Cyclosporine and the renin-angiotensin axis · 2017. 1. 11. · gave no family history for renal...
13
Kidney International, Vol. 52 (1997), pp. 248—260 NEPHROLOGY FORUM Cyclosporine and the renin-angiotensin axis Principal discussant: DAVID B.N. LEE Sepulveda Veterans Affairs Medical Center, and University of California, Los Angeles, California, USA Editors JORDAN J. COHEN JOHN T. HARRINGTON NICOLAOS E. MADIAS Managing Editor CHERYL J. ZUSMAN Tufts University School of Medicine CASE PRESENTATION Patient 1. A 58-year-old man was hospitalized with hypertension, 168/114 mm Hg, congestive heart failure secondary to fluid retention, and a serum creatinine of 6.9 mgldl. Six years earlier he had received a cardiac transplant for end-stage idiopathic cardiomyopathy and was given cyclo- sporine (CsA). Prior to transplantation he was normotensive (blood pressure, 100/70 mm Hg) and had a serum creatinine concentration of 3.6 mg/dl, which was attributed to his refractory biventricular heart failure. He gave no family history for renal disease or high blood pressure. The serum creatinine decreased to 0.8 mg/dl one month after cardiac transplantation and fluctuated between 1 to 2 mg/dl for about four years before beginning an inexorably upward course. His blood pressure rose rapidly after transplantation, reaching 160/120 mm Hg by the second month. Four months before this admission, he had been evaluated for rapid deterioration in renal function and refractory hypertension; his blood pressure reached as high as 180/140 mm Hg. A percutaneous renal biopsy was obtained. An endomyocardial biopsy at the same time revealed no evidence of rejection. During this admission, acute dialysis was initiated, and thc patient's congestive heart failure improved markedly following a 10-liter fluid removal. He subsequently was maintained on chronic dialysis with continued good cardiac graft function. Patient 2. A 6-year-old girl first developed steroid-dependent nephrotic syndrome at age 26 months. A renal biopsy at 33 months showed minimal-change disease and normal juxtaglomerular apparatus (JGA, Fig. 1A). A chlorambucil-induced remission of eight weeks was followed by a relapse two months after the drug was discontinued. Her nephrotic syndrome became resistant to oral corticosteroid administration, respond- ing only to intravenous methyiprednisolone. yclosporine (10—12 mg/kg/day), given in divided doses at eight-hour Key words: cyclosporine, renin-angiotensin system, hypertension. The Nephrology Forum is funded in part by grants from Hoechst Marion Roussel, Incorporated; Amgen, Incorporated; Merck & Co., Incorpo- rated; Dialysis Clinic, Incorporated; and R & D Laboratories. © 1997 by the International Society of Nephrology intervals, was started at age 41 months. A repeat renal biopsy at age 52 months confirmed the initial diagnosis of minimal-change disease and mild JGA enlargement (Fig. 1B). She remained symptom-free during a 14-month course of CsA monotherapy. Thereafter, her nephrotic syn- drome recurred and became resistant to intravenous methyiprednisolone. Four monthly intravenous doses of cyclophosphamide (1 g/m2/dose) also produced no response. Her other medications at the time included enalapril, diltiazem, furosemide, spironolactone, metolazone, and ferrous sulfate. At age 63 months, and after 9 months of persistent nephrotic syndrome, she was given a second course of CsA, this time for 25 months: Concom- itantly she received intravenous methylprednisolone and alternate-day oral prednisone (the Mendoza protocol [1]). She remained in complete remission during this entire period. Her growth normalized, as did her serum albumin. Serum creatinine ranged from 0.2 to 0.5 mg/dl; the calculated GFR [2] was 73—95 ml/min/1.73 m2. At age 75 months, 12 months into the second course of CsA, a third renal biopsy demonstrated further enlargement of the JGA (Fig. IC). The patient maintained an average blood pressure of 90/60 mm Hg before, during, and after CsA therapy. Enalapril was given for its antiproteinuric effect and diltiazem for its ability to reduce CsA clearance and dosage, and thus, cost. Renal biopsy DR. ARTHUR H. COHEN (Renal Pathologist, Cedars-Sinai Medical Center, and Professor of Pathology and Medicine, UCLA School of Medicine, Los Angeles, California): Pathologic examination of the biopsy specimen from Patient 1 revealed arterial intimal fibrosis, arteriolar insudative lesions (hyalinization), extensive tubular atrophy with interstitial fibrosis, com- plete and segmental glomeruloscierosis, and enlargement of the JGA. These changes, in aggregate, clearly indicate severe nephrosclerosis; however, the JGA enlargement, probably out of proportion to the other changes, suggests a component of chronic CsA toxicity. Light microscopy of the first biopsy from Patient 2 revealed glomeruli of normal size and morphology, no tubular or interstitial changes, and no abnormalities of the arteries or arterioles. The JGA was not enlarged or otherwise abnormal (Fig. IA). Glomeruli were negative by immunofluo- rescence; ultrastructural examination disclosed complete effacement of foot processes as the sole structural alteration. The second biopsy, following 11 months of CsA therapy, was characterized by glomeruli with the same appearance as earlier. The specimen contained a few scattered atrophied tubules. The JGA was mildly enlarged (Fig. 1B). Thus, the features of minimal-change disease persisted, along with an increase in the size of the JGA. This latter finding is observed in chronic CsA toxicity. The third biopsy, performed after 12 months of a second course of CsA, was characterized by several zones ("stripes") of tubular atrophy and intersti- tial fibrosis (Fig. 1D), few (10%) glomeruli with some ischemic capillary wall wrinkling (Fig. 1E), and moderate enlargement of the JGA (Fig. 1C). Ultrastructural examination revealed partial (70%) effacement of glomer- ular visceral epithelial cell foot processes and increased protogranules and mature granules in cells of the JGA. In short, renal biopsy reveals the structural changes associated with chronic CsA administration: chronic ischemic changes, including varying degrees of glomerular capillary wall wrinkling, tubular atrophy with interstitial fibrosis in a vascular arterial distribution ("striped fibrosis"), normal arteries, and enlargement of the JGA. There also can be necrosis/ degeneration of arteriolar smooth muscle and plasma protein insudative lesions in arteriolar walls, typically in an adventitial location; these findings are termed CsA-associated arteriolopathy [3]. 248
Transcript of Cyclosporine and the renin-angiotensin axis · 2017. 1. 11. · gave no family history for renal...

Kidney International, Vol. 52 (1997), pp. 248—260
NEPHROLOGY FORUM
Cyclosporine and the renin-angiotensin axis
Principal discussant: DAVID B.N. LEE
Sepulveda Veterans Affairs Medical Center, and University of California, Los Angeles, California, USA
EditorsJORDAN J. COHENJOHN T. HARRINGTON
NICOLAOS E. MADIAS
Managing EditorCHERYL J. ZUSMAN
Tufts University School of Medicine
CASE PRESENTATION
Patient 1. A 58-year-old man was hospitalized with hypertension,168/114 mm Hg, congestive heart failure secondary to fluid retention, anda serum creatinine of 6.9 mgldl. Six years earlier he had received a cardiactransplant for end-stage idiopathic cardiomyopathy and was given cyclo-sporine (CsA). Prior to transplantation he was normotensive (bloodpressure, 100/70 mm Hg) and had a serum creatinine concentration of 3.6mg/dl, which was attributed to his refractory biventricular heart failure. Hegave no family history for renal disease or high blood pressure. The serumcreatinine decreased to 0.8 mg/dl one month after cardiac transplantationand fluctuated between 1 to 2 mg/dl for about four years before beginningan inexorably upward course. His blood pressure rose rapidly aftertransplantation, reaching 160/120 mm Hg by the second month.
Four months before this admission, he had been evaluated for rapiddeterioration in renal function and refractory hypertension; his bloodpressure reached as high as 180/140 mm Hg. A percutaneous renal biopsywas obtained. An endomyocardial biopsy at the same time revealed noevidence of rejection. During this admission, acute dialysis was initiated,and thc patient's congestive heart failure improved markedly following a10-liter fluid removal. He subsequently was maintained on chronic dialysiswith continued good cardiac graft function.
Patient 2. A 6-year-old girl first developed steroid-dependent nephroticsyndrome at age 26 months. A renal biopsy at 33 months showedminimal-change disease and normal juxtaglomerular apparatus (JGA, Fig.1A). A chlorambucil-induced remission of eight weeks was followed by arelapse two months after the drug was discontinued. Her nephroticsyndrome became resistant to oral corticosteroid administration, respond-ing only to intravenous methyiprednisolone.
yclosporine (10—12 mg/kg/day), given in divided doses at eight-hour
Key words: cyclosporine, renin-angiotensin system, hypertension.
The Nephrology Forum is funded in part by grants from Hoechst MarionRoussel, Incorporated; Amgen, Incorporated; Merck & Co., Incorpo-rated; Dialysis Clinic, Incorporated; and R & D Laboratories.
© 1997 by the International Society of Nephrology
intervals, was started at age 41 months. A repeat renal biopsy at age 52months confirmed the initial diagnosis of minimal-change disease andmild JGA enlargement (Fig. 1B). She remained symptom-free during a14-month course of CsA monotherapy. Thereafter, her nephrotic syn-drome recurred and became resistant to intravenous methyiprednisolone.Four monthly intravenous doses of cyclophosphamide (1 g/m2/dose) alsoproduced no response. Her other medications at the time includedenalapril, diltiazem, furosemide, spironolactone, metolazone, and ferroussulfate.
At age 63 months, and after 9 months of persistent nephrotic syndrome,she was given a second course of CsA, this time for 25 months: Concom-itantly she received intravenous methylprednisolone and alternate-dayoral prednisone (the Mendoza protocol [1]). She remained in completeremission during this entire period. Her growth normalized, as did herserum albumin. Serum creatinine ranged from 0.2 to 0.5 mg/dl; thecalculated GFR [2] was 73—95 ml/min/1.73 m2. At age 75 months, 12months into the second course of CsA, a third renal biopsy demonstratedfurther enlargement of the JGA (Fig. IC). The patient maintained anaverage blood pressure of 90/60 mm Hg before, during, and after CsAtherapy. Enalapril was given for its antiproteinuric effect and diltiazem forits ability to reduce CsA clearance and dosage, and thus, cost.
Renal biopsyDR. ARTHUR H. COHEN (Renal Pathologist, Cedars-Sinai Medical Center,
and Professor of Pathology and Medicine, UCLA School of Medicine, LosAngeles, California): Pathologic examination of the biopsy specimen fromPatient 1 revealed arterial intimal fibrosis, arteriolar insudative lesions(hyalinization), extensive tubular atrophy with interstitial fibrosis, com-plete and segmental glomeruloscierosis, and enlargement of the JGA.These changes, in aggregate, clearly indicate severe nephrosclerosis;however, the JGA enlargement, probably out of proportion to the otherchanges, suggests a component of chronic CsA toxicity.
Light microscopy of the first biopsy from Patient 2 revealed glomeruli ofnormal size and morphology, no tubular or interstitial changes, and noabnormalities of the arteries or arterioles. The JGA was not enlarged orotherwise abnormal (Fig. IA). Glomeruli were negative by immunofluo-rescence; ultrastructural examination disclosed complete effacement offoot processes as the sole structural alteration. The second biopsy,following 11 months of CsA therapy, was characterized by glomeruli withthe same appearance as earlier. The specimen contained a few scatteredatrophied tubules. The JGA was mildly enlarged (Fig. 1B). Thus, thefeatures of minimal-change disease persisted, along with an increase in thesize of the JGA. This latter finding is observed in chronic CsA toxicity. Thethird biopsy, performed after 12 months of a second course of CsA, wascharacterized by several zones ("stripes") of tubular atrophy and intersti-tial fibrosis (Fig. 1D), few (10%) glomeruli with some ischemic capillarywall wrinkling (Fig. 1E), and moderate enlargement of the JGA (Fig. 1C).Ultrastructural examination revealed partial (70%) effacement of glomer-ular visceral epithelial cell foot processes and increased protogranules andmature granules in cells of the JGA.
