CYANOTIC CONGENITAL HEART · CYANOTIC CONGENITAL HEART DISEASE By JAMES W. BROWN, M.D., F.R.C.P....
20
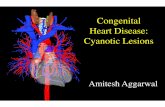
.-51.I CYANOTIC CONGENITAL HEART DISEASE By JAMES W. BROWN, M.D., F.R.C.P. Physician, General Hospital, Grimsby, and Grimsby and Lindsey Rheumatism and Heart Clinics The last 15 years have witnessed a very re- markable change in the attitude of the clinician towards cyanotic congenital heart disease. It is within the memory of many that it was the custom to make a simple diagnosis of congenital heart abnormality with cyanosis, and express the opinion that little or nothing could be done about it. Then there appeared the pioneer work of Abbott and others which produced not only a classification of the various abnormalities, but furnished a mass of clinical and postmortem observations from which it was possible to build up a clinical picture and so arrive at a reasonably correct anatomical diagnosis. At the same time knowledge of the natural history of congenital heart disease has also increased, and some idea of its prognosis has been ascertained. Lastly, the conception of Taussig that an in- adequate pulmonary blood supply was the critical abnormality in many cyanotic cases, and the de- velopment of an anastomotic operation between the systemic and pulmonary circulations so as to furnish an artificial ductus arteriosus, by Blalock FIG. i.-Tetralogy of Fallot. Female aged 3 years. subvalvular stenosis. of the pulmonary artery. into it behind the crista supraventricularis. Right ventricle opened. An arrow marks the Ventricular septal defect with probe passing by copyright. on March 19, 2021 by guest. Protected http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.25.289.511 on 1 November 1949. Downloaded from
Transcript of CYANOTIC CONGENITAL HEART · CYANOTIC CONGENITAL HEART DISEASE By JAMES W. BROWN, M.D., F.R.C.P....

.-51.I
CYANOTIC CONGENITAL HEART DISEASEBy JAMES W. BROWN, M.D., F.R.C.P.
Physician, General Hospital, Grimsby, and Grimsby and Lindsey Rheumatism and Heart Clinics
The last 15 years have witnessed a very re-markable change in the attitude of the cliniciantowards cyanotic congenital heart disease. It iswithin the memory of many that it was the customto make a simple diagnosis of congenital heartabnormality with cyanosis, and express the opinionthat little or nothing could be done about it. Thenthere appeared the pioneer work of Abbott andothers which produced not only a classification ofthe various abnormalities, but furnished a mass ofclinical and postmortem observations from which
it was possible to build up a clinical picture and soarrive at a reasonably correct anatomical diagnosis.At the same time knowledge of the natural historyof congenital heart disease has also increased, andsome idea of its prognosis has been ascertained.Lastly, the conception of Taussig that an in-adequate pulmonary blood supply was the criticalabnormality in many cyanotic cases, and the de-velopment of an anastomotic operation between thesystemic and pulmonary circulations so as tofurnish an artificial ductus arteriosus, by Blalock
FIG. i.-Tetralogy of Fallot. Female aged 3 years.subvalvular stenosis. of the pulmonary artery.into it behind the crista supraventricularis.
Right ventricle opened. An arrow marks theVentricular septal defect with probe passing
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

5ta POSTGRADUATE MEDICAL JOURNAL November i949
.....*::. ...
.S:n .'}: ..:. ..: :..
........
..:a:M :i .i..:..
S: :^!::: .. .:.:fir..':i ... ...
Wilti... . ...8 .... ...
.. -:::.:....: .... :...
t. ..sy .....i....
. ,̂. ;.........
:.s,'.'S:....... .... ...
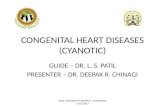
FIG. 2.-Tetralogy of Fallot. Female aged 3 years. Left ventricle opened. A largeaorta lies astride a high ventricular septal defect.
and Taussig (1945), has entirely revolutionized ouroutlook on the treatment of the cyanotic case.The assessment by Campbell (1948) that only onein two cyanotic children is likely to reach the ageof 7 years, only one in four to reach the age of I4,and less than one in ten to reach the age of 2I,certainly justifies an operation even if its risks areconsiderable. It is all we have to offer to a patientwho may exist rather than live. Accordingly, eachcase that presents itself should be fully investigatedwith a view to an accurate anatomical diagnosis, sothat its suitability for operation may be considered.The investigation demands well-planned teamwork between the cardiologist, surgeon, radiologistand clinical pathologist. Important contributionsare made by all of these towards the elucidation ofthe case both in regard to diagnosis and treatment.Highly specialized technical work is involved inboth cardiac catheterization and angiocardio-graphy. The pioneer work of Cournand (I949) in
cardiac catheterization and its development byothers, together with numerous studies in angio-cardiography have made it possible to observephysiological alterations in the living patient, andso furnish important diagnostic information.There was a time when cyanotic congenital heart
disease was considered to be uncommon, and it wascertainly rare in individual experience. The pub-licity in connection with operation for blue babieshas literally brought to light many cases that haveremained sheltered in their homes, incapable ofany sustained activity and so incapacitated thatsome have not even walked. Many, but not all, ofthe children are underdeveloped. Some are re-tarded mentally because they have not had theopportunities for education afforded to theirnormal fellows. All are the subjects of greataffection from their parents, and it is peculiar thatboth parents usually accompany the child to theout-patient department.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November i949 BROWN: Cyanotic Congenital Heart Disease 513
FIG. 3.-Pulmonary atresia. Female aged 4 years. (a) Posteroanterior. (b) Left anterior oblique.
