Cystic Fibrosis: A Disease for a Multidisciplinary Team Kim Otsuka, MD Pediatric Pulmonary Fellow...
51
Cystic Fibrosis: A Cystic Fibrosis: A Disease for a Disease for a Multidisciplinary Multidisciplinary Team Team Kim Otsuka, MD Kim Otsuka, MD Pediatric Pulmonary Pediatric Pulmonary Fellow Fellow September 21, 2004 September 21, 2004 UoA PPC 2004 Workshop UoA PPC 2004 Workshop Lectures Lectures
-
date post
22-Dec-2015 -
Category
Documents
-
view
215 -
download
2
Transcript of Cystic Fibrosis: A Disease for a Multidisciplinary Team Kim Otsuka, MD Pediatric Pulmonary Fellow...

Cystic Fibrosis: A Cystic Fibrosis: A Disease for aDisease for a
Multidisciplinary Multidisciplinary TeamTeam
Kim Otsuka, MDKim Otsuka, MD
Pediatric Pulmonary FellowPediatric Pulmonary Fellow
September 21, 2004September 21, 2004
UoA PPC 2004 Workshop UoA PPC 2004 Workshop LecturesLectures

ObjectivesObjectives
Brief overview of cystic fibrosis (CF) Brief overview of cystic fibrosis (CF) Review some of the “newer” Review some of the “newer”
pulmonary therapies in CFpulmonary therapies in CF Highlight nutritional issues in CFHighlight nutritional issues in CF Highlight psychosocial issues in CFHighlight psychosocial issues in CF Highlight respiratory care issues in Highlight respiratory care issues in
CFCF
CF Center TeamCF Center Team
Center directorCenter director Associate center directorAssociate center director Clinic coordinatorClinic coordinator Social workerSocial worker Respiratory therapistRespiratory therapist NurseNurse Registered dietitianRegistered dietitian

Cystic Fibrosis - A recapCystic Fibrosis - A recap
EpidemiologyEpidemiology Most common life-threatening inherited Most common life-threatening inherited
diseasedisease Autosomal recessiveAutosomal recessive Incidence 1:3200 live births Incidence 1:3200 live births
(Caucasians)*(Caucasians)* Hispanics 1:9200, Blacks 1:15,000, Asians Hispanics 1:9200, Blacks 1:15,000, Asians
1:31,0001:31,000 1:28 Caucasians are carriers1:28 Caucasians are carriers
Hispanics 1:48, Blacks 1:61; Asians 1:88Hispanics 1:48, Blacks 1:61; Asians 1:88
*Adapted from Hamosh A, et al. J Pediatr 1998; 132: 255-259

GeneticsGenetics
Single gene defect Single gene defect on chromosome 7on chromosome 7 Dicovered in 1989Dicovered in 1989 Cystic fibrosis Cystic fibrosis
transmembrane transmembrane regulator (CFTR)regulator (CFTR)
Most common Most common F508F508
Over 1000 Over 1000 mutations mutations identifiedidentified
Zeitlin P, N Engl J Med 2004; 351: 606-8.

PathophysiologyPathophysiology
CFTR mutations affect epithelial CFTR mutations affect epithelial cells, thus affecting:cells, thus affecting: Airways (sinuses, lungs)Airways (sinuses, lungs) Pancreas (endocrine and exocrine)Pancreas (endocrine and exocrine) GI tract (liver/biliary system, intestines)GI tract (liver/biliary system, intestines) Reproductive organsReproductive organs SkinSkin
Pulmonary Pulmonary PathophysiologyPathophysiology
2 theories2 theories Composition hypothesisComposition hypothesis
Airway epithelia regulate the airway surface Airway epithelia regulate the airway surface liquid (ASL) salt content that is important liquid (ASL) salt content that is important for lung defensefor lung defense
Volume hypothesisVolume hypothesis Airway epithelia regulate the volume of Airway epithelia regulate the volume of
liquid in the mucus and periciliary liquid liquid in the mucus and periciliary liquid layers of ASL for efficient ciliary mucus layers of ASL for efficient ciliary mucus interactions and airway clearance. interactions and airway clearance.