In short, renal biopsy reveals the structural changes associated withchronic CsA administration: chronic ischemic changes, including varyingdegrees of glomerular capillary wall wrinkling, tubular atrophy withinterstitial fibrosis in a vascular arterial distribution ("striped fibrosis"),normal arteries, and enlargement of the JGA. There also can be necrosis/degeneration of arteriolar smooth muscle and plasma protein insudativelesions in arteriolar walls, typically in an adventitial location; these findingsare termed CsA-associated arteriolopathy [3].
248

1): !6 t IT. $4SW
C
B
a
Nephrology Forum: GsA and the renin-angiotensin axis 249
A B
C
D E
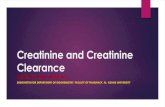
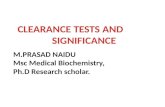
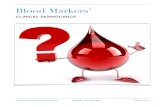
Fig. 1. Renal biopsy findings, Patient 2. First biopsy. A. The glomeruli, tubules, interstitium, and juxtaglomerular apparatus all are unremarkable.(Periodic acid-methenamine silver, x 195). Second biopsy: B. The only abnormality is the mildly enlarged juxtaglomerular appartus (arrow). (Masson'strichrome, X 195). Third biopsy: C. Stripe of tubular atrophy and interstitial fibrosis separates a normal glomerulus (arrow) from an ischemic one (doublearrows). (Periodic acid-methenamine silver, >< 45). D. Normal and ischemic glomcruli, with portion of normal artery at the left border. (Periodicacid-methenamine silver, X 195). E. Vascular pole of glomerulus with enlarged juxtaglomerular apparatus. (Periodic acid-methenamine silver, )< 295).
DISCUSSION these two patients. Patient 1, the heart transplant recipient,DR. DAVID B. N. LEE (chief Nephrolo' Section, Department of initially had normal blood pressure and normal renal function, as
Veterans Affairs Medical Center, Sepulveda, and UCLA-San Fer- reflected by the serum creatinine concentration of 0.8 mg/dlnando Valley Medical Program, Sepulveda and Sylmar; and Profes-. immediately after the restoration of normal cardiac function. Hesor of Medicine, UCLA School of Medicine, Los Angeles, Galifor- had no family history of hypertension or renal disease. His CsAnia): Thank you, Dr. Cohen. Let me first summarize the course of dosage was tapered to 5 mg/kg/day at about 10 weeks after

250 Nephrology Forum: CsA and the renin-angiotensin axis
System component Animals Humans
Plasma renin activity (PRA) a (Pattern I) . (Pattern II)Plasma toal renin and pro-reninRenin synthesis and secretion
1 1'NS'
Renin processing and secretory defects + +JGA hypertrophy and hyperplasia + +Recruitment of renin-containing cells + NSTissue and plasma ACE activity C) NSAT1 receptor density C) NS
transplantation and thereafter was maintained at 1—3 mg/kg/day.His postoperative course was characterized by the rapid develop-ment of hypertension and progressive loss of renal function, whichculminated in end-stage renal failure and chronic hemodialysis sixyears later. The heart graft remained free of rejection andmaintained good function. The second patient, a 6-year-old girl,was given CsA for minimal-change nephrotic syndrome, whichwas initially steroid-dependent and subsequently steroid-resistant.In contrast to the first patient, she was given high doses of CsA—asmuch as 17 mg/kg/day—but her blood pressure and renal functionremained stable throughout the cumulative treatment period of39 months. Serial renal biopsies, however, demonstrated progres-sive structural changes attributable to CsA administration (Fig. 1).
These two patients illustrate the serious hypertensive [4] andnephrotoxic 15] effects of CsA. However, individual susceptibilityto the toxic effects of CsA varies. For example, children appear totolerate higher CsA dosage. This difference has been attributed tothe presence in children of a less efficient CsA absorptive processand a more efficient CsA metabolic process than those in adults[6]. The relatively low plasma CsA level, in the face of high-doseCsA administration in our younger patient, is consistent with sucha postulate. The second case also reminds us that markedstructural damage in the kidney can occur in the absence of overtclinical evidence of hypertension or nephrotoxicity.
Finally, both patients exhibited hypertrophy and hyperplasia ofthe juxtaglomerular apparatus, and this observation leads us tothe focus of this Forum. In the nephrotic child, serial biopsiesdemonstrated JGA enlargement only after the initiation of CsAtherapy; sustained CsA treatment exaggerated this enlargement.This finding is a well-recognized feature of CsA administration inpatients [7—9] and rats [10—12]. However, because plasma reninactivity (PRA) is either normal or low in humans taking CsA [13,14], the renin-angiotensin system (RAS) has not been consideredimportant in the pathogenesis of CsA hypertension [4] andnephrotoxicity [5].
This Forum will address the complex interactions between CsAand the RAS and the possible role of the renin axis in thepathogencsis of CsA hypertension and nephrotoxicity. I do notsuggest that CsA causes hypertension and ncphrotoxicity solelythrough its action on the RAS. Rather, I will summarize evidencesupporting RAS as one importants participant in the pathogenesisof these two complications of CsA administration.
Effect of CsA on the RAS
Cyclosporine has a variety of effects on the renin-angiotensinsystem (Table 1). In virtually all animal studies done by our groupand others, CsA increases PRA [13, 15, 16]. Although most of
these have been rat studies, CsA also stimulates PRA in the dog[17]. In-vitro, studies using renal cortical slices suggest that CsAdirectly stimulates renin release [18, 19]. Using rat juxtaglomeru-lar cell culture, Kurtz, Bruna, and Kuhn concluded that CsA notonly increases reniri secretion, as reflected by increases in reninactivity in the incubation medium, but also stimulates its synthesis[20]. This stimulatory action is dose-dependent and rapid in onset:CsA produces a secretory response within 10 minutes and asynthetic response by 24 hours. In addition to direct stimulation ofrenin secretion and synthesis in juxtaglomerular cells in vitro, CsAalso is associated with juxtaglomerular hypertrophy and hyperpla-sia in vivo [10—12]. Using immunocytochemistry, Tufro-McRed-die and associates demonstrated increased renin-staining cells inthe JGA and recruitment of renin-containing cells in the afferentarterioles of rats treated with CsA for three weeks [21]. Theseauthors noted that CsA altered neither the level nor the distribu-tion of intrarenal renin mRNA and suggested that CsA acts onrenal renin metabolism through post-transcriptional events. Thisreport contrasts with short-term (up to 24 hours) in-vitro studies,which clearly demonstrated a direct CsA-induced stimulatoryeffect on renin synthesis in juxtaglomerular cells [20].
The mechanism by which CsA activates the renin-angiotensinsystem is not known. Acute incubation studies demonstrated thatCsA's effect on reniri is not mediated by changes in cellularprostaglandin or cAMP [20]. The estimated half-maximal effecton renin secretion and production was iO M, a value approxi-mating the dissociation constant for CsA binding to cyclophilin,2 x iO M. This observation suggests that CsA-cyclophilinbinding is involved in the activation of the renin axis. CyclosporineH (CsH), which differs from CsA in one amino acid at position 11,binds cyclophilin weakly and has no effect on juxtaglomerular cellrenin secretion [20].
After giving rats CsA (12.5 mg/kg/day for three weeks), Shehataand associates detected selective accumulation of platelet-derivedgrowth factor (PDGF) within the enlarged secretion granules ofthe hypertrophied juxtaglomerular cells [12]. The same laboratoryalso observed increased transforming growth factor-/3 (TGF-/3) injuxtaglomerular cells of CsA-treated rats [22]. Transforminggrowth factor-p stimulates renin secretion by juxtaglomerularcells [23]. Are these growth-regulatory factors responsible forRAS activation, JG cell hypertrophy and hyperplasia, or both?Also, angiotensin II (Ang II) stimulates the synthesis of bothPDGF [24] and TGF-13 [25, 26]; does CsA therefore activate thesefactors directly, or indirectly by stimulating the RAS? Clearlythese and many other questions await resolution.
Cyclosporine also acts on other components of the RAS. Ourlaboratory has reported a dramatic elevation in plasma pro-reninconcentration in rats treated with CsA for two weeks [19]. Ermanand colleagues reported that angiotensin-converting enzyme(ACE) activity was stimulated in the lung and serum, but reducedin renal cortex, in rats given CsA [27]. Two studies have investi-gated the effect of CsA on type-I angiotensin receptor (AT1).Tufro-McReddie and coworkers found that CsA reduced renalAT1 receptor mRNA levels [21]; Regitz-Zagrosek and associatesnoted a CsA-induced increase in the number of AT1 receptors inrat kidney, liver, and adrenal cortex and medulla [28]. Simulta-neous treatment with the AT1 antagonist losartan (DUP 753)aborted this CsA-induced upregulation.
In most respects, cyclosporine's effects are similar in animalsand humans (Table 1). The exception is CsA's action on PRA. Incontrast to findings in animal studies, CsA fails to increase [29,
Table 1. Cyclosporine and the renin-angiotensin system
Symbols: 1., decreases; 1' increases; +, induces; C) modulates.Not studied.

Nephrology Forum: CsA and the renin-angiotensin axis 251
30], and in most instances decreases [8, 31], PRA in human studies[13]. Nor does cyclosporine stimulate PRA in monkeys (marmo-set, Callithrixjacchus) [32]. These observations have contributedto the general impression that the RAS probably does not play animportant role in CsA toxicity in humans [3—5]. Less appreciatedare the observations that CsA markedly elevates plasma totalrenin and pro-renin concentrations [8, 33] and enlarges the JGA,as in the patients presented in this Forum. "Striking" JGAhyperplasia has been reported in heart transplant recipientsreceiving CsA [8, 9]. In renal transplant recipients, conversion oftherapy from CsA to azathioprine dramatically reduces the num-ber of renin-containing cells in the JGA of the grafted kidney [7].
The striking increase in secretion granules in these renin-containing cells in humans is not reflected by a concomitantincrease in PRA. The lack of rise in plasma renin activity raisesthe possibility of an alteration in cellular renin processing and inthe release of active renin. Indeed, clinical studies have demon-strated a markedly blunted PRA secretoly response to a low-sodium diet and diuretic administration in CsA-treated renaltransplant recipients [31] or to acute converting enzyme inhibitionin CsA-treated cardiac transplant recipients [34]. In insulin-dependent diabetic patients, CsA is also associated with juxtaglo-merular cell hypertrophy and a reduced renin secretory responseto furosemide [35].
A similar renin secretory defect also can develop in CSA-treated rats. Burdmann et al found that ACE inhibition inCsA-treated rats did not produce an anticipated increase in PRA[36]; this observation is consistent with the possible presence of adefect in renin secretion. A CsA-induced renal renin secretorydefect is more convincingly demonstrated in the rat under condi-tions of maximal renin-axis activation. Helmchen and associatesexamined the effect of CsA on renal renin content (RRC) andplasma renin content (PRC) in two-kidney, one-clip hypertensiverats [37]. Cyclosporine dramatically decreased the PRC (48.63.0 versus 82.2 5.0 [vehicle controll nglml/hr) and markedlyincreased RRC in both the clipped (49.2 8.0 versus 11.9 1.0
jtg/100 mg/hr) and the intact (23.3 3.1 versus 1.7 0.4) kidney.The study also noted morphologic evidence of increased JGAactivation [37].