The Approach to the Cyanotic CaseThe obvious presenting sign is cyanosis which
may be of all degrees. It is most necessary toenquire carefully as to the first appearance ofcyanosis. It may have existed since birth or havedeveloped subsequently. Extreme cyanosis atbirth usually denotes a severe abnormality, oftenincompatible with prolonged existence. It isusually in the nature of a transposition of thevessels with a closed septum, a severe pulmonaryatresia without a patent ductus arteriosus, or apulmonary atresia with extreme dextroposition ofthe aorta. Moderate and obvious cyanosis frombirth is the most usual finding, the cyanosis be-coming more marked as age advances. Only asmall percentage of cases develop cyanosis at thetransition between the vegetative stage of infancyand the more active stage that follows it. Cyanosisappearing at puberty or in later childhood suggeststhe Eisenmenger anomaly, or pulmonary stenosiswith a patent foramen ovale. Cyanosis appearingfor the first time in the late teens or early 20'Sbrings t6 mind the auricular septal defect and israrely very marked. Isolated pulmonary stenosiswith a closed septum may also show cyanosis atthis time from changes that have occurred in thesmaller pulmonary vessels. Lastly, the duration
of cyanosis may have some bearing on thediagnosis. If it has existed in any marked degreesince birth, growth and nutrition are likely to bebelow average. In older children the presence orabsence of clubbing furnishes an important clueas to its duration. Recent cyanosis with noclubbing may be due to the simple reversal of ashunt from extracardiac causes such as pulmonaryinfection, and is unaccompanied by polycythaemia.Cyanosis may develop as a permanency in the latestages of a patent ductus arteriosus, auricular septaldefect, or ventricular septal defect in response topulmonary vascular changes and pulmonaryhypertension.
Anatomical Factors in CyanosisMost cases of cyanotic congenital heart disease
present two basic developmental disturbances tocause cyanosis. Firstly, there is stenosis of somepart of the pulmonary tract, in either conus, valveor artery, so that an insufficient volume of bloodreaches the lungs for oxygenation. It is this factorwhich is capable of surgical modification and it istowards its detection, and the estimation of itsseverity, that our efforts must be directed.Secondly, there may be a shunt of mixed bloodinto the aorta which commonly overrides a high
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

5I4 POSTGRADUATE MEDICAL JOURNAL November I949
F2 9
FIG. 4.-Tetralogy of Fallot. Right aortic arch.Female aged 2I years recently delivered of a normalchild.
A entricular septal defect, or perhaps the ventricularseptum is absent in the functional sense. Thisfactor in cyanosis cannot be remedied. It is avariable factor partially depending upon the extentto which the dextroposed aorta overrides theseptum and right ventricular cavity, and theseverity of the pulmonary stenosis. Severe pul-monary stenosis prevents the rapid passage ofblood into the pulmonary artery during systole sothat a large volume of venous blood is diverted intothe aorta. Slighter degrees of pulmonary stenosisallow the more easy passage of blood into thepulmonary artery and a corresponding diminutionin the volume shunted into the aorta. Exercise,which increases the cardiac output, at the sametime must increase this shunt for the narrowedpulmonary artery cannot utilize this augmentedblood flow. Thus cyanosis may be minimal atrest and increases with exertion. In some casesthe only indication that exists of such a shunt isa reduction in the oxygen saturation of arterialblood, insufficient to cause clinical cyanosis.There are other shunts and other factors whichmay contribute to, or emphasize already existingcyanosis, but they will not be considered in anydetail here. Mention should be made that intransposition of the vessels the pulmonary bloodsupply is adequate and the main difficulty is insecuring a return of the oxygenated blood to thesystemic circulation. In certain abnormalities and
in polycythaemia there may be important changesin the pulmonary capillaries and endothelium,which prevent the blood from being properlyoxygenated.
Physiological FactorsA detailed discussion of the physiological
mechanisms involved in cyanosis will not beattempted here. Only its general effects andcomplications will be mentioned. Cyanosis maybe due to anoxaemia from any cause and impliesthe presence of at least 5 gm. reduced haemo-globin in the peripheral blood. Persistent cyanosisover a period of time results in polycythaemia andclubbing, the former being an effort by the bodyto increase its oxygen carrying capacity and adaptitself to the anoxaemia. Polycythaemia has im-portant implications, and although accompaniedby clubbing is unaccompanied by enlargement ofthe spleen. Red cell counts of seven or eightmillion are common and the level of haemoglobinis correspondingly raised above ioo per cent. Arising red cell count is of bad prognostic signifi-cance. A falling count, due to anaemia, is also abad sign because it means a lower oxygen capacityof the blood, although the patient may look muchbetter and less cyanosed as a result of this. Poly-cythaemia has the attendant dangers of thrombosis,cerebral thrombosis with hemiplegia occurring attimes. Severe polycythaemia may also inducechanges in the pulmonary capillaries and endo-thelium, or cause areas of infarction in the lung.All these conditions interfere with adequateoxygenation. There is also the risk of cerebral
FIG. 5.-Tetralogy of Fallot. Female aged 6 vears.Marked right axis with z to I block.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease 5I5
abscess in the cyanotic case where a large volumesof blood does not reach the lung and so escapesthe filter of the pulmonary endothelium. Theposition of the aorta over a septal defect is afavourable circumstance for this to occur.
Laboratory ExaminationsThe recent work in cardiac catheterization and
blood analysis has materially increased ourknowledge and has greatly assisted diagnosis.Estimation of the arterial oxygen saturation of theblood is an important and informative examination.It should be done with the subject at rest and afterexercise. In severe pulmonary stenosis or atresiathe oxygen saturation may be as low as 20 per cent.In cases with a higher oxygen saturation theremay be a marked and rapid fall on slight exertion,and if this occurs it means a severe stenosis withpoor pulmonary circulation. In less severe casesthere may be a level of 70 per cent. oxygensaturation which hardly falls on exercise, con-firming that the pulmonary stenosis is not ofmarked degree. Lastly, an estimation of arterialoxygen saturation reveals the presence of reduced
014
FIG. 6.-Eisenmenger complex. Female aged 24 years.Infective arteritis of pulmonary artery.
