Cytologic spectrum of 227 fine-needle aspiration cases of chest-wall lesions
5
Cytologic Spectrum of 227 Fine-Needle Aspiration Cases of Chest-Wall Lesions Amit Goel, M.D., D.N.B., S.K. Gupta, M.D., F.A.M.S., * P. Dey, M.D., M.I.A.C., S. Radhika, M.D., Ph.D., and R. Nijhawan, M.D. This study was carried out with the objective of studying the cytomorphology of the wide variety of chest-wall lesions. Two hundred twenty-seven chest-wall lesions were studied over a pe- riod of 4 yr. Routine May-Gru ¨nwald-Giemsa (MGG) and hema- toxylin-eosin (H&E) slides were studied along with special stains, whenever required. The malignant lesions comprised 36.13% of all cases (81/227). Of the 126 benign lesions, the majority were inflammatory in nature (68/126), the next commonest lesion being lipoma (38/126). Rare cases of tuberculosis involving the sternum, epithelioid leiomyosarcoma, and neuroendocrine tumors involving ribs, malignant nerve sheath tumors involving the chest wall, metastatic carcinoma of the stomach and prostate, and papillary carcinoma thyroid are reported in this series. Histopathology was available in 24 cases, and hematological correlation in one case. A 100% cytohistological and cytohematological correlation was found, with no false positives or false negatives. In conclusion, fine-needle aspiration cytology is a rapid, diagnostic tool, eliciting many interesting lesions in the chest wall. It is useful not only in detecting primary and metastatic lesions, but also in follow-up of tumor recurrence. Diagn. Cytopathol. 2001;24:384 –388. © 2001 Wiley-Liss, Inc. Key Words: fine-needle aspiration cytology; chest wall The pathologic processes involving the chest wall arise from native tissue inherent to this region and include infec- tive/inflammatory, benign, and malignant lesions. They can be classified according to site of origin as skin and adnexal, soft-tissue tumors, bony cage lesions (arising from the ribs, sternum, and costo-chondral junction), and secondary tu- mors. The latter can be further subcategorized as direct extensions of underlying malignancies arising from the breast, lung, and mediastinum, or metastatic tumors. A comprehensive study of the various chest-wall lesions is, to the best of our knowledge, not available in the literature, although scattered reports of cold abscess of the chest wall, 1 tuberculous involvement of the ribs 2 and sternum, 3 invasion of the chest wall by bronchogenic carcinoma, 4 breast car- cinoma, 5 epithelial malignancies, 6 chondrosarcoma, 7 rib tu- mors, 8 malignant small round cell tumor, 9 –12 desmoid tu- mors, 13 and plexiform fibrohistocyte lesions 14 are available in the literature. This study is an attempt to present the cytomorphology of the plethora of chest-wall lesions. Materials and Methods Fine-needle aspiration cytology (FNAC) was performed on 227 cases of chest-wall lesions over a 4-yr period from 1996 –1999, in the Department of Cytology, Post Graduate Institute of Medical Education and Research (P.G.I.M.E.R.) (Chandigarh, India). The conventional procedure of FNAC was used with a 20-ml disposable syringe for suction and a 23-gauge, 1–1.5-inch-long needle. Palpable rib/sternal masses could be punctured with the thin needle in most instances, with or without local anesthesia, but sometimes thicker 18- or 20-gauge needles were required. Care was taken not to penetrate deeper tissues such as the pleura or lung. Nonpalpable lesions involving the ribs or sternum were aspirated under the suitable radio-imaging technique. The slides were immediately wet-fixed for hematoxylin- eosin (H&E) stain/immunostaining, and air-dried smears were used for the conventional Giemsa stain. Special stains such as periodic acid-Schiff (PAS), PAS-Alcian blue, or Ziehl-Neelson (Z-N) for acid-fast bacilli were carried out when indicated. If pus was aspirated, it was sent for culture for acid-fast bacilli. Limited immunostaining was done, using the indirect immunoperoxidase method for difficult cases. The primary antibodies used were directed against cytokeratin, leukocyte-common antigen Mic-2, HMB-45, and smooth muscle actin (SMA), all from Dako. Results The age range of 227 patients aspirated was from 5 mon to 86 yr, with a male:female ratio of 1.3:1. The variety of lesions are enumerated in Table I. Department of Cytology, Post Graduate Institute of Medical Education and Research (P.G.I.M.E.R.), Chandigarh, India * Correspondence to: Dr. S.K. Gupta, Department of Cytology, P.G.I.M.E.R., Chanidgarh-160012, India. E-mail: [email protected] Received 9 June 2000; Accepted 26 October 2000 384 Diagnostic Cytopathology, Vol 24, No 6 © 2001 WILEY-LISS, INC.