The mechanism for this CsA-induced intrarenal renin accumu-lation is not clear. Early observations suggest that CsA reducesthe conversion of pro-renin into active renin [8, 13], the usualform of renin secreted through the regulated pathway. Cyclospor-me also can directly block renin secretion, as it inhibits exocytoticdegranulation in a number of cell systems, possibly through itsinhibitory effect on the phosphatase activity of calcineurin [38, 39].More recently, Norling and associates reported the progressiveaccumulation of an acidic renin isoform (p1 5.5, MW 32—36 kD)in the kidneys of CsA-treated rats [40]. Since acidic renin isoformsnormally constitute only a small fraction of the stored renin [41],its accumulation suggests the presence of one or more CsA-induced renin processing and trafficking defects. An increase inthe acidic forms of renin correlates with an elevation in systolicblood pressure in stroke-prone hypertensive rats [42].
In summary, GsA has multiple effects on the RAS. First,evidence is convincing for its direct stimulatory action on reninsynthesis and release in cultured juxtaglomerular cells. In additionto this short-term response, CsA also causes a more sustainedresponse characterized by JGA hypertrophy and hyperplasia.Finally, CsA induces alterations in renin processing and secretion,reflected by increases in renal renin content and renin granule
accumulation, and by decreases in plasma renin content (inhumans). Are these effects the consequences of different mecha-nisms or, more likely, do they represent different facets of a single,complex process? The answers remain to be determined.
Differences in experimental and human peripheral reninprofiles
Much has been written on the dissimilarity in the RAS'response to CsA in experimental and human studies. But the onlymajor difference is the level of circulating PRA (Table 1). Inexperimental studies, both active and inactive renins increase(Pattern I); in human and primate studies, only the inactive reninincreases (Pattern II). Two possible, but not mutually exclusive,mechanisms could account for the evolution of these differentpatterns.
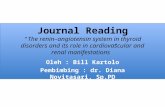
Multiple sites of action of CsA on juxtaglomerular cells. Cyclo-sporine acts on the juxtaglomerular cell's renin synthetic andsecretory process at three possible steps: stimulation of pro-reninsynthesis, inhibition of pro-renin-active renin conversion, andblockade of active renin secretion (Fig. 2). The relative potency ofaction at each site varies under different experimental conditions,for example, the animal species used, and the duration and dosageof CsA treatment. Thus, under short-term, in-vitro incubationconditions, and in most animal studies, the greatest action is onstimulation of pro-renin synthesis, whereas the inhibitory actionon pro-renin-to-active renin conversion or on active renin secre-tion, if present, is relatively minor and inapparent (Fig. 2, upperpanel). The net effect of these actions can account for a Pattern Irenin profile in the circulation.
In more long-term human and primate studies, the inhibitoryeffect of CsA on pro-renin-to-active renin conversion and thesecretion of active renin might dominate its stimulatoiy action onpro-renin synthesis (Fig. 2, lower panel). The constitutive pro-renin secretory pathway remains intact or minimally inhibited[38]. This hypothesis would explain the finding of low PRA andhigh pro-renin in the circulation of humans and primates, thePattern II profile. Circulating pro-renin can be further augmentedby pro-renin released from extrarenal tissues, while circulatingactive renin can be further inhibited by CsA's effect on renalhemodynamics resulting in sodium retention and volume expan-sion [141.
Not all experimental studies yield a Pattern I renin profile.Although PRA was consistently elevated in rats treated with CsAfor two weeks [16], when the treatment was prolonged to twomonths, an elevation in PRA was no longer evident (unpublishedobservation). Burdmann et al found that PRA was significantlyhigher in CsA-treated rats when compared to vehicle-treated ratsat two weeks, hut by four weeks, the PRAs in the CsA-trea ted andcontrol rats no longer differed [36]. lntrarenal renin mRNA didnot increase in rats treated with CsA for three weeks [21]; thisfinding suggests that this treatment regimen did not raise therenin synthesis rate. In addition to the duration of the treatment,varying the dosage of CsA also can exert a biphasic effect on PRA.Siegl et al found that CsA caused a dose-dependent stimulation ofPRA up to 20 mg/kg/day. Further increases in dosage wereassociated with a return of PRA to baseline levels [43]. Thus,increasing the duration or dosage of CsA can change the reninprofile in animal studies from Pattern I to Pattern II. Likewise,although most clinical studies have found circulating renin con-forming to the Pattern II profile, some studies have reported aPattern I profile in GsA-treated patients [33, 44, 45]. Thus, under

Pattern II
TI't
Renin
(Tissue proreniri)/Prorenin
Tissue
cRAS(JGA)
tRAS
Circulation
Active renin
F'rorenin
Cell
tGSA -
+,JGA
Circulation
Pattern I
*
*GSA
Renin
tPro renin —
4. Renin
Pro renin —
GSA
+3 ___JGA L
252 Nephrology Forum: CsA and the renin-angiotensin axis
Fig. 2. Possible actions of cyclosporine (CsA)on juxtaglomerular apparatus (JGA) reninsynthesis and secretion.
Fig. 3. Sources of circulating active renin andpro-renin. cRAS = circulating renin-angiotensin system; JGA = juxtaglomerularapparatus; tRAS = tissue renin-angiotensinsystem.
certain conditions, human RAS might respond to CsA in a fashionsimilar to that of the animal RAS.
C'yclosporine acts on circulating as well as tissue R.4S. The RAScomprises two components: the classical circulating (cRAS) andthe relatively recently recognized tissue (tRAS) components [46].The eRAS consists of angiotensinogen, which is secreted by theliver into the circulation, where it is cleaved by renin derived fromthe kidney to form angiotensin I. Angiotensin I then is convertedby the angiotensin-converting enzyme in the pulmonary vascula-ture into angiotensin II, which circulates to various tissues, whereit exerts its effects through interaction with angiotensin TI recep-tors. Thus, the cRAS functions as a classical endocrine system,and its activity traditionally is monitored by measurement of thecirculating renin activity, the PRA. Conventional practice classi-fies a disorder as "high-renin" and "renin-dependent" if the PRAis abnormally high, and "low-renin" or "renin-independent" if thePRA is low.
The early phase of experimental renovascular hypertension is aclassic example of a renin-dependent disorder with a high PRA[47]. Constriction of one renal artery produces a parallel rise inblood pressure and PRA. Blockade of the RAS abrogates thehypertension. However, if the renal artery constriction is sus-tained chronically, the PRA falls to normal or below normal [47,48]. Nevertheless, the hypertension persists and remains "renin-dependent," that is, it continues to respond to maneuvers thatblock the RAS. The observed changes in PRA might reflect a"switch" from an initial activation of the eRAS to a moresustained activation of the tRAS. Because the circulating activerenin is derived exclusively from the eRAS component of thekidney (Fig. 3) [46], a fall in PRA would be anticipated when theacute activation of the eRAS is replaced by the chronic activationof the tRAS.
Evidence is accumulating that supports the existence of a localtRAS whose activity is not reflected by PRA levels. The biologic

Nephrology Forum: CsA and the renin-angiotensin axis 253
Table 2. Diabetes mellitus and the renin-angiotensin system (RAS)
Low-renin syndromeLow PRA and high renal renin contentHigh plasma pro-reninPro-renin correlates with microvascular damages
High incidence of hypertensionHigh incidence of renal damage
Affhrent arteriolopathyIntrarenal RAS mediates renal injury
role of tRAS, particularly in terms of blood pressure homeostasis,is highlighted by the recent generation of transgenic rats harbor-ing the mouse Ren2d renin gene [TGR(mREN2)271 [49]. Theserats develop fulminant hypertension, low PRA, suppressed renalrenin content, high plasma inactive renin, and high extrarenaltransgene expression. These findings are not unlike those inducedby CsA. Angiotensin-converting-enzyme inhibition in this modelreproducibly reduced blood pressure by 40 to 60 mm Hg [50].Proteins and messenger RNA encoding all the components of theclassical cRAS, including angiotensin receptors, have been co-localized within many tissues, including the kidney, brain, adrenal,pituitary and reproductive tissues, and the heart and vasculature[46]. The kidney, although a major participant in the cRAS, has inaddition its own complete system of tRAS [51].
Cyclosporine clearly activates the cRAS in animals, as reflectedby its stimulatory action on PRA both in in-vitro and in-vivostudies. In addition, CsA appears to stimulate the tRAS, asevidenced by its activation of the different components of the RASin the vasculature [52], the kidney, the liver, and the adrenals [28].Thus, like experimental renovascular hypertension, CsA stimu-lates both the eRAS and the tRAS. I would argue that theelevated PRA reported in most of the animal studies (Pattern I)probably represents the early cRAS-stimulatory phase, while thesuppressed PRA observed in most human studies (Pattern II)probably represents the chronic tRAS-stimulatory phase.
Diabetes mellitus: A CsA-like low-renin state
yclosporine's effects on the RAS and the microvasculatureclosely resemble the hemodynamic and hormonal abnormalities indiabetes mellitus (Table 2). Diabetes mellitus has been classifiedas a low-renin condition because PRA is low in the circulation.Nevertheless, the role of RAS in the microvascular damage seenin diabetes is well established [53, 54]. Most studies in experimen-tal as well as in clinical (type-I and type-Il) diabetes report normalor low PRA in the circulation [53]. Renal renin content, on theother hand, is disproportionately high; this finding suggests animpairment in renal renin release into the circulation [54, 551. Asin the CsA studies cited earlier, plasma pro-renin is elevated indiabetic patients, particularly in those with microvascular damage[56, 57].
Relatively little is known about the function of pro-renin.Pro-renin-activating enzymes have been found in the aorta and incultured endothelial cells [58]; these findings suggest that thecirculating renin precursor acts as a reservoir for the localactivation and amplification of the RAS activity in the bloodvessel. MUller-Schweinitzer, using canine saphenous veins, alsoconcluded that the vascular effect of CsA is the consequence ofactivation of circulating pro-renin rather than the result of theaction of one or more angiotensin-forming enzymes located in thevenous vessel wall [52]. Sealey et al proposed that pro-renin can
be activated by binding at local tissue sites without cleavage of thepro-sequence [591; this form of activation can lead to the localgeneration of Ang II.
In long-standing diabetes mellitus complicated by microvascu-lar disease, plasma inactive renin is high, and plasma activepro-renin is normal or low [53—57]. Luetscher and colleaguesreported that the frequency of vascular complications (retinopa-thy and albuminuria) varied directly with plasma inactive renin:patients with plasma inactive renin of less than 20 ng/ml'/hr,above 50 nml1/hr', and more than 100 ngIml/hr1 exhib-ited these complications at a frequency of 0%, greater than 50%,and greater than 95%, respectively [56]. Myers and associatesreported the mean value of plasma inactive renin in hearttransplant recipients with CsA-associated chronic nephropathy tobe 224 ng/ml/hr' [8]. Whether microvascular disease associ-ated with CsA therapy correlates with plasma pro-renin levels hasnot been studied.
Finally, diabetes mellitus, like CsA administration, is accompa-nied by a high incidence of hypertension and renal injury associ-ated with afferent arteriolopathy [53]. In diabetes mellitus, evi-dence now implicates the local renal tissue RAS in thepathogenesis of renal injury [53, 51.
