CVA Perspectives - chiro.org · Web viewFrumkin LP, Raloh Rw. Wallenberg's syndrome following...
37
Perspectives: An Overview of Comparative Considerations of Cerebrovascular Accidents PETER L. ROME ╪ ABSTRACT: This paper seeks to contrast reports concerning major adverse side effects, viz. cerebrovascular accidents (CVAs) attributed to cervical spine manipulation, within a broad perspective of medical procedures. It also seeks to correlate the incidence rates of other adverse events and medical procedures with the general incidence rate of CVAs. On analysis, an accurate position would indicate that cervical spinal manipulation is one of the more conservative, least invasive and safest of procedures in the provision of human health care services. The paper also alludes to the political connotations on the subject. INDEX TERMS: MeSH: ARTERIES; CEREBROVASCULAR DISORDERS; CERVICAL VERTEBRAE; CHIROPRACTIC; MANIPULATION, ORTHOPEDIC; IATROGENIC DISEASE; ORTHOPEDICS; OSTEOPATHIC MEDICINE; PERSUASIVE COMMUNICATION; PHYSICAL THERAPY; SPINE; VERTEBROBASILAR ACCIDENTS. ╪ Peter L. Rome, D.C. Private practice of chiropractic Mount Waverley, Victoria Received 26 March 1999, accepted 14 May 1999. Chiropr J Aust 1999; 29 (3): 87—102 INTRODUCTION There can be a risk involved with virtually all medical procedures, from the taking of blood samples, 1 use of vitamins 2 and "natural" medications, 3 to vaccinations, 4 drugs 2 and surgery. 5 At times, these risks seem to be either disregarded or categorised as an acceptable adverse side effect — the risk/benefit ratio. For instance, the Australian College of Ophthalmologists has issued a policy relating to laser surgery to correct myopia “... with low and acceptable rates of complications.” 6 A further study on endarterectomies stated that, “On average, the immediate risk of surgery was worth trading off against the long-term risk of stroke without surgery (but only) when the stenosis was greater than about 80% diameter...” 7 Currently, there is a greater move towards “informed consent” so that such risk factors are understood by patients. White defines apoplexy as brain damage where there is “... an acute neurological deficit resulting in death, or lasting more than 24 hours and classified by a physician as a stroke.” 8 In his literature search, Terrett found that historically, the first adverse accident related to bone-setting was recorded in 1871 — almost a quarter century before chiropractic was founded in 1895. The first vascular accident following manipulation was reported in 1934 — almost 40 years after our profession was founded. 9 It has been estimated that the incidence of apoplexy in Australia is likely to
Transcript of CVA Perspectives - chiro.org · Web viewFrumkin LP, Raloh Rw. Wallenberg's syndrome following...
Perspectives: An Overview of Comparative Considerations of Cerebrovascular Accidents
PETER L. ROME ╪
ABSTRACT: This paper seeks to contrast reports concerning major adverse side effects, viz. cerebrovascular accidents (CVAs) attributed to cervical spine manipulation, within a broad perspective of medical procedures. It also seeks to correlate the incidence rates of other adverse events and medical procedures with the general incidence rate of CVAs. On analysis, an accurate position would indicate that cervical spinal manipulation is one of the more conservative, least invasive and safest of procedures in the provision of human health care services. The paper also alludes to the political connotations on the subject.INDEX TERMS: MeSH: ARTERIES; CEREBROVASCULAR DISORDERS; CERVICAL VERTEBRAE; CHIROPRACTIC; MANIPULATION, ORTHOPEDIC; IATROGENIC DISEASE; ORTHOPEDICS; OSTEOPATHIC MEDICINE; PERSUASIVE COMMUNICATION; PHYSICAL THERAPY; SPINE; VERTEBROBASILAR ACCIDENTS.
╪ Peter L. Rome, D.C.Private practice of chiropractic Mount Waverley, VictoriaReceived 26 March 1999, accepted 14 May 1999.Chiropr J Aust 1999; 29 (3): 87—102
INTRODUCTION
There can be a risk involved with virtually all medical procedures, from the taking of blood samples, 1 use of vitamins 2 and "natural" medications, 3 to vaccinations, 4 drugs 2 and surgery. 5 At times, these risks seem to be either disregarded or categorised as an acceptable adverse side effect — the risk/benefit ratio. For instance, the Australian College of Ophthalmologists has issued a policy relating to laser surgery to correct myopia “... with low and acceptable rates of complications.” 6 A further study on endarterectomies stated that, “On average, the immediate risk of surgery was worth trading off against the long-term risk of stroke without surgery (but only) when the stenosis was greater than about 80% diameter...” 7
Currently, there is a greater move towards “informed consent” so that such risk factors are understood by patients.White defines apoplexy as brain damage where there is “... an acute neurological deficit resulting in death, or lasting more than 24 hours and classified by a physician as a stroke.” 8
In his literature search, Terrett found that historically, the first adverse accident related to bone-setting was recorded in 1871 — almost a quarter century before chiropractic was founded in 1895. The first vascular accident following manipulation was reported in 1934 — almost 40 years after our profession was founded. 9
It has been estimated that the incidence of apoplexy in Australia is likely to rise by 70% in the next twenty years, due to the ageing of the population.10 The relative prevalence of such incidents is further exemplified by the indication that “everyone had some degree of stroke risk.” 10 This statement is reflected later in this paper, citing Myler, who calculated that the rate of fatal cerebrovascular accidents (CVAs) in the general population is greater than that of manipulated patients.11
Concern at the serious nature of CVAs should also be tempered by the knowledge that a significant proportion of those who experience an adverse reaction to spinal manipulative therapy (SMT) undergo complete or partial recovery,12 similar to those who experience vertebral artery dissection (VAD) due to other causes. 13-15

This paper also compares the mortality rates of nonsteroidal anti-inflammatories (NSAIDs) and other medical procedures with SMT. The relative incidence rates show SMT to be considerably more favourable than NSAIDs from a safety viewpoint. 16
To castigate or reject spinal manipulative therapy as inappropriate or comparatively dangerous is not only unwarranted, but conveniently overlooks the morbidity and mortality rates of other interventions. Such concern would seem out of proportion to that involved with everyday articular release of an intervertebral facet fixation — a vertebral manipulation.Concern over, and considerations of, spinal manipulation does, however, also serve to emphasise the potential for positive integrated influences associated with important neurological and vascular elements within the dysfunction of dynamic vertebral segments — the vertebral subluxation complex.
METHOD
This paper was compiled from a number of sources as ongoing research over some years. These sources included reference lists, Index Medicus, manual searches and computer searches as well as news items. The network of citations obtained led to further searches. As this paper was being prepared for submission, relevant papers continued to appear in the literature. It was necessary 10 “draw the line,” so these further references had to be omitted.
Information thus gleaned was collated and reviewed in an attempt to assess a comparative risk of CVAs attributed to SMT. A contrast of morbidity and mortality rates of other medical procedures and health conditions has been considered as a means of illustrating the risk factor of various therapeutic procedures and interventions.To gain a more accurate perspective of the claimed adverse events attributed to chiropractic, a comparison has been made of the apparent high rate of adverse events of some medical procedures with the apparent low rate of adverse events involving spinal manipulation.
