
D IAGNOSTICS AT WORK : From the clinic to the community Nitika Pant Pai, MD, MPH., PhD Madhukar Pai,...
51
DIAGNOSTICS AT WORK: From the clinic to the community Nitika Pant Pai, MD, MPH., PhD Madhukar Pai, MD, PhD
-
Upload
katherine-trick -
Category
Documents
-
view
213 -
download
0
Transcript of D IAGNOSTICS AT WORK : From the clinic to the community Nitika Pant Pai, MD, MPH., PhD Madhukar Pai,...

DIAGNOSTICS AT WORK: From the clinic to the community
Nitika Pant Pai, MD, MPH., PhD
Madhukar Pai, MD, PhD

WHY SCREENING, DIAGNOSTIC AND PROGNOSTIC TESTS MATTER
o Diagnosis is the first and important step in the pathway to correct treatment• “Companion diagnostics” are emerging as a critical theme
o Early and rapid diagnosis can reduce morbidity, improve patient outcomes, and reduce cost of care
o Tests can o identify risk factors
o predict prognosis
o monitor therapy over time
o promote healthy behaviours
o tailor therapies (i.e. personalized medicine)

IN THE PAST, DOCTORS RELIED ON THEIR CLINICAL INTUITION…
Source: The Hindu

AND SOME BASIC TESTS LIKE MICROSCOPE
Antonie van Leeuwenhoek (1632–1723), the father of microbiology, is best known for his work to improve the microscope and use it for microbiology
Source: Wikipedia

STETHOSCOPE AND X-RAYS
Rene Laënnec in Paris invented the first stethoscope in 1816.
Wilhelm Rontgen detected x-rays in 1895.
Source: Wikipedia

TODAY, WE HAVE COME A LONG WAY…
www.nature.com


THE OLD STETHOSCOPE COMES OF AGE!
http://www.thinklabs.com/

TESTS FOR TUBERCULOSIS: FROM MICROSCOPE TO RAPID MOLECULAR TESTS (<2 HOURS)

TESTS FOR HIV: FROM THE LAB TO OUR HOMES
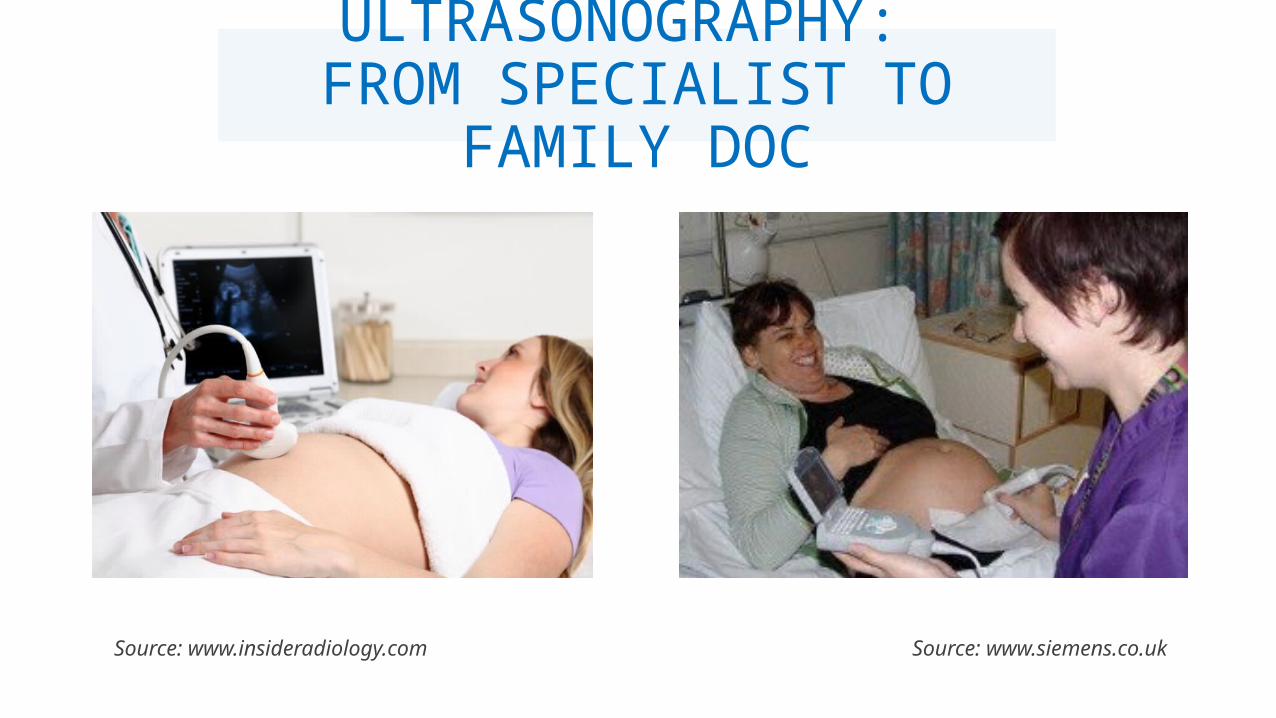
Source: www.insideradiology.com Source: www.siemens.co.uk
ULTRASONOGRAPHY: FROM SPECIALIST TO
FAMILY DOC