RAS in CsA-induced hypertension and nephrotoxicity
cyclosporine-induced hypertension. Multiple mechanisms havebeen proposed for the hypertensive effects of CsA [4, 14, 60],including the possibility that several events and systems interact togenerate alterations in blood pressure. The role of the RAS ismost effectively demonstrated under controlled conditions inwhich a relatively "pure" CsA hypertension can be induced. We[16] and others [43, 61] have reported that spontaneously hyper-tensive rats (SHR) predictably respond to CsA by a dramaticexacerbation of hypertension, associated with marked increases inPRA and pro-renin. Concomitant administration of enalaprilcompletely reversed this CsA-exacerbated hypertension [16].
More recently, Clozel, Fischli, and Ménard demonstrated thatACE inhibition with colazapril and renin inhibition with Ro42—5892 completely suppressed plasma Ang II and amelioratedCsA-induced hypertension in monkeys [62], a model in whichCsA, as in humans, does not elevate PRA. Similarly, reninantibodies suppressed circulating Ang II without reducing bloodpressure. This disparity was attributed to the inability of therelatively large antibodies to diffuse out of the vasculature antiinhibit local angiotensin generation. Thus, the tRAS likely partic-ipates in the pathogenesis of CsA-induced hypertension.
The role of the renin axis on CsA-associated hypertension inhumans, as reflected by the blood pressure response to renin-axisblockade, is less straightforward. The finding of low PRA inCsA-treatcd patients and the concern over possible ACE inhibi-tion-induced hypcrkalcmia and acute renal failure have led to theavoidance of ACE inhibitors and the use of calcium-channelblockers [41. Mourad, Ribstein, and Mimran reported a prospec-tive, randomized 30-month study comparing the effects of lisino-pril and nifedipine in the treatment of hypertension in CsA-treated renal transplant recipients [631. They concluded thatlisinopril was as effective as nifedipine in the control of hyperten-sion in these patients. Only 2 of the 14 lisinopril-treated patientsrequired furosemide as a second drug for adequate control ofhypertension; 7 of the 11 nifedipine-treated patients needed asecond drug, atenolol, for alleviation of a side effect (flushing) or

254 Nephrology Forum: CsA and the renin-angiotensin axis
for adequate blood pressure control. No relationship was ob-served between ACE inhibition and renal functional deteriorationand hyperkalemia. In contrast to calcium-channel blockade, ACEinhibition was associated with a significant reduction in thefiltration fraction and a decrease in the intraglomerular capillarypressure. The effect of ACE inhibitors on hypertension appearedto increase with the duration of drug administration [63]. AcuteACE inhibition with captopril caused a smaller decrement inblood pressure than did acute calcium-channel blockade withnifedipine in CsA-treated, hypertensive heart transplant recipi-ents [34]. The blood pressure response to calcium-entry blockadecan be mediated through the RAS. Thus, CsA potentiates theaction of Ang II on vascular smooth muscle cells [64], andcalcium-entry blockade can prevent this CsA-induced hypersensi-tivity to Ang II [65].
Most likely, RAS activation is only one of many components inthe pathogenesis of CsA-induced hypertension [4, 14, 601. Wehave noted that the hypertensive effect of CsA is most apparent ina rat population genetically susceptible to hypertension [66].Cyclosporine significantly worsened hypertension in the SHR butdid not increase blood pressure in the normotensive Sprague-Dawley (SD) rat. Cyclosporine also increased blood pressure inWistar-Kyoto (WKY) rats that have higher than normal baselineblood pressure [66], but had no hypertensive effect in Wistar-Kyoto rats that have normal baseline blood pressure [61]. Othergroups also have observed that normotensive rats are relativelyresistant to the hypertensive effect of CsA [67, 68]. An inter-species difference in response to CsA's hypertensive effect becameapparent when, in contrast to findings in the rat, CsA consistentlycaused hypertension in normotensive marmosets [321. It is notclear why virtually all heart transplant recipients appear suscep-tible to the hypertensive effect of CsA, while recipients of otherorgans and patients given CsA for conditions unrelated to trans-plantation exhibit less susceptibility [4]. Bone marrow transplantrecipients, children [69] as well as adults [70], appear to be moresusceptible to severe hypertension when given CsA.
GsA nephrotoxicily. Several clinical and morphologic forms ofCsA nephrotoxicity have been described [3, 5]. Of greatestconcern to nephrologists is the progressive, irreversible tubuloin-terstitial fibrotic form characterized by afferent arteriolopathy,interstitial fibrosis (the so-called "striped" fibrosis), and some-times by glomerular and arteriolar thrombi [3, 711.
Cyclosporine stimulates rabbit renal fibroblast production [72]and increases collagen production both in human and animal renalcell lines [73, 74]. Nast and associates have demonstrated an earlyand sustained increase in cortical al(I) pro-collagen mRNA inrenal tissue of CsA-treated rats [75]. Perhaps CsA induces renalfibrosis directly or indirectly, or both. We will focus on evidencesuggesting the participation of the RAS in this process.
Myers and colleagues proposed that chronic CsA therapy inheart transplant recipients causes an obliterative arteriolopathy ofthe afferent arterioles that leads to irreversible downstreamstructural damage [76]. Three-dimensional morphometric analysisof renal tissue revealed a marked deviation in the glomerularcapillary tuft volume distribution pattern in CsA-treated hearttransplant recipients [9] and in rats with a renal isograft [77]. Incontrol tissue, the capillary tuft volume was normally distributedaround the mean (bell-shaped curve), hut the CsA-treated tissuehad a relative increment in the number of glomeruli that wereeither smaller or larger than the mean volume. The smallerglomeruli possibly reflected CsA-induced ischemic damage and
capillary collapse, while the glomeruli unaffected by the ischemicinjury enlarged.
Mason and associates proposed that accumulation of renin inthe JG cells might cause arteriolopathy [13]. The lesion developsin distal afferent arterioles as they enter glomeruli, where reninproduction is most abundant and where renin accumulates withCsA therapy in humans and animals. The lesion is characterizedby early vacuolation of the endothelial and smooth muscle cells,followed by necrosis and proteinaceous deposits. Ultimate occlu-sion and obliteration of the arteriole cause ischemic collapse andfibrosis of the corresponding glomerulus and the associatedtubulointerstitium, and inflicts the greatest damage to the regionmost vulnerable to reduction in oxygen supply, that is, the innerstripe of the outer medulla and the medullary rays [78]. Themedullary rays are cortical invaginations of medulla extendingtowards the capsule and consisting of collecting tubule, ascendinglimb, and S2 and S3 proximal tubules. The striped appearancedescribed in CsA-treated humans and animals [71, 79] is attrib-uted to the fibrosis of this medulla/medullary ray complex.
The spontaneously hypertensive rat was the first experimentalmodel to develop human-type afferent arteriolopathy with CsAtherapy. Electron microscopic examination of the kidneys in theserats revealed increased accumulation of intracellular renin gran-ules [61]. In subsequent studies, similar arteriolar lesions withhyaline deposits have been produced in normotensive rats [80, 81]and in rabbits [82]. In salt-depleted, Sprague-Dawley rats, theCsA-induced "hyaline" injury in the smooth muscle cells corre-lates with intracellular renin granule accumulation [81]. Enalapriland losartan were found to reverse the rapid and sustainedafferent arteriolar vasoconstriction caused by CsA treatment inthese rats.
In addition to the juxtaglomerular apparatus and vascularrenin, the local, intrarenal RAS also might participate in thepathogenesis of CsA nephrotoxicity. The inner zone of the outermedulla has the highest density of angiotensin II receptors (AT1subtype) [83], both in rat and human kidneys. Ultrastructuralstudies localized the receptor to the interstitial cells between thetubules and the vasa recta bundles. These cells exhibit character-istics of type-i interstitial cells [84]. Because type-i interstitialcells are most abundant toward the tip of the inner medulla, whichhas almost no Ang II receptor-binding activity, these Ang IIreceptor-rich cells are considered a subtype of type-I interstitialcells. These medullaiy receptor sites are not easily accessible tocirculating Ang II and are more likely to respond to Ang IIgenerated in the kidney [83]. In addition to its traditional role ofstimulating vasoconstriction and aldosterone secretion, Ang II isalso an important growth factor [85]. Chronic infusion of Ang IIhas been shown to cause renal interstitial cell proliferation andfibrosis [86].
Young and associates have reproduced human-type CsA-in-duced nephropathy in salt-depleted, male Sprague-Dawley rats;the lesions comprised striped tubulointerstitial fibrosis, afferentarteriolar hyalinosis, and increased JGA renin expression [87].Fibrosis was preceded by tubular and interstitial cell proliferationand macrophage infiltration, which in turn correlated with in-creased expression of osteopontin at the same sites. Osteopontin,a glycoprotein containing the RGD (Arg-Gly-Asp) sequence, ischemotactic and adhesive for macrophages [881. In a model ofAng Il-induced hypertension, renal tubulointerstitial injury alsoevolved at sites of osteopontin overexpression and monocyte/macrophage accumulation [89]. The authors postulated that CsA

Nephrology Forum: CsA and the renin-angiotensin axis 255
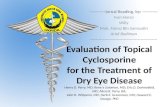
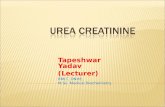
Fig. 4. Cyclosporine (CsA) and the refill-angiotensin system (RAS) in the pathogenesisof renal striped fibrosis (nephrotoxicity). AngTI = angiotensin II. 'Inner stripe of outermedulla; **lnfiltration and proliferation:***Ameliorated by ACE inhibition andlosartan.
directly activates intrarenal RAS, which then stimulates osteopon-tin expression, macrophage infiltration and release of growthfactors, and increased extracellular matrix deposition and stripedcortical interstitial fibrosis [87].
Burdmann and associates have demonstrated that the tubulo-interstitial fibrosis induced by CsA in rats kept on a low-salt dietcan be ameliorated by coadministration of an ACE inhibitor,enalapril, or an angiotensin IT receptor antagonist, losartan [36].Other, earlier studies also have reported a reduction in CsAnephrotoxicity with converting enzyme inhibition therapy [90, 91].
Let me summarize how cyclosporine administration inducesstriped fibrosis in the kidney (Fig. 4). Cyclosporine can inducerenal fibrosis directly (pathway #1) or indirectly through eitherJGA and vascular renin accumulation (pathway #2) or stimula-tion of intrarenal RAS (pathway #3). The activation of local AngII receptors can stimulate fibrogenesis directly (pathway #4), orthrough the overproduction of osteopontin (pathway #5).
As in the case of CsA-induced hypertension, additional factorsand systems are likely to participate in the pathogenesis ofCsA-induced nephrotoxicity. Gillum and Truong did not find thatACE inhibition protected against CsA-induccd tubulointerstitialdisease [92], although the CsA dose used (25 mg/kg intraperito-neally for 28 days) was higher than that used by Burdmann (15mg/kg subcutaneously for 28 days) [36] or Lafayette (9 mg/kg/dayorally for 12 months) [91]. The role of the RAS in renal fibrosis islikely to be more complex than we now understand. For example,both enalapril and losartan ameliorate CsA-induced fibrosis, butonly losartan, not enalapril, blocked the CsA-induced elevation incortical ol(l) pro-collagen mRNA [36]. It is likely that multipleAng Il-mediated pathways—for example, cell activation, cytokinerelease, and matrix production—participate in the mediation ofCsA-induced nephrotoxicity.
