor by low-energy shockwavetherapy in random-pattern skin flap model. Ann PlastSurg 2008; 61(6):646-53.
17. Gerdesmeyer L, von Eiff C, Hom C, Henne M,Roessner M, Diehl P, Gollwitzer H. Antibacterialeffects of extracorporeal shock WAVES. Ultrasoundin Med Bioi 2005; 31:115-19.
18. Kuo YR, Wang CT, Wang FS, Yang KD, ChiangYC, Wang CJ. Extracorporeal shock wave treatmentmodulates skin fibroblast recruitment and leukocyteinfiltration for enhancing extended skin-flap survival.Wound Repair Regen 2009; 17(1):80-7.
19. Wang CJ, Ko JY, Kuo YR, Yang YJ.Molecular changes in diabetic foot ulcers. DiabetesRes Clin Pract 20 II; 94( I): I05-1O.
20. Wang CJ, Wu RW, Yang Y1. Treatment of diabeticfoot ulcers: a comparative study of extracorporealshockwave therapy and hyperbaric oxygen therapy.Diabetes Res Clin Pract 20 II; 92(2): 187-93.
21. Haake M, Thon A, Bette M. Unchanged c-Fosexpression after extracorporeal shock wave therapy:an experimental investigation in rats. Arch OrthopTrauma Surg 2002; 122(9-10):518-21.
22. Sistermann R, Katthagen BD. Complications, side-effects and contraindications in the use of mediumand high-energy extracorporeal shock wavesin orthopedics. Z Orthop Ihre Grenzgeb 1998;136(2):175-81.
23. Larking AM, Duport S, Clinton M, Hardy M,Andrews K. Randomized control of extracorporealshock wave therapy versus placebo for chronicdecubitus ulceration. Clinical Rehabilitation 20 I0;24:222-29.
24. Pragnell J, Nelison 1. The social and psychologicalimpact of hard-to-heal wounds. Br J Nurs 20 I0;19(19):1248-52.
25. Ueberle F, Delius M, Guo L. Using shock waves fortransfer of molecules in cells. Biomed Tech(Berl)2002; 47(S):382-5.
26. Buch SW. Extracorporeal shock waves III
orthopaedics. Springer 1998; 59-87.27. Chen YJ, Wang CJ, Yang KD, Kuo YR, Huang HC,
Huang YT, Sun YC, Wang FS. Extracorporeal shockwaves promote healing of collagenase-inducedAchilles tendinitis and increase TGF-betal andIGF-I expression. J Orthop Res 2004; 22(4):854-61.
28. Ikeda K, Tomita K, Takayama K. Application ofextracorporeal shock wave on bone: preliminaryreport. J Trauma 1999; 47(5):946-50.
29. Kuo YR, Wu WS, Hsieh YL, Wang FS, Wang CT,Chiang YC, Wang C1. Extracorporeal shock waveenhanced extended skin flap tissue survival viaincrease of topical blood perfusion and associatedwith suppression of tissue pro-inflammation. J SurgRes 2007; 143(2):385-92.
30. Kuo YR, Wang CT,Wang FS, Chiang YC, Wang C1.Extracorporeal shock-wave therapy enhanced woundhealing via increasing topical blood perfusion andtissue regeneration in a rat model of STZ-induceddiabetes. Wound Wound Repair Regen 2009;17(4):522-30.
31. Rompe 10, Kirkpatrick CJ, Kullmer K, Schwitalle M,Krischek O. Dose-related effects of shock waves onrabbit tendo Achillis. A sonographic and histologicalstudy. J Bone Joint Surg Br 1998; 80:546-52.

European Journal of Inflammation 509
32. Rompe JD, Hope C, Kullmer K, Heine J, BurgerR. Analgesic effect of extracorporeal shock-wavetherapy on chronic tennis elbow. J Bone Joint SurgBr 1996; 78:233-37.
33. Rompe JD, Hope C, Kullmer K, Heine J, BurgerR, Nafe B. Low energy extracorporeal shock wavetherapy for persistent tennis elbow. Int Orthop 1996;20:23-27.
34. Schelling G, Delius M, Gschwender M, Grafe P,Gambihler S. Extracorporeal shock waves stimulatefrog sciatic nerves indirectly via a cavitation-mediated mechanism. Biophys J 1994; 66:133-40.
35. Maier M, Averbeck B, Milz S, Refior HJ, Schmitz C.Substance P and prostaglandin E2 release after shockwave application to the rabbit femur. Clin OrthopRelat Res 2003; 406:237-45.


















