CYTOPATHOLOGY-8 DR. MAHA AL-SEDIK. Sputum, bronchial wash and bronchial brush cytology.
43
CYTOP A THO LO GY-8 DR. MAHA AL-SEDIK
-
Upload
leslie-tucker -
Category
Documents
-
view
232 -
download
5
Transcript of CYTOPATHOLOGY-8 DR. MAHA AL-SEDIK. Sputum, bronchial wash and bronchial brush cytology.
CYTOPA
THOLO
GY-8
DR
. M
AH
A A
L-SED
IK
Sputum , bronchial wash and bronchial
brush cytology
Objectives:1- introduction.
2- Safety in work.
3- Role of cytology in respiratory disease.
4- Cytological sample methods.
5- Sputum.
6- Hemoptysis
7- Importance of sputum culture.
8- Sputum collection and processing.
9- Bronchial washing.
10- Bronchial brushing.
Introduction: Cytological examination of specimens obtained from
the respiratory tract is a primary and frequently the
initial diagnostic technique performed in patients
with respiratory symptoms or in those presenting
with a pulmonary abnormality.
Due to the complexity of the respiratory tract and the
location of various target lesions, a variety of
cytological techniques have been developed for the
study of diseases involving the respiratory system.
Safety at Work:
Laboratory staff processing pulmonary cytological
materials are at particular risk of exposure to aerosol
infections.
They must protect themselves from this potential
hazard by wearing protective masks and gloves during
dealing with the samples, and following standard
laboratory hygienic procedures.
Major role:• Diagnosis of malignant neoplasms involving lung
both primary and metastatic.
Minor role:• Specific inflammatory process.
• Benign neoplasms.
Role of cytology in respiratory disease
Cytological Sampling Methods in respiratory
system:Sputum: from a spontaneous deep cough, obtained on
arising in the morning.
Bronchial Brushings: using bronchoscope.
Bronchial Washings: using bronchoscope.
Sputum
It is a mucous layer that covers the airways and
protects bronchial epithelium against inhaled noxious
substances.
Sputum is a mucous substance that is secreted into
the airways of the respiratory tract (lungs ,bronchi,
trachea) and can be coughed up, spit out or
swallowed.
It is produced by surface epithelial cells and sub
mucous glands.
Sputum Cytology
The spontaneous production of significant amounts of
sputum often indicates pulmonary disease.
Sputum is composed predominantly of mucoid
substances, and variable numbers of inflammatory
and epithelial cells.
Variations in the numbers of macrophages,
neutrophils, and epithelial cells and morphologic
alterations in the latter elements can yield significant
insight into the underlying pathologic process.
Chemical composition:
95% water
5 % organic components:
Squamous epithelial cells.
Respiratory epithelial cells.
Polymorphonuclear leukocytes.
Mononuclear cells.
Alveolar macrophages.
Carbohydrates ( such as sialic acid which contribute to
its high viscosity).
Proteins ( enzymes, immunoglobulins), glycoproteins.
Lipids.
5 CELLS3 FOOD
Abnormality of sputum:
Normal sputum is either white or colorless.
Yellow to green sputum can be an indication of pus,
infection such as pneumonia.
Blood in sputum is called hemoptysis which could be
due to e.g. ; lung cancer, tuberculosis, lung abscess ,
hemorrhage.
Parasites in sputum can occur as in ascaris.
Hemoptysis:
The expectoration (coughing up) of blood or of blood
stained sputum .
1 •TB
2 •Chronic bronchitis
3 •Cancer
4 •Pneumonia
5 •Trauma
6 •Autoimmune disease
Common causes of hemoptysis
Sputum
Culture
cytology
Importance of culture:
Detect and identify bacteria or fungi causing an
infection (such as pneumonia or tuberculosis).
Identify the best antibiotic to treat the infection
(sensitivity testing).
Monitor treatment of an infection.
Importance of Sputum Cytology:
Major role:• Diagnosis of malignant neoplasms involving lung
both primary and metastatic.
Minor role:• Specific inflammatory process.
• Benign neoplasms.