4..
.
FIG. 7.--The Eisenmenger complex. Pulmonary ar-tery enlarged and the aorta.lying astride a highventricular septal defect.
haemoglobin in the circulating blood in an amountinsufficient to produce clinical cyanosis in someabnormalities where a venous arterial shunt is ofimportance.The measurement of pressures within the
cardiac cavities and pulmonary artery, and themovements of the catheter itself within the hearthave also furnished much valuable information.These techniques are discussed in another paperand will not be entered into here. Although thesemethods have the greatest possible value, theimpression should not be formed that it is im-possible to make a diagnosis without them. Thepioneer work of Blalock and Taussig was largelydone without these highly specialized aids todiagnosis, their reliance being placed on clinicalobservation and radiological examination.
Types of Congenital Heart Disease withCyanosisIt is impossible to describe every type of con-
genital heart disease with cyanosis within thecompass of this paper. Only certain anomalieswill be described and these are mainly those thatrmay derive benefit from surgery. They are notarranged in order of severity of cvanosis, as every
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL November I949
FIG. 8.-The Eisenmenger complex. Male aged I 2years. Incipient cyanosis. Marked right axis inelectrocardiogram.
case within a group m7y vary, but are arranged inthe order of their frequencv from the author'sexperience.
(i) Tetralogy of Fallot (pulmonary stenosis,ventricular septal defect, overriding aorta andright ventricular hypertrophy).
(2) Eisenmenger complex (ventricular septaldefect witE overriding aorta and normal or dilatedpulmonary artery).
(3) Isolated pulmonary stenosis (pulmonarystenosis with or without a patent foramen ovale).
(4) Tricuspid atresia.(5) Transposition of the great vessels.(6) Persistent truncus arteriosus.(7) Single ventricle with diminutive outlet
chamber.
The Tetralogy of FallotThe tetralogy of Fallot is by far the commonest
type of congenital heart disease and accounts forabout 75 per cent. of cyanotic cases surviving in-fancy. The anatomical findings, which are variablefrom case to case within considerable but definedlimits, are stenosis or atresia of the pulmonary
.rE,
;.
20;-'4
- '; A
FIG. 9 -Pulmonary stenosis with patent foramen ovale.Male aged I 5 years.
artery, a high ventricular septal defect, dextro-position of the aorta so that it overrides the septaldefect, and hypertrophy of the right ventricle, alogical sequence of these structural abnormalities(Figs. i and 2). The pulmonary stenosis may beat almost any point in the pulmonary tract andmay be valvular, infundibular or both, the arterydistal to the stenosis being generally hypoplastic.In severe atresias the trunk of the pulmonary arterymay be reduced to an impermeable fibrous cordending blindly in the ventricle. Sometimes theremay be just sufficient blood flow through a stenoticvessel to maintain life, and the ductus and foramenovale may be closed. Where there is anatomical orfunctional atresia a pulmonary circulation ismaintained through a patent ductus arteriosus andalso by means of a collateral circulation developedthrough the bronchial and other arteries. Thesetwo different types of pulmonary circulation haveled some to classify pulmonary atresia as a distinctsyndrome from a functional point of view. Attimes the dextroposition of the aorta is so markedthat the aorta may arise wholly from the rightventricle. Occasionally, transposition of thevessels also occurs and the stenosed pulmonaryartery arises from the left ventricle. In at least afifth of the cases there is a right aortic arch withthe aorta crossing the right bronchus.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease 517
The physiological results of this combination ofstructural abnormalities is that, firstly, a largevolume of blood from both ventricles passesdirectly into the aorta, the proportions of venousand arterial blood being to some extent determinedby the position of the dextroposed aorta vis-a-visthe higher septal defect and right ventricularcavity; secondly, an inadequate volume of bloodreaches the lungs for oxygenation through thestenosed pulmonary tract, or through a patentductus arteriosus. The severity of pulmonarystenosis naturally influences the volume of bloodthat can reach the lungs for oxygenation and con-sequently there are variations from case to case inregard to the onset and degree of cyanosis. Slightstenosis of the pulmonary artery may well becompatible with life with relatively small handicap,and cyanosis appearing first in response to exertion,often is not marked until late childhood. Insevere pulmonary stenosis amounting to functionalatresia the main blood supply to the lungs may bethrough a patent ductus arteriosus and corres-pondingly early and marked cyanosis is likely.Clearly the severity of the pulmonary stenosis andits consequent effects upon the pulmonary circula-tion determines the survival of the patient and itbecomes necessary to distinguish, as far as possible,between those cases with pulmonary atresia,actual or functional, and those with pulmonarystenosis of lesser degree. The patient with pul-monary atresia is at the mercy of his patent ductusarteriosus. Should this close, and it may closespontaneously early or late, there is a markeddeterioration in his condition and death may result.
Clinical PictureMarked cyanosis from birth and clubbing of the
fingers in a child or young adult at once suggeststhe tetralogy as a probable diagnosis on the basisof survival alone. Cyanosis may not necessarilybe clinically apparent at birth and may only appearwhen the child becomes active, or when the ductuscloses. Once it appears it becomes permanent andprogressive and it is accompanied by dyspnoea onthe least exertion so that activity is strictly limited.Clubbing is proportional to the degree of cyanosis.It is a curious fact that most cyanotic childrenwhen suffering from dyspnoea assume a squattingposition which enables them to breathe moreeasily. The child sits on his heels with the kneesdrawn up to his chest and may even sleep in thisattitude. Spontaneous attacks of paroxysmaldyspnoea with intense cyanosis and difficulty inexpiration sometimes occur in young children andare a potential cause of sudden death.The heart is not enlarged. Some deformity of
the left chest from right ventricular hypertrophyoccurring at an early age may be present and there
is frequently a basal systolic thrill and accom-panying systolic murmur. The murmur isgenerally not heard in the neck but is heard alongthe left sternal margin. The systolic murmur iscaused by the pulmonary stenosis and is oftenabsent in pulmonary atresia. The pulmonarysecond sound is usually unaltered.