Transcript of Cytologic spectrum of 227 fine-needle aspiration cases of chest-wall lesions
Cytologic Spectrum of 227Fine-Needle Aspiration Casesof Chest-Wall LesionsAmit Goel, M.D., D.N.B., S.K. Gupta, M.D., F.A.M.S.,* P. Dey, M.D., M.I.A.C.,S. Radhika, M.D., Ph.D., and R. Nijhawan, M.D.
This study was carried out with the objective of studying thecytomorphology of the wide variety of chest-wall lesions. Twohundred twenty-seven chest-wall lesions were studied over a pe-riod of 4 yr. Routine May-Gru¨nwald-Giemsa (MGG) and hema-toxylin-eosin (H&E) slides were studied along with special stains,whenever required. The malignant lesions comprised 36.13% ofall cases (81/227). Of the 126 benign lesions, the majority wereinflammatory in nature (68/126), the next commonest lesion beinglipoma (38/126). Rare cases of tuberculosis involving the sternum,epithelioid leiomyosarcoma, and neuroendocrine tumors involvingribs, malignant nerve sheath tumors involving the chest wall,metastatic carcinoma of the stomach and prostate, and papillarycarcinoma thyroid are reported in this series. Histopathology wasavailable in 24 cases, and hematological correlation in one case.A 100% cytohistological and cytohematological correlation wasfound, with no false positives or false negatives. In conclusion,fine-needle aspiration cytology is a rapid, diagnostic tool, elicitingmany interesting lesions in the chest wall. It is useful not only indetecting primary and metastatic lesions, but also in follow-up oftumor recurrence. Diagn. Cytopathol. 2001;24:384–388.© 2001 Wiley-Liss, Inc.
Key Words:fine-needle aspiration cytology; chest wall
The pathologic processes involving the chest wall arisefrom native tissue inherent to this region and include infec-tive/inflammatory, benign, and malignant lesions. They canbe classified according to site of origin as skin and adnexal,soft-tissue tumors, bony cage lesions (arising from the ribs,sternum, and costo-chondral junction), and secondary tu-mors. The latter can be further subcategorized as directextensions of underlying malignancies arising from thebreast, lung, and mediastinum, or metastatic tumors. Acomprehensive study of the various chest-wall lesions is, tothe best of our knowledge, not available in the literature,although scattered reports of cold abscess of the chest wall,1
tuberculous involvement of the ribs2 and sternum,3 invasionof the chest wall by bronchogenic carcinoma,4 breast car-cinoma,5 epithelial malignancies,6 chondrosarcoma,7 rib tu-mors,8 malignant small round cell tumor,9–12 desmoid tu-mors,13 and plexiform fibrohistocyte lesions14 are availablein the literature. This study is an attempt to present thecytomorphology of the plethora of chest-wall lesions.
Materials and MethodsFine-needle aspiration cytology (FNAC) was performed on227 cases of chest-wall lesions over a 4-yr period from1996–1999, in the Department of Cytology, Post GraduateInstitute of Medical Education and Research (P.G.I.M.E.R.)(Chandigarh, India). The conventional procedure of FNACwas used with a 20-ml disposable syringe for suction and a23-gauge, 1–1.5-inch-long needle. Palpable rib/sternalmasses could be punctured with the thin needle in mostinstances, with or without local anesthesia, but sometimesthicker 18- or 20-gauge needles were required. Care wastaken not to penetrate deeper tissues such as the pleura orlung. Nonpalpable lesions involving the ribs or sternumwere aspirated under the suitable radio-imaging technique.The slides were immediately wet-fixed for hematoxylin-eosin (H&E) stain/immunostaining, and air-dried smearswere used for the conventional Giemsa stain. Special stainssuch as periodic acid-Schiff (PAS), PAS-Alcian blue, orZiehl-Neelson (Z-N) for acid-fast bacilli were carried outwhen indicated. If pus was aspirated, it was sent for culturefor acid-fast bacilli. Limited immunostaining was done,using the indirect immunoperoxidase method for difficultcases. The primary antibodies used were directed againstcytokeratin, leukocyte-common antigen Mic-2, HMB-45,and smooth muscle actin (SMA), all from Dako.