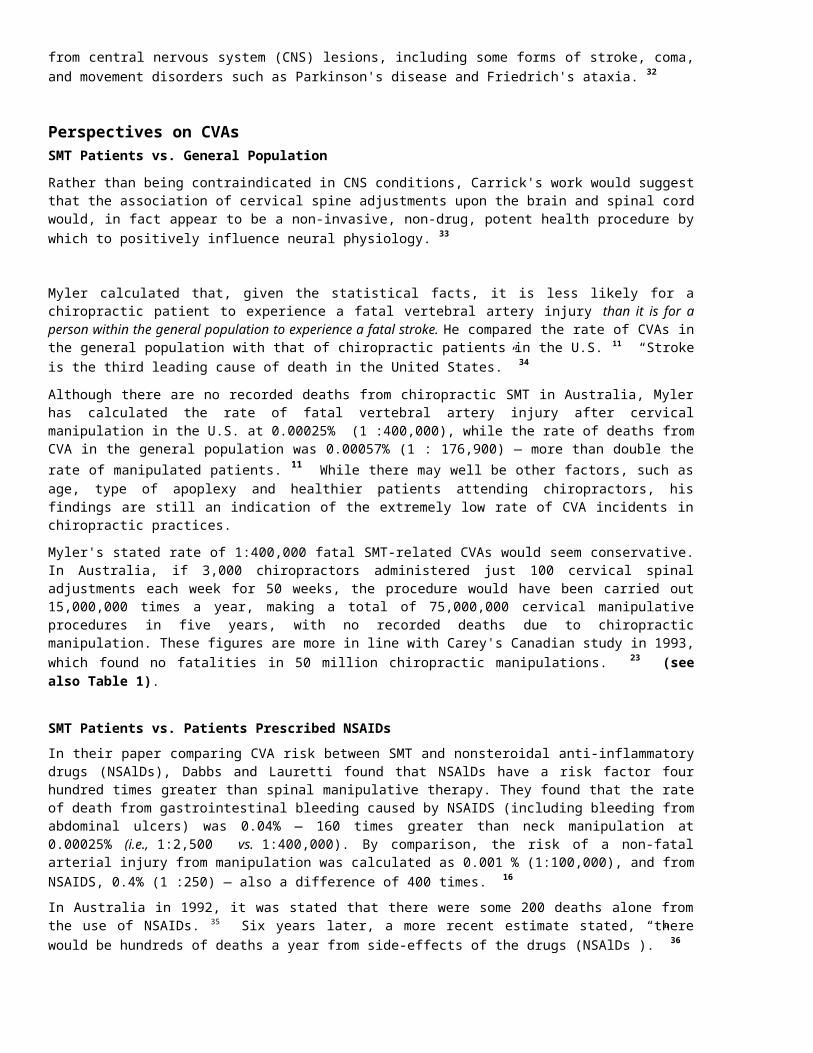
As a further perspective, the incidence rates of CVAs associated with everyday events are also noted.
Table 1INCIDENCE RATES OF CEREBROVASCULAR ACCIDENTSASSOCIATED WITH SPINAL MANIPULATIVE THERAPY
YEAR AUTHORS INCIDENCE1963 Cyriax 17 1: 1 0,000,0001968 Livingstone 18 “Few” in “possibly 75,000,000” p.a.1972 Maigne 19 1 :” "Several tens of millions”1980 Jaskoviak 20 (over 15 yr) 0:5,000,0001981 Hosek et al. 12 1:1,000,0001983 Gutman 12,21 1 :400,0001985 Dvorak & Orelli
12,212-3:1,000,000
1991 Patjin 16 1 :518,0001992 Shekelle 22 1:100,000,000 (cauda equina/lumbar manipulations)1993 Carey 23 1:3,846,1531993 Haldeman 16 1-2: 1,000,0001994 Haynes 24 1:100,000 (N.B.: This statistic applies to the ratio per
patient, not per visit)1995 Carlini 16 1 :500,0001996 Lauretti 25 1 :2,000,000 (National Chiropractic Mutual Insurance
Company per cervical manipulation)1996 Lauretti 26 1:1,000,000 (1 neurological complication per 1 million
patient visits)
* Manipulation-related mortality rate averaged for all professions is 1 in 2 years, 34 over 61 years, worldwide. 21
** Spinal Mobilization: In 1993, the physiotherapist Michaeli reported a “...similarity in the nature and prevalence of complications following cervical mobilisation and manipulation...” In some instances the reported incidence rate of adverse effects was higher for mobilisation than manipulation. 27
LIMITATIONS OF THIS REVIEW
A review such as this is limited in the consideration of such factors as the patient's age and underlying health status, frequency of the procedure involved, necessity for a particular procedure, and available options to a particular procedure against the benefit/outcome.Consideration has been given to the following: Some of the references are not recent, however it has been noticed that morbidity and
mortality rates in many medical procedures have altered little in 20-30 years. While it is difficult to draw direct comparisons on a topic such as this, the inference from
published medical papers is that SMT has a high incidence rate — presumably compared to medical care and procedures. In researching this topic it appeared that there were more papers published on the side effects of medical procedures than on the prevention of such side effects.
While it may be argued that medicine is involved with more serious conditions, this paper is an attempt to portray certain perspectives only. It is relevant to compare one procedure with another to be able to rate its risk in perspective — to know where it stands in the overall picture.
Consideration was also given to various forms of CVA and the sites of CVA lesions. Rather than differentiate these, it was decided to conduct a general overview at this stage.
It could be argued that in relation to SMT, incidence figures relate only to published reports, however the same can also be said for the incidence rates involving all professions, as not all adverse side effects are necessarily recorded in the literature.
REVIEWThe incidence rate of serious neurological compromise associated with manipulation is remarkably low in itself. Estimates range from as low as 1:10 million 17 (see Table 1). The incidence rate gains an even lower perspective when comparisons are made with other medical procedures, and when considered in light of incidents associated with some everyday circumstances (see other tables). In relation to SMT, it is rare that a serious side effect occurs. 16,28,29 A significant proportion of these appear to be of minor severity and transient in nature. 28,30
Michaeli also states that “The vast majority of these 'accidents' (CVAs) are of a transient nature and therefore may not have been worthy of mention in the literature.” 31

Assendelft et al. found that of the 165 patients with associated side effects of spinal manipulation, 44 (26.7%) made a complete recovery following the initial onset and that “serious complications (are) generally considered to be low.” This study included both cervical and lumbar complications. Some 49% of the lumbar complications occurred during manipulation under anaesthesia (MUA). MUA is not a customary chiropractic procedure. 28
On the positive side, clinical observations of the beneficial influence of spinal manipulation on neurological function have already been noted. Carrick reported that certain procedures, including manipulative techniques, can provide remarkably promising responses in assisting some patients in degrees of recovery from central nervous system (CNS) lesions, including some forms of stroke, coma, and movement disorders such as Parkinson's disease and Friedrich's ataxia. 32
Perspectives on CVAsSMT Patients vs. General PopulationRather than being contraindicated in CNS conditions, Carrick's work would suggest that the association of cervical spine adjustments upon the brain and spinal cord would, in fact appear to be a non-invasive, non-drug, potent health procedure by which to positively influence neural physiology. 33
Myler calculated that, given the statistical facts, it is less likely for a chiropractic patient to experience a fatal vertebral artery injury than it is for a person within the general population to experience a fatal stroke. He compared the rate of CVAs in the general population with that of chiropractic patients in the U.S. 11 “Stroke is the third leading cause of death in the United States.” 34
Although there are no recorded deaths from chiropractic SMT in Australia, Myler has calculated the rate of fatal vertebral artery injury after cervical manipulation in the U.S. at 0.00025% (1 :400,000), while the rate of deaths from CVA in the general population was 0.00057% (1 : 176,900) — more than double the rate of manipulated patients. 11 While there may well be other factors, such as age, type of apoplexy and healthier patients attending chiropractors, his findings are still an indication of the extremely low rate of CVA incidents in chiropractic practices.
Myler's stated rate of 1:400,000 fatal SMT-related CVAs would seem conservative. In Australia, if 3,000 chiropractors administered just 100 cervical spinal adjustments each week for 50 weeks, the procedure would have been carried out 15,000,000 times a year, making a total of 75,000,000 cervical manipulative procedures in five years, with no recorded deaths due to chiropractic manipulation. These figures are more in line with Carey's Canadian study in 1993, which found no fatalities in 50 million chiropractic manipulations. 23 (see also Table 1).