YOUR MOBILE SMARTPHONE HAS EMERGED AS A POWERFUL NEW
DIAGNOSTIC TOOL!
http://www.healthcanal.com/eyes-vision/41915-eye-phone-that-could-help-prevent-blindness.html http://lgtmedical.com/global-health/pneumonia.html
Retina imaging
Vital signs, oxygen saturation

YOUR TABLET IS NOW A HEALTH TECHNOLOGY
ASSISTANTThis Slate is a book-sized machine; it wirelessly communicates with an Android tablet and includes a bag of plug-and-play sensors that measure blood pressure and levels of blood sugar and hemoglobin, conduct electrocardiography (EKG) tests, etc.
http://www.the-scientist.com/?articles.view/articleNo/33761/title/A-Dime-a-Dozen/

WEARABLE HEALTH TECHNOLOGIES:
Fitbit, iWatch, OMwear RECORD SLEEP, VITAL SIGNS
http://www.nuubo.com/ http://www.cnet.com/news/wearable-tech-most-important-race-turning-heartbeats-into-cash/
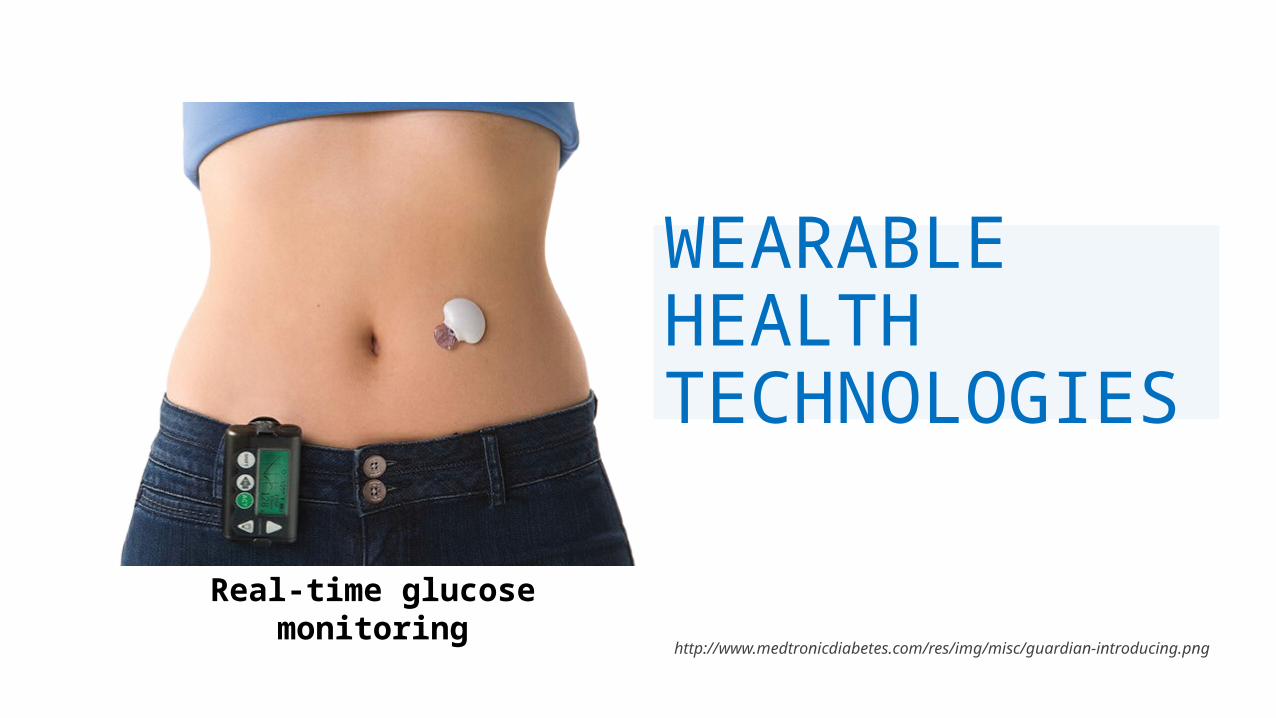
WEARABLE HEALTH TECHNOLOGIES
http://www.medtronicdiabetes.com/res/img/misc/guardian-introducing.png
Real-time glucose monitoring
MADHUKAR PAI

WE ARE SO READY FOR THE TRICORDER!
http://blogs-images.forbes.com/markpmills/files/2012/01/tricorder-spock1.jpg


INNOVATION: HIVSmart!: INTEGRATED SMARTPHONE
APP AND INTERNET BASED HIV SELF TESTING STRATEGY
PROBLEM: HEALTH FACILITY BASED
TESTINGoBarriers:
o Stigma and Discrimination
o Social Embarrassment
o Fear of visibility
o Lack of Confidentiality
o Judgemental Attitudes
o About 50% people WORLDWIDE and 25% DOMESTICALLY don’t
know their HIV status!!
19

NEEDa. Confidential, Anonymous,
personalized, b. convenient, non invasive, cost
effective
c. Easy linkages, easy conduct
d. Saves time and money

HIV SELF-TEST APP: ANDROID, iPHONE
21Copyright protected. HIVSmart! is copyright protected authored by Dr Pant Pai and trainees (Roni Deli-Houssein, Sushmita Shivkumar, Caroline Vadnais) and owned by McGill University

22
SMARTER CONDUCT & LINKAGES
© Pant Pai and McGill University 2013

SO, WE HAVE NOW ENTERED THE BRAVE NEW WORLD OF
DIAGNOSTICS!o Faster, Easier, time savingso Real-timeo Personalizedo Connectivity (from your
mobile to your doctor’s laptop)
o At point of clinical care, at home, any place, anywhere!