RadiologyThe heart is not enlarged and there is a con-
cavity at the site of the pulmonary arc (Figs. 3 and4). In the left anterior oblique view there is en-largement of the right ventricle which projects
Xffl1 = ';1 - = - :c;-^ t - - $ Aw - $| ., .| l . |F \ \ *- - + 4-
l | b ^ ||l t w Cl - - ^ +.%P - # l ! i w - t- - - - - w -. M ^ - .. . -F - - - e. - ^ - F-- w w -. F.
- rs- - "1 --
1; | ! . -- r - - -
r - e - X - - . -.1o v . . ..+.. .. .. ... e ... .. i.,.t i t - - wW i ll - o. b +3f > . .. .>. . . * . t -ffX e .f
H wE rXg i
E ET Fgg fgg.-e meg E--i::-L:i::1::i:§: } i- t--/ (--et
gW;gr aTrX at- t;i###X WelE t-+;+;.F..-:.H-,7Tq
FFFffFHT
FIG. io.-Pulronary atresia with closed ventricularseptumand patent foramen ovale. Collateralbronchial artery circulation. Marked right ven-tricular hypertrophy. Tall P waves.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

5I8 POSTGRADUATE MEDICAL, JOURNAL November I949
mgX
0.... ,... ........................................................... .. ... . ....;........-o.............
.-.
....................................................0.....
...........
.......iE-
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease 519
IM.
:::::^.....:..
-".5 cn
D)-
0-)
-e .-.4
--E.
>C0)
Q 0)
07co)
to.
rCA
0)
* .0)
0 4-
Co i-s-
Cot
.-).
4-
,..
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

520 POSTGRADUATE MEDICAL JOURNAL November I949
FIG. I3a.-Tricuspid atresia. Female aged 2i years.
towards the anterior wall of the chest. There isan unusually clear pulmonary window. The hilarshadows are smaller than normal owing to thereduced pulmonary circulation, and on the screenpulsation is not evident. Where there is a col-lateral circulation the hilum has a peppered appear-ance due to numerous small vessels. The lungfields are abnormally clear. In about a fifth ofthe cases there is a right aortic arch.
ElectrocardiogramMarked right axis is the rule. The P waves are
often tall and peaked in lead 2. Conductionabnormalities are rare (Fig. 5).
DiagnosisThe tetralogy of Fallot is the commonest
anomaly found in children who survive infancy.The history of cyanosis appearing at birth or in theneonatal period, together with polycythaemia andclubbing gives a good diagnostic lead. Thediagnosis is essentially radiological and thecharacteristic silhouette shows no enlargement ofthe heart as a whole, a concave pulmonary arc anda blunt turned up apex. The aortic window isabnormally clear and there are ischaemic lungfields with small hila and absent hilar pulsation.Catheterization shows an increased pressure in the
FIG. I 3b.-Tricuspid atresia. Female aged 2 years.Left anterior oblique view shows enlargement ofthe left ventricle. E.C.G. left axis.
right ventricle and a diminished pressure in thepulmonary artery. Final proof can be obtainedfrom the angiocardiographic picture. The mostdifficult differential diagnosis is from transpositionof the vessels, or from a persistent truncus ar-teriosus. In transposition with a ventricular septaldefect the heart is enlarged, the aortic window isnot clear and there are congestive changes in thelung fields. In addition the vascular pedicle isnarrow and widens as the patient is rotated to theoblique view. The persistent truncus shows anabnonnally broad aorta and a narrow pedicle inthe oblique view.
The Eisenmenger ComplexThe Eisenmenger complex consists of an inter-
ventricular septal defect with an overriding aortaand a normal or dilated pulmonary artery (Figs.6 and 7). There is no deficit in the pulmonarycirculation. Cyanosis is apt to occur and it is notknown whether this is consequent upon secondarychanges in the lungs due to the large volume ofblood that flows to them, or due to a congenitalabnormality of the alveolar endothelium prevent-ing proper oxygenation. There is always a shuntof venous blood into the aorta and its volumevaries, depending upon the position of the aortain regard to the ventricular septal defect. It must
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November 1949 BROWN: Cyanotic Congenital Heart Disease
be very rare for this shunt alone to cause visiblecyanosis.
Clinical FeaturesCyanosis is usually absent until late childhood or
adolescence and in childhood the patient is notseverely incapacitated. The late development ofcyanosis, which increases gradually, with theappearance of symptoms of dyspnoea and tired-ness, is quite characteristic of the Eisenmengeranomaly. Clubbing is rarely marked. Haemop-tysis occurs occasionally. The heart is slightlyenlarged and there is a loud systolic murmur in thepulmonary area and in the third and fourth leftintercostal spaces. Quite often there is a diastolicmurmur and this may be due to either relativepulmonary incompetence or to aortic incom-petence. The latter is due to a frequentlyassociated abnormality of the aortic cusps. Thepulmonary second sound is accentuated.
RadiologyThe cardiac silhouette is variable in appearance
depending upon the size of the pulmonary artery.There is always prominence of the pulmonary arc,and large pulsating pulmonary branches (Fig. 8).The right side of the heart is enlarged and veryoccasionally there may be the coeur-en-sabotappearance. Where the pulmonary artery isgrossly enlarged the cardiac silhouette is identicalwith that of an auricular septal defect.
LA 11 ietX -+.
-.....-. .
z~~ ~ ~ ~ ~ ~......-......-.-t t-t .
z... ............
FIG. 14.-Tricuspid atresia. Cyanotic child aged 2years. Left axis.
ElectrocardiogramThe electrocardiogram is almost invariably
found to show a right axis and large P waves areusual.