SMT Patients vs. Patients Prescribed NSAIDsIn their paper comparing CVA risk between SMT and nonsteroidal anti-inflammatory drugs (NSAlDs), Dabbs and Lauretti found that NSAlDs have a risk factor four hundred times greater than spinal manipulative therapy. They found that the rate of death from gastrointestinal bleeding caused by NSAIDS (including bleeding from abdominal ulcers) was 0.04% — 160 times greater than neck manipulation at 0.00025% (i.e., 1:2,500 vs. 1:400,000). By comparison, the risk of a non-fatal arterial injury from manipulation was calculated as 0.001 % (1:100,000), and from NSAIDS, 0.4% (1 :250) — also a difference of 400 times. 16
In Australia in 1992, it was stated that there were some 200 deaths alone from the use of NSAIDs. 35 Six years later, a more recent estimate stated, “there would be hundreds of deaths
a year from side-effects of the drugs (NSAlDs ).” 36
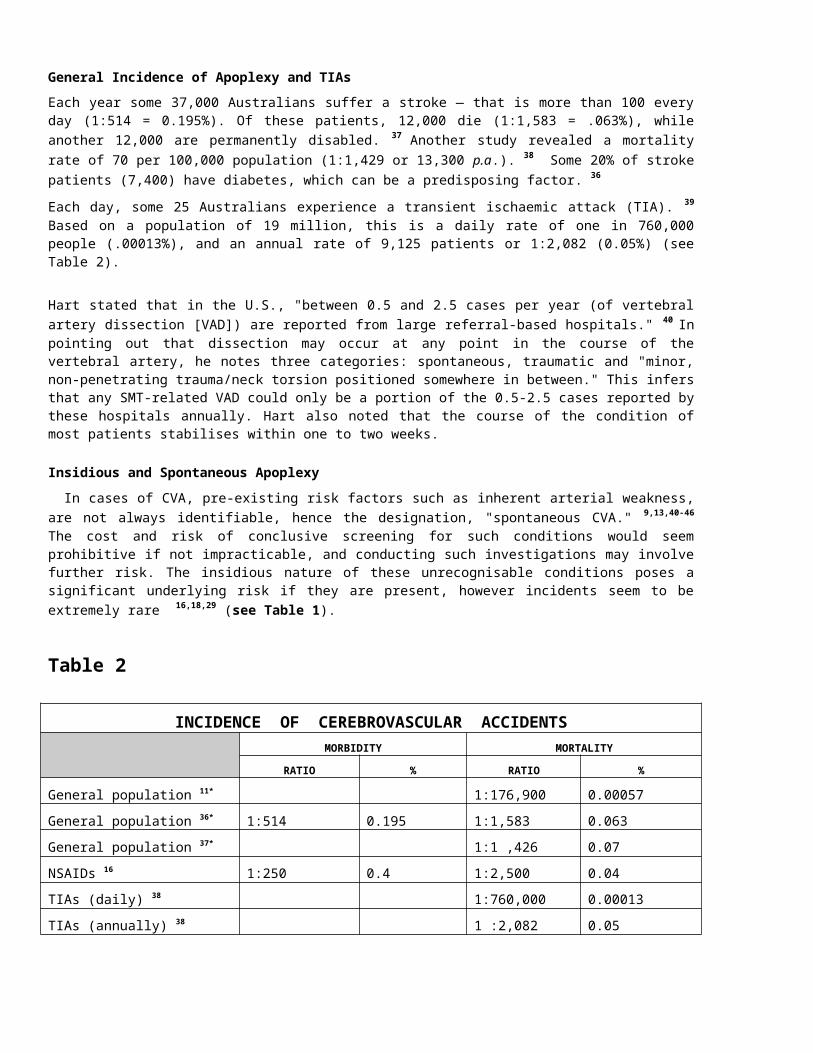
General Incidence of Apoplexy and TIAsEach year some 37,000 Australians suffer a stroke — that is more than 100 every day (1:514 = 0.195%). Of these patients, 12,000 die (1:1,583 = .063%), while another 12,000 are permanently disabled. 37 Another study revealed a mortality rate of 70 per 100,000 population (1:1,429 or 13,300 p.a.). 38 Some 20% of stroke patients (7,400) have diabetes, which can be a predisposing factor. 36
Each day, some 25 Australians experience a transient ischaemic attack (TIA). 39 Based on a population of 19 million, this is a daily rate of one in 760,000 people (.00013%), and an annual rate of 9,125 patients or 1:2,082 (0.05%) (see Table 2).
Hart stated that in the U.S., "between 0.5 and 2.5 cases per year (of vertebral artery dissection [VAD]) are reported from large referral-based hospitals." 40 In pointing out that dissection may occur at any point in the course of the vertebral artery, he notes three categories: spontaneous, traumatic and "minor, non-penetrating trauma/neck torsion positioned somewhere in between." This infers that any SMT-related VAD could only be a portion of the 0.5-2.5 cases reported by these hospitals annually. Hart also noted that the course of the condition of most patients stabilises within one to two weeks.
Insidious and Spontaneous ApoplexyIn cases of CVA, pre-existing risk factors such as inherent arterial weakness, are not always
identifiable, hence the designation, "spontaneous CVA." 9,13,40-46 The cost and risk of conclusive screening for such conditions would seem prohibitive if not impracticable, and conducting such investigations may involve further risk. The insidious nature of these unrecognisable conditions poses a significant underlying risk if they are present, however incidents seem to be extremely rare 16,18,29 (see Table 1).
Table 2
INCIDENCE OF CEREBROVASCULAR ACCIDENTSMORBIDITY MORTALITY
RATIO % RATIO %
General population 11* 1:176,900 0.00057General population 36* 1:514 0.195 1:1,583 0.063General population 37* 1:1 ,426 0.07NSAIDs 16 1:250 0.4 1:2,500 0.04TIAs (daily) 38 1:760,000 0.00013TIAs (annually) 38 1 :2,082 0.05Chiropractic/SMT 11,16 1:100,000 0.001 1:400,000 .00025Chiropractic/SMT 23 1:3,840,153 0.000035 Nil:50,000,00
0———
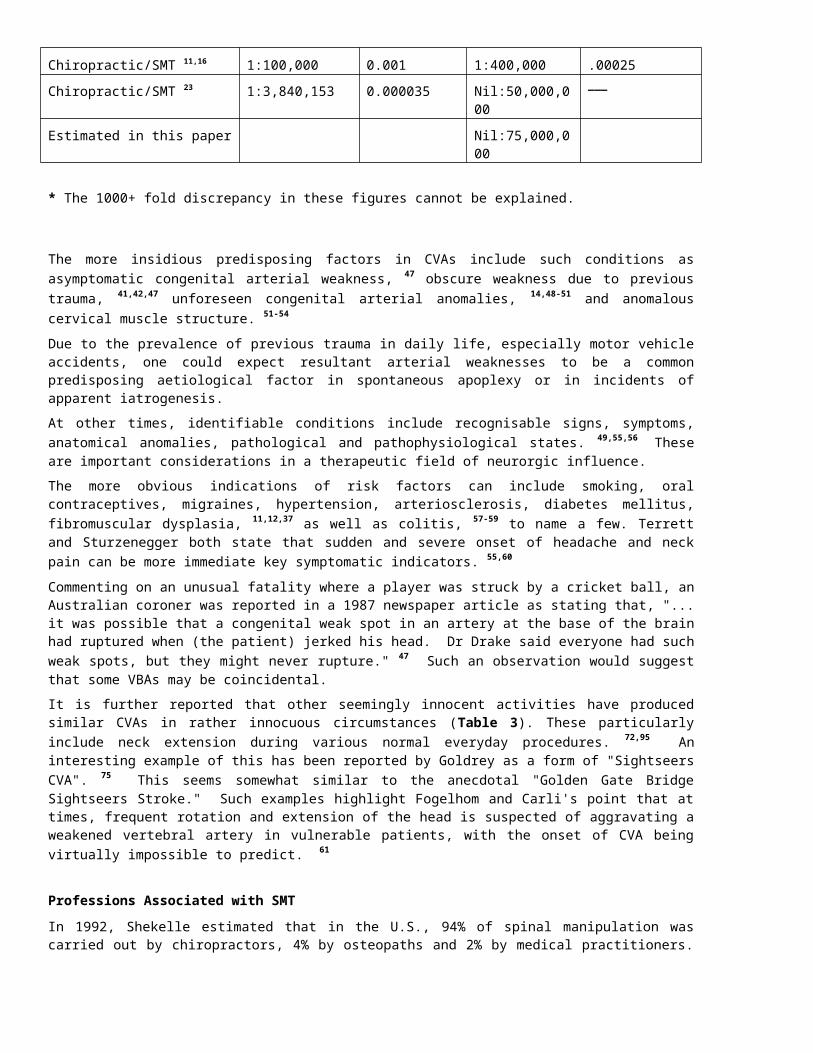
Estimated in this paper Nil:75,000,000
* The 1000+ fold discrepancy in these figures cannot be explained.