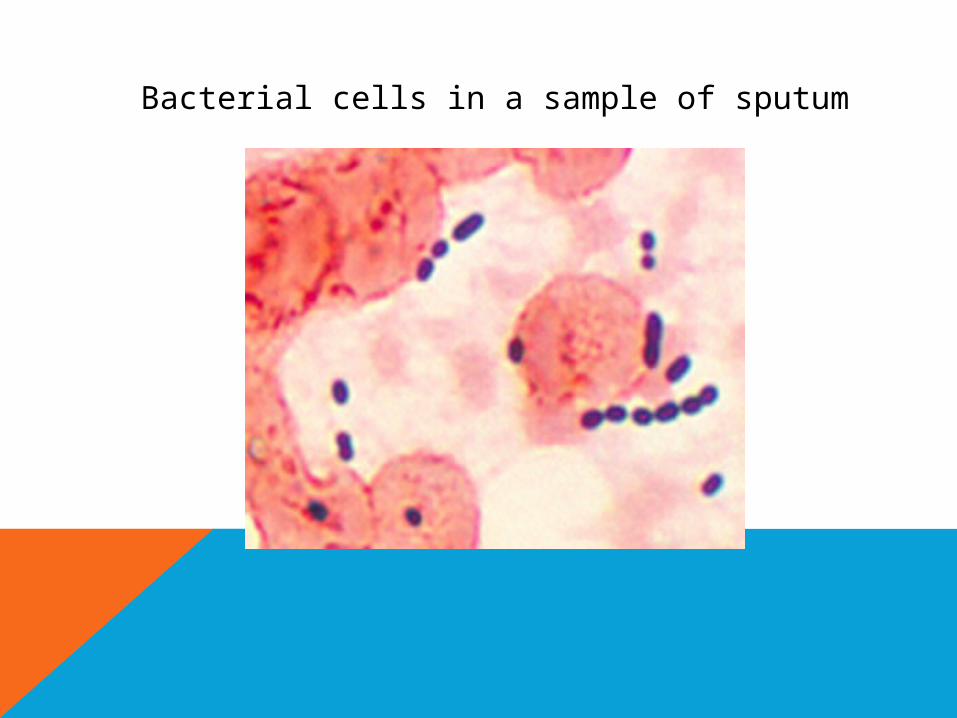
Bacterial cells in a sample of sputum
Collection Procedure:
a. Patient Preparation:
• The optimum time for specimen collection is within
15 to 30 minutes after waking and before eating
breakfast.
• Brushing of teeth or rinsing of the mouth with water
will reduce contamination by saliva.
• Instruct the patient to inhale and exhale deeply
forcing air from the lungs using the diaphragm.
Repeat until the patient coughs and is able to
produce a sputum specimen.
b. Collect the specimen in the sterile container,
attempting to obtain at least one teaspoon of sputum.
Saliva is of no diagnostic value.
Greater diagnostic yield may be obtained if specimens
are submitted on three to five successive mornings.
When sufficient amounts of spontaneously
produced sputum are unobtainable,
specimens may be induced by inhalation of a
nebulized solution composed of 15% sodium
chloride, with or without 20% propylene
glycol, or simply 3–8% sodium chloride
heated to 115°F.
c. Add 70% alcohol as soon as possible in a volume
equal to the specimen collected. Label each
container with the patient name, site, source and
requisition peel off number.
d. STORAGE: Submit the specimen at room
temperature.
The most popular techniques in handling sputum are
the ‘‘pick-and-smear’’ technique and the Saccomanno
methodology.
I. pick-and-smear:
Experience is essential to pick out significant areas
for processing.
They are prepared as direct smears for immediate
fixation (95% ethyl alcohol or spray fixation) then
stained with hematoxylin-eosin.
Saccomanno methodology:
When a significant delay is anticipated between
specimen taking and laboratory processing, prefixation
and processing by the Saccomanno method are
preferred.
Cells are collected in 50% ethanol and 2% polyethylene
glycol (carbowax).
Upon receipt in the laboratory, a blender is used to
emulsify the specimen, which is subsequently
centrifuged and prepared as smears.
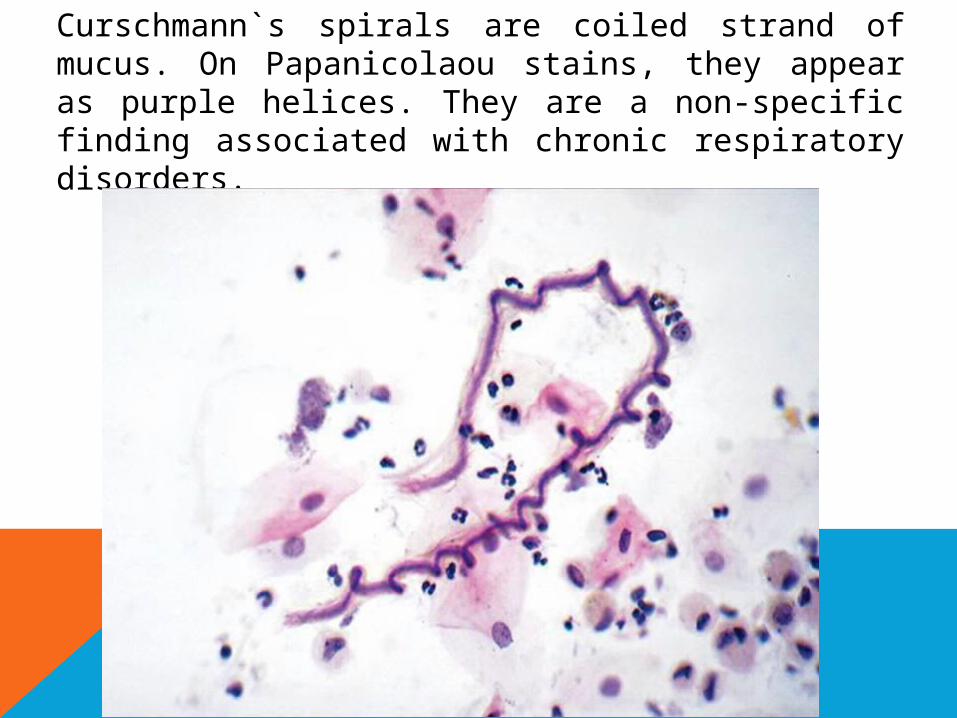
Curschmann`s spirals are coiled strand of mucus. On Papanicolaou stains, they appear as purple helices. They are a non-specific finding associated with chronic respiratory disorders.