QUESTIONS AND ANSWERS
DR. ALAN WIlKINsoN (Medical Director, Kidney and PancreasTransplantation, UCLA Medical Center, Los Angeles, California): I
have a question for Dr. Arthur Cohen. Most of the biopsy reportswe see are from patients who have had renal transplants. There isstill some debate as to whether the pathologic effects of cyclo-sporine A differ in these kidneys as compared to effects innon-transplant patients receiving cyclosporine for the treatmentof other diseases. You often call us when you see significant JGAhypertrophy to inquire whether we suspect renal artery stenosis.Do you see JGA hypertrophy less frequently in renal allograftsthan in native kidneys exposed to cyclosporine?
DR. COHEN: In my experience, cases of enlarged juxtaglomer-ular apparatus are not more frequent or more prominent intransplanted than in native kidneys. The question of renal arterystenosis is raised in transplants because of two considerations: (1)the well-known fact that renal artery stenosis can be a complica-tion of the arterial anastomosis or of arterial rejection, usuallychronic, involving the main or large renal arteries, and (2) thecommon co-existence in the transplanted kidney of zones ofreduced tubular diameters with variable interstitial fibrosis, fea-tures that are often part of the structural abnormalities of renalartery stenosis.
DR. WILKINSON: Dr. Lee, ACE inhibitors as well as calcium-channel blocking agents are effective in the treatment of post-transplant hypertension. Calcium-channel blockers also mightconfer a measure of protection against cyclosporine nephrotoxie-ity. Do you have any information on the effect of calcium-channelblockers on tissue renin concentration?
DR. LEE: I am not aware of any observations on the effect ofcalcium-channel blockers on the concentration of tissue renin inCsA-treated animals or patients. However, we do know thatcalcium entry blockers stimulate, and calcium entry "facilitators"inhibit, renin in studies using juxtaglomerular cells, renal glomer-uli, renal cortical slices, and whole kidneys [93]. These responsesare consistent with the general observation that renin secretion isinversely related to the ambient calcium concentration. Renin andparathyroid hormone are two exceptions to the more typical
f intra-fl 3renalRAS
vascularCSA 2 IfJGA&
L____________
I $Afferent vaso-
1 constriction& arteriopathy I
4,lAbundance td VulnerableLAng II receptors MedU1Ia* & medullary rays to hypoxemia
Osteopontin 11
[f Cell activity**
17Striped fibrosis***

256 Nephrology Forum: CsA and the renin-angiotensin axis
secretory mechanism, in which the secretory rate correlatespositively with the intracellular calcium concentration [941.
DR. NIcoLAos E. MADIAS (Chief Division of Nephrology, NewEngland Medical Center, Boston, Massachusetts): My questionconcerns the reliability of enzymatic assays for different compo-nents of the renin system. Monoclonal antibodies recently havebeen used for this purpose. Can you comment on their use in themeasurement of total, active, and inactive renins? Are therestudies on the effects of cyclosporine on the renin system that haveused specific monoclonal antibodies?
DR. LEE: The recently developed immunoradiometric assay ofrenin using monoclonal antibodies allows direct measurement ofthe active and inactive forms of the enzyme [95]. Compared to thetraditional enzymatic assay, it is simpler to perform, can becompleted within one working day, and exhibits greater inter- andintra-laboratory reproducibility [96]. However, for clinical andexperimental applications, the enzymatic assay still might provemore reliable and useful than the direct renin assay, particularly inconditions associated with marked alterations in angiotensinogenconcentrations, for example, pregnancy or primary aldosteronism[96]. The enzymatic assay measures the activity of endogenousplasma renin and renin substrate (angiotensinogen) to formangiotensin I in plasma. Because angiotensin-converting enzyme,which converts angiotensin Ito angiotensin II, is not rate-limiting,the enzyme method reflects the capacity of a patient's plasma togenerate the active hormone, angiotensin II. Thus, the enzymaticassay gives a better reflection of circulating in-vivo activity of therenin system. Finally, I am not aware of data on the effect of CsAon the renin system based on measurements using monoclonalantibodies.
DR. WILKINSON: You have developed a very nice hypothesis.Can you fit the data from Luke and Curtis [14] into your schema?They have shown that in hypertensive renal transplant patientswhose hypertension is salt-dependent, ACE inhibitors and bilat-eral nephrectomy of the native kidneys each produce a similarreduction in systemic blood pressure and about 30% improvementin renal plasma flow and GFR of the transplanted kidney. Thisobservation implies that the retained native kidneys still exert aneffect on salt retention, blood pressure, and on the effective renalplasma flow and GFR of the grafted kidney.
DR. LEE: One can postulate that allograft vasoconstrictioncaused by renin release from the native kidneys is the primaryevent. Bilateral nephrectomy or ACE inhibition then would beexpected to reverse the abnormalities you cited. Possible partici-pation, or lack of participation, of CsA in the modulation of therenin-angiotensin system in these complicated patients wouldrequire more detailed studies.
DR. MADIAS: A captopril challenge test was introduced in thelate 1970s to differentiate among causes of post-transplant hyper-tension. To what extent has the introduction of CsA affected theutility of this test?
DR. LEE: In the "pre-CsA" era, a captopril-induced reduction inallograft GFR was used as a screening test for the presence ofrenal artery stenosis [4, 14, 97]. The sensitivity of the test isincreased by pre-treatment with a diuretic. A positive captopril-challenge test is also observed with chronic vascular rejection, inwhich small intrarenat vascular lesions can induce an angiotensinIl-dependent efferent vascular constriction [4, 14, 97]. The intro-duction of CsA as a routine therapy for transplant recipients,markedly reduced the diagnostic usefulness of this test. Captopriland other ACE inhibitors can markedly reduce GFR in CsA-
treated allograft patients in whom either renal artery stenosis norvascular rejection is present [4, 14, 97, 98]. This is hardlysurprising since, as we have just discussed, CsA can directlystimulate both the circulating and the intrarenal RAS to generateangiotensin II. The effect of ACE inhibition on GFR is expectedto be magnified in patients with concomitant CsA afferent arte-riolopathy. Parenthetically, CsA has been reported to causereversible stenosis of major brances of the renal artery in renalallograft [99].
DR. MADJAS: Is cyclophilin found in the juxtaglomerular appa-ratus?
DR. LEE: Cyclophiliri is found in almost all organisms and celltypes and is the leading candidate for the receptor responsible forthe biologic effects of CsA [100, 101]. The renin stimulatoiy effectof CsA in isolated juxtaglomerular cells was attributed to itsbinding to cyclophilin, because cyclosporine H (CsH), which bindscyclophilin weakly, did not affect renin secretion [20]. Quantita-tive immunofluorescence and confocal microscopy have demon-strated in rat kidneys the presence of cyclophilin, which increasedwith CsA administration [101]. An examination of differentisoforms of cyclophilin using murine renal tissue revealed arestricted distribution of cyclophilin C to proximal straight tubule[102, 103] and proximal convoluted tubule [103]; cyclophilin Awas more evenly distributed along the nephron segments [103].Cyclosporine A treatment increased the cyclophilin C signal [100].I am not aware of any specific attempts at demonstrating thepresence of cyclophilin in the juxtaglomerular apparatus.
DR. IRA KURTZ (Chief Nephrology Division, UCLA MedicalCenter, Los Angeles): Not only is CsA nephrotoxic, but it alsoaffects the liver, pancreas, and heart. What is known about theextrarenal tissue renin-angiotensin system in these organs? Doesthe RAS have a role in the abnormal function of these organs asit does in the kidney?
DR. LEE: The effects of CsA on the tissue renin-angiotensinsystem in the liver, pancreas, and heart have not received muchattention. Cyclosporine has been reported to upregulate angio-tensin receptors in the liver, and this effect is blocked by lisinopriland losartan (DUP 753), an angiotensin receptor antagonist [281.This is a good question and deserves further exploration.
DR. MADIAS: You showed data on cardiac transplant patientsindicating that those receiving azathioprine had substantiallyhigher PRA levels than those receiving CsA. Could you review thedata on what happens to PRA in renal transplant recipients afterthey are converted from CsA to azathioprine?
DR. LEE: The effect of CsA on PRA in most studies isdocumented by comparing PRA in CsA-treated patients with thatin non-CsA (usually azathioprine)-treated patients. In a recentreport, 18 renal transplant patients were studied both before and16 weeks after conversion from CsA to azathioprine [104]. Plasmarenin concentration rose from 27.7 12.4 .tU/ml to 34.7 12.2U!ml before and after discontinuation of CsA, respectively. Thischange did not attain statistical significance, however.
DR. CLAUDIA LANDIS (Nephrology Section, VA Medical Center,West Los Angeles): My comment relates to the renin secretorypathway. Perhaps pro-renin is secreted constitutively and activerenin through the regulated pathway, and possibly CsA inhibitsonly the regulated secretory pathway, leaving the pro-renin secre-tory pathway intact. This could lead to the pattern of low activerenin and high pro-renin you find in the circulation of CsA-treatedpatients.
DR. LEE: The pro-renin that comes out of the Golgi apparatus

Nephrology Forum: CsA and the renin-angiotensin axis 257
is directed to one of the two secretory pathways: the regulatedpathway, which involves the processing of pro-renin to activerenin in the secretory granules prior to secretion, and the corlsti-tutive pathway through which pro-renin is secreted without pro-cessing. Evidence in extrarenal tissue also suggests that thecellular release of pro-renin utilizes the constitutive secretorypathway [1051. You have postulated a plausible explanation forthe peripheral renin profile in CsA-treated patients.
DR. MADIAS: Cyclosporine induces changes in a number ofother vasoactive substances, for example, endotheliri, nitric oxide,atrial natriuretic peptide, and the prostanoids. Could you com-ment on the contribution of these substances to the changes inrenin that you have described?
DR. LEE: As I mentioned, CsA affects a large number ofvasoregulatory agents, and each of these agents can interact withthe renin-angiotensin system. In this Forum I have tried to focusroy discussion on the possibility that, in addition to modulatingrenin activity indirectly through other vasoregulatory agents andmechanisms, CsA also can act directly on the renin-angiotensinaxis.
DR. MAmAs: You mentioned that ACE inhibitors and Ang IIreceptor antagonists ameliorate CsA-induced fibrosis. Might thisproperty be secondary, at least in part, to these drugs' effects onCsA metabolism?
DR. LEE: As I recall, Burdmann and associates did not addressthat possibility in their paper [361. However, I am not aware of anydata suggesting that the blockade of the RAS is associated with analteration in CsA metabolism.
DR. GLENN NAGAMI (Chief Nephrology Section, VA MedicalCenter, West Los Angeles): What is the evidence that cyclosporinedirectly alters renal cell components of the renin-angiotensinsystem such as angiotensinogen, renin, and ACE? Is there anyevidence that CsA alters the expression of angiotensin receptorsin the kidney?
DR. LEE: I believe that the most convincing evidence for a directeffect of CsA on renal renin metabolism is its stimulatory actionon renin synthesis and release in isolated juxtaglomerular cells[20]. I know of no data on the effect of CsA on intrarenal reninRAS outside the juxtaglomerular cells, but, as I mentioned, CsAdoes modulate AT1 receptor expression in the kidney [21, 28].
DR. CHARLES R. KLEEMAN (Nephrology Section, VA MedicalCenter, West Los Angeles): David, thank you for an excellentsynthesis of the information on cyclosporine and the renin system.Would you comment on the role of calcium on renin secretion? Ithought you said that a high calcium level stimulates reninsecretion.
DR. LEE: I meant that calcium-channel blockers increase reninsecretion. In general, it is believed that a low calcium levelstimulates renin secretion.
DR. KLEEMAN: yclosporine causes salt retention. You have notmentioned that important phenomenon in relation to the renin-angiotensin system and the development of high blood pressure.