ResultsThe age range of 227 patients aspirated was from 5 mon to86 yr, with a male:female ratio of 1.3:1. The variety oflesions are enumerated in Table I.
Department of Cytology, Post Graduate Institute of Medical Educationand Research (P.G.I.M.E.R.), Chandigarh, India
*Correspondence to: Dr. S.K. Gupta, Department of Cytology,P.G.I.M.E.R., Chanidgarh-160012, India. E-mail: [email protected]
Received 9 June 2000; Accepted 26 October 2000
384 Diagnostic Cytopathology, Vol 24, No 6 © 2001 WILEY-LISS, INC.
The inflammatory lesions comprised 68 of 227 cases(29.96%), the bulk of the lesions being acute/organizinginflammatory lesions (38/68). A definite etiology for theinflammation could be obtained in 30/68 cases, of whichgranulomatous inflammation was seen in 21 cases (Fig. 1),cysticercosis in 8 cases (Fig. 2), and filarasis in one case.acid-fast bacilli (AFB) positivity with Z-N stain was seen in11/21 (52.4%) cases of granulomatous inflammation.
Lipomas were the commonest benign tumors encoun-tered, accounting for 38 of 126 benign lesions. The otherlesions included epidermal inclusion cysts (8), spindle-celllesions (6), benign chondromas (3), benign adnexal tumors(2), and hematoma (1).
Inconclusive aspirates were obtained in 16/27 (7.05%)cases. The material aspirated consisted of blood, fat, skeletalmuscle, and/or stromal fragments. The clinical diagnosisoffered in these cases included cold abscess (1), costochon-dritis (1), adnexal tumor (1), arterio-venous (A-V) malfor-mation (1), hematoma (1), cystic mass, possibly malignantfibrous histiocytoma or malignant teratoma (1), neuroblas-toma (1), multiple myeloma with lytic lesion in the sixth rib(1), metastasis from carcinoma of the breast (2), metastasisfrom squamous-cell carcinoma of the lung (1), and noclinical diagnosis in the remaining few cases.