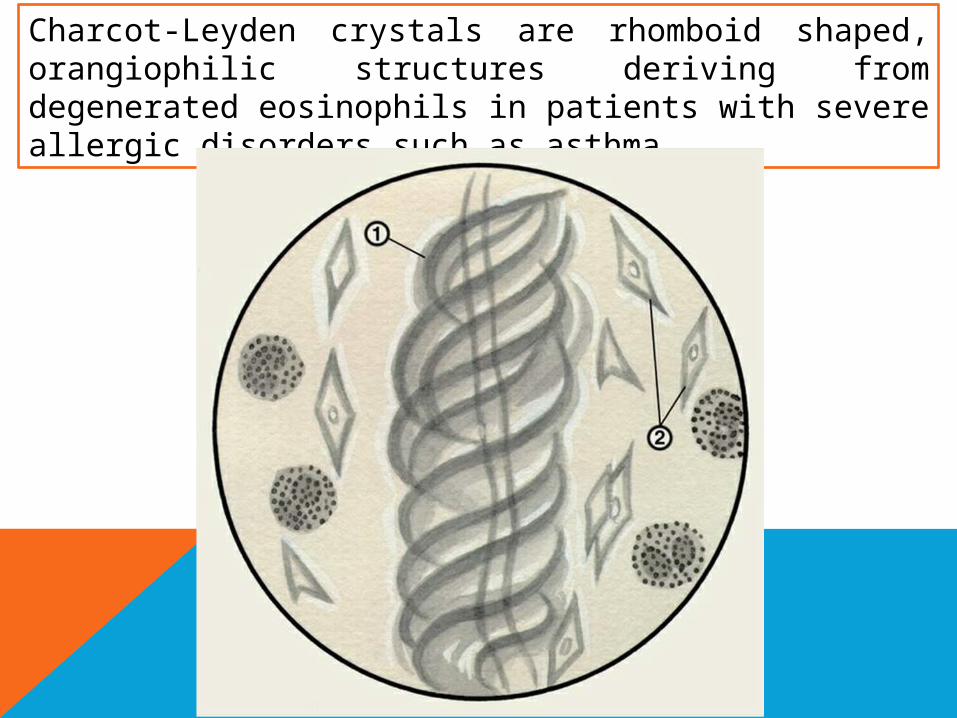
Charcot-Leyden crystals are rhomboid shaped, orangiophilic structures deriving from degenerated eosinophils in patients with severe allergic disorders such as asthma.