DiagnosisIn no other congenital abnormality is the
diagnosis more frequently missed. This is per-haps due to failure in remembering the existenceof the anomaly, or perhaps because in acyanoticcases the physical signs, particularly if there is adiastolic murmur, bear a superficial resemblanceto those of rheumatic aortic valvular disease.Aortic stenosis can usually be differentiated by itssmall pulse pressure and the absence of anyrheumatic history. The isolated ventricular septaldefect may also present somewhat similar physicalsigns but, in this case, the heart is not enlargedand the pulmonary arc is never as prominent as inthe Eisenmenger anomaly. The greatest difficultyis in connection with the auricular septal defectwhere the radiological picture may be identical.Basal systolic murmurs and thrills occur in bothconditions. The circulation time is markedlyshortened in the Eisenmenger type owing to theoverriding aorta. The oxygen saturation of thearterial blood is always lowered and oxygen in-halation will not raise it to a normal figure owing tothe venous arterial shunt. Angiocardiography willdemonstrate the presence of an overriding aortaby simultaneous visualization of both aorta and
A
-~~~ ~ ~ . . . . .
I I Ii iiiC--i-i I -~-
F.l:T I T .I ..lII--- a- FII:I- - .(
I-rIIIl- .:-I--l
lft
f - -
FIGYXIS.-Tricuspid atresia. Male aged 12 years.Left axis.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

522 POSTGRADUATE MEDICAL JOURNAL November I949
..EI- ............. . ......
-:.. R........... ii .....-
=. ......-iP -'a J - --! --
..-
-~ ~ ~ ~-...- .. - .
...........
-. --r-....-,...
.....- .... ...
......... 7! ---
-. :......
FIG. i6.-Female aged 7 months with tricuspid atresia.Cyanosis and normal axis in electrocardiogram.
pulmonary artery. Measurements of intracardiacpressures are of great value, as also in othercyanotic cases where the differentiation from thetetralogy may be in question. Pulmonary arterypressure is always raised in the Eisenmenger typeand abnormally low in the tetralogy. In a markedlycyanotic case there may be difficulty in the dis-tinction between the tetralogy and this anomaly,but such cases are rare. Fluoroscopy showspulsating pulmonary arteries and the lung fieldsare not ischaemic as in the tetralogy.
Isolated Pulmonary StenosisThe term isolated pulmonary stenosis is applied
to a group of cases in which there is pulmonarystenosis with or without a patent foramen ovale.It might also be applied to those cases of pul-monary stenosis where there is an interventricularseptal defect, but the aorta is normally sited anddoes not override it. Some hold that pulmonarystenosis as a sole abnormality is a condition of greatrarity. Those working in children's heart clinicswill generally be struck by the number of caseswhich satisfy the diagnostic criteria usually appliedto this anomaly. It is important to make a
Me:vntr:i:u1aiatlg.|eet*13,. cuS:]d: i
I'M lFIG. 17.-Transposition of the vessels with ventricular
septal defect. Pulmonary valve bicuspid. Markedcyanosis from birth.
separation between those cases that have a closedauricular septum and those which have a patentforamen ovale. In this latter group there is ashunt of blood from the right to the left so that acertain volume of blood is not returned to thelungs for oxygenation. Consequently, in somecases, cyanosis may appear relatively early andbecome marked.
Clinical PictureIn childhood there is no cyanosis unless the
stenosis is of a severity amounting to functionalatresia. The chief symptom is dyspnoea. Cyanosisusually develops in the teens in cases with apatent foramen ovale and gradually becomes per-manent. It ultimately becomes marked and moresevere than in the Eisenmenger anomaly and isaccompanied by clubbing and polycythaemia. Inthe case without an auricular septal defect cyanosisis later still in appearance and depends to a greatextent upon pulmonary vascular changes and pul-monary hypertension. The physical signs are aharsh systolic murmur and thrill in the second leftspace. The murmur is conducted towards theleft clavicle and the pulmonary second sound maybe diminished and sometimes absent. Occasion-
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November 1949 BROWN: Cyanotic Congenital Heart Disease 523
ally a diastolic murmur may be heard in thepulmonary area.
RadiologyThe heart is enlarged, especially the right side.
The pulmonary arc is convex and the hilar shadowsa little smaller than usual (Fig. 9). There is somepulsation in the hila but no pulmonary congestion.The heart does not usually assume the coeur-en-sabot appearance of the tetralogy.
ElectrocardiogramThis almost invariably shows a right axis
deviation. The P waves are often tall and peaked(Fig. io).Diagnosis
It is important to make a distinction betweenthe case with a patent foramen ovale and the casewith a closed auricular septum. The latterproperly belongs to the acyanotic group andcyanosis only develops late in life consequent uponpulmonary vascular changes. Pulmonary stenosiswith open foramen ovale can be distinguished fromthe tetralogy by its radiological picture of a convexpulmonary arc and the presence of some hilarpulsation, and from the Eisenmenger complex bythe large pulmonary artery and its branches. It
FIG. I8.-Transposition of the vessels with ventricularseptal defect. Male aged 20 years.
seems fair to say that in the present state of ourknowledge the final and completely accuratediagnosis must depend upon the results of cardiaccatheterization and angiocardiography.