Malignant tumors comprised 36.13% of all cases (81/27),the commonest being metastatic carcinomas (57/81 cases).Poorly differentiated carcinomas (13/57) were comprised ofepithelial cells with moderately to markedly pleomorphicnuclei with high nuclear/cytoplasmic ratio, fine nuclearchromatin with focal clumping, and scanty to moderatecytoplasm. No gland formation, moulding, or squamousdifferentiation was seen in these patients. Squamous-cellcarcinoma cases (12/57) were usually metastatic from un-derlying benign masses, as seen on chest X-ray. Only onecase was metastatic, from a known case of carcinoma cervixin a woman 50 yr old. The aspirates in most cases showeda necrotic background, with scattered malignant cells. Infil-trating duct carcinomas from an underlying breast malig-nancy occurred in 11/57 cases. The diagnosis of metastaticnonsmall-cell carcinoma was given in 9/57 cases, and ofsmall-cell anaplastic carcinoma in 3/57 cases. The small-cell anaplastic carcinoma was characterized by highly cel-lular smears of malignant epithelial cells with very highnuclear/cytoplasm ratio, fine, evenly dispersed chromatin,conspicuous nucleoli, and scanty cytoplasm. The cells were
Table I. Spectrum of 227 FNAC Cases of Chest-Wall Lesions
Nature of lesion Number
Benign 126Inflammatory 68
Acute/organizing abscess 38Tuberculosis/granulomatous 21Cysticercosis 8Filariasis 1
Lipoma 38Epidermal inclusion cysts 8Spindle-cell lesions/tumor 6Chondroma 3Benign adnexal tumor 2Hematoma 1Malignant 81
Carcinoma 57Ewing’s/malignant round-cell tumors 6NHL 2Plasma-cell tumor 4Chondrosarcoma 1Malignant melanoma 2Mixed germ-cell tumor 1Neuroendocrine tumor 1Malignant nerve-sheath tumor 1Epithelioid leiomyosarcoma 1AML infiltrate 1Malignancy, not otherwise specified 3Consistent with dermatofibroma 1
No evidence of malignancy 4Descriptive 16
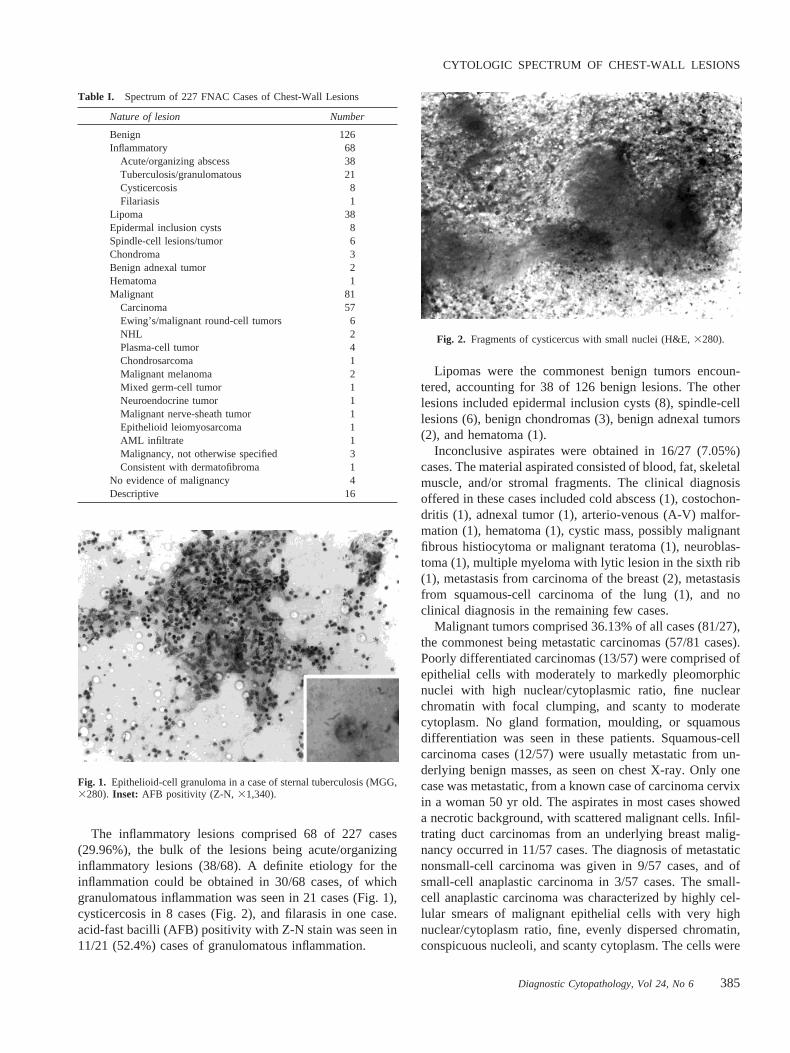
Fig. 1. Epithelioid-cell granuloma in a case of sternal tuberculosis (MGG,3280). Inset: AFB positivity (Z-N, 31,340).