Pulmonary - Pulmonary - PathophysiologyPathophysiology
Ratjen F, Coring G. Lancet 2003; 361: 681-89.

Pulmonary Pulmonary PathophysiologyPathophysiology
CFTR mutation --> abnormal airway CFTR mutation --> abnormal airway surface microenvironment --> surface microenvironment --> thickened mucus, chronic infection, thickened mucus, chronic infection, chronic inflammation --> damages chronic inflammation --> damages airway ---> bronchiectasis, airway ---> bronchiectasis, respiratory failure and often deathrespiratory failure and often death

Inflammation in CFInflammation in CF
Konstan MW, Davis PB. Advanced Drug Delivery Reviews 2002; 54: 1409-1423

Treatment: Anti-Treatment: Anti-inflammatoriesinflammatories
IbuprofenIbuprofen Konstan et al, Konstan et al,
NEJM 1995NEJM 1995 85 patients85 patients
5 - 39 y/o5 - 39 y/o FEV1 FEV1 >> 60 % 60 %
predictedpredicted 20-30 mg/kg of 20-30 mg/kg of
ibuprofenibuprofen peak plasma peak plasma
concentrations 50-concentrations 50-100 mcg/mL100 mcg/mL
ResultsResults FEV1FEV1
-2.17 -2.17 ++ 0.57 vs. - 0.57 vs. -3.60 3.60 ++ 0.55 0.55 (p=0.02)(p=0.02)
weight better in weight better in ibuprofen group ibuprofen group (p=0.02)(p=0.02)
Adverse eventsAdverse events No difference No difference
between groups in between groups in studystudy
Increased GI Increased GI hemorrhage in f/uhemorrhage in f/u
Treatment: Anti-Treatment: Anti-inflammatoriesinflammatories
AzithromycinAzithromycin Multicenter US trialMulticenter US trial double-blind, double-blind,
randomized, placebo-randomized, placebo-controlled trialcontrolled trial
185 patients, >6 y/o185 patients, >6 y/o FEV1 >30% FEV1 >30%
predictedpredicted weight <40 kg: 250 weight <40 kg: 250
mg azithromycin mg azithromycin 3x/wk3x/wk
weight >40 kg: 500 weight >40 kg: 500 mg azithromycin mg azithromycin 3x/wk3x/wk
ResultsResults At 24 weeks into At 24 weeks into
studystudy FEV1 gain 4.77% FEV1 gain 4.77%
in azithromycin in azithromycin groupgroup
FEV1 loss -1.77% FEV1 loss -1.77% in placeboin placebo
Improved weight Improved weight gain and decreased gain and decreased hospitalizations in hospitalizations in azithromycin groupazithromycin group
Adverse events: Adverse events: nausea, diarrhea, nausea, diarrhea, wheezingwheezing

MucolyticsMucolytics
King M, Rubin BK. Advanced Drug Delivery Review 2002; 54: 1475-90