Tricuspid AtresiaUntil the present time tricuspid atresia has been
regarded as a rather uncommon abnormality. Theimpetus given to the study of cyanotic children bythe possibilities of surgical treatment has broughtmany of these cases to light.There are several distinct anatomical types but
the basic anomaly is a non-functioning rightventricle which is virtually cut off from the restof the heart. The right ventricle may be entirelyabsent; it may exist as a blind cavity or it maycommunicate by a small orifice with the leftventricle (Figs. ii and 12). The tricuspid valvemay be entirely absent and represented only by adimple in the floor of the right auricle, or it mayshow extreme hypoplasia. Corresponding to thedefect of the tricuspid valve the pulmonary arteryis commonly atresic or else arises in an abnormalsituation. The right auricle is hypertrophied andthe foramen ovale widely open. The auricularseptum may be so defective that it makes the heartfunctionally biloculate. A patent ductus arteriosusis generally present in order to maintain a pul-
4~ t i- . 4.-.. .dtl. - -.----
FIG. I9.-Transposition of the vessels with ventricularseptal defect. Male aged I3 years. Marked rightaxis. Tall P waves.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

524 POSTGRADUATE MEDICAL JOURNAL November I949
R.
FIG. 20.-Persistent truncus arteriosus. Female aged 12 years, cyanotic since birth. At operation an enormouscollateral circulation through bronchial and mediastinal vessels and no visible pulmonary artery. (a) Posteroanterior.(b) Left anterior oblique.
monary circulation and is usually of largedimension. In some cases transposition of thevessels coexists and may result in some prolonga-tion of life.The effects upon the circulation are such that
the only means of escape of blood from the rightauricle is through an auricular septal defect intothe left auricle. A pulmonary blood supply ismaintained through a patent ductus arteriosus incases where there is pulmonary atresia, and inthose cases where a stenotic and hypoplasticpulmonary artery arises from the rudimentaryright ventricle some blood reaches the lungsthrough a defect in the ventricular septum andhence the pulmonary artery. A transposed pul-monary artery arising from the left ventricle some-times affords a pulmonary circulation. Not onlyis there a mixture of arterial and venous bloods inthe auricles but an inadequate volume of blood ispassed to the lungs, consequently cyanosis ismarked and severe.
Clinical PictureCyanosis of marked degree is the rule and
clubbing is commensurate with the cyanosis. Theheart may be normal in size or slightly enlarged.A systolic murmur is occasionally present but moreoften murmurs are absent. It is very rare to heara ductus murmur. The pulmonary second soundis well heard and never reduplicated.
RadiologyIn the postero-anterior view the silhouette of the
heart resembles that of the tetralogy (Figs. 143aand i3b). There is a concavity of the pulmonaryarc, small root shadows with an ischaemic lungand an upturned apex reminiscent of the coeur-en-sabot. In the left anterior oblique view it is atonce evident that the right ventricle is very smalland that the left ventricle is hypertrophied. Thepulmonary window is abnormally clear.
ElectrocardiogramThe electrocardiogram consistently shows a left
axis and for a long time this change was thoughtto be pathognomonic of tricuspid atresia (Figs.I4 and IS). It is now clear that other cyanoticcases may equally show a left axis, but the finding
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease
of a left axis is strong evidence in favour of tri-cuspid atresia, as it is more frequent in this thanin any other cyanotic congenital abnormality.Occasionally a normal axis is present (Fig. i6).
DiagnosisThe combination of cyanosis with left axis in
the electrocardiogram and radiological evidence ofa non-functioning right ventricle is presumptive*evidence of tricuspid atresia. The only other con-genital heart conditions in which a left axisoccasionally may be associated with cyanosis are asingle ventricle with diminutive outlet chamber, apersistent truncus arteriosus and transposition ofthe vessels. Cardiac catheterization will demon-strate the impossibility of entering the pulmonaryartery in tricuspid atresia, whereas in the singleventricle and persistent truncus it is possible toobserve the catheter moving freely within thecavity of the large ventricle. Complete trans-position of the vessels with tricuspid atresia isusually associated with a large interventricularseptal defect so that for a time an adequate volumeof blood reaches the lungs and cyanosis may de-velop late. Like other cases of transpositionwithout tricuspid atresia, the heart hypertrophiesand failure develops.
Complete Transposition of the Great VesselsThis is a severe form of congenital abnormality
only compatible with life in certain anatomicalcircumstances. The position of the great vesselsis reversed so that the aorta arises from the rightventricle and the pulmonary artery from the left,both vessels being of normal dimensions (Fig. 17).
............
FIG. 2 I.-Persistent truncus arteriosus in an infant,with a ' sitting duck' silhouette.
This places the subject at a very grave disadvantagefor although an adequate volume of blood reachesthe lungs for oxygenation it cannot be returned tothe systemic circulation unless the foetal passagesremain open, or unless there is a ventricular septaldefect. Accordingly, life is governed by the rela-tive efficiency of either a patent ductus arteriosus,patent foramen ovale, or ventricular septal defect,alone or in combination with each other. Froma practical point of view, only those cases with aventricular septal defect survive for any length oftime.
Clinical PictureThis depends to a great extent upon the
associated abnormalities accompanying the trans-posed great vessels and their efficiency in allowingcommunication between the two circulations. Ifthe ventricular septum is closed cyanosis is intenseand progressive. Attacks of dyspnoea often occur.The heart rapidly enlarges and the patient dies ofanoxaemia in days or weeks before there is timeto develop clutbbing or marked polycythaemia.When there is an associated ventricular septal
defect cyanosis may not be much in evidence atbirth but soon appears and may be evident withsucking or crying. Once apparent it is progressiveand accompanied by enlargement of the heart.Life may be prolonged for a year or in exceptional
. e -e ~ .. +... ..* . '''+------T------ --------..-. ..~...i....... ..-..
.~..-.--..~.-...;- --e +...Se- --... .
eT-i - -we- F ..~.
~~~ ~~~~~~~~~...... .. - ii7 rr.........-.
--.. ..... .......... .... ..-...
--S~~~~~~
;:F --::--:.--..
FIG. 22.-Persistent truncus arteriosus. Female aged14 years. Major deflection downwards in all threeleads.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
cases for several years. Prolonged survival maydepend upon the position of the pulmonary arteryvis-a-vis the septal defect.