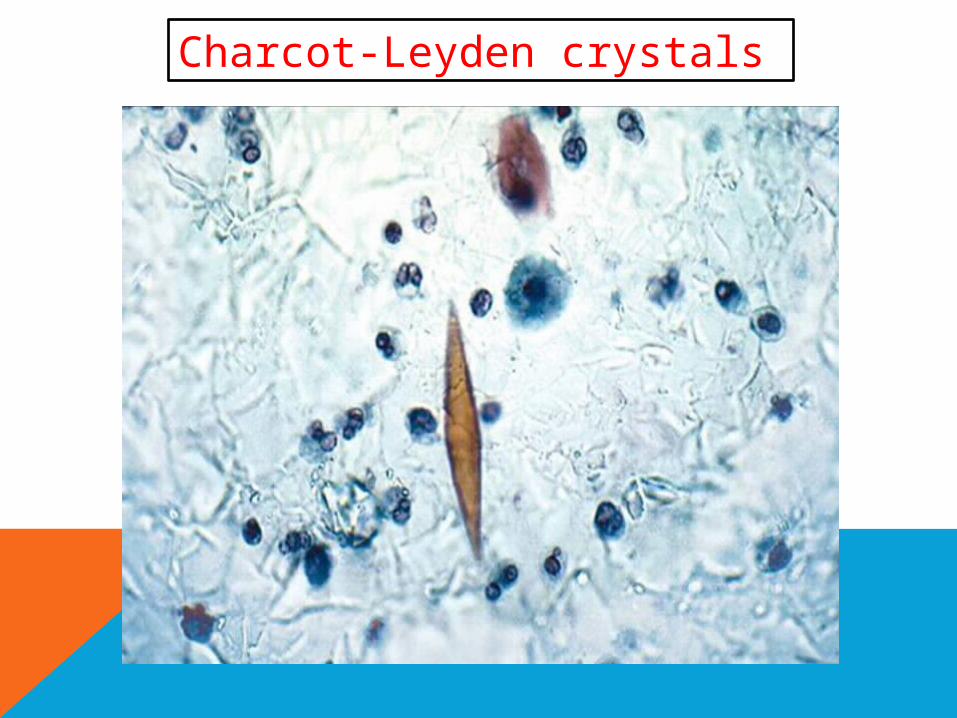
Charcot-Leyden crystals
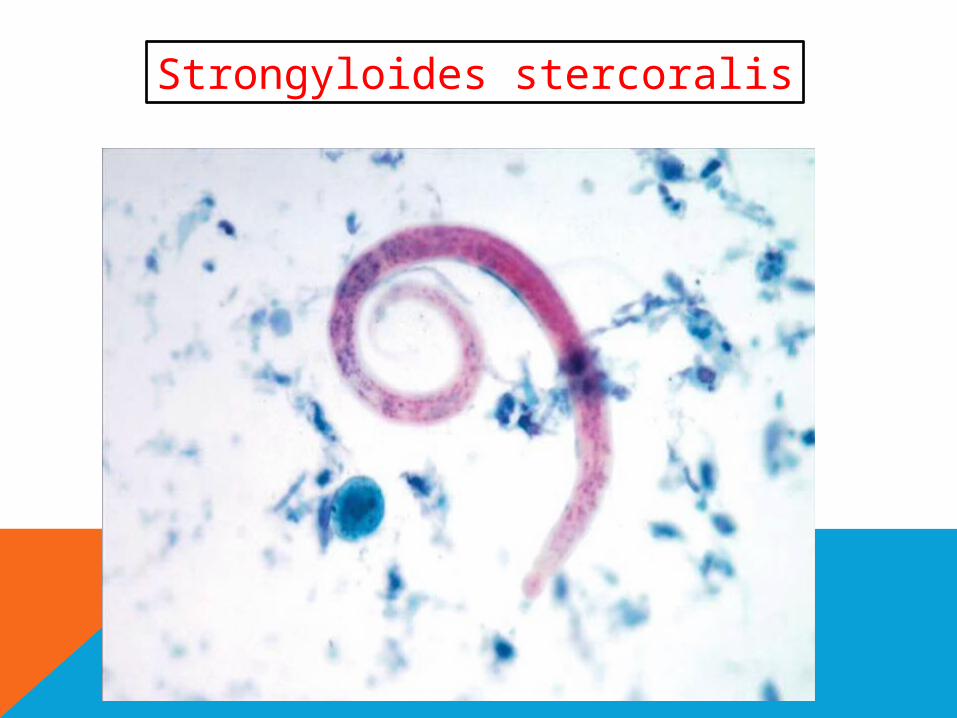
Strongyloides stercoralis
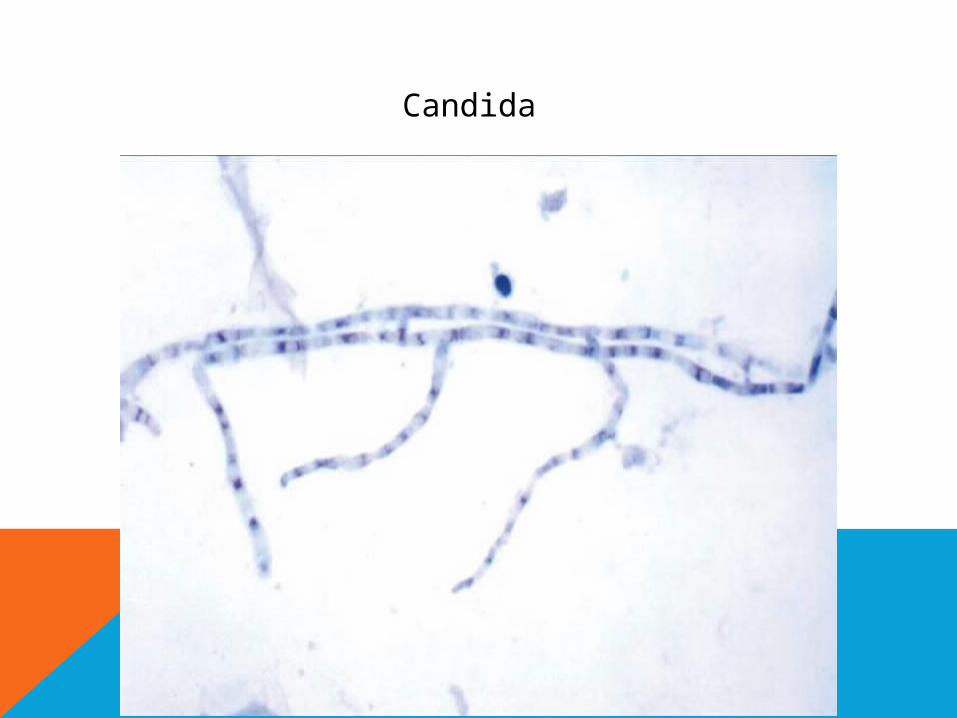
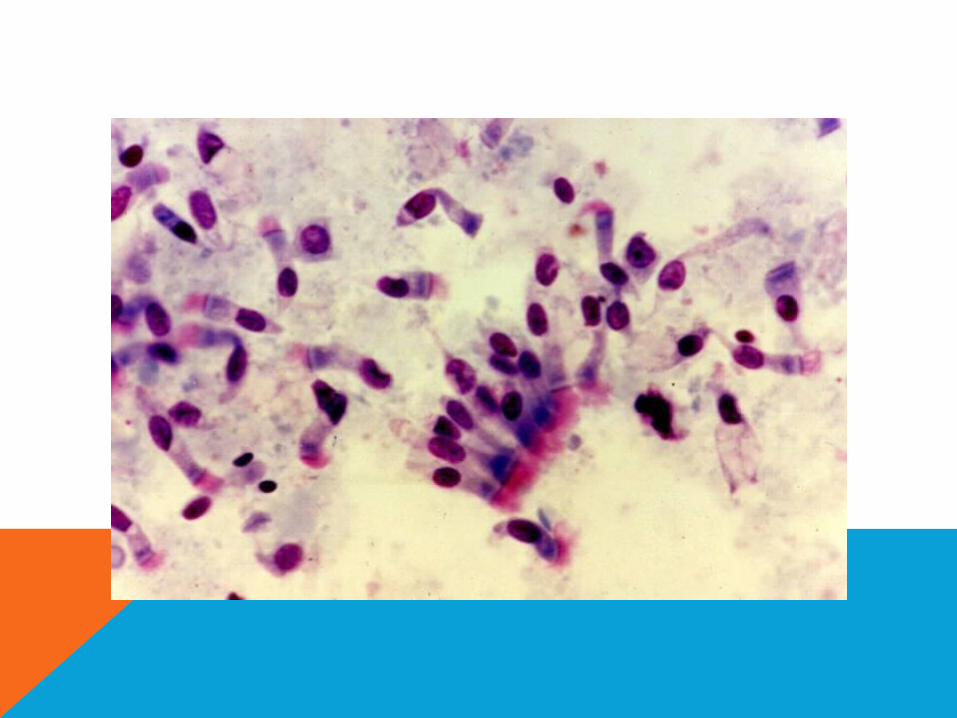
Candida
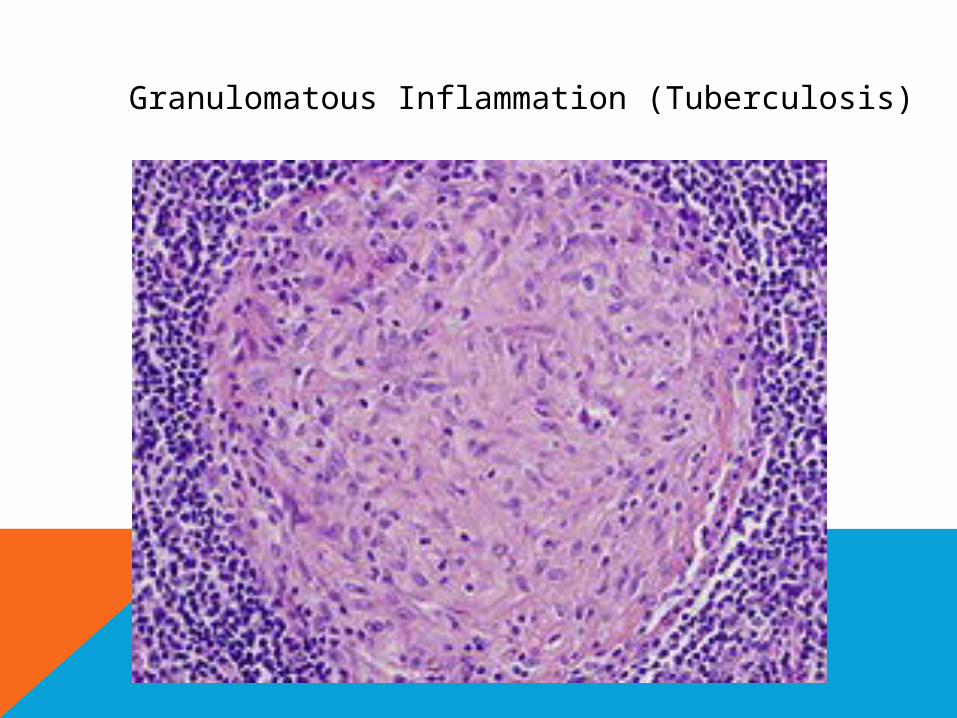