PulmozymePulmozyme®®
Dornase alfaDornase alfa Fuchs, et al 1994Fuchs, et al 1994 968 patients 968 patients
(youngest 5 y/o)(youngest 5 y/o) Randomized, double-Randomized, double-
blinded placebo blinded placebo controlled trialcontrolled trial
placebo vs. once or placebo vs. once or twice daily DNAsetwice daily DNAse
ResultsResults Improved QOL, Improved QOL,
health economicshealth economics
Pulmonary Pulmonary exacerbationsexacerbations once daily: RR 0.78 once daily: RR 0.78
(CI 0.57-1.06; p=0.11)(CI 0.57-1.06; p=0.11) twice daily: RR = 0.66twice daily: RR = 0.66 (CI 0.48-0.91; p=0.01)(CI 0.48-0.91; p=0.01)
FEV1 FEV1 (improved (improved p<0.01)p<0.01) once daily 5.8 once daily 5.8 ++ 0.7 0.7 twice daily 5.7 twice daily 5.7 ++ 0.7 0.7
Adverse eventsAdverse events Voice alteration, Voice alteration,
laryngitis, rashlaryngitis, rash
AntibioticsAntibiotics
Often unable to eradicate the Often unable to eradicate the organismorganism
Determining optimal delivery mode Determining optimal delivery mode for a drug is difficultfor a drug is difficult
CF patients require higher dosesCF patients require higher doses Altered volume of distributionAltered volume of distribution Rapid clearance of drugsRapid clearance of drugs
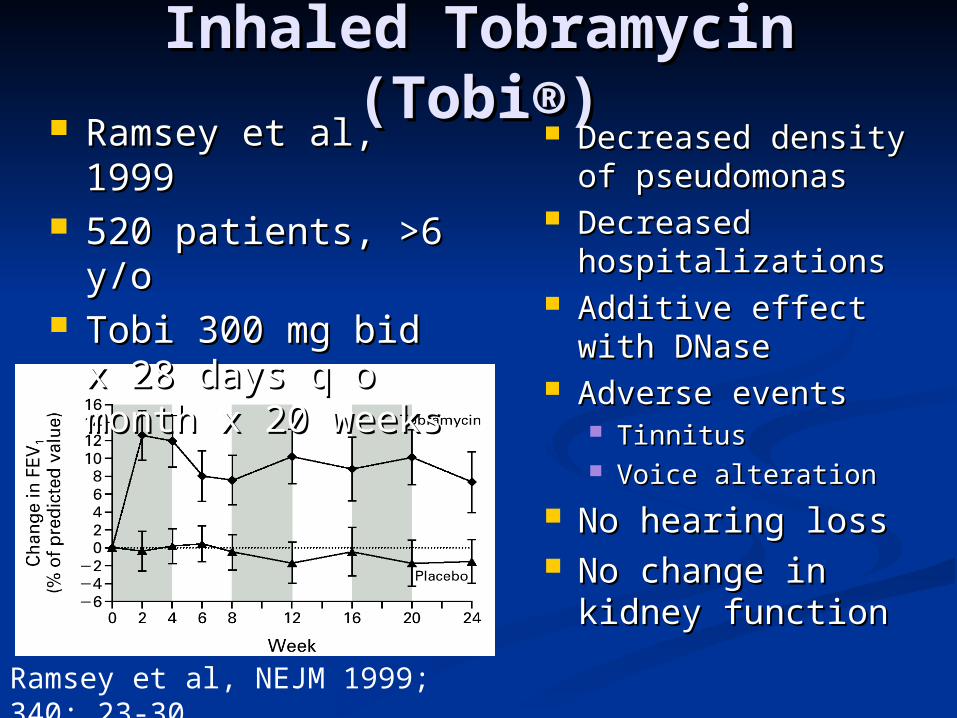
Inhaled Tobramycin Inhaled Tobramycin (Tobi®)(Tobi®)
Decreased density Decreased density of pseudomonasof pseudomonas
Decreased Decreased hospitalizationshospitalizations
Additive effect Additive effect with DNasewith DNase
Adverse eventsAdverse events Tinnitus Tinnitus Voice alterationVoice alteration
No hearing lossNo hearing loss No change in No change in
kidney functionkidney functionRamsey et al, NEJM 1999; 340: 23-30
Ramsey et al, Ramsey et al, 19991999
520 patients, >6 520 patients, >6 y/oy/o
Tobi 300 mg bid x Tobi 300 mg bid x 28 days q o month 28 days q o month x 20 weeksx 20 weeks
Nutritional Nutritional IssuesIssues

Nutritional IssuesNutritional Issues
Nutrition is closely tied to overall Nutrition is closely tied to overall healthhealth
Malnutrition in CF associated withMalnutrition in CF associated with Stunted growthStunted growth Pubertal delayPubertal delay Deterioration of lung functionDeterioration of lung function Early deathEarly death