In both groups of cases there may be a harshsystolic murmur but this has no definite charactersand may be absent. A systolic murmur is morefrequent and obvious when there is a ventricularseptal defect.
RadiologyThis is of great importance in diagnosis. Pro-
gressive enlargement of the heart over a shortspace of time has been stressed by Taussig (I947).In the antero-posterior view there is a narrowvascular pedicle which broadens as the patient isrotated into the oblique position (Fig. i8). Hilarpulsation is increased.
ElectrocardiogramRight axis deviation is generally present. The
P waves tend to be large (Fig. i9).
DiagnosisThe clinical picture is one of severe cyanosis and
dyspnoea occurring at birth. The radiologicalevidence is most important from the point of viewof diagnosis. This discloses an enlarged heartwith a narrow vascular pedicle which latter in-creases in width as the patient is rotated into theoblique position. There is pulmonary congestion.Serial photographs show rapid and progressivecardiac enlargement. The presence or absence ofa systolic murmur is of small diagnostic importanceA bruit is most likely to be heard when a ventricularseptal defect is present.
Persistent Truncus ArteriosusA persistent truncus arteriosus is an abnormally
large vessel occupying the site of the aorta andpulmonary artery and provided with a variablenumber of cusps. It overrides a high septal de-fect and the heart as a whole is enlarged, particu-larly the right ventricle. There are two importantanatomical varieties distinguished by their pul-monary arteries either separately, or from apersistent truncus gives off right and left pul-monary arteries either separately or from acommon stem; in the other group the pulmonarycirculation is maintained through bronchial ar-teries and other collaterals. The type of pul-monary circulation influences the clinical pictureso that cyanosis may not be apparent in those caseswhere the pulmonary arteries arise directly fromthe truncus unless these vessels are very small, butmay be very marked and severe in the cases wherea pulmonary circulation is through collateralchannels such as the bronchial arteries.
Clinical PictureAs mentioned previously the presence of
cyanosis depends upon the type of pulmonarycirculation. Clubbing is proportional to thecyanosis, especially in cases with a bronchial arterycirculation. There may be particularly severedyspnoea in these latter. The heart is enlarged inall cases, whether cyanosis is present or absent,,and may be greatly enlarged with deformity of theleft chest in some cases. A systolic murmur andthrill is usually present at the base. A continuous.murmur has been occasionally described and itssite of maximum intensity is at a lower level thanin the patent ductus arteriosus. The second soundis abnormally loud and is not reduplicated.Radiology
In infancy there is gross enlargement of theheart with a cardiac silhouette which bears someresemblance to a sitting duck. The heart is en-larged to both left and right with a concave pul-monary arc, prominent aortic knuckle and anupturned apex from left ventricular hypertrophy(Fig. 21). In the left anterior oblique view theright ventricular border passes like a shelf fromthe base of the aorta towards the anterior chestwall. The hilar shadows in the presence of abronchial artery circulation are small and peppered,and the lung fields abnormally clear. As the childgrows older the thorax lengthens and the heartbecomes more vertical; there is a change in theshape of the heart so that it comes to resemble thesilhouette of the tetralogy so closely that distinctionfrom it is difficult. A left anterior oblique viewmay furnigh a clue to the diagnosis at this age butnot always (Fig. 2oa and b).
ElectrocardiogramThis may show a right axis. Occasionally there
is a left axis. In several cases there has been abizarre electrocardiogram with the major deflectiondownwards in all three leads (Fig. 22).
DiagnosisThe radiological picture in infancy is charac-
teristic with an extremely large heart and apeculiar shelf-like projection of the right ventriclein the left oblique view. The vascular pedicle iswide. The point may be made that this abnor-mality presents the largest heart of any con-genital malformation, the only other comparableabnormality being the infantile type of coarctation.In older cases diagnosis is more difficult becausethe heart silhouette may so closely resemble thetetralogy that distinction from it is impossible onradiological grounds alone. Catheterization of theheart shows that the tip of the catheter may befreely moved about and a blood sample may have
526 November I1949by copyright.
on March 19, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.289.511 on 1 Novem
ber 1949. Dow
nloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease 527
the same oxygen content as blood from the femoralartery, demonstrating a single ventricle in thefunctional if not always in the completelyanatomical sense. Angiocardiography may alsohave obvious advantages in diagnosis.
Single Ventricle with Rudimentary OutletChamber
This may be regarded as a rather rare anomalyof which there are several anatomical types. It isof importance because one of these types maybenefit from surgical operation. Embryologicallythe anomaly represents persistence of the bulbuscordis as a rudimentary chamber. Anatomically,the rudimentary chamber occupies the site of thenormal pulmonary conus. It is separated from asingle ventricle by a band of muscular tissue, andcommunicates freely with it. Both auriculo-ventricular orifices open into the single ventricle.There is thus a functional cor biatriatum trilo-culare, and if there is associated maldevelopmentof the auricular septum, a functional cor biloculareresults. One or both of the great vessels mayarise from the rudimentary chamber, and de-pending upon whether there is associated mal-development of the great vessels, in normal or intransposed relationship. The great vessel arisingfrom the rudimentary cavity is usually small. Anaorta arising from the single ventricle, and thepulmonary artery from the rudimentary outletchamber, is an uncommon abnormality, usuallyknown as the Holmes' heart, of which but fewexamples are recorded (Fig. 23). More commonlythe vessels are transposed.The effects of the abnormality upon the circula-
tion will naturally vary according to the anatomicalarrangement of the great vessels. In all cases,because both auricles empty into the singleventricle there is a mixture of arterial and venousbloods; in consequence the inhalation of oxygencan never bring oxygen saturation to a normallevel. If both great vessels arise from the rudi-mentary chamber and are equal in size, equalvolumes of blood reach the respective circulationsand arterial and venous bloods are mixed in aboutequal proportions and one finds some degree ofcyanosis. When the pulmonary artery arises fromthe single ventricle and a smaller aorta from thediminutive chamber, a greater volume of bloodreaches the lungs than the volume reaching thesystemic circulation and consequently cyanosis isusually not apparent. An aorta arising from thesingle ventricle and a small pulmonary arteryarising from the rudimentary chamber, entails adiminished volume of blood to the lungs foroxygenation together with a large proportion ofvenous blood mixing with arterial blood in thesingle ventricle, hence cyanosis is marked and
...5'i1
FIG. 23.-Single ventricle with diminutive outletchamber. The great vessels are not transposed. Aprobe is placed in the small foramen communicatingbetween the single ventricle and the small outletchamber. An anastomotic operation has beenperformed.