And the world of big data 1. Data:
1. Social, medical, genetic, daily caloric intake, daily sleep, vital signs. Step count, all will be available (in real time)
2. Anonymized, compliant with confidentiality guidelines
2. Sources:
1. from electronic medical records available on your phone, to your family physician and in your health facility
2. from smart wear and Fitbits- on the internet and phones
3. from personalized genomics testing are available on the cloud
3. What for?
1. For a personalized, plan for health promotion, targeted medication intake, monitoring, and better management.
This is all exciting, but…

HOW DO WE KNOW THESE NEW TESTS ARE ACCURATE? THAT THEY ACTUALLY MAKE A DIFFERENCE??
o This is where clinical epidemiologists enter the picture.
o Diagnostic tests, just like drugs and vaccines, need adequate validation before they can be used on people.
o Just like drug trials, we do diagnostic trials.
DIAGNOSIS VS SCREENING:
THEY ARE DIFFERENT!
29
o A diagnostic test is done on sick people• patient presents with symptoms• pre-test probability of disease is high (i.e. disease
prevalence is high)
o A screening test is usually done on asymptomatic, apparently healthy people• healthy people are encouraged to get screened• pre-test probability of disease is low (i.e. disease
prevalence is low)
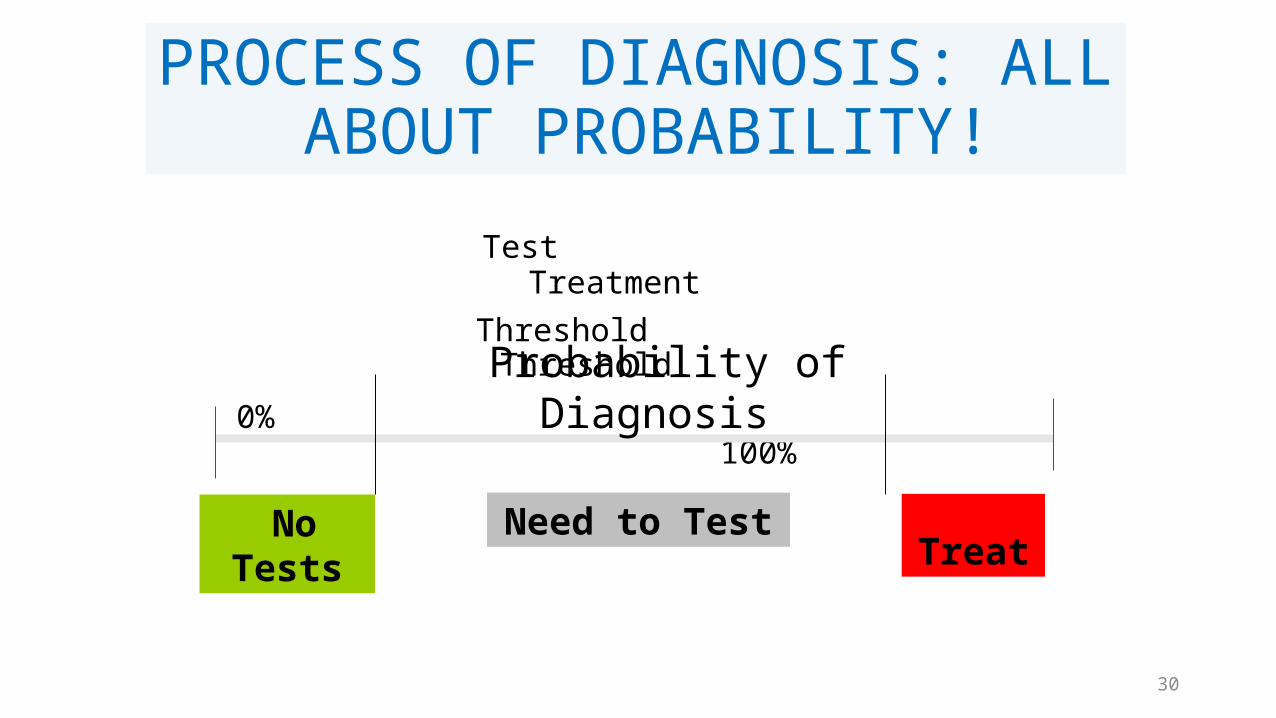
PROCESS OF DIAGNOSIS: ALL ABOUT PROBABILITY!
Test Treatment
Threshold Threshold
0% 100%
Probability of Diagnosis
No Tests
Need to Test Treat
30