The more insidious predisposing factors in CVAs include such conditions as asymptomatic congenital arterial weakness, 47 obscure weakness due to previous trauma, 41,42,47 unforeseen congenital arterial anomalies, 14,48-51 and anomalous cervical muscle structure. 51-54
Due to the prevalence of previous trauma in daily life, especially motor vehicle accidents, one could expect resultant arterial weaknesses to be a common predisposing aetiological factor in spontaneous apoplexy or in incidents of apparent iatrogenesis.At other times, identifiable conditions include recognisable signs, symptoms, anatomical anomalies, pathological and pathophysiological states. 49,55,56 These are important considerations in a therapeutic field of neurorgic influence.The more obvious indications of risk factors can include smoking, oral contraceptives, migraines, hypertension, arteriosclerosis, diabetes mellitus, fibromuscular dysplasia, 11,12,37 as well as colitis, 57-59 to name a few. Terrett and Sturzenegger both state that sudden and severe onset of headache and neck pain can be more immediate key symptomatic indicators. 55,60
Commenting on an unusual fatality where a player was struck by a cricket ball, an Australian coroner was reported in a 1987 newspaper article as stating that, "... it was possible that a congenital weak spot in an artery at the base of the brain had ruptured when (the patient) jerked his head. Dr Drake said everyone had such weak spots, but they might never rupture." 47 Such an observation would suggest that some VBAs may be coincidental.It is further reported that other seemingly innocent activities have produced similar CVAs in rather innocuous circumstances (Table 3). These particularly include neck extension during various normal everyday procedures. 72,95 An interesting example of this has been reported by Goldrey as a form of "Sightseers CVA". 75 This seems somewhat similar to the anecdotal "Golden Gate Bridge Sightseers Stroke." Such examples highlight Fogelhom and Carli's point that at times, frequent rotation and extension of the head is suspected of aggravating a weakened vertebral artery in vulnerable patients, with the onset of CVA being virtually impossible to predict. 61
Professions Associated with SMTIn 1992, Shekelle estimated that in the U.S., 94% of spinal manipulation was carried out by chiropractors, 4% by osteopaths and 2% by medical practitioners. 22 Recently De Fabio claimed that physiotherapists also conduct 2% of SMT in the U.S. 101
Calculations based on Terrett's 1995 study covering 58 years, however, showed that only 64.1 % of 78 manipulation-related "catastrophes "were attributed to chiropractors, while 8.97% were attributed to medical practitioners, who conduct only 2% of the manipulative procedures, and 10.26% to osteopaths, who conduct only 4% of manipulative procedures in the U.S. The balance of some 17% comprised a miscellaneous grouping. Terrett questions the reliability and accuracy of ascribing and impugning chiropractors by incorrectly attributed involvement in "all" adverse effects through the medical literature. 54
Winterstein also noted that the proportion of chiropractor-related incidents is far less than 94% of spinal manipulation carried out by this one profession. 102
Further extrapolation of these available figures would suggest that while conducting only 1/47 of manipulative procedures, medicine has 20.89 times, and osteopathy (2/47) has 3.92 times greater mortality rates in spinal manipulation than chiropractic.
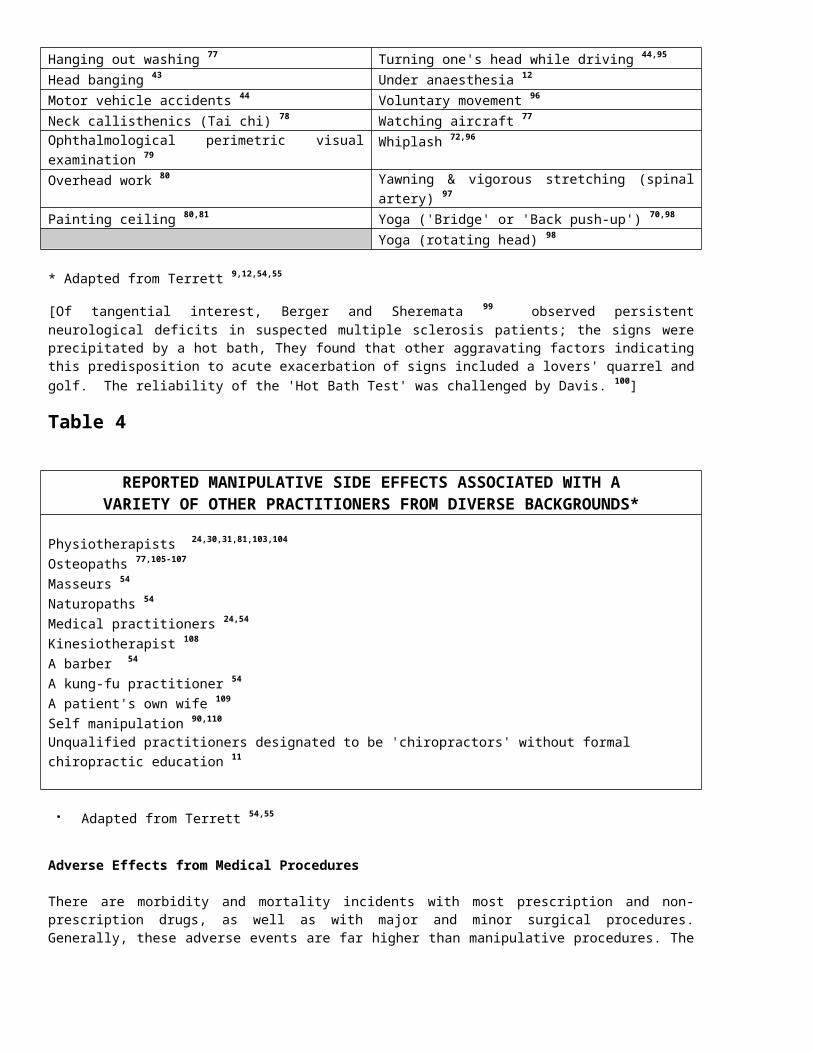
In his 1998 study, Terrett found that in over 61 years, the practitioners reported as being associated with major manipulative side effects in 219 examined cases were actually practitioners from quite diverse backgrounds, education and training, not just from a
chiropractic background, as mostly reported. The list also includes physiotherapists, osteopaths, naturopaths, a barber, masseurs, and medical practitioners (see Table 4). These major side effects comprised a total of 34 deaths worldwide over the 61 years (1: 1.8 yr). In addition, of the 185 other, more serious side effects, 44 (23.8%) either subsided or almost completely resolved with minor neurological deficits. 54
As a comparison to the 34 deaths associated with manipulation over 61 years worldwide, Burgess reported in 1998 that there were nine reported deaths in thirteen months due to pertussis in Australia in 1997. 4 The pertussis deaths did not receive anything like the publicity the manipulative incidents seem to. At the monthly rate (1.44 per million), there would be 1,054.08 pertussis deaths over the same 61 year time span-a rate 3,100% higher. By comparison, there have been three SMT-associated fatalities ever recorded in Australia — all involving medical practitioners. 112
Cyriax, the doyen of medical spinal manipulation, stated that in relation to major side effects associated with manipulation of the cervical spine, "the risk works out at about one in ten million manipulations, and provides no argument against an attempt at manipulative reduction in suitable cases." He then goes on to discuss "The danger of not manipulating." 17
Livingstone, in commenting on the "25,000 manipulators" in the U.S. in 1968, stated that there were surprisingly "few reported injuries to show for possibly 75,000,000 yearly manipulations." (This appears to be based on 3,000 per practitioner per year — 60 per week.) Livingstone does not specify whether his calculations are based on a unilateral (single), or bilateral ( double) manipulation per visit. 18
In 1993, a Canadian study by Carey estimated that of 50,000,000 neck manipulations over a five-year period, there were 13 serious YBA incidents and no deaths. 23 This is a VBA rate of 1:3,846,153. A U.S. insurance company has estimated the serious YBA rate at 1:2,000,000. 25
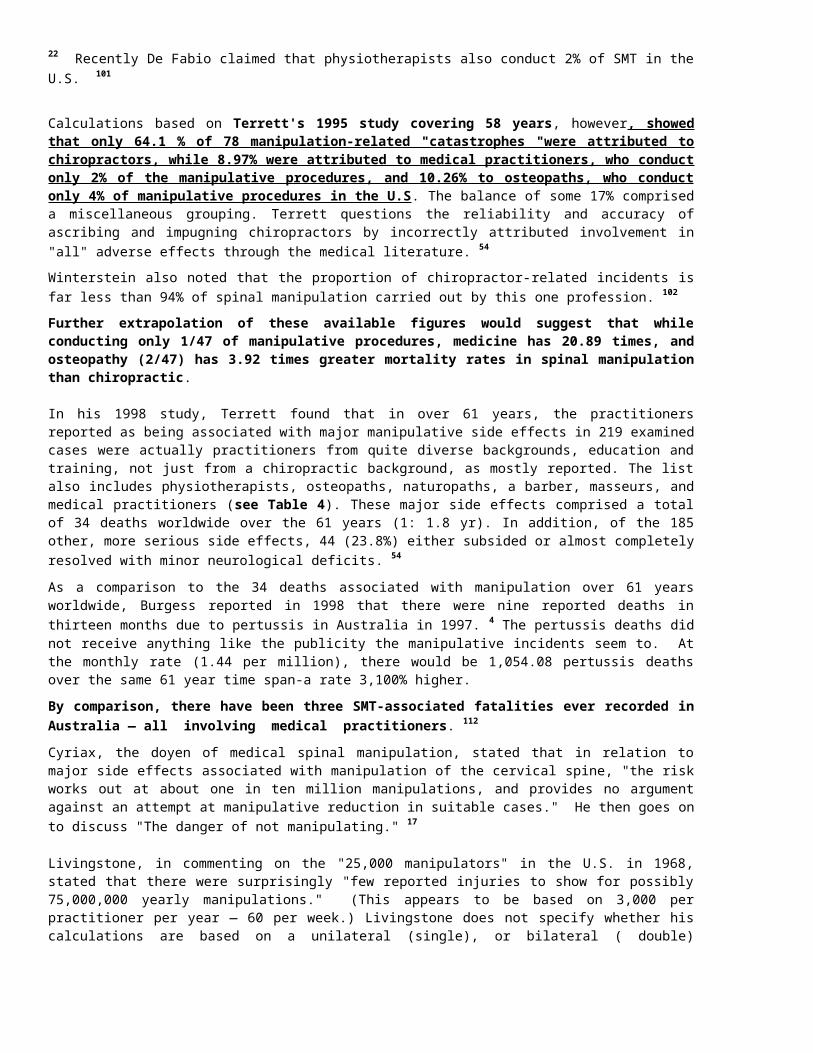
Table 3REPORTED ACTIVITIES INVOLVING THE CERVICAL SPINE
SUSPECTED OF BEING INVOLVED WITH DISRUPTION OF CEREBRAL CIRCULATION*
Age not a factor 9 Post-operative complications of thyroidectomy 82
A bleeding nose 12,61 Postural head changes 83,84
Angiography 43,62 Radiographic procedure (VA angiography) 43
Archery (bow hunter) 12 Rap dancing 67-69,85,86
Athletics 63 Reversing a vehicle (see 'backing up')Axial traction 64 Roller coaster 87,88
Backing up a car 44,62 Self manipulation 'clicked on turning' 89
Beauty parlour 65 Self manipulation (rapid) 90,91
Birth trauma 66 (see also 'childbirth') Sitting in a barber's chair 77
Break dancing (see also rap dancing) 67-69 Sit-up exercises 24
Calisthenics 70 Sliding head-first down a water slide 24
Childbirth 'doubtful relationship' 55 Sleeping positions 50
Contraceptive pill 13,43 Spontaneous rupture of aneurisms 43
Coughing 71 Spontaneous turning of head 40,44
Dental procedure 44 Spontaneous vertebral artery dissection 9,40-46