Granulomatous Inflammation (Tuberculosis)
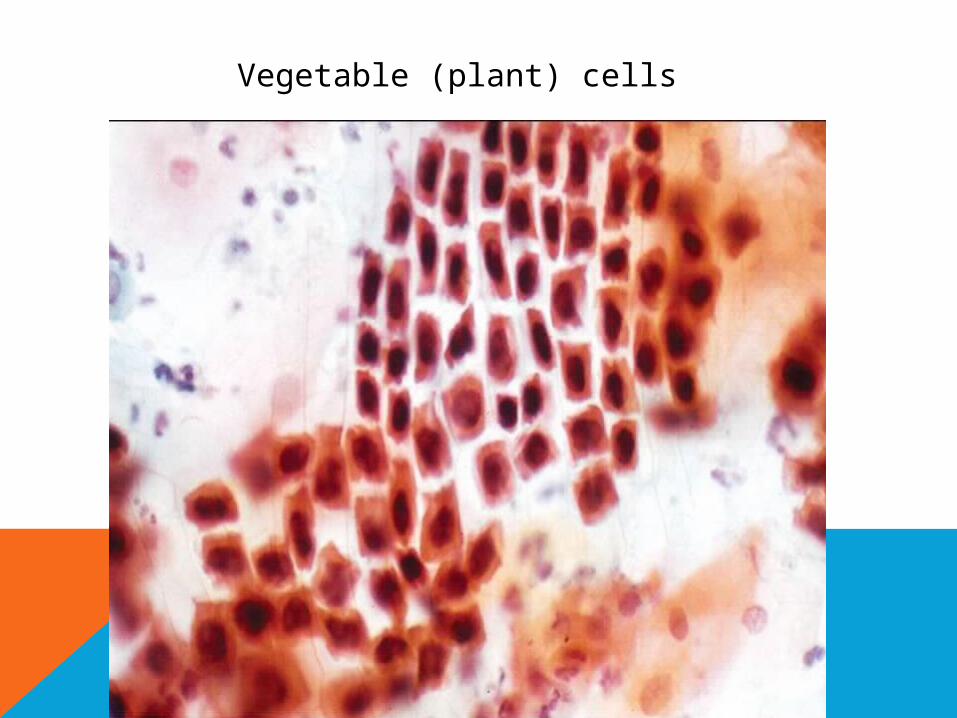
Vegetable (plant) cells
Bronchial Washings and Brushings
Indications:
Bronchial brushings and washings are complementary to
sputum cytology in the diagnosis of pulmonary lesions.
The most common indications for bronchoscopy: Persistent cough.
Radiographic documentation of a new solitary
pulmonary nodule.
Un diagnosed hemoptysis.
Persistent localized wheezes.
persistent infiltrates on chest x-ray.