ESCF StudyESCF Study J. Pediatrics 2003J. Pediatrics 2003 931 patients931 patients 3-6 years3-6 years Parameters evaluated:Parameters evaluated:
Height, weight, s/sx of lung disease Height, weight, s/sx of lung disease recorded at age 3 and 6recorded at age 3 and 6
Respiratory tract culture Respiratory tract culture << 3 y/o 3 y/o 1 valid spirometry obtained when 1 valid spirometry obtained when
stable between 5.5 and 7.5 y/ostable between 5.5 and 7.5 y/o

Results - age 3Results - age 3
Konstan MW, J. Pediatr 2003; 142:624-30

Results - age 6Results - age 6
Konstan MW, J. Pediatr 2003; 142:624-30
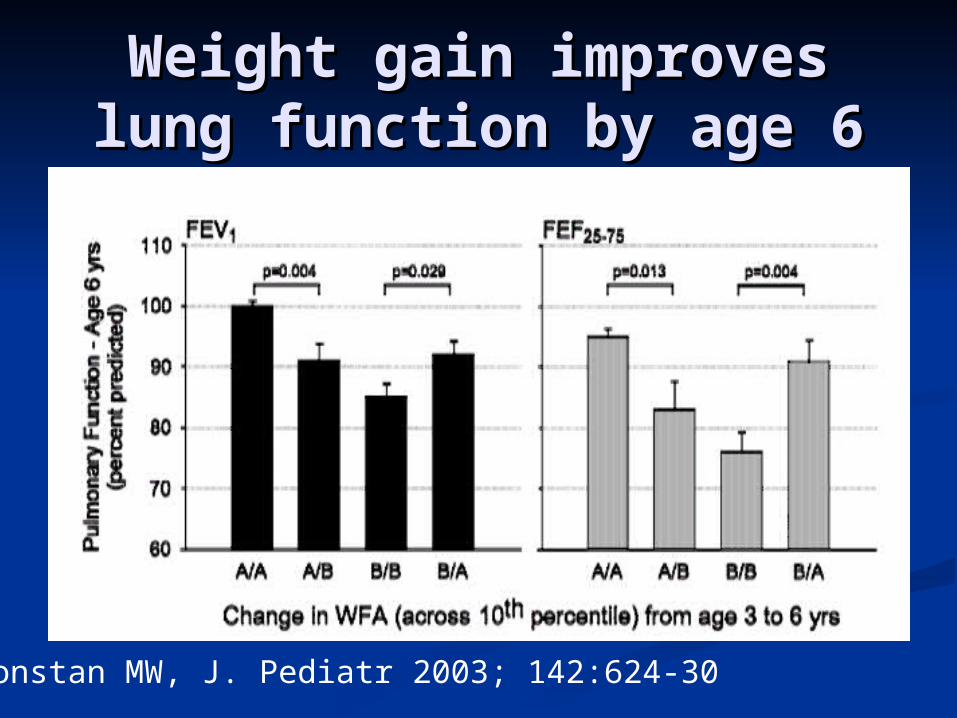
Weight gain improves Weight gain improves lung function by age 6lung function by age 6
Konstan MW, J. Pediatr 2003; 142:624-30
ConclusionsConclusions
Indexes of growth and nutrition at age 3 Indexes of growth and nutrition at age 3 associated with lower pulmonary function associated with lower pulmonary function at age 6at age 6
S/sx of lung disease at age 3 are also S/sx of lung disease at age 3 are also associated with lower pulmonary function associated with lower pulmonary function at age 6at age 6
Relative weight loss was associated with Relative weight loss was associated with worse lung functionworse lung function
Relative weight gain was associated with Relative weight gain was associated with improved lung functionimproved lung function
Care team Care team responsibilitiesresponsibilities
Monitor growthMonitor growth Provide anticipatory counseling and Provide anticipatory counseling and
plan interventional strategies for those plan interventional strategies for those who are undernourished or are at high who are undernourished or are at high riskrisk
DietitianDietitian Provides discipline-specific expertise Provides discipline-specific expertise
needed for optimal nutritional managementneeded for optimal nutritional management Provide expertise concerning Provide expertise concerning
developmental and behavioral aspects of developmental and behavioral aspects of eatingeating
Nutritional managementNutritional management
Growth and nutritional status Growth and nutritional status monitored every 3 monthsmonitored every 3 months
Annual pubertal assessmentAnnual pubertal assessment Especially important times for Especially important times for
monitoringmonitoring First 12 months after diagnosisFirst 12 months after diagnosis Birth to 12 months for those diagnosed Birth to 12 months for those diagnosed
prenatally or by GDS prenatally or by GDS Peripubertal growth periodPeripubertal growth period