Diving into shallow water 72 (see 'falls') Star gazing 16
During surgery 12 Stooping to pick up a bucket 24
During x-ray examination 61 Surgery, neck positioning during anaesthesia
79
Emergency resuscitation 12 Swimming 92
Falls (minor) 43 Tai chi 78
Falls causing hyperextension 43 Telephone call (cordless) 89
Fitness exercise 71 Traction of cervical spine 48,63,77
Football 72-74 Traction and short wave diathermy 89
'Golden Gate Bridge' syndrome (sightseeing) 75
Trampoline 40
Gymnastics 70 Trauma 94
Hair dressing 76 Turning one's head 83
Hanging out washing 77 Turning one's head while driving 44,95
Head banging 43 Under anaesthesia 12
Motor vehicle accidents 44 Voluntary movement 96
Neck callisthenics (Tai chi) 78 Watching aircraft 77
Ophthalmological perimetric visual examination 79
Whiplash 72,96
Overhead work 80 Yawning & vigorous stretching (spinal artery) 97
Painting ceiling 80,81 Yoga ('Bridge' or 'Back push-up') 70,98
Yoga (rotating head) 98
* Adapted from Terrett 9,12,54,55
[Of tangential interest, Berger and Sheremata 99 observed persistent neurological deficits in suspected multiple sclerosis patients; the signs were precipitated by a hot bath, They found that other aggravating factors indicating this predisposition to acute exacerbation of signs included a lovers' quarrel and golf. The reliability of the 'Hot Bath Test' was challenged by Davis. 100]
Table 4
REPORTED MANIPULATIVE SIDE EFFECTS ASSOCIATED WITH AVARIETY OF OTHER PRACTITIONERS FROM DIVERSE
BACKGROUNDS*
Physiotherapists 24,30,31,81,103,104
Osteopaths 77,105-107
Masseurs 54
Naturopaths 54
Medical practitioners 24,54
Kinesiotherapist 108
A barber 54
A kung-fu practitioner 54
A patient's own wife 109
Self manipulation 90,110
Unqualified practitioners designated to be 'chiropractors' without formal chiropractic education 11
Adapted from Terrett 54,55

Adverse Effects from Medical Procedures
There are morbidity and mortality incidents with most prescription and non-prescription drugs, as well as with major and minor surgical procedures. Generally, these adverse events are far higher than manipulative procedures. The mortality and morbidity rates of certain medical procedures can be viewed to gain a perspective on the risks involved 113-116 (see Tables 5-7).It would be grossly irresponsible and misleading if patients were led to believe that adverse effects from medical procedures did not exist, or were disproportionately low. It is surprising how patients seem to accept the incidence of risks and complications from medical procedures as "normal," yet still be alarmed at the limited possibility and significantly lower adverse incident rates ("negligible" 24) involving manipulative procedures in chiropractic or other professions using manipulation. Unwarranted sensationalism of cases involving chiropractors threatens to create an impression out of proportion to the actual facts. One wonders what would happen if all medical procedures were subject to the same levels of safety, efficacy, journalistic scrutiny and particularly inaccurate publicity.Issues concerning the efficacy of medical care have already been raised in such respected journals as the Lancet, British Medical Journal, the Journal of the American Medical Association and the Medical Journal of Australia. Such controversial issues do not appear to have received general media exposure or public discussion to any great degree. 125,172-177
What should be of serious concern, however, is the statement in one of the world's most respected journals in 1991, the British Medical Journal:
"... only about 15% of medical interventions are supported by solid scientific evidence..." and "only 1 % of the articles in medical journals are scientifically sound and partly because many treatments have never been assessed at all. 174
Six years earlier, in 1985, medicine was already aware of the problem when Leeder wrote in the Medical Journal of Australia:
"Much medical practice has escaped critical appraisal...many treatment schedules, new and old, simple and complex, have been adopted and endorsed without firm evidence that they achieve more good than harm... (or) have never been satisfactorily evaluated... Some procedures … became entrenched in professional mythology long ago (and) have remained unchallenged despite their appalling cost in terms of human suffering." 175
In 1998, Moore and colleagues noted two drugs which were shown to have serious and potentially lethal cardiac side effects. They had been on the market for twelve and fourteen years, respectively. They stated:
"Discovering new dangers of drugs after marketing is common. Over 51 % of approved drugs have serious adverse effects not detected prior to approval. Merely discovering adverse effects is not by itself sufficient to protect the public." 176
The International Classification of Diseases code 178 lists the following iatrogenic classifications which include numerous headings under "misadventure" and "complications":
E850-858 - Accidental poisoning and medication errors. E870-879 - Misadventures during surgical and medical care.E930-949 - Drugs causing adverse effects in therapeutic use. E977.9 - Medicine poisoning by overdose- wrong substance given or taken in error.E995.2 - Adverse effect, correct substance properly administered.
Adverse drug reactions rank as the fifth ("between fourth and sixth") leading cause of
death in the U.S. — 106,000 deaths in 1994. 125
In relation to medical complications, a 1982 study by Steel et al. found"... a 36% incidence of iatrogenic illnesses among 815 consecutively selected patients in a tertiary care university hospital." In 2% (16.3 of those admitted), " … these complications were believed to have contributed to death." 114 By 1998, Lazarou and colleagues found that there was virtually no change in the incidence rate of adverse drug reactions in the 32 years of their study. 125
A two-year study by Rankin et al. (1990-1992) found that in Australia, "Between 170 and 850 (1-5%) strokes occur (annually as) a major iatrogenic complication of cardiopulmonary by-pass surgery." 179 Other major surgical procedures also carry the risk of stroke (see Table 8).In 1993, Nachemson stated that in relation to spinal surgery, "... the clinical studies have largely lacked validity: controlled, prospective tr1als are disappointingly rare." 182
These issues alone should_overshadow and create more concern than political medicine's preoccupation with otherprofessions which it may see as competitors.While medicine seems interested in highlighting incidents involving spinal manipulation, it can be questioned as to whether patients are fully cognisant of the high rates of medical incidents. This is not intended as a criticism, but more to place the rate of incidents in context. One cannot ignore the assumption of "acceptable statistics" in the absence of public awareness.