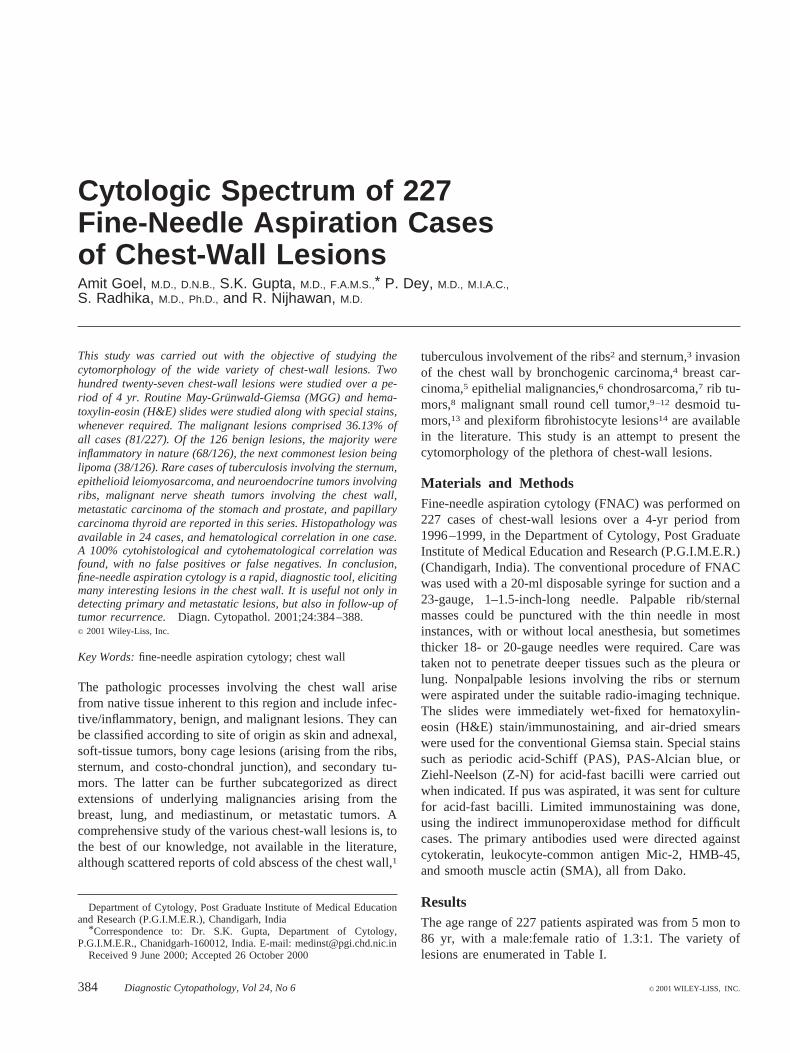
Fig. 2. Fragments of cysticercus with small nuclei (H&E,3280).
CYTOLOGIC SPECTRUM OF CHEST-WALL LESIONS
Diagnostic Cytopathology, Vol 24, No 6 385

fragile and showed nuclear moulding and streaking of nu-clear material. Adenocarcinomas comprised 6/57 cases, andshowed gland formation. Two of the adenocarcinomas wereknown cases of carcinoma of the stomach and carcinoma ofthe prostate. The other had lung shadows with a clinicaldiagnosis of possibly bronchogenic carcinoma. In two of themetastatic carcinomas, the cells were markedly pleomor-phic and showed high mitotic activity. A diagnosis of ana-plastic carcinoma was offered in these cases. One case wasa metastatic, previously biopsy-proven case of papillarycarcinoma of the thyroid (Fig. 3).
The other malignant tumors included six small round celltumors, three of which were diagnosed as Ewing’s sarcoma,based on small round cells with salt-and-pepper nuclearchromatin, and moderate amounts of bluish vacuolated cy-toplasm, which were positive with PAS stain and sensitiveto diastase. The age of these patients was on average 13 yr,the age of other small round cell tumor cases being 18–20yr. The cases of Ewing’s sarcoma were later confirmed onhistopathology and with Mic-2 immunostaining. In theother three tumors, no lymphoglandular bodies, rosette for-mation, neurofibrillary background, or rhabdoid differenti-ation was seen to ascribe them to a particular category.Immunostaining was not available in these cases.
Plasmacytomas comprised 4/57 cases, two occurring inthe sternum and two in the ribs. The other cases included achest infiltrate from a hematologically proven case of acutemyeloid leukemia (AML-1), malignant melanoma (2),mixed germ-cell tumor (1), malignant nerve sheath tumor(1), epithelioid leiomyosarcoma (1), soft-tissue tumor con-sistent with dermatofibroma (1), non-Hodgkin’s lymphoma(NHL) of the ribs (2), chondrosarcoma (1), neuroendocrinetumor (1), and malignancy not specified (3). No evidence ofmalignancy was found in four follow-up cases of carcinomaof the breast.
One interesting case of soft-tissue lesion was of a left-sided rib mass in a 55-yr-old male, the FNAC from whichshowed highly pleomorphic tumor cells and tumor giantcells with prominent nucleoli and abundant cytoplasm. Theinitial report was that of a pleomorphic high-grade malig-nant tumor, possibly carcinoma or sarcoma. Later, immu-nostaining was done and was positive for smooth muscleactin (SMA) and cytokeratin. A diagnosis of epithelioidleiomyosarcoma was given, which was confirmed onbiopsy.
