Integrating Mahara as e-portfolio system and social network in the BScE
description

Effect of Donor Processing and Storage Time and Preoperative Endothelial Cell Counts on DSAEK Detachment Rates Daniel Demsey BScEStephanie Baxter MD, FRCSC
Queen’s University School of Medicine, Department of Ophthalmology. Kingston, ON, Canada
The authors have no financial interest in the subject matter of this poster.

Rationale
•To determine whether the rate of graft detachment in patients undergoing the DSAEK procedure is influenced by the time elapsed between donor death, tissue procurement, processing, storage, and implantation, as well as endothelial cell count, in one surgeon’s practice.

Introduction• The DSAEK procedure is primarily used to treat
corneal endothelial dystrophies1, and more recently to treat endothelial failure in previous penetrating keratoplasty, irido-corneal-endothelial (ICE) syndrome, aphakia, aniridia, and complex anterior segments with anterior chamber lenses2.
• Descemet’s membrane and endothelium are removed through a small incision and replaced with donor tissue, which adheres to the recipient’s inner corneal stroma1.
• The major post-operative complication of the DSAEK procedure is dislocation of the donor tissue from the corneal transplant bed, which has been reported to happen in 4-27% of patients1,5,8,10,11. Donor detachments are most likely attributed to surgeon error or a lack of donor tissue viability.

Introduction• In Ontario, Canada donor tissue is procured from
cadavers and sent to the Eye Bank of Canada, Ontario Division in Toronto before being shipped to the transplanting surgeons for implantation in a patient.
• A period of time, typically hours, passes between the death of the donor and enucleation of the eye, and between enucleation and processing by the Eye Bank.
• The tissue then spends a period of days in storage at the Eye Bank before implantation in the recipient eye.
• Currently all DSAEK donor tissue is currently prepared by individual surgeon’s at the site and time of transplantation.

Hypothesis• It is our hypothesis that a greater period of
time spent in storage or prior to processing results in a potentially greater loss of tissue viability and concordantly leads to a higher rate of detachment post operatively.
• Additionally, it is hypothesized that the endothelial cell count of the donor tissue plays a role in detachment rate, with a higher count possibly indicating better tissue function and thus a lower detachment rate.
• The primary aim of our investigation is to determine whether these factors play a predictive role in tissue detachment in one surgeon’s practice.

Methods• Data on procedure outcome and donor tissue
for all patients in one surgeon’s practice undergoing the DSAEK procedure between April 1, 2007 and April 30, 2010 was reviewed through a retrospective chart review.
• Data on time elapsed between harvest, processing, storage, and implantation of the tissue was obtained from reports made available from the Eye Bank of Canada, Ontario Division.
• The adverse outcome of interest was graft detachment requiring re-bubbling.

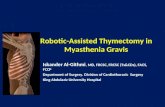
ResultsNo Detachment SD Detachment SD P
N 61 10Time to Procurement (hours) 6.2 3.5 7.4 4.0 0.36
Time to Processing (hours) 13.1 5.9 13.5 6.3 0.87
Time in Bank (days) 3.9 2.2 4.6 2.2 0.36
Cell Count 2647.4 244.5 2776.5 299.5 0.14

Results• 71 cases were reviewed, with 14% resulting
in dislocation. • Averages were determined of the time
between donor death and tissue procurement, procurement and processing, storage at the Eye Bank, and implantation in the recipient, as well as endothelial cell count , and compared between the grafts that failed and those that did not using a paired student’s t-test. There was no statistically significant difference in any of these parameters between the two groups.

Discussion
•As demonstrated in the results section, there was no statistically significant difference in the storage and processing times between the detachment and non-detachment groups.
•This suggests that slight variations in donor tissue processing and storage times do not result in a higher incidence of DSAEK graft dislocation.

Conclusions
•The range of processing times and endothelial cell counts in donor tissue available from the Eye Bank did not predict a change in the rate of graft dislocation in one surgeon’s practice.

References• (1) M.S. Gorovoy, Descemet-stripping automated endothelial keratoplasty, Cornea 25 (2006), pp. 886–889.• (2) Ghaznawi N. Chen ES. Descemet's stripping automated endothelial keratoplasty: innovations in
surgical technique. [Review] Current Opinion in Ophthalmology. 21(4):283-7, 2010 Jul• (3)G.R. Melles, R.H. Wijdh and C.P. Nieuwendaal, A technique to excise the Descemet membrane from a
recipient cornea (descemetorhexis), Cornea 23 (2004), pp. 286–288. • (4)F.W. Price Jr and M.O. Price, Descemet's stripping with endothelial keratoplasty in 50 eyes: a refractive
neutral corneal transplant, J Refract Surg 21 (2005), pp. 339–345. • (5) F.W. Price Jr and M.O. Price, Descemet's stripping with endothelial keratoplasty in 200 eyes: early
challenges and techniques to enhance donor adherence, J Cataract Refract Surg 32 (2006), pp. 411–418. • (6) M.O. Price and F.W. Price Jr, Descemet's stripping with endothelial keratoplasty comparative outcomes
with microkeratome-dissected and manually dissected donor tissue, Ophthalmology 113 (2006), pp. 1936–1942.
• (7) M.S. Gorovoy, Descemet-stripping automated endothelial keratoplasty, Cornea 25 (2006), pp. 886–889. • (8) M.A. Terry, K.L. Hoar, J. Wall and P. Ousley, Histology of dislocations in endothelial keratoplasty (DSEK
and DLEK): a laboratory-based, surgical solution to dislocationin 100 consecutive DSEK cases, Cornea 25 (2006), pp. 926–932.
• (9) S.B. Koenig and D.J. Covert, Early results of small-incision Descemet's stripping and automated endothelial keratoplasty, Ophthalmology 114 (2007), pp. 221–226.
• (10) Dapena I, Moutsouris K, Ham L, Melles G. Graft Detachment Rate. Ophthalmology. 2010; 117, 4: 847.
• (11) Koenig SB, Covert DJ, Dupps WJ, et al. Visual acuity, refractive error, and endothelial cell density six months after Descemet stripping and automated endothelial keratoplasty (DSAEK). Cornea. 2007;26:670-674.
• (12) Terry MA. Endothelial Keratoplasty: A Comparison of Complication Rates and Endothelial Survival between Precut Tissue and Surgeon-Cut Tissue by a Single DSAEK Surgeon. Trans Am Ophthalmol Soc. 2009 December; 107: 184–191.
• (13) Price MO. Baig KM. Brubaker JW. Price FW Jr. Randomized, prospective comparison of precut vs surgeon-dissected grafts for descemet stripping automated endothelial keratoplasty. American Journal of Ophthalmology. 146(1):36-41, 2008 Jul.