DR. LEE: Thank you for pointing out that changes in sodiumbalance can both cause and be a consequence of changes in reninaxis activities. However, sodium retention as a cause of CsA-induced hypertension remains controversial [4]. 1 believe thepoint of your question is that CsA can cause changes in the reninaxis through multiple pathways and can induce hypertension andnephrotoxicity via many mechanisms. I agree with you. As I saidearlier, in this Forum I have focused my remarks on the possibilitythat CsA might act directly on the renin-angiotensin system, and
I raised the possibility that this action might constitute onecomponent in the pathogenesis of CsA-induced hypertension andnephrotoxicity.
DR. JOEL D. KOPPLE (Chief Division of Nephrology and Hyper-tension, Harbor/UCLA Medical Center, Los Angeles): Data suggestthat CsA also affects blood pressure by ways other than the RASsystem. Would you briefly comment on them?
DR. LEE: A host of agents and mechanisms have been proposedin the pathogenesis of CsA-associated hypertension [4, 14, 60].These include adrenergic hyperactivity, the vasoregulatory sys-tems such as the eicosanoids and the kinins, endothelium-derivedfactors, renal hemodynamics and function, and a direct vasculareffect of CsA.
DR. MAjIJAs: Does cyclosporine alter the vascular responsive-ness to Ang II?
DR. LEE: Cyclosporine potentiates the action of Ang II onvascular smooth muscle cells [64]; calcium entry blockade canprevent this CsA-induced hypersensitivity to Ang II [65].
DR. KOPPLE: What is known about the effect of CsA on cytosolicCa2, both in acute and chronic states?
DR. LEE: In general, CsA increases cytosolic Ca2 concentra-tion [Ca2 ] [106]. It is more difficult to explain the acute andchronic effects of CsA on intracellular [Ca2] without gettingdown to the specifics. Let us take the example of mesangial cells[107]. Pre-incubation with CsA caused a small but significantincrease in basal cytosolic [Ca2] and a marked, up to fourfold,increase in the vasoconstrictor-induced rise in peak levels and (inthe presence of external Ca) a more persistent post-peak elevationin cytosolic [Ca2]. The time-dependent changes in the responseof intracellular [Ca2] to CsA would be expected to depend onmultiple factors.
DR. MADIAS: A number of vasoactive substances, for example,angiotensin II, endothelin, and TGFI3, increase fibrosis by increas-ing the synthesis of extracellular matrix proteins. They also candecrease the degradation of collagen by inhibiting collagenaseactivity. Is there any evidence that CsA affects collagen degrada-tion?
DR. LEE: That is an interesting thought. I don't believe the ideahas been looked into in detail.
DR. NORIMOTO YANAGAWA (Associate Chief Nephrology Section,VA Medical Center, Sepulveda): You mentioned an interestingpossibility, specifically, that CsA initially activates the circulatingrenin-angiotensin system (eRAS) and later switches to activate thetissue renin-angiotensin system (tRAS). I guess this is whatunderlies the Pattern I and Pattern El responses to CsA, and Iwonder whether the trigger for this "switch" is the suppression ofactive renin conversion and/or secretion. Do you know whetherthe same mechanism occurs in other situations, such as in thechronic phase of renal artery constriction and in diabetes mellitus,where the Pattern II profile prevails?
DR. LEE: You have correctly pointed out that an evolution fromPattern 1, high plasma active renin and high plasma pro-renin, toPattern II, normal or low plasma active renin and high plasmapro-renin, peripheral renin profile has been observed in experi-mental renovascular hypertension and also has been proposed tooccur in experimental diabetes mellitus [55]. I would propose thatCsA acts on juxtaglomerular cell renin metabolism at three steps:(1) stimulation of pro-renin synthesis, (2) inhibition of pro-renin—active renin conversion, and (3) blockade of active reninsecretion. In short-term experimental studies, the action on step Iappears to predominate, giving rise to a Pattern I renin profile.

258 Nephrology Fonim: CsA and the renin-angiotensin axis
With more sustained or high-dose CsA treatment, the effect onsteps 2 and 3 overshadows that on step 1, while the constitutivepro-renin secretory pathway remains intact, thus giving rise to aPattern II renin profile. Plasma pro-renin might be furtheraugmented by pro-renin release from extrarenal tissues, whileplasma active renin can be further reduced by the renal vasocon-strictive effect of CsA with consequent sodium retention andvolume expansion.
DR. MADIAS: Low-renin essential hypertension is characterizedby disproportionately high levels of plasma aldosterone. Couldyou please comment on the effects of CsA on plasma aldosterone?
DR. LEE: Experimental studies suggest that CsA does not affectplasma aldosterone in the presence of a marked stimulatory effecton plasma active renin and pro-renin [16]. This lack of effect isattributed to the induction of a selective adrenal resistance to AngII, leaving the adrenal response to potassium and ACTH intact[16, 1081. In clinical studies, CsA has been reported to increase[109, 110], decrease [111, 1121, or cause no change [33, 113—115]in plasma aldosterone. Clearly, CsA-aldosterone interaction isanother complex area for further investigation.
ACKNOWLEDGMENTS
The author is grateful to both patients and their physicians, LindaGerrits, M.D. (Westlake Village, CA), Peter Hoagland, M.D. (San Diego,CA) and Elaine S. Kamil, M.D. (Los Angeles, CA) for their permission touse the clinical material presented in this Forum and for their assistancein the preparation of the manuscript. The author appreciates the collab-oration of Jack D. Bennett, Ph.D.; Peter H. Eggena, Ph.D; Ming-Shu Hu,M.D.; Nora J. Jamgotchian; Shamir Lustig, M.D.; and Harry J. Ward,M.D. This work was supported in part by grants from the VeteransAdministration, the American Heart Association (the Greater Los Ange-les Affiliate), and the National Kidney Foundation of Southern California.
Reprint requests to Dr. D.B.N. Lee (IJIR), 16111 Plummer Street,Sepulveda, California 91343, USA.
REFERENCES
1. MENDOZA SA, REZNIK VM, GRISWOLD WR, KRENSKY AM, Y0RGINPD, TUNE BM: Treatment of steroid-resistant focal segmental gb-merubosclerosis with pulse methylprednisobone and alkylating agents.Pediatr Nephrol 4:303—307, 1990
2. SCHWARTZ GJ, HAYCOCK GB, EDELMANN CM JR, SPITZER A: Asimple estimate of glomerular filtration rate in children derived fromthe body length and plasma creatinine. Pediatrics 58:259—263, 1976
3. MIHATSCH Mi, RYFFEL B, GUDAT F, THIEL G: Cyclosporine neph-rotoxicity, in Renal Pathology with Clinical and Functional Correla-tions, edited by TISHER CC, BRENNER BM, Philadelphia, Lippincott,1994, pp 1641—1681
4. MIMRAN A, MOURAD G, RIBSTEIN J, HALIMI J-M: yclosporin-associated hypertension, in Hypertension: Pathophysiology, Diagnosisand Management (2nd ed), edited by LARAGH JH, BRENNER BM,New York, Raven Press, 1995, pp 2459—2469
5. Kop JB, KLOTMAN PE: Cellular and molecular mechanisms ofcyclosporin nephrotoxicity. JAm Soc Nephrol 1:162—179, 1990
6. YADIN 0, GRIMM P, EYrENGER R: Renal transplantation in children:Clinical aspects, in Pediatric Nephrology, edited by HOILIDAY MA,BARRATr TM, AVNER ED, KOGAN BA, Baltimore, William &Wilkins, 1994, pp 1390—1418
7. GARDINER DS, WATSON MA, JUNOR BJR, BRIGGS JD, MORE IAR,LINDOP GBM: The effect of conversion from cyclosporin to azathio-prine on renin-containing cells in renal allograft biopsies. NephrolDial Transplant 6:363—367, 1991
8. MYERS BD, SIBLEY R, NEWTON L, TOMLANOVICH Si, Bosiiios C,STINSON E, LUETSCIIER JA, WHITNEY Di, KRASNY D, COPLON NS,PERLROTI 1 MG: The long-term course of cyclosporine-associatedchronic ncphropathy. Kidney mt 33:590—600, 1988
9. BERTANI T, FERRAZZI P, SCHIEPPATI A, RUBBENENTI P, GAMBA A,PARENZAN L, MECCA 0, PERICO N, IMBERTI 0, REMUZZI A, RE-
MUZZI G: Nature and extent of gbomerular injury induced bycyclosporine in heart transplant patients. Kidney mt 40:243—350, 1991
10. VERPOOTEN GA, WYBO I, PATrYN VM, HENDRIX P0, GIULIANO RA,NOD WEN EJ, ROELS F, DE BROE ME: Cyclosporine nephrotoxicity:Comparative cytochemical study of rat kidney and human allograftbiopsies. Clin Nephrol (suppl 1)25:S18—S22, 1986
11. Nirr K, FRIEDMAN AL, NICASTRI AD, PAIK S, FRIEDMAN EA:Granular juxtaglomerular cell hyperplasia caused by cyclosporine.Transplantation 44:417—421, 1987
12. SHEHATA M, NAHAS ME, BARKWORTH E, COPE GH, RAFTERY AT:Localization of PDGF-BB in the juxtaglomerular cells of cyclospor-me-treated rats. Exp Nephrol 3:173—179, 1995
13. MASON J, MULLER-SCHWEINITZER E, DUPONT M, CASELLAS D,MIHATSCH M, MOORE L, KASKEL F: Cyclosporine and the renin-angiotensin system. Kidney mt 39(suppl 32):S28—S32, 1991
14. LUKE RG, CURTIS JJ: Biology and Treatment of transplant hyper-tension, in Hypertension: Pathophysiology, Diagnosis and Management(2nd ed), edited by LARAGH JH, BRENNER BM, New York, RavenPress, 1995, pp 2471—2483
15. SIEGL H, RYFFEL B: Effect of cycbosporine on renin- angiotensin-aldosterone system. Lancet 2:1274, 1982
16. LUSTIG 5, STERN N, EGGENA P, TUCK ML, LEE DBN:Thc effect ofcyclosporinc A on blood pressure and renin-angiotensin-aldosteroneaxis in spontaneously hypertensive rats. Am J Physiol 253:H1596—H1600, 1987
17. CIRESI DL, LLOYD MA, SANDBERG SM, HEUBLEIN DM, EDWARDSBS: The sodium retaining effects of cyclosporine. Kidney mt 41:1599—1605, 1992