severe. It is in this latter type that benefit may beexpected from surgical operation. Obviously in thecase where the pulmonary artery arises from thesingle ventricle the volume of blood supplied tothe lungs is adequate and surgery can be of novalue. A clinical manifestation of this type of caseis that the subject tends to be underdeveloped be-cause of the small volume of blood reaching thesystemic circulation through a small aorta. Thereremains the type in which both vessels may arisefrom the small chamber with pulmonary stenosis,and if this latter is at all severe, benefit may beexpected from surgery provided that there is alow pulmonary artery pressure. If pressures areabout the same in both aorta and pulmonary artery,which they will be if there is not marked pul-monary stenosis, an anastomosis is useless.
Clinical PictureThere are very great difficulties in the
recognition of this type of case. Cyanosis may bemarked where the pulmonary artery arises from therudimentary chamber or where there is pulmonary
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

528 POSTGRADUATE MEDICAL JOURNAL November I949
ew ii| ~~~~~~.... .. ..................::
FIG. 24.-Single ventricle with diminutive outletchamber. The great vessels not transposed.Pulmonary artery arises from the diminutivechamber. Marked cyanosis and left axis in theelectrocardiogram. Female aged 7.
stenosis with both vessels arising from the smallchamber. In other cases clinical cyanosis may beabsent, but in all cases, whether cyanotic or noi,there is an increased level of reduced haemoglobinin the arterial blood and a normal oxygen satura-tion cannot be produced by the inhalation ofoxygen. The heart is not enlarged. Murmursmay or may not be present, and if present aresystolic in time and have no definite characters orlocalization.
RadiologyX-ray examination furnishes important diag-
nostic clues. In the very young child there maybe prominence of the pulmonary conus due to thefact that the rudimentary chamber occupies thissite. At a later stage of childhood, as the lengthof the chest increases, the heart becomes morevertical and this apparent prominence disappears,so there may be little in the postero-anterior viewto distinguish it from the tetralogy (Fig. 24). Inthe left anterior oblique view there is no enlarge-ment of the right ventricle towards the chest walland the line of the aorta is virtually continuous asa straight line with that of the heart border. Whenthe pulmonary artery arises from the singleventricle pulmonary congestion is present.
ElectrocardiogramThere may be no deviation of the electrical
axis. Right axis has been reported. Left axisoccurred in a case of the author (Fig. 25).
DiagnosisThe difficulties in differential diagnosis were
well exemplified in a personal case of a child aged7. She had been cyanotic since birth and wasmarkedly cyanotic with clubbing when first seen.Her X-ray examination disclosed a small or absentright ventricle and her electrocardiogram a leftaxis. A confident diagnosis of tricuspid atresiawas made and following further investigation shewas submitted to operation. This was success-fully done, but the child died suddenly and un-expectedly. Autopsy disclosed that she had asingle ventricle with diminutive outlet chamberfrom which the pulmonary artery arose, a situationidentical with that of the Holmes heart.The lesions most likely to cause difficulty in
differential diagnosis are tricuspid atresia and thetetralogy of Fallot in cases with marked cyanosis.It is evident that the age of the patient will, tosome extent, determine the radiological pictureand in infancy an enlarged pulmonary arc, withor without congestion of the lung fields, wouldexclude the tetralogy. In later childhood the
aE W WF
; w * .| ||
FIG. 25.-Single ventricle with diminutive outletchamber Great vessels not transposed. Leftaxis, tall pointed P waves, deep Q3.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

November I949 BROWN: Cyanotic Congenital Heart Disease 529
R'0
U). 01co a (44).
'0'
44 44)
40 0
'00 50co ' 0
'0
z co ~
U 4"- (4 '0s Cs
co W 44(4(4
cu(4(4 (4 :4 0.~4
44 40
o c
4" : 0-404cis44.) 4) 4) ,(4beU)V.'s
co2 4)
1o 444)4be(4 ) ' 4. 4) '0'
(4 co2'.0~ ) ~ 4 0( 4 44co
Cs0 014
.!4) 2 '
0 4
40 Or0.c(n ~ 0
V co
04 U
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from

530 POSTGRADUATE MEDICAL JOURNAL November 1949
difficulties ate very real, particularly in the casewith a left axis in the electrocardiogram and a leftanterior oblique view closely resembling that of thenon-functioning right ventricle of tricuspid atresia.In tricuspid atresia it will be impossible to intro-duce the catheter into the pulmonary artery. In
cases with a common ventricle the catbeter movesfreely within the heart and may be readily intro-duced into the aorta if this arises from the commonventricle. Further, a sample of blood from thecommon ventricle would have the same oxygencontent as blood from the femoral artery.
BIBLIOGRAPHYBLALOCK, A., and TAUSSIG, H. B. (1945), . Amer. Med.
Ass., I28, I89.CAMPBELL, M. (1948), Guy's Hospital Rep., 97, I.COURNAND, A., BALDWIN, J. S., AND HIMMELSTEIN, A.
(I949), 'Cardiac Catheterization in Congenital Heart Disease.'Commonwealth Fund. New York.
by copyright. on M
arch 19, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.289.511 on 1 N
ovember 1949. D
ownloaded from