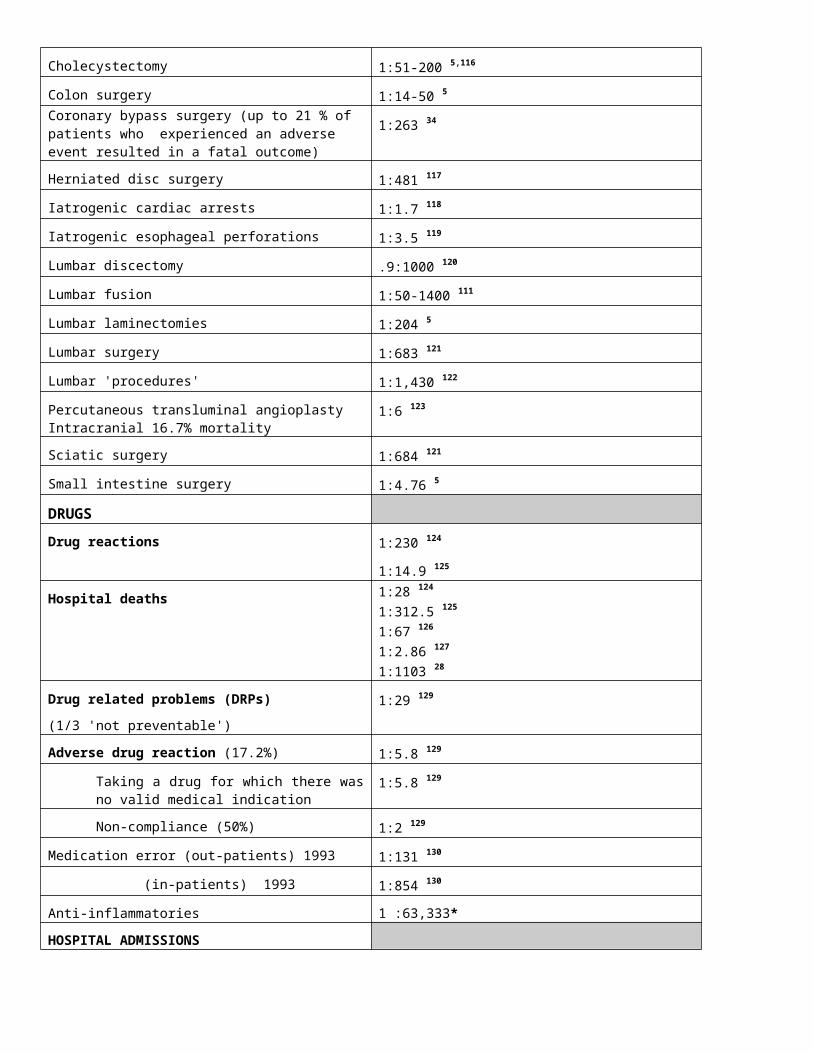
Table 5
MORTALITY RATES OF VARIOUS MEDICALPROCEDURES AND DAILY EVENTS*
SURGERYAppendectomies 1:74 5
Cervical spine surgery 1:145 5
Cholecystectomy 1:51-200 5,116
Colon surgery 1:14-50 5Coronary bypass surgery (up to 21 % of patients who experienced an adverse event resulted in a fatal outcome)
1:263 34
Herniated disc surgery 1:481 117
Iatrogenic cardiac arrests 1:1.7 118
Iatrogenic esophageal perforations 1:3.5 119
Lumbar discectomy .9:1000 120
Lumbar fusion 1:50-1400 111
Lumbar laminectomies 1:204 5
Lumbar surgery 1:683 121
Lumbar 'procedures' 1:1,430 122
Percutaneous transluminal angioplasty Intracranial 16.7% mortality
1:6 123
Sciatic surgery 1:684 121
Small intestine surgery 1:4.76 5
DRUGSDrug reactions 1:230 124
1:14.9 125
Hospital deaths 1:28 124
1:312.5 125
1:67 126
1:2.86 127
1:1103 28
Drug related problems (DRPs) (1/3 'not preventable')
1:29 129
Adverse drug reaction (17.2%) 1:5.8 129
Taking a drug for which there was no valid medical indication
1:5.8 129
Non-compliance (50%) 1:2 129
Medication error (out-patients) 1993 1:131 130
(in-patients) 1993 1:854 130
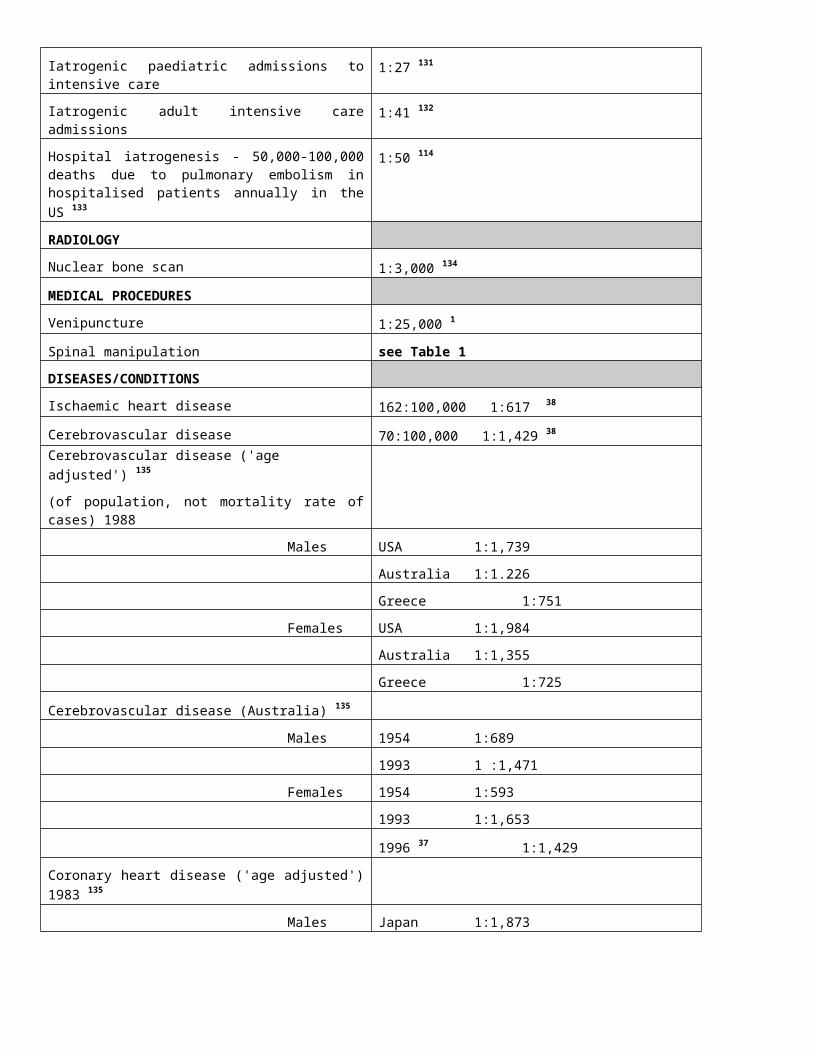
Anti-inflammatories 1 :63,333*HOSPITAL ADMISSIONSIatrogenic paediatric admissions to intensive care
1:27 131
Iatrogenic adult intensive care admissions 1:41 132
Hospital iatrogenesis - 50,000-100,000 deaths due to pulmonary embolism in hospitalised patients annually in the US 133
1:50 114
RADIOLOGYNuclear bone scan 1:3,000 134
MEDICAL PROCEDURESVenipuncture 1:25,000 1
Spinal manipulation see Table 1DISEASES/CONDITIONSIschaemic heart disease 162:100,000 1:617 38
Cerebrovascular disease 70:100,000 1:1,429 38
Cerebrovascular disease ('age adjusted') 135
(of population, not mortality rate of cases) 1988
Males USA 1:1,739
Australia 1:1.226
Greece 1:751
Females USA 1:1,984
Australia 1:1,355
Greece 1:725
Cerebrovascular disease (Australia) 135
Males 1954 1:689
1993 1 :1,471
Females 1954 1:593
1993 1:1,653
1996 37 1:1,429
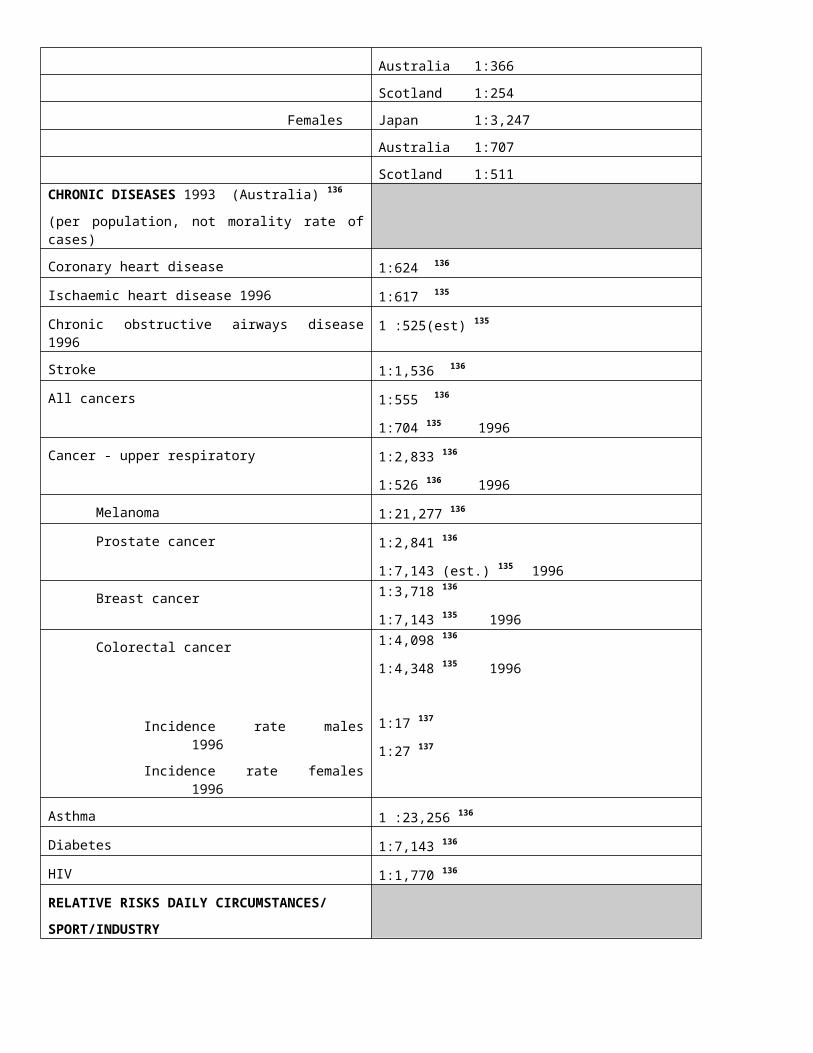
Coronary heart disease ('age adjusted') 1983 135
Males Japan 1:1,873
Australia 1:366
Scotland 1:254
Females Japan 1:3,247
Australia 1:707
Scotland 1:511CHRONIC DISEASES 1993 (Australia) 136
(per population, not morality rate of cases)
Coronary heart disease 1:624 136