THE PERFECT DIAGNOSTIC TEST
☻☺
X YDisease No
Disease 31
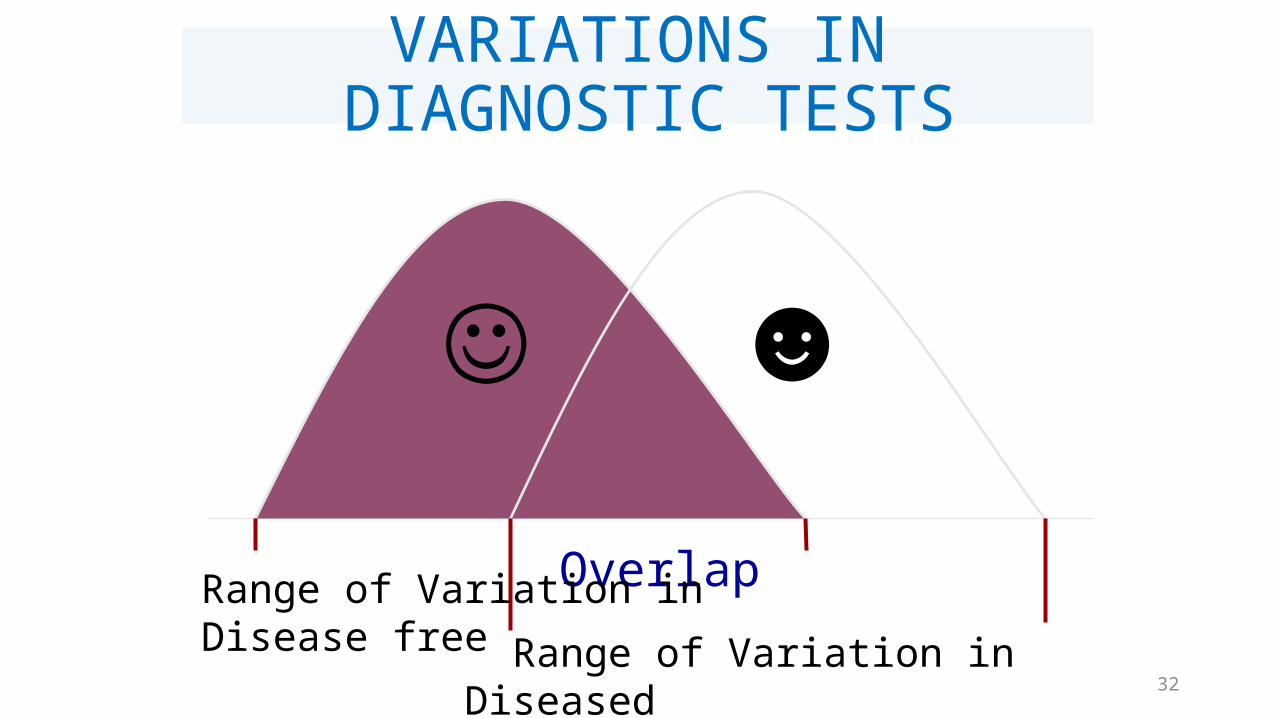
VARIATIONS IN DIAGNOSTIC TESTS
☺ ☻ Overlap
Range of Variation in Disease free
Range of Variation in Diseased 32
SO, CUT-POINTS MATTER A LOT!
o Many tests produce continuous numbers, and doctors tend to use cut-points to make decisions
o Cut-points are a compromise – they are not perfect
o Same test can produce different results, based on cut-points used
o Cut-points can change over time

There is no perfect test!
All we can hope to do is increase or decrease probabilities, and Bayes’ theorem helps with this process
34

BAYES' THEORY
pre-test probability
post-test probability
Test
Post-test odds = Pre-test odds x Likelihood ratio
35
What you thought before + New information = What you think now

pre-test probability
LOW
post-test probability
HIGH
Test
o An accurate test will help reduce uncertainty
o The pre-test probability is revised using test result to get the post-test probability
o Tests that produce the biggest changes from pretest to post-test probabilities are most useful in clinical practice [very large or very small likelihood ratios]
pre-test probability
HIGH
post-test probability
LOWTest
Bayesian approach to diagnosis
36