18. BAXTER CR, DUGGIN GO, HALL BM, HORVATH iS, TILLER DJ:Stimulation of renin release from rat cortical slices by cyclosporin A.Res Commun Pathol Pharmacol 43:417—423, 1984
19. LUSTIG 5, EGGENA P, BARREn' J, STERN N, LEE DBN: Furtherstudies on cyclosporine-induced hyperreninemic hypoaldosteronism:Evidence for a direct stimulatory action on renin release. Kidney mt33:274, 1988
20. KURTZ A, BRUNA RD, KUHN K: yclosporine A enhances reninsecretion and production in isolated juxtaglomerular cells. Kidney mt33:947—953, 1988
21. TUFRO-MCREDDIE A, GOMEZ RA, NORLING LL, OMAR AA, MOORELC, KASKEL FJ: Effect of CsA on the expression of renin andangiotensin type 1 receptor genes in the rat kidney. Kidney mt43:614—622, 1993
22. SHEHATA M, COPE GH, BARKWORTH E, RAFrERY AT, EL NAHASAM: The role of juxtagbomerular cells and growth factors in exper-imental cyclosporin nephrotoxicity (abstract). Nephrol Dial Trans-plant 9:919A, 1994
23. ANTONIPILLAI I, HOANG LE T, SOCENNEANTU L, HORTON R: Trans-forming growth factor-/3 is a renin secretagogue at picomolar con-centrations. Am Physiol Soc 265:F537—F541, 1993
24. NAFTILAN Ai, PRATT RE, DZAU Vi: Induction of platelet-derivedgrowth factor A-chain and c-myc expression by angiotensin II incultured rat vascular smooth muscle cells.JClin Invest 83:1419—1424,1989
25. STOUGGER GA, OWENS 0K: Angiotensin IT-induced mitogenesis ofspontaneously hypertensive rat-derived cultured smooth muscle cellsis dependent on autocrine production of transforming growth factor.Circ Res 70:820—828, 1992
26. GIBBONS GH, Prr RE, DZAU VJ: Vascular smooth muscle cellhypertrophy versus hyperplasia: Autocrine transforming growth fac-tor-f31 determines response to angiotensin II. J Clin Invest 90:456—461, 1992
27. ERMAN A, CHEN-GAL B, ZABLUDOWSKI J, ROSENFELD B: CyclosporinA treatment enhances angiotensin converting enzyme activity in lungand serum of rats. J Pharm Phumacol 42:525—5 27, 1990
28. REGITZ-ZAGROSEK V, AUCH-SCIIWELK W, HESS B, KLEIN U, DUSKEE, STEFFEN C, HILDEBRANDT AG, FLECK E: Tissue- and subtype-specific modulation of angiotensin II receptors by chronic treatmentwith cyclosporin A, angiotensin-converting enzyme inhibitors andAT1 antagonists. J C'ardiovasc Pharmacol 26:66—72, 1995
29. MYERS BD, ROSS iC, NEwtoN LD, LUETSCHER JA, PERLROTII MG:yclosporine-associated chronic nephropathy. N EngI J Med 311:699—705, 1984
30. HELD P, YUSUF 5, MATHIAS C, DHALIA N, THE0D0R0P0IJL05 S,

Nephrology Fonim: GsA and the renin-angiotensin axis 259
YACOUB M: Renin response to sympathetic stimulation in cyclospor-in-treated heart transplant patients. Am J Cardiol 63:1142—1144, 1989
31. BANTLE JP, NATH KA, SUTHERLAND DER, NAJARIAN JS, FERRIS TF:Effects of cyclosporine on renin- angiotensin-aldosterone system andpotassium excretion in renal transplant recipients. Arch Intern Med145:505—508, 1985
32. CLOZEL J-P, .FIsCHLI W: Cyclosporin-induced hypertension in mar-mosets: A new model of hypertension sensitive to angiotensin-converting enzyme inhibition. J Cardiovasc Pharmacol 14:77—81,1989
33. JULIEN J, FARGE D, KREFF-JAIS C, GUYENE T-T, PLOUIN P-F,HOUSSIN D, CARPENTIER A, CoRvoL P: Cyclosporine-induced stim-ulation of the renin-angiotensin system after liver and heart trans-plantation. Transplantation 56:885—891, 1993
34. BELLET M, CABROL C, SASSANO P, LEGER P, COR VOL P, MENARD J:Systemic hypertension after cardiac transplantation: effect of cyclo-sporine on the renin-angiotensin system. Am J Cardiol 56:927—931,1985
35. HEERING P, WESTHOFF A, BACH D, SPRENGER KBG, PASSLICK J,HELMCHEN U, GRABENSEE B: Renin-aldosterone system and renalfunction under cyclosporine A. Transplant Proc 20(suppl 3):556—562,1988
36. BURDMANN EA, AND0H TF, NAST CC, EVAN A, CONNORS BA,COFFMAN TM, LINDSLEY J, BENNETr WM: Prevention of experimen-tal cyclosporine-induced interstitial fibrosis by losartan and enalapril.Am J Physiol 269:F493—F499, 1995
37. HELMCHEN U, BACH D, ROHLAND C, GROENE H-i: Dissociation ofrenal renin content (RRC) and plasma renin content (PRC) incyclosporine A (CyA)-treated two kidney, one-clip hypertensive rats.Kidney mt 33:267, 1988
38. DUTZ JP, FRUMAN DA, BURAKOFF SJ, BIERER E: A role of cal-cineurin in degranulation of murine cytotoxic T lymphocytes. J Im-munol 150:2591—2598, 1993
39. HULTSCH T, ALBERS MW, SCHREIBER SL, HOHMAN RJ: Immunophi-lin ligands demonstrate common features of signal transductionleading to exocytosis or transcription. Proc Nati Acad Sci USA88:6229—6233, 1991
40. NORLING LL, TUFRO-MCREDDIE A, G0MEZ RA, MOORE LC,KASKEL FJ: Accumulation of acidic renin isoforms in kidneys ofcyclosporine-A-treated rats. JAm Soc Nephrol 7:331—337, 1996
41. OP5AHL JA, ABRAHAM PA, SHAKE JG, KATZ SA: Role of reninisoelectric heterogeneity in renal storage and secretion of renin. JAmSoc Nephrol 4:1054—1063, 1993
42. LEE J, MALVIN RL, JOKELAINEN PT: Blood pressure and acidic reninforms in stroke-prone hypertensive rats. Am J Physiol 257:F275—F279, 1989
43. SIEGL H, RYFFEL B, PETRIC R, SHOEMAKER P, MULLER A, Do-NATSCH P, MIHATSCH M: Cyclosporine, the renin-angiotensin-aldo-sterone system, and renal adverse reactions. Transplant Proc l5(suppl
1):2719—2725, 198344. SHAPIRO AP, RUTAN GH, THOMPSON ME, NIGALYE RL: Hyperten-
sion following orthotopic cardiac transplantation. Cardiovasc Clin20(2):179—188, 1990
45. NILSZPOREK T, GRZESZCZAK W, K0K0r F, ZUKOVSKA-SZCZEX-HOWSKA E, WIECEK A, KUSMIERSKI 5, SZKODNY A: Does the kind of
immunosuppressive therapy influence plasma renin activity, aldoste-rone and vasopressin in patients with a kidney transplant? mt UrolNephrol 21(2):223—240, 1989
46. REUDEIHUBER FL, MERCURE C, RAMLA D, METHOT D, PosrNovÀY: Molecular mechanisms of processing and sorting refill secre-tion, in Hypertension: Pathophysioloey, Diagnosis and Management(2nd ed), edited by LARAGH JH, BRENNER BM, New York, RavenPress, 1995, pp 1621—1636
47. BARGER AC: The Goldblatt memorial lecture. Part I: Experimentalrenovascular hypertension. Hypertension 1:447—455, 1979
48. OKAMURA T, MIYAZAKI M, INAGAMI T, TODA N: Vascular renin-angiotensin system in two-kidney, one-clip hypertensive rats. Hyper-tension 8:560—565, 1986
49. PETERS J, MUNTER M, HACKENTHAL E, MULLINS JJ, GANTEN D:Increased adrenal renin in transgenic hypertensive rats, TGR(m-REN2)27, and its regulation by cAMP, angiogensin II and calcium.J Clin Invest 91:742—747, 1993
50. MULLINS JJ, PETERS J, GANTEN D: Fulminant hypertension in
transgenic rats harbouring the mouse Ren-2 gene. Nature 344:541—544, 1990
51. JOHNSTON Cl, FABRIS B, JANDELEIT K: Intrarenal renin-angiotensinsystem in renal physiology and pathophysiology. Kidney mt 44(suppl42)S59—S63, 1993
52. MULLER-SCHwEINITZER E: Interaction of cyclosporine-A with therenin-angiotensin system in canine veins. Naunyn Schmiedebergs ArchPharmacol 340:252—257, 1989
53. RITZ E, FLISER D, N0wICKI M: Hypertension and vascular disease ascomplications of diabetes, in Hypertension: Pathophysiology, Diagno-sis and Management, (2nd ed), edited by LARAGH JH, BRENNER BM,New York, Raven Press, 1995, pp 2321—2334
54. ANDERSON A, JUNG FF, INGELFINGER JR: Renal renin- angiotensinsystem in diabetes: functional, immunohistochemical, and molecularbiological correlations. Am J Physiol 265:F477—F486, 1993
55. LUSH DJ, KING JA, FRAY JCS: Pathophysiology of low reninsyndrome: sites of renal renin secretory impairment of proreninovcrexpression. Kidney mt 43:983—999, 1993
56. LUETSCHER JA, KRAEMER FB, WILsON DM, SCHWARTZ HC, BRYER-ASH M: Increased plasma inactive renin in diabetes mellitus. Amarker of microvascular complications. N EnglJ Med 312:1412—1417,1985
57. FRANKEN AAM, DERKX FHM, MAN UB'T VELD, HOP WCJ, VANRuNS GH, PEPERKAMP E, DE JONG PTVM, SCHALEKAMP MADH:High plasma prorenin in diabetes mellitus and its correlation withsome complications. J Gun EndocrinolMetab 71:1008—1015, 1990
58. DZAU VJ: Possible prorenin activating mechanisms in the bloodvessel wall. J Hypertens 5(suppl 2):S15—S18, 1987
59. SEALEY JE, VON LUrrEROTITI N, RUBATrU 5, CAMPBELL WG JR,GAHNEM F, HALIMI J-M, LARAGH JH: The greater renin system. Itsprorenin-directed vasodilator limb: relevance to diabetes mellitus,pregnancy, and hypertension, in Hypertension: Pathophysiology, Diag-nosis and Management (2nd ed), edited by LARAGH JH, BRENNERBM, New York, Raven Press, 1995, pp 1889—1895
60. LEE DBN, NAKHOUL F, VON HUNGEN K, JAMGOTCHIAN N: Hyper-tensive and metabolic effects of cyclosporine, in Nephrology: Proc 4thAsian-Pacific Cong Nephrol, edited by ZANG J-H, DU X-H, LI0 A-H,LI L-S, Beijing, International Academic Publishers, 1991, pp 573—583
61. NAHMAN NS JR, Cosio FG, HENRY ML, FERGUSON RM: Cyclospor-inc nephrotoxicity in spontaneously hypertensive rats. Transplanta-tiOn 45:768—772, 1988
62. CLOZEL J-P, FISCHLI WM, MENARD J: Effects of the blockade of therenin-angiotensin system in cyclosporin-induced hypertension. J J-Jv-pertens 11:75—81, 1993
63. MOURAD G, RIBSTEIN J, MIMRAN A: Converting-enzyme versuscalcium antagonist in cyclosporine-treated renal transplants. KidneyInt 43:419—425, 1993
64. PFEILSCHIFTER J, RUEGG UT: yclosporin A augments angiotensinIl-stimulated rise in intracellular free calcium in vascular smoothcells. Biochem J 248:883—887, 1987
65. GOTZE 5, AUCH-SCHwELK W, BOSSALLER C, THELEN J, ELECK E:Calcium entry blockade may prevent cyclosporin A-induced hyper-sensitivity to angiotensin 11 and endothelial dysfunction in the rataorta. Eur Heart J 14(suppl I):104—110, 1993