Pancreatic InsufficiencyPancreatic Insufficiency
85-90% affected85-90% affected Malabsorption Malabsorption
fats, protein, and fats, protein, and other nutrientsother nutrients
Diagnostic testsDiagnostic tests 72 hour fecal fat72 hour fecal fat fecal elastase-1fecal elastase-1
PS patient re-PS patient re-evaluated annuallyevaluated annually
TreatmentTreatment Pancreatic enzyme Pancreatic enzyme
supplementationsupplementation Improved release Improved release
with H2 blocker or with H2 blocker or PPIPPI
Proprietary enzymes Proprietary enzymes better than genericbetter than generic
Complication: Complication: fibrosing colonopathyfibrosing colonopathy
Taurine Taurine supplementationsupplementation
CurcuminCurcumin
Calorie intakeCalorie intake
Greater than RDA for those without Greater than RDA for those without CFCF Weight goal is 100-110% IBWWeight goal is 100-110% IBW
Fat intake 35-40%Fat intake 35-40% Protein 15-20%Protein 15-20% SupplementsSupplements
Oral: controversialOral: controversial EnteralEnteral

The VitaminsThe Vitamins Vitamin AVitamin A
15-40% deficient15-40% deficient 18% adults deficits 18% adults deficits
in dark field in dark field adaptationadaptation
Negative acute Negative acute phase reactant (do phase reactant (do not draw with not draw with acute illness)acute illness)
Vitamin DVitamin D 10-40% deficient10-40% deficient
Vitamin EVitamin E 5-10% deficient5-10% deficient
Vitamin KVitamin K PIVKA-II vs. PTPIVKA-II vs. PT
Essential Fatty Essential Fatty AcidsAcids
Minerals and Minerals and ElectrolytesElectrolytes CalciumCalcium IronIron ZincZinc SodiumSodium
Bone monitoringBone monitoring Children > 8 y/o Children > 8 y/o
with risk factorswith risk factors Post-organ Post-organ
transplanttransplant End-stage lung End-stage lung
diseasedisease Bone fracture with Bone fracture with
low-impact activitylow-impact activity Chronic Chronic
corticosteroid usecorticosteroid use Delayed pubertal Delayed pubertal
developmentdevelopment Nutritional failureNutritional failure
ScreeningScreening DEXA lumbar spineDEXA lumbar spine Annual serum Annual serum
calcium, calcium, phosphorous, intact phosphorous, intact PTH, 25-hydroxy vit DPTH, 25-hydroxy vit D
Dietary assessment of Dietary assessment of calcium and vit Dcalcium and vit D
TreatmentTreatment Optimize nutrition Optimize nutrition
and intake of vit D, and intake of vit D, K, calciumK, calcium
Weight bearing Weight bearing physical activityphysical activity

Cystic Fibrosis Related Cystic Fibrosis Related DiabetesDiabetes
Leading comorbidity associated with CFLeading comorbidity associated with CF Prevalence increased by 173% from 1992-Prevalence increased by 173% from 1992-
20022002 Prevalence increases with agePrevalence increases with age
3-12% are reported to have diabetes3-12% are reported to have diabetes 14% of CF patients >14 years old14% of CF patients >14 years old 25% of CF patients 35-44 years old25% of CF patients 35-44 years old
Average age of onset 18-21 y/oAverage age of onset 18-21 y/o Females > MalesFemales > Males