The cases of malignant melanoma (Fig. 4) showed large,round to oval cells with high N/C ratio, prominent nucleoli,and cytoplasmic melanin pigment. These were positive forSchmorl’s stain and for HMB-45 immunostaining, thusconfirming the diagnosis.
The single case of chondrosarcoma presented with a leftchest-wall nodular mass measuring 4 cm diameter in a45-yr-old woman, involving the lower thoracic cage. Theaspirated material was gelatinous in consistency andshowed chondrocytes in lacunar spaces with minimal nu-clear pleomorphism, nuclear membrane irregularity, andoccasional prominent nucleoli (Fig. 5) in a chondromyxoidbackground. Occasional cells showed binucleation.
The malignant neuroendocrine tumor presented as a re-current swelling in the chest wall of 6-mo duration in apreviously biopsy proven case in a 32-yr-old male. FNACshowed a discohesive, monomorphic population of roundcells with scanty cytoplasm, most of which was stripped off,and a peripheral arrangement of spindle cells at places (Fig. 6).
Histopathology correlation was available in 24 of 81malignant tumors, and there was a perfect cytology-histopa-thology correlation of 100% (Table II). Hematological cor-relation was found in one case of acute myeloid leukaemia(AML). There were no false-positive or false-negativediagnoses.
Fig. 3. Papillae formation with nuclear overlapping in a case of metastaticpapillary carcinoma thyroid (MGG,3280).Insets:Nuclear groove (upper)and pseudoinclusion (lower) (H&E,31,340; MGG,31,340).
Fig. 4. Cells in a case of malignant melanoma with melanin pigment(H&E, 31,340).
GOEL ET AL.
386 Diagnostic Cytopathology, Vol 24, No 6

DiscussionThe native tissues inherent to this region explain the widevariety of lesions seen here. Many of the lesions aredistinctly uncommon, and some have an interestinghistogenesis.
Although tuberculosis is rampant in our country andaffects any organ and site, the ribs, sternum, and surround-ing chest wall are uncommon sites.1–3 Cold abscesses of thechest wall are rare lesions,1 and tuberculosis in this regionhas an interesting histogenesis, with a primary focus in theunderlying ribs2 or sternum,3 the latter being very uncom-mon. In our 21/227 cases of tuberculosis of the chest wall,only one case had involvement of the sternum, and in thiscase AFB was strongly positive. The presence of underlyingrib lesions cannot be commented upon, as most of the casesdid not have chest X-rays at the time of initial presentation
to the clinic, and many were lost to follow-up after startingantituberculous treatment (ATT). Six of the 21 cases, how-ever, did give a clinical history of previous treatment withATT. It is important to look for an underlying focus in theribs, as some of these cases are resistant to treatment andmay require surgical intervention.2
Lipoma is a common soft-tissue lesion occurring at thissite, as seen in our results. However, the malignant coun-terpart, i.e., liposarcoma is very rare. Other benign soft-tissue lesions which can occur here include cutaneousleiomyoma arising form pillar arrector muscles around hairfollicles, hemangioma lymphangioma, and fibrous lesionsincluding nodular fascitis and fibromatosis. The latter com-prise 17.2% of extraabdominal fibromatosis at this site.15
Chest-wall desmoids account for approximately 20% of allpatients with desmoid tumors.13 We had six cases of benignspindle-cell lesions involving the chest wall, but with nospecific features to categorize them as leiomyomas or be-nign fibrous lesions. There are case reports of malignantfibrous histiocytoma of the chest wall.7,14 One of our caseswas diagnosed as a soft-tissue tumor, possibly dermatofi-broma, and one as a malignant nerve sheath tumor. There isno mention in the literature, to the best of our knowledge, ofa nerve sheath tumor involving the chest wall, but as nervesare an intrinsic part of any site of the body, there is noreason why it cannot occur here.
The available literature mentions invasion of the chestwall by underlying bronchogenic carcinoma4 and breastcarcinoma,4,6 and by various other epithelial malignanciessuch as colonic, ovarian, rectal, endometrial, cervical, andesophageal carcinomas.6 Most of our cases were also ex-tensions from underlying lung and breast carcinomas, ex-cept in four cases, of which one each was of metastaticcarcinoma of the cervix, papillary carcinoma of the thyroid,carcinoma of the stomach, and prostatic carcinoma. Thechest wall is not mentioned as a metastatic site for thesemalignancies and this, to the best of our knowledge, is thefirst report mentioning it. Cutaneous/subcutaneous metasta-
Fig. 5. Cells in lacunae in a chondroid background with mild nuclearanisonucleosis, in a case of well-differentiated chondrosarcoma (H&E,3550).