66. CHAN DWS, LUSTIG 5, STERN N, EGGENA P, LEE DBN: Geneticsusceptibility to cyclosporin (CS)-induced hypertension (HTN): Re-lation to adrenal resistance to angiotensin (All). Kidney mt 33:293,1988
67. CI 101 KC, PARK YS, LEE J, BAlK YH: The effects of cyclosporine onvascular responsiveness and renin release from the kidney. Trans-plantation 53:1157—1160, 1992
68. TExroR SC, SMITH-POWELL L, TELLES T: Altered pressor responsesto NE and ANG tt during cyclosporinc A administration to con-scious rats. Am J Physiol 258:H854, 1990
69. JoSs DV, BARREn AJ, KENDRA JR, LUCAS CR, DESAI 5: Hyperten-sion and convulsions in children receiving cyclosporin A. Lancet1:906, 1982
70. TEXTOR SC, FORMAN SJ, BRAVO EL, CARLSON J: Dc novo acceler-ated hypertension during sequential cyclosporine and prednisonetherapy in normotensive bone marrow transplant recipients. Trans-plantProc 20(suppl 3):480—486, 1988
71. MIHATSCH MJ, THIEL G, RYFFEL B: Histopathology of cyclosporinenephrotoxicity. Transplantation Proc 20(suppl 3):759 —771, 1988
72. SHULMAN L, KNECHT A, BLAU A, RAPOPORT J: yclosporine directly

260 Nephrology Forum: GsA and the renin-angiotensin axis
induces proliferation of renal fibroblasts in culture. JAm Soc Nephrol4:759, 1993
73. WoLF G, KILLEN PD, NEILSON EG: Cyclosporine A stimulatestranscription and procollagen secretion in tubulointerstitial fibro-blasts and proximal tubular cells. JAm Soc Nephrol 1:918—922, 1990
74. GHIGGERI GM, ALTIERI P, OLEGGINI R, VALENTI R, GINEVRI F,PERFUMO F, GUSMANO R: yclosporine enhances the synthesis ofselected extracellular matrix proteins by renal cells in 'culture."Different cell responses and phenotype characterization. Transplan-tation 57:1382—1388, 1994
75. NAST CC, ADLER SG, ARTISHEVSKY A, KRESSER CT, AHMED K,ANDERSON PS: Cyclosporine induces elevated procollagen alpha 1(I)mRNA levels in the rat renal cortex. Kidney mt 39:631—638, 1991
76. MYERS BD, NEWTON L, BosI-IKos C, MACOVIAK JA, FRIST WH,DERBY GC, PERLROTH MG, SIBLEY RK: Chronic injury of humanrenal microvessels with low-dose cyclosporine therapy. Transplanta-tion 46:694—703, 1988
77. PERICO N, DETCI-IEVA A, KA1-IAUL El, REMUZZI G: Cyclosporineinduces glomerulosclerosis: three-dimensional definition of the lesionsof a rat model of renal transplant. Kidney mt 49:1283—1288, 1996
78. HEPTINSTALL RH: Anatomy of the Kidney, in Pathology of the Kidney(vol I, 3rd ed), edited by HEPTINSTALL RH, Boston, Little, Brown,1983, pp 1—60
79. DIEPERINK H, STARKLINT H, KEMP E, LEYSSAC PP: Comparativepathophysiology and histopathology of cyclosporine nephrotoxicity.Transplant Proc 20(suppl 3):785—791, 1988
80. FASEL J, KAISSLING B, LUDWIG KS, RYFFELL B, MIHATSCI-I Mi: Lightand electron microscopic changes in the kidney of Wistar ratsfollowing treatment with cyclosporine A. Ultrastruct Pathol 11:435—448, 1987
81. YOUNG BA, BURDMANN EA, JOHNSON RJ, ANDOH T, BENNETT WA,COUSER WG, ALPERS CE: Cyclosporine A induced arteriolopathy ina rat model of chronic cyclosporine nephropathy. Kidney mt 48:431—438, 1995
82. THLIVERIS JA, YATSCOFF RW, LUKOWSKI MP, COPELAND KR,JEFFERY JR, MURPHY GF: Chronic ciclosporin nephrotoxicity: arabbit model. Nephron 57:470—476, 1991
83. ZHUO J, ALCORN D, HARRIS P, MENDELSOHN FAO: Localization andproperties of angiotensin II receptors in rat kidney. Kidney mt44(suppl 42):S40—S46, 1993
84. BOHMAN S-O: The ultrastructure of the renal medulla and theinterstitial cells, in The Renal Papilla and Hypertension, edited byMANDAL AK, BOHMAN S-O, New York, Plenum, 1987, p 7
85. WOLF G, NEILSON EG: Arigiotensin II as a renal growth factor. JAmSoc Nephrol 3:1531—1540, 1993
86. JOHNSON Ri, ALPERS CE, YOSHIMURA A, LOMBARDI D, PRITZL P,FLOEGE J, SCHWARTZ S: Renal injury from angiotensin H-mediatedhypertension. Hypertension 19:464—474, 1992
87. YOUNG BA, BURDMANN EA, JOHNSON Ri, ALPERS CE, GIACHELLICM, ENG E, ANDOH T, BENNETT WM, COUSER WG: Cellularproliferation and macrophage influx precede interstitial fibrosis incyclosporine nephrotoxicity. Kidney mt 48:439—448, 1995
88. KANETO K, MORRISSEY J, MCCRACKEN R, REYES AA, KLAHR 5:Osteopontin expression in the kidney during ureteral obstruction(abstract). JASIV 5:784, 1994
89. GIACHELLI CM, PICHLER R, LOMBARDI D, DENIIAWF DT, ALPERSCE, SCHWARTZ SM, JOHNSON RJ: Elevated osteopontin expressionmarks angiotensin 11-induced renal tubulointerstitial injury and iscorrelated with sites of monocyte/macrophage accumulation. Kidneyfnt 45:515—524, 1994
90. THOMSON AW, MCAUIEY FT, WHITING PH, SIMPSON JO: Angioten-sin-converting enzyme inhibition or aldosterone antagonism reducescyclosporine nephrotoxicity in the rat. Transplant Proc 19:1242, 1987
91. LAFAYE-I-I'E RA, MAYER 0, MEYER TW: The effects of bloodpressure reduction on cyclosporine nephrotoxicity in the rat. J AmSoc Nephrol 3:1892—1899, 1993
92. GILLUM DM, TRUONG L: Effects of chronic volume expansion andenalapril on chronic cyclosporine nephropathy. Am J Physiol 258:F934—F939, 1990
93. KURTZ A: Cellular control of renin secretion. Rev Physiol BiochemPharmacol 113:2—40, 1989
94. RASMUSSEN H: The calcium messenger system. N Engi J Med314:1094—1101, 1164—1 170, 1986
95. MORGANTI A, PELIZZOLA D, MANTERO F, GAZZANO G, OPOCHER G,PIFFANELLI A: Immunoradiometric versus enzymatic renin assay:results of the Italian Multicenter Comparative Study. J Hypertens13:19—26, 1995
96. SEALEY JE, TRENKWALDER P, GAHNEM FM, CATANZARO D, LARAGHJH: Plasma renin methodology: inadequate sensitivity and accuracyof direct renin assay for clinical applications compared with tradi-tional enzymatic plasma renin activity assay. J Hypertens 13:27—30,1995
97. CURTIS JJ: Hypertension after renal transplantation: cyclosporineincreases the diagnostic and therapeutic considerations. Am J KidneyDis 13(suppl 1):28—32, 1989
98. MURRAY BM, VENUTO RC, K0HLI R, CUNNINGHAM EE: Enalapril-associated acute renal failure in renal transplants: possible role ofcyclosporine. Am J Kidney Dis 16:66—69, 1990
99. SAWAYA B, PROVENZANO R, KUPIN WL, VENKAT KK: Cyclosporine-induced renal microangiopathy. Am J Kidney Dis 12:534—537, 1988
100. SCHREIBER SL, CRABTREE GR: The mechanism of action of cyclo-sporin A and FK506. Immunol Today 13:136—142, 1992
101. MCDONALD ML, ARDITO T, MARKS WH, KASHGARIAN M, LORBERMI: The effect of cyclosporine administration on the cellular distri-bution and content of cyclophilin. Transplantation 53(2):460—466,1992
102. FRIEDMAN J, WEISSMAN I, FRIEDMAN J, ALPERT S: An analysis of theexpression of cyclophilin C reveals tissue restriction and an intriguingpattern in the mouse kidney. Am J Pathol 144(6):1247—1256, 1994
103. OTSUKA M, TERADA Y, YANG T, NONOGUCHI H, TOMITA K, MA-RUMO F: Localization of cyclophilin A and cyclophilin C mRNA inmurine kidney using RT-PCR. Kidney mt 45(5):1340—1345, 1994
104. VAN DEN DORPEL MA, VAN DEN MEIRACKER AH, LAMERIS TW,B00M5MA F, LEVI M, MAN IN 'T VELD AJ, WEIMAR W, SCHALEKAMPMADH: Cyclosporin A impairs the nocturnal blood pressure fall inrenal transplant recipients. Hypertension 28:304—307, 1996
105. POISNER AM: Regulation of utero-placental prorenin. Adv Exp MedBiol 377:411—426, 1995
106. SKORECKI KL, RUTLEDGE WP, SCHRIER RW: Acute cyclosporinenephrotoxicity—prototype for a renal membrane signalling disorder.Kidney mt 42:1—10, 1992
107. GOLDBERG Hi, WONG PY, COLE EH, LEVY GA, SKORECKI KL:Dissociation between the immunosuppressive activity of cyclosporinederivatives and their effects on intracellular calcium signalling inmesangial cells. Transplantation 47:731—733, 1989
108. STERN N, LUSTIG 5, PETRASOK D, JENSEN G, EGGENA P, LEE DBN,TUCK ML: Cyclosporin A-induced hyperreninemic hypoaldosteron-ism. A model of adrenal resistance to angiotensin II. Hypertension9(suppl 3):11131—11135, 1987
109. CUGINI P, BA-r-i-ISTI P, DI PALMA L, CAVALLINI M, P0zZILLI P,SCIBILIA G, LETIZIA C, CASSISI A, CI0LI AR, MARINO B, ET AL:Secondary aldosteronism documented by plasma renin and aldoste-rone circadian rhythm in subjects with kidney or heart transplanta-tion. Renal Fail 14(1):69—76, 1992
110. CUGINI P, LUCIA P, SCIBILIA G, Di PALMA L, CI0LI AR, MARINO B,CIANETFI A, GASBARRONE L, CANOVA R: Twenty-four-hour patternof atrial natriuretic peptide in heart transplantation: evidence forlack of circadian rhythm. Temporal interrelationships with plasmarenin activity, aldostcrone and cortisol. mt J Gardiol 1:7—14, 1993
111. JONES JW, GRUESSNER RW, GoRIs PF, MATAS AJ: Flypoaldoste-ronemic hyporeninemic hyperkalemia after renal transplantation.Transplantation 56(4):1013—1015, 1993
112. TEXTOR SC, WILSON DJ, LERMAN A, ROMERO JC, BURNETT JC JR,WIUSNER R, DtCKSON ER, KROM RA: Renal hemodynamics, urinaryeicosanoids, and endothelin after liver transplantation. Transplanta-tion 54:74—80, 1992
113. FORSLUND T, HANNONEN P, REITAMO 5, FYHRQUIST F: Hypertensionin cyclosporin A-treated patients is independent of circulating endo-thelin levels. J Intern Med 238(1):71—75, 1995
114. AGIJILERA S, DERAY G, DESJOBERT H, BENHMIDA M, Le HOANG P,JACOBS C: Effects of cyclosporine on tubular acidification function inpatients with idiopathic uveitis. Am J Nephrol 12:425—430, 1992
115. BALLARDIE FW, EDWARDS BD, HowS J, JONES L, PETERS AM:Disturbance in renal haemodynamics and physiology in bone marrowtransplant recipients treated with ciclosporin A. Nephron 60(1):17—24, 1992