Moran, et al. J. Pediatrics. 133(1998)
Glucose Intolerance Increases Glucose Intolerance Increases with Agewith Age

SurvivalSurvival
Finnkelstein et al. . J Pediatr 1988; 112: 373-7
Analysis of survival at University of Minnesota has demonstrated that the rapid decline in survival can be attributed to females with CFRD since males with CFRD has ~equivalent suvival rates to males without CFRD

Milla CE et al: Am J Resp Crit Care Med 162:891-5, 2000
Rate of Decline in Pulmonary Function is Related to Oral Glucose Tolerance Status

Comparison of CFRD Comparison of CFRD with type 1 and type 2 with type 1 and type 2
DMDM Type 1 Type 2 CFRD Insulin secretion Absent Insulin sensitivity
Autoimmunity Yes No No
Age <20 >40 18-21
Body habitus Normal Obese Slender
Ketoacidosis Yes Rare Rare
Microvascular Yes Yes Yes
Macrovascular Yes Yes No?
Moran T: Mountain West Consortium June 24, 2004

Therapy - CFRDTherapy - CFRD
Treatment: insulinTreatment: insulin Control glucose to avoid acute/chronic Control glucose to avoid acute/chronic
complicationscomplications FPG 80-120 mg/dlFPG 80-120 mg/dl Post-prandial FSBS with Post-prandial FSBS with ++ 30 mg/dl 30 mg/dl
from pre-meal valuefrom pre-meal value HgA1c HgA1c << 7% 7%
Maintain optimal nutritional status and Maintain optimal nutritional status and growthgrowth Continue high energy intakeContinue high energy intake
Respiratory Care Respiratory Care IssuesIssues

Pulmonary Function Pulmonary Function TestsTests
SpirometrySpirometry Respiratory rateRespiratory rate Pulse oximetryPulse oximetry Lung volumeLung volume Exercise studiesExercise studies

Aerosol Delivery SystemsAerosol Delivery Systems
They are not all They are not all equalequal
2 important 2 important considerationsconsiderations VolumeVolume Concentration of Concentration of
therapeutic agenttherapeutic agent

Airway ClearanceAirway Clearance
Standard daily therapy for patients Standard daily therapy for patients with cystic fibrosiswith cystic fibrosis
CF --> viscous airway secretions + CF --> viscous airway secretions + poor clearance --> airway poor clearance --> airway obstruction and infection --> airway obstruction and infection --> airway injury, fibrosis --> bronchiectasisinjury, fibrosis --> bronchiectasis
Goal: enhance clearance of airway Goal: enhance clearance of airway secretionssecretions

Airway ClearanceAirway Clearance
Wagener JS, Headley AA. Respir Care 2003; 48: 234-45

Airway ClearanceAirway Clearance
Chest physiotherapyChest physiotherapy Accepted standardAccepted standard Goal move peripheral Goal move peripheral
mucus into central mucus into central airwaysairways
Active cycle Active cycle breathingbreathing
Autogenic drainageAutogenic drainage PEP and flutterPEP and flutter
low, high pressurelow, high pressure oscillatingoscillating
Intrapulmonary Intrapulmonary percussive percussive ventilationventilation
High-Frequency High-Frequency Chest CompressionChest Compression Shears mucus away Shears mucus away
from airwaysfrom airways Modifies viscoelastic Modifies viscoelastic
properties of mucusproperties of mucus ExerciseExercise

Typical Day Airway Typical Day Airway Clearance/AerosolsClearance/Aerosols
Albuterol 2x/day (15-20 minutes Albuterol 2x/day (15-20 minutes each)each)
Dnase 1x/day (15-20 minutes)Dnase 1x/day (15-20 minutes) Inhaled tobramycin 2x/day (15-20 Inhaled tobramycin 2x/day (15-20
minutes)minutes) Chest clearance 2x/day (20-30 Chest clearance 2x/day (20-30
minutes)minutes) Step up to 3-4x/day will illnessesStep up to 3-4x/day will illnesses