Steps in evaluating a diagnostic test
37
o Define gold standard
o Recruit consecutive patients in whom the test is indicated (in whom the disease is suspected)
o Perform gold standard and separate diseased and disease free groups
o Perform test on all and classify them as test positives or negatives
o Set up 2 x 2 table and compute:
• Sensitivity• Specificity• Predictive values• Likelihood ratios
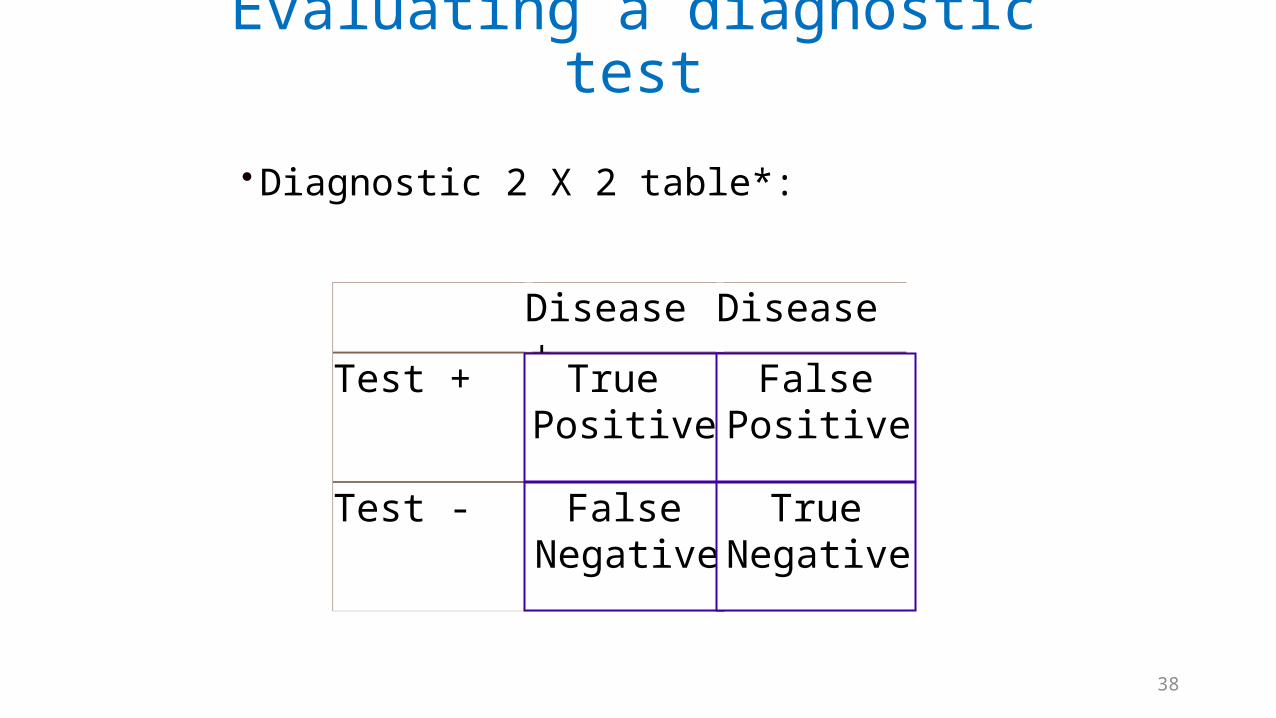
Evaluating a diagnostic test
• Diagnostic 2 X 2 table*:
Disease + Disease -
Test + True Positive
False Positive
Test - False Negative
True Negative
38

Disease present
Disease absent
Test positive
True positives
False positives
Test negative
False negative
True negatives
Sensitivity[true positive rate]
The proportion of patients with disease who test positive = P(T+|D+) = TP / (TP+FN)
39

Disease present
Disease absent
Test positive
True positives
False positives
Test negative
False negative
True negatives
Specificity[true negative rate]
The proportion of patients without disease who test negative: P(T-|D-) = TN / (TN + FP).
40

Disease present
Disease absent
Test positive
True positives
False positives
Test negative
False negative
True negatives
Predictive value of a positive test
Proportion of patients with positive tests who have disease = P(D+|T+) = TP / (TP+FP)
41
Disease present
Disease absent
Test positive
True positives
False positives
Test negative
False negative
True negatives
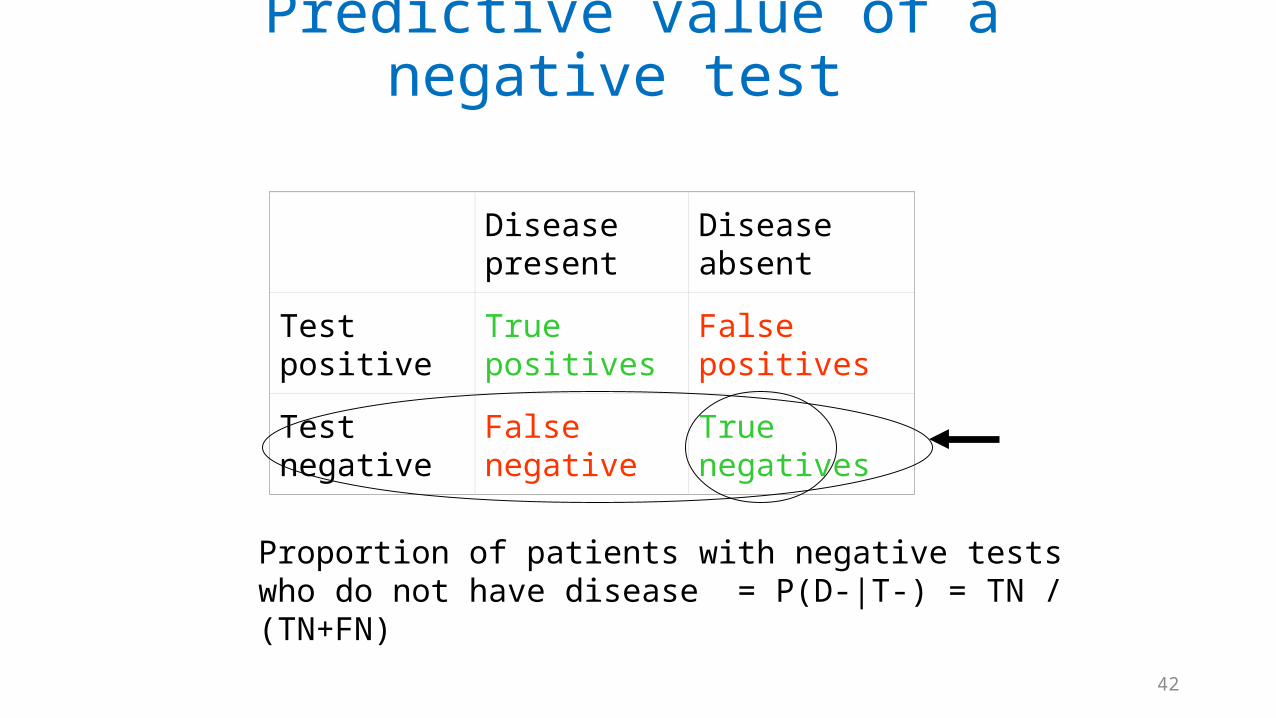
Predictive value of a negative test
Proportion of patients with negative tests who do not have disease = P(D-|T-) = TN / (TN+FN)
42