Fig. 6. Monomorphic population of round to oval cells with scanty cyto-plasn, in a biopsy-proven case of neuroendocrine tumor (MGG,3550).
Table II. Twenty-Five Cases With Cytohistological andCytohematological Correlation
Diagnosis Number of cases
Cytohistological correlation 24Infiltrating duct carcinoma (breast) 11Metastatic carcinoma of the stomach 1Metastatic carcinoma of the cervix 1Metastatic carcinoma of the prostate 1Metastatic papillary carcinoma of the thyroid 1Metastatic neuroendocrine tumor 1Plasmacytoma/multiple myeloma 3Ewing’s/PNET 3Chondrosarcoma 1Epithelioid leiomyosarcoma 1
Cytohematological correlation 1AML infiltrate 1
CYTOLOGIC SPECTRUM OF CHEST-WALL LESIONS
Diagnostic Cytopathology, Vol 24, No 6 387

ses from carcinomas are rare and are indicative of a badprognosis. They may be the initial presentation of an un-known/unsuspected primary, and FNAC helps in the rapid,early detection of these cases.
In 1979, Askin and Rosai described the unique clinico-pathological entity of Askin’s tumor (or primitive neuroec-todermal tumor), a rare tumor of the chest wall.16 The tumorarises in the periosteum, soft tissue, or extrapulmonaryfields of the thoracic wall and in the lung, with or withoutrib involvement. The entity embraces the Ewing’s-primitiveneuroectodermal tumor (PNET) group of the chest wall.10
An estimated 6.5% of primary Ewing’s sarcomas arise inthe chest wall.17 The precise histogenesis of this entity isunknown, but a derivation from a primitive pluripotent cellexpressing a neuroectodermal phenotype was proposed.18
Rosette-like structures may be seen in 45% of these tu-mors.9 All three cases diagnosed as Ewing’s sarcoma in thisseries had rib involvement. The other three unclassifiedmalignant small round cell tumors did not show any specificfeatures of lymphoma, neuroblastoma, rhabdomyosarcoma,or the Ewing’s-PNET group, as mentioned in our results.Immunohistochemistry using desmin, neuroblastoma geneproduct, and Mic-2 may further resolve the issue. Limitedimmunostaining was available in this study. Immunopheno-typing may be restored to in difficult cases.
Malignant bone tumors constitute only 0.2% of all tu-mors.7 Malignant bone tumors of the chest wall and sternumare even rarer, as most bone tumors occur in the long bones.Chondrosarcoma is the commonest bony, malignant chest-wall lesion,7 others being Ewing’s, osteosarcoma, malignantfibrous histiocytoma (MFH), solitary plasmacytoma, andAskin’s tumor. We found only one case of chondrosarcomainvolving the ribs, four cases of plasma-cell tumor (twoinvolving the ribs and two the sternum), and two cases ofhigh-grade non-Hodgkin’s lymphoma (NHL) involving theribs. Metastatic carcinomas to the ribs are mentioned in theliterature.8 We had three cases of carcinoma metastatic tothe ribs, and three to the sternum. Cases of epithelioidleiomyosarcoma and neuroendocrine tumors involving theribs, as diagnosed in this series, are not mentioned in theliterature.
In 16 cases, FNAC was inconclusive in obtaining a di-agnosis; two cases were radiologically cystic lesions, andone each had a diagnosis of hemangioma and hematoma.The limited role of FNAC in cystic lesions and hemangiomais well-known. In other cases, FNAC may be inconclusivedue to surrounding fibrosis or deep-seated lesions whichwere missed by blind FNAC. In the present era, theseinconclusive cases may also be decreased by performingFNAC under radiological guidance in difficult cases.
In this series, we reported on rare cases of tuberculosisinvolving the sternum, epithelioid leiomyosarcoma and neu-roendocrine tumors involving the ribs, malignant nervesheath tumors involving the chest wall, and metastatic pap-
illary carcinoma thyroid, carcinoma of the stomach, andprostatic carcinoma to the chest wall.