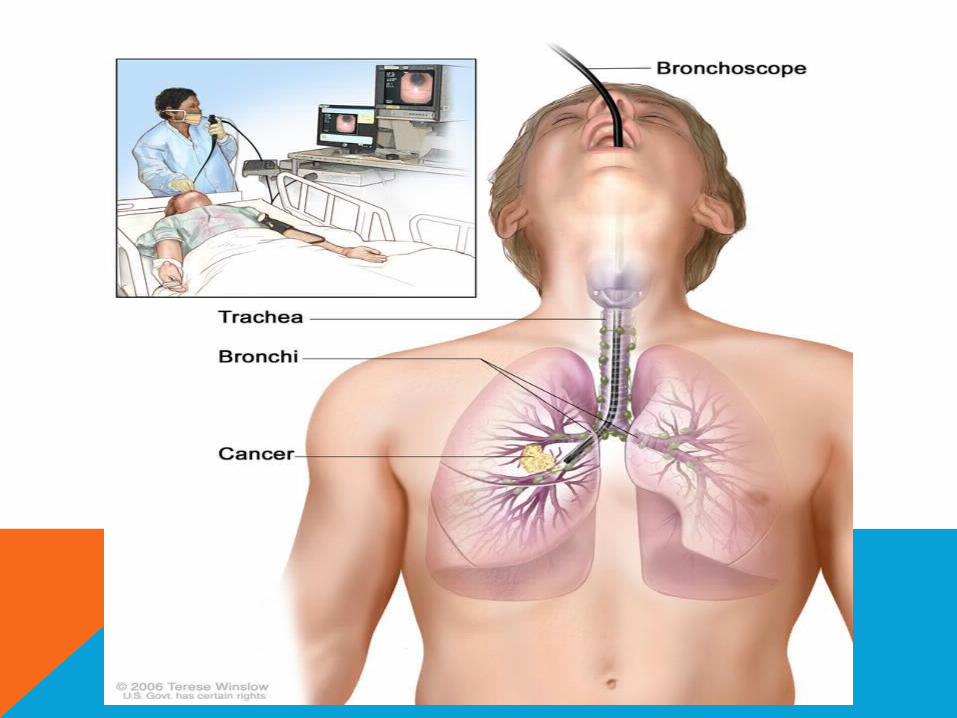
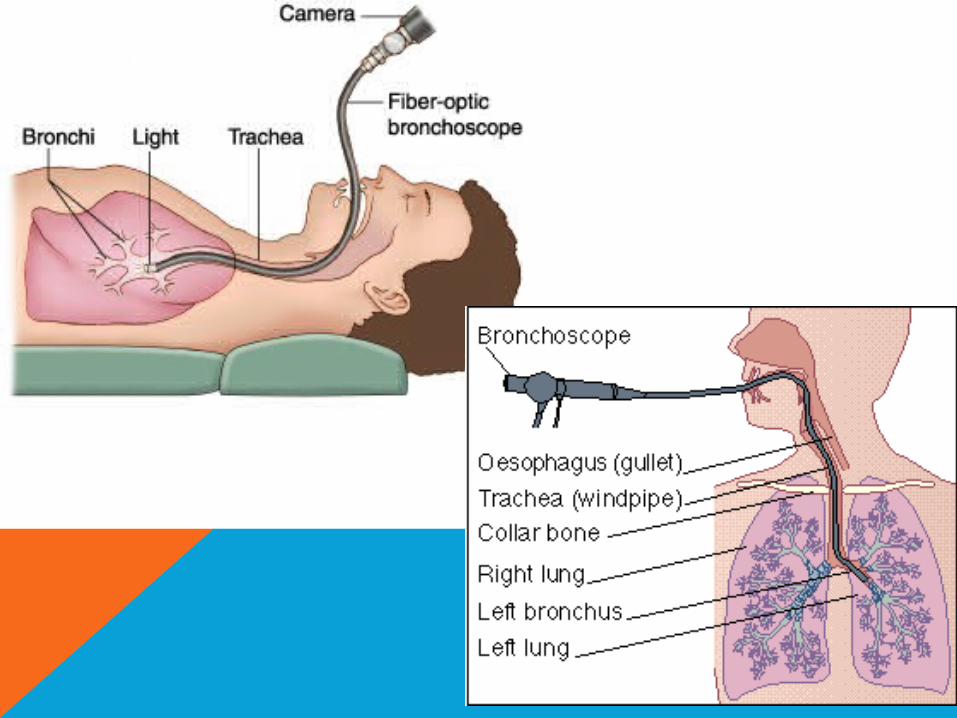
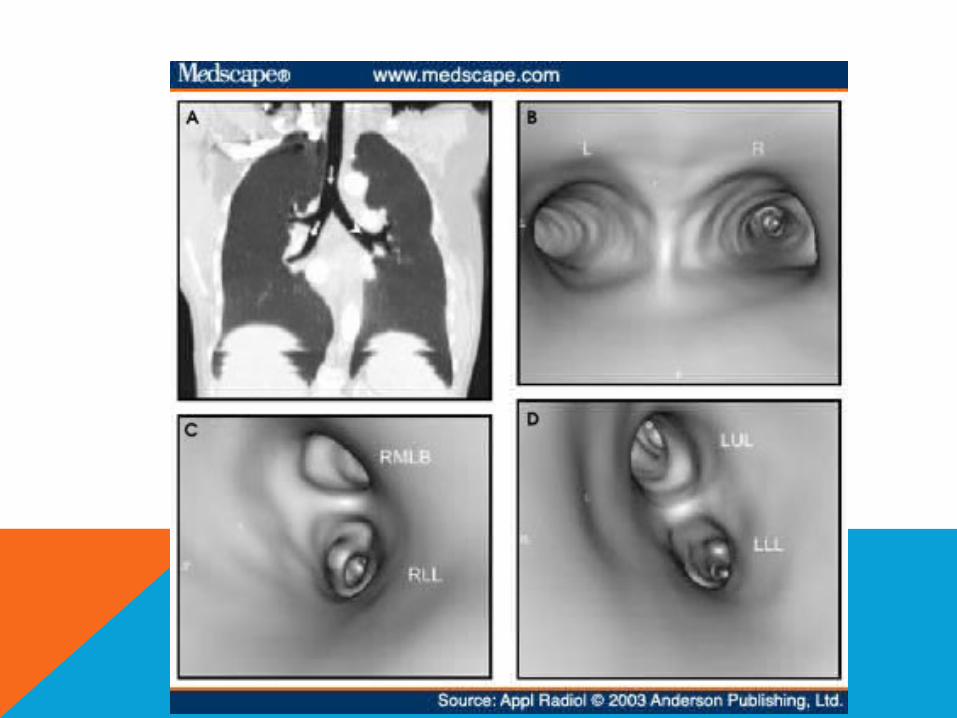
Bronchial washing
is part of a procedure called a bronchoscopy, in which a
physician looks into the lungs with a fiber optic
bronchoscope to check for irregularities and take tissue
samples.
Technique:
The physician injects saline through the bronchoscope
into the lung and then suctions it back out.

By checking the wash return fluid, the doctor can
diagnose bleeding, pneumonia, industrial pollutants,
fungal infections and different kinds of lung cancer.
Patients undergoing bronchial washing usually
receive topical anesthesia with sedation.