Imagine a hypothetical population (some with disease and others without)
Loong T BMJ 2003;327:716-719©2003 by British Medical Journal Publishing Group
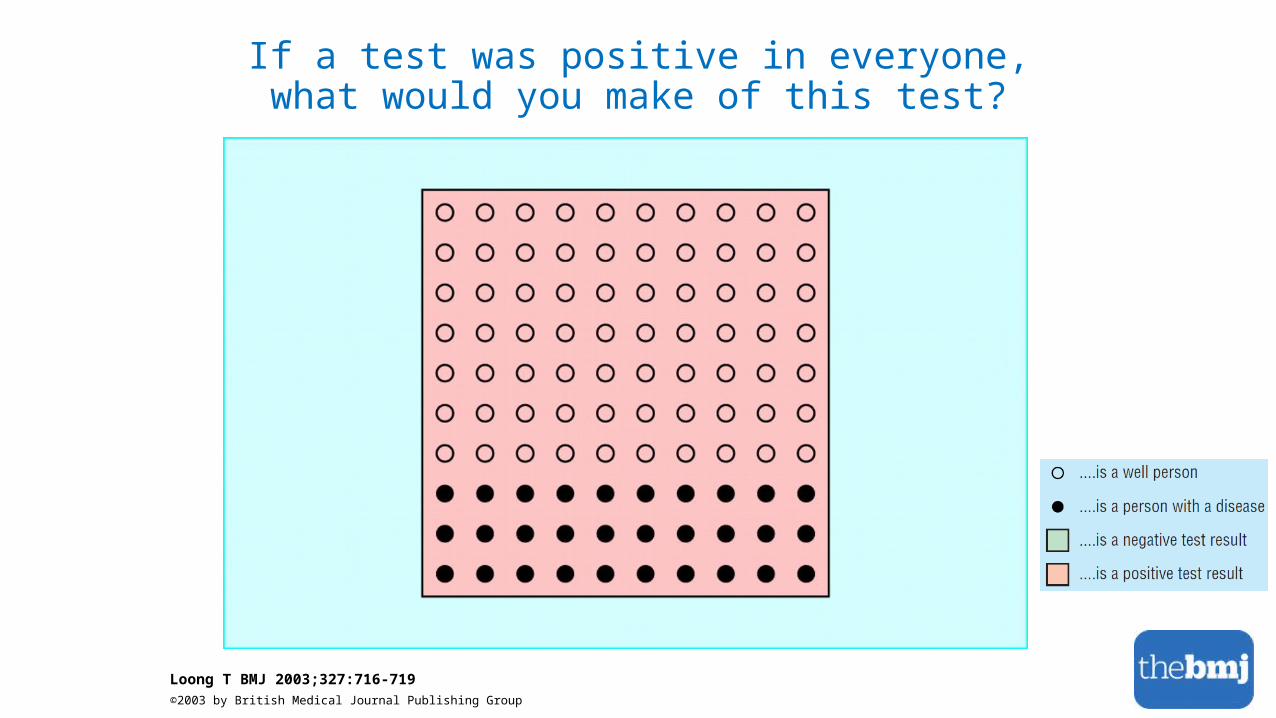
If a test was positive in everyone, what would you make of this test?
Loong T BMJ 2003;327:716-719©2003 by British Medical Journal Publishing Group
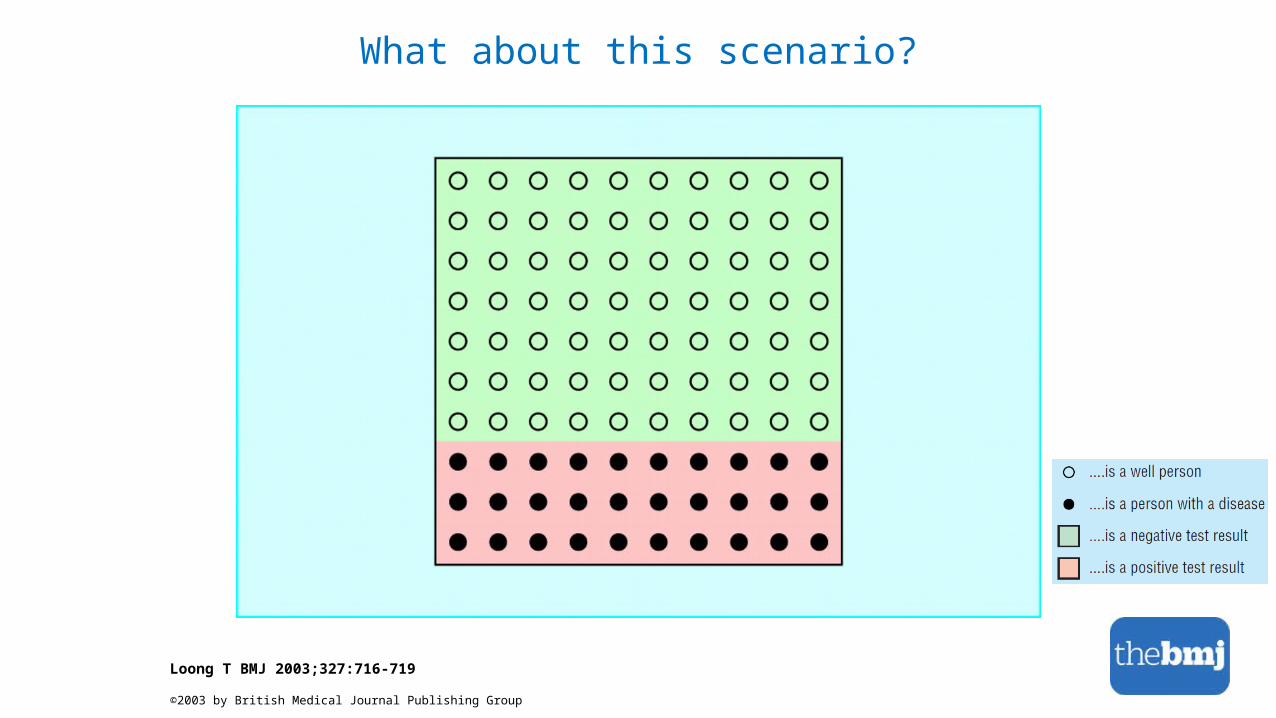
What about this scenario?
Loong T BMJ 2003;327:716-719
©2003 by British Medical Journal Publishing Group
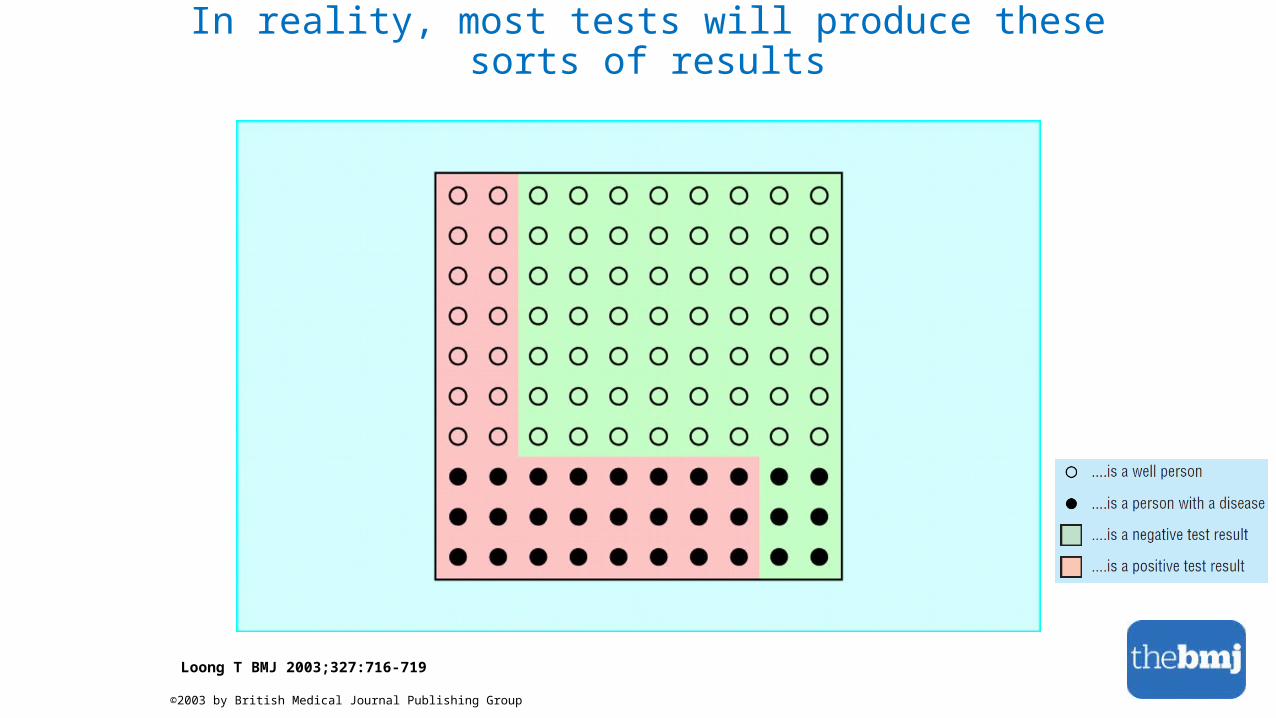
In reality, most tests will produce these sorts of results
Loong T BMJ 2003;327:716-719
©2003 by British Medical Journal Publishing Group