Psychosocial Psychosocial IssuesIssues
Social IssuesSocial Issues Address social concerns every 3 Address social concerns every 3
monthsmonths Complete assessment by an MSW or Complete assessment by an MSW or
psychologist should be performed psychologist should be performed annually includingannually including Changes in family structure and copingChanges in family structure and coping School and work performanceSchool and work performance Participation in age appropriate activitiesParticipation in age appropriate activities Developmental and emotional issuesDevelopmental and emotional issues Vocational training and preparation for Vocational training and preparation for
adult lifeadult life

Social IssuesSocial Issues
OtherOther Concerns about CF patient care and Concerns about CF patient care and
understanding of disease manifestations understanding of disease manifestations and treatmentand treatment
Compliance with treatment regimensCompliance with treatment regimens Financial issues related to the illnessFinancial issues related to the illness Family planning when reaching Family planning when reaching
reproductive agereproductive age

Psychosocial AspectsPsychosocial Aspects
WHO definition of healthWHO definition of health““A State of complete physical, mental, A State of complete physical, mental,
and social well being and not merely and social well being and not merely the absence of disease or infirmity”the absence of disease or infirmity”
Health related quality of life Health related quality of life (HRQOL)(HRQOL) Physical healthPhysical health Mental healthMental health Social functionSocial function Role functionRole function General health perceptionsGeneral health perceptions
Psychosocial AspectsPsychosocial Aspects Overall Overall
psychosocial psychosocial function is goodfunction is good
Problem areasProblem areas Exacerbations - neg Exacerbations - neg
impact on general impact on general and physical healthand physical health
Increased Increased vulnerability to vulnerability to stress of lifestress of life
More dysfunction More dysfunction seen in families seen in families with older patientswith older patients
Lower PFT’s had a Lower PFT’s had a greater impact on greater impact on the parents than the parents than the patientsthe patients
Patients >12 years Patients >12 years increased distress increased distress with hospitalizationwith hospitalization
Compliance of Compliance of treatment regimens treatment regimens improved in mother improved in mother with less frequent with less frequent social contacts and social contacts and less satisfactory less satisfactory marital marital relationshipsrelationships

Psychosocial AspectsPsychosocial Aspects
Intellectual function distributed Intellectual function distributed normallynormally
Inversely related to ageInversely related to age Academic function distributed normallyAcademic function distributed normally
No changes with ageNo changes with age Lower levels of academic and intellectual Lower levels of academic and intellectual
functioning in lower SES classesfunctioning in lower SES classes Age and SES account for 21% and 43% Age and SES account for 21% and 43%
of variance in level of functioningof variance in level of functioning
Risk BehaviorsRisk Behaviors
Cystic fibrosis patients vs. age-Cystic fibrosis patients vs. age-matched adolescent peersmatched adolescent peers Alcohol use 45.5% vs. 63.1% Alcohol use 45.5% vs. 63.1% Cigarettes 21.1% vs 53.3% Cigarettes 21.1% vs 53.3% Marijuana use 9.7% vs 29.4%Marijuana use 9.7% vs 29.4% Cocaine and other injectable drugs Cocaine and other injectable drugs
2.6% vs. 5.7%2.6% vs. 5.7%

Risk BehaviorsRisk Behaviors
H/O sexually activity 28.3% vs. H/O sexually activity 28.3% vs. 46.4%46.4% No difference in risky sexual behaviors: No difference in risky sexual behaviors:
condom use, no contraception, and condom use, no contraception, and pregnancypregnancy
Tendency for improved health Tendency for improved health promoting behaviorspromoting behaviors Seat belt use, bicycle helmetsSeat belt use, bicycle helmets
Take Home PointsTake Home Points
CF management requires the CF management requires the coordinated efforts of a CF care coordinated efforts of a CF care teamteam
Growth and nutrition is critical for Growth and nutrition is critical for pulmonary healthpulmonary health ““Breakfast is as important as morning Breakfast is as important as morning
CPT”CPT” All adolescents need risk behavior All adolescents need risk behavior
assessmentsassessments