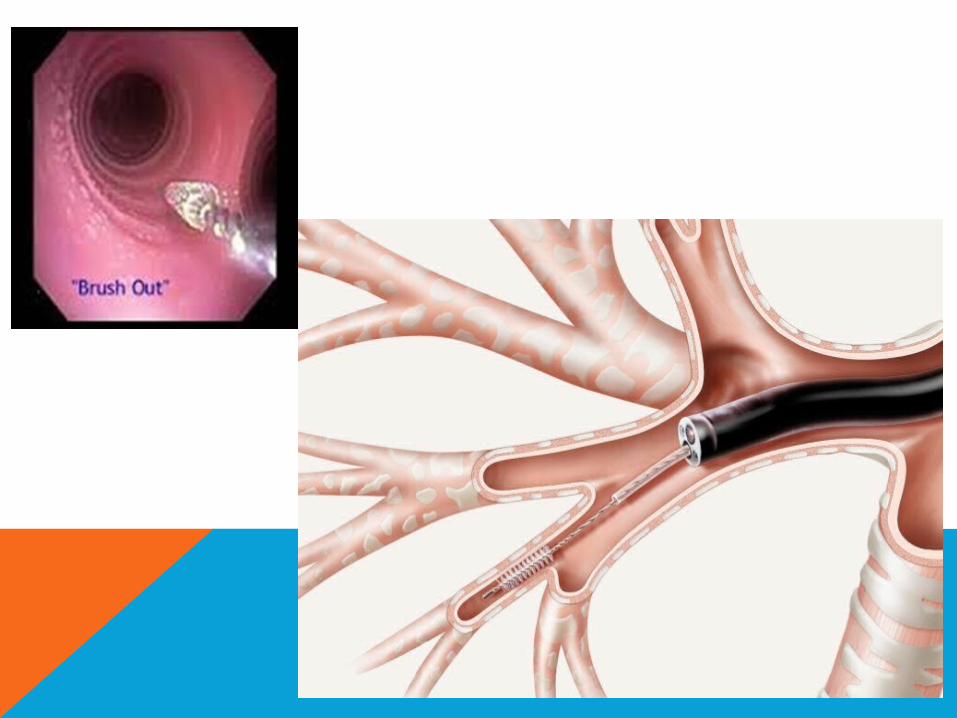
Bronchial brushing:
is a procedure in which cells are taken from the inside
of the airway mucosa or bronchial lesions.
Flexible brushes are passed through the bronchoscope,
and the bronchial surface is gently abraded to obtain
the specimen.
A bronchial brushing is used to find cancer and changes
in cells that may lead to cancer. It is also used to obtain
specimens for microbiologic diagnosis.
Upon withdrawing the brush, agitate the brush
vigorously in a 5 to 10 mL vial of sterile saline or
fixative. DO NOT APPLY THE BRUSH DIRECTLY TO
SLIDES. If possible, detach the brush and leave it
in the vial and better to be examined in 4 hours.