Example: Ultrasonography for Down Syndrome
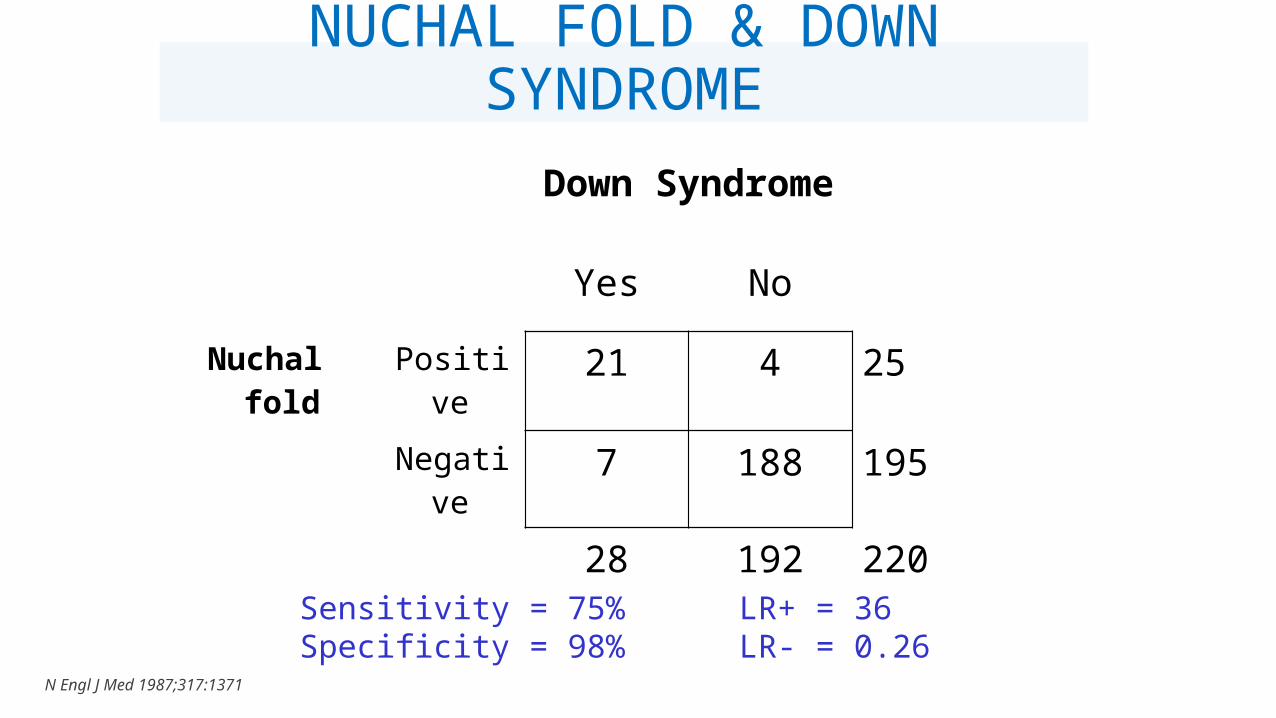
NUCHAL FOLD & DOWN SYNDROME
Down Syndrome
Yes No
Nuchal fold Positive 21 4 25
Negative 7 188 195
28 192 220
Sensitivity = 75%Specificity = 98%
LR+ = 36LR- = 0.26
N Engl J Med 1987;317:1371