In conclusion, FNAC of chest wall lesions plays animportant role in rapidly confirming the diagnosis and pre-vents surgical intervention in the majority of cases, asevidenced by the limited histopathology done in our series.It is an invaluable tool in detecting metastases from knownand unknown primaries, and in follow-up of tumorrecurrence.
References1. Faure E, Souilamas R, Riquet M, Chehab A, Le Pimpec-Barthes F,
Manac’h D, Debesse B. Cold abscess of the chest wall: a surgicalentity? Ann Thorac Surg 1998;66:1174–1178.
2. Chang JH, Kim SK, Lee WY. Diagnostic issues in tuberculosis of theribs with a review of 12 surgically proven cases. Respirology 1999;4:249–253.
3. Karnak I, Akcoren Z, Gogus S, Caglar M, Tanyel FC. Granulomatousosteomyelitis of the sternum presenting with a parasternal mass: apossible relation to the bacillus Calmette-Guerin vaccine. J PediatrSurg 1999;34:1534–1536.
4. Pairolero PC. Extended resections for lung cancer. How far is too far?Eur J Cardiothorac Surg 1999;1:48–50.
5. Seyfer AE. Breast cancer invasion into the chest wall with resectionand reconstruction. Semin Thorac Cardiovasc Surg 1999;11:285–292.
6. Gupta RK, Naran S. Fine needle aspiration cytology of cutaneous andsubcutaneous metastatic deposits from epithelial malignancies. Ananalysis of 146 cases. Acta Cytol 1999;43:126–130.
7. Liptay MJ, Fry WA. Malignant bone tumors of the chest wall. SeminThorac Cardiovasc Surg 1999;11:278–284.
8. Andrianopoulos EG, Lautidis G, Kormas P, Karameris A, Lahanis S,Papachristos I, Kaselouris C, Argyropoulos A. Tumors of the ribs:experience with 47 cases. Eur J Cardiothorac Surg 1999;15:615–620.
9. Contesso G, Llombart-Bosch A, Terrier P, et al. Does malignant smallround cell tumor of the thoracopulmonary region (Askin tumor) con-stitute a clinicopathologic entity? An analysis of 30 cases with immu-nohistochemical and electron-microscopic support treated at the Insti-tute Gustave Roussy. Cancer 1992;69:1012–1020.
10. Shamberger RC, Tarbell NJ, Perez-Atayde AR, Grier HE. Malignantsmall round cell tumor (Ewing’s-PNET) of the chest wall in children.J Pediatr Surg 1994;29:179–185.
11. Promnitz S, Petri F, Schulz HJ, Gellert K. Askin’s tumor—a rareentity. Case report with references to the literature. Pneumologie1999;53:393–399.
12. Sallustio G, Pirronti T, Lasorella A, Natale L, Bray A, Marano P.Diagnostic imaging of primitive neuroectodermal tumour of the chestwall (Askin tumour). Pediatr Radiol 1998;28:697–702.
13. Allen PJ, Shriver CD. Desmoid tumors of the chest wall. SeminThorac Cardiovasc Surg 1999;11:264–269.
14. Redlich G, Bocklage T, Joste N. Fine needle aspiration cytology ofplexiform fibrohistiocytic tumor. A case report. Acta Cytol 1999;43:867–872.
15. Enzinger FM, Weiss SW. Fibromatoses. In: Gay SM, editor. Softtissue tumors, 3rd ed. St. Louis, Toronto, London: C.V. Mosby Co.;1995. p 201–230.
16. Askin FB, Rosai J, Sibley RK, Dehner LP, McAlister WH. Malignantsmall cell tumor of the thoracopulmonary region in childhood. Adistinctive clinicopathologic entity of uncertain histogenesis. Cancer1979;43:2438–2451.
17. Thomas PRM, Foulkes MA, Gilula LA, et al. Primary Ewing’s sar-coma of the ribs: a report from the Intergroup Ewing’s Sarcoma Study.Cancer 1983;51:1021–1027.
18. Fujii Y, Hongo T, Nakagawa Y, et al. Cell culture of small round celltumor originating in the thoracopulmonary region: evidence for deri-vation from a primitive pluripotent cell. Cancer 1989;64:43–51.
GOEL ET AL.
388 Diagnostic Cytopathology, Vol 24, No 6