The interpretation of this test will depend a lot on the context (i.e. prior
probability)
o Scenario 1:• Mrs. B, a 20-year old woman with a previous normal pregnancy,
seen at a community hospital
o Scenario 2:• Mrs. A, a 37-year old woman with a previous affected pregnancy,
seen at a high-risk clinic in a tertiary, referral hospital
o Who has a higher pretest probability of Down syndrome?

TAKE HOME MESSAGES
o Diagnostic tests are important and can help all of us
o But, they are not perfect
o Diagnostic and screening tests are very different and should not be confused
o Doctors and patients need to understand that all tests have their inherent error (i.e. false positives and false negatives)
o Tests should always be interpreted in context
o Tests should be avoided unless there is a clear indication
THANK YOU!!!We are grateful to:
• Prof Jim Hanley• Prof Abe Fuks• Mini-Med team:
• Elise, Gloria, Ibby & Kappy
• Department of Epidemiology, Biostatistics & Occupational Health
Slide credits: Sehar Manji, Executive Assistant











![Official Pai Sho Rules And Gameplay Kopielyrislaser.com/wp-content/uploads/2014/08/Pai-Sho-Rules-Gameplay.pdf · 2" [OFFICIAL(PAI(SHO(RULES(AND(GAMEPLAY]!! Basic Pai Sho Playing Materials](https://static.fdocuments.in/doc/165x107/5c4368b893f3c34c5500e85e/official-pai-sho-rules-and-gameplay-2-officialpaishorulesandgameplay.jpg)