Ischaemic heart disease 1996 1:617 135
Chronic obstructive airways disease 1996 1 :525(est) 135
Stroke 1:1,536 136
All cancers 1:555 136
1:704 135 1996
Cancer - upper respiratory 1:2,833 136
1:526 136 1996
Melanoma 1:21,277 136
Prostate cancer 1:2,841 136
1:7,143 (est.) 135 1996
Breast cancer 1:3,718 136
1:7,143 135 1996
Colorectal cancer
Incidence rate males 1996
1:4,098 136
1:4,348 135 1996
1:17 137
Incidence rate females1996
1:27 137
Asthma 1 :23,256 136
Diabetes 1:7,143 136
HIV 1:1,770 136
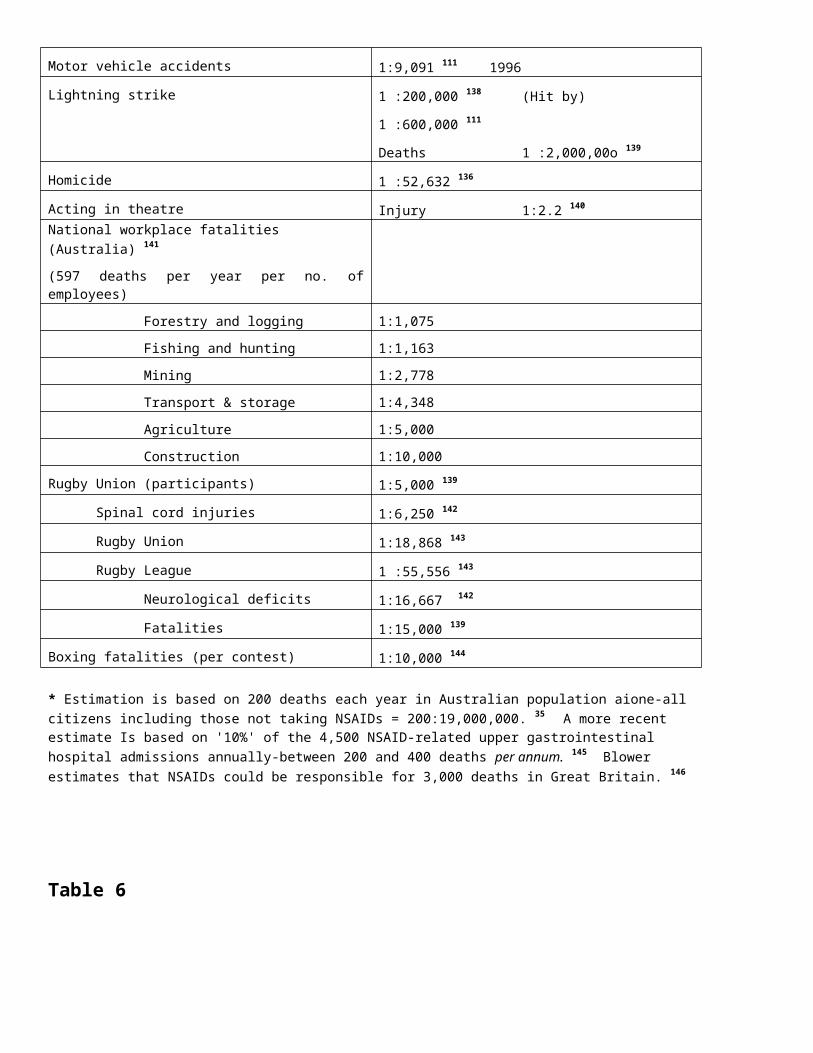
RELATIVE RISKS DAILY CIRCUMSTANCES/SPORT/INDUSTRYMotor vehicle accidents 1:9,091 111 1996
Lightning strike 1 :200,000 138 (Hit by)
1 :600,000 111
Deaths 1 :2,000,00o 139
Homicide 1 :52,632 136
Acting in theatre Injury 1:2.2 140
National workplace fatalities (Australia) 141 (597 deaths per year per no. of employees)
Forestry and logging 1:1,075
Fishing and hunting 1:1,163
Mining 1:2,778
Transport & storage 1:4,348
Agriculture 1:5,000
Construction 1:10,000
Rugby Union (participants) 1:5,000 139
Spinal cord injuries 1:6,250 142
Rugby Union 1:18,868 143
Rugby League 1 :55,556 143
Neurological deficits 1:16,667 142
Fatalities 1:15,000 139
Boxing fatalities (per contest) 1:10,000 144
* Estimation is based on 200 deaths each year in Australian population aione-all citizens including those not taking NSAIDs = 200:19,000,000. 35 A more recent estimate Is based on '10%' of the 4,500 NSAID-related upper gastrointestinal hospital admissions annually-between 200 and 400 deaths per annum. 145 Blower estimates that NSAIDs could be responsible for 3,000 deaths in Great Britain. 146
Table 6
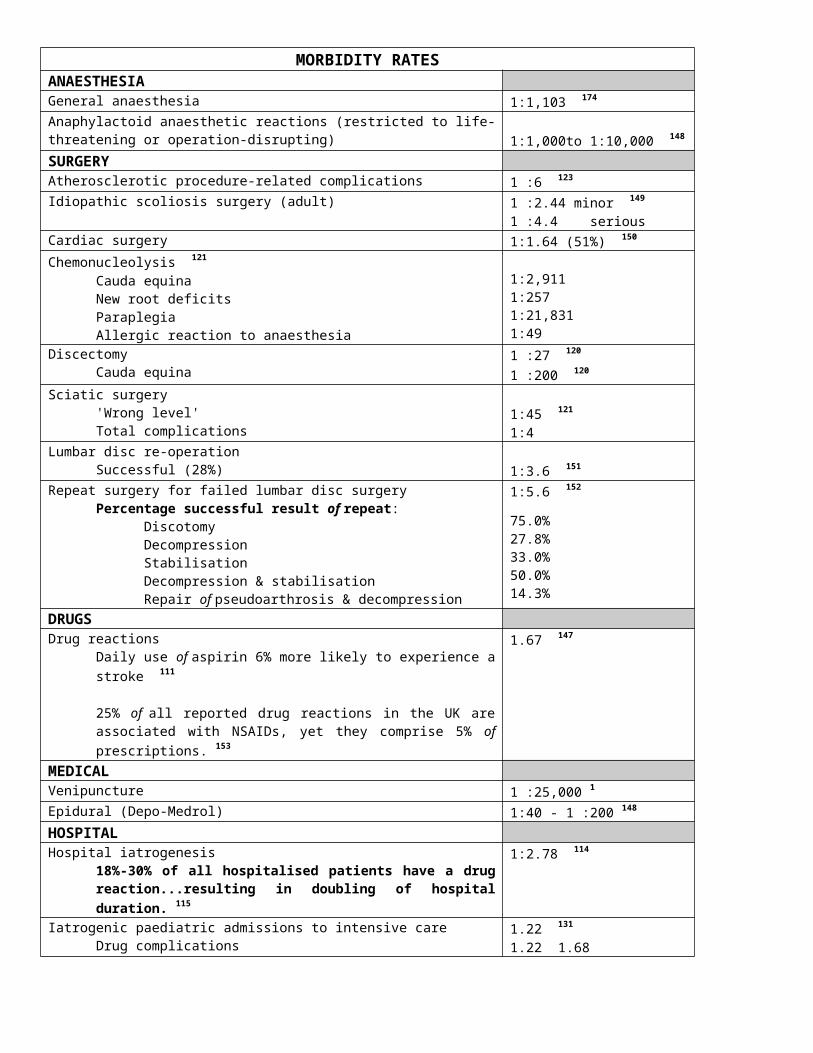
MORBIDITY RATESANAESTHESIAGeneral anaesthesia 1:1,103 174
Anaphylactoid anaesthetic reactions (restricted to life-threatening or operation-disrupting) 1:1,000to 1:10,000 148
SURGERYAtherosclerotic procedure-related complications 1 :6 123
Idiopathic scoliosis surgery (adult) 1 :2.44 minor 149 1 :4.4 serious
Cardiac surgery 1:1.64 (51%) 150
Chemonucleolysis 121
Cauda equinaNew root deficitsParaplegiaAllergic reaction to anaesthesia
1:2,9111:2571:21,8311:49
DiscectomyCauda equina
1 :27 120
1 :200 120
Sciatic surgery'Wrong level'Total complications
1:45 121
1:4Lumbar disc re-operation
Successful (28%) 1:3.6 151
Repeat surgery for failed lumbar disc surgeryPercentage successful result of repeat:
DiscotomyDecompressionStabilisationDecompression & stabilisationRepair of pseudoarthrosis & decompression
1:5.6 152
75.0%27.8%33.0%50.0%14.3%
DRUGSDrug reactions
Daily use of aspirin 6% more likely to experience a stroke 111
25% of all reported drug reactions in the UK are associated with NSAIDs, yet they comprise 5% of prescriptions. 153
1.67 147
MEDICALVenipuncture 1 :25,000 1Epidural (Depo-Medrol) 1:40 - 1 :200 148
HOSPITALHospital iatrogenesis
18%-30% of all hospitalised patients have a drug reaction...resulting in doubling of hospital duration. 115
1:2.78 114
Iatrogenic paediatric admissions to intensive careDrug complicationsSurgical complication
1.22 131
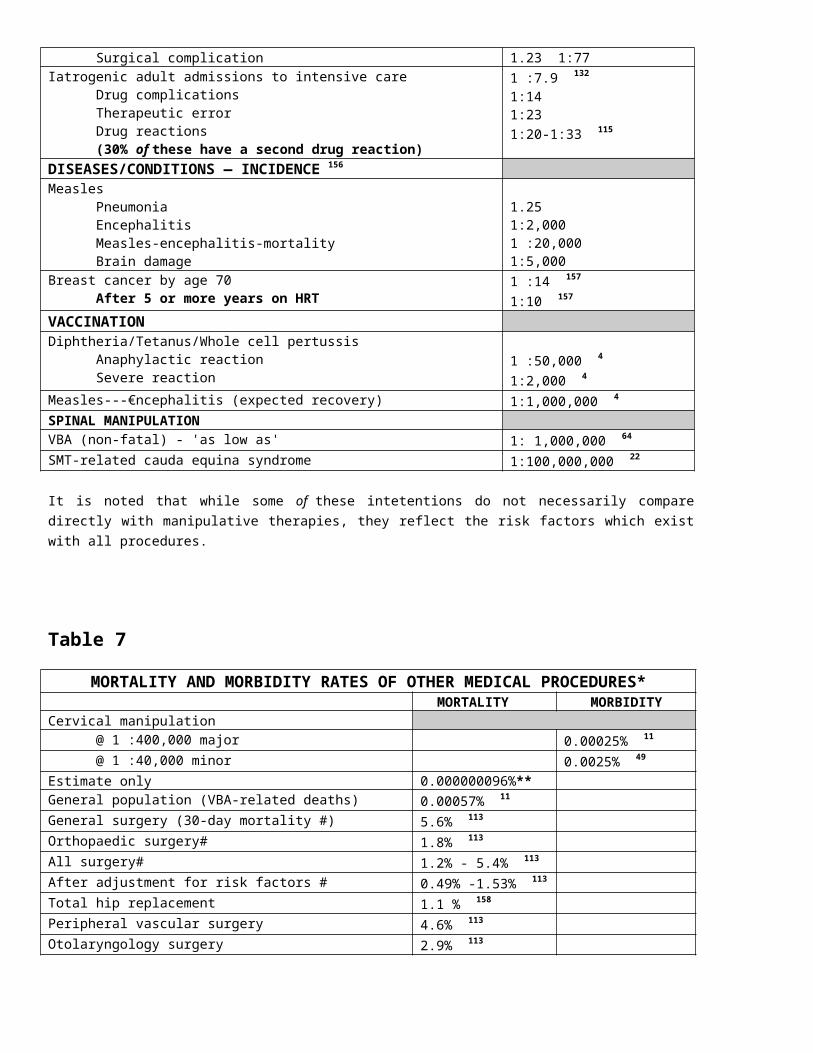
1.221.681.231:77
Iatrogenic adult admissions to intensive careDrug complicationsTherapeutic errorDrug reactions(30% of these have a second drug reaction)
1 :7.9 132
1:141:231:20-1:33 115
DISEASES/CONDITIONS — INCIDENCE 156
MeaslesPneumoniaEncephalitisMeasles-encephalitis-mortalityBrain damage
1.251:2,0001 :20,0001:5,000
Breast cancer by age 70After 5 or more years on HRT
1 :14 157
1:10 157
VACCINATIONDiphtheria/Tetanus/Whole cell pertussis
Anaphylactic reactionSevere reaction
1 :50,000 41:2,000 4
Measles---€ncephalitis (expected recovery) 1:1,000,000 4SPINAL MANIPULATIONVBA (non-fatal) - 'as low as' 1: 1,000,000 64
SMT-related cauda equina syndrome 1:100,000,000 22
It is noted that while some of these intetentions do not necessarily compare directly with manipulative therapies, they reflect the risk factors which exist with all procedures.
Table 7MORTALITY AND MORBIDITY RATES OF OTHER MEDICAL
PROCEDURES*MORTALITY MORBIDITY
Cervical manipulation@ 1 :400,000 major 0.00025% 11
@ 1 :40,000 minor 0.0025% 49
Estimate only 0.000000096%**General population (VBA-related deaths) 0.00057% 11
General surgery (30-day mortality #) 5.6% 113
Orthopaedic surgery# 1.8% 113
All surgery# 1.2% - 5.4% 113
After adjustment for risk factors # 0.49% -1.53% 113
Total hip replacement 1.1 % 158
Peripheral vascular surgery 4.6% 113
Otolaryngology surgery 2.9% 113
Iatrogenic hospital admissions 1.84% 36.0% 114
Vaccination at wrong body location 33% 159
Medication error (out-patients 1:131) .76% 130
Misinterpretation of medical jargon in laboratory reports
80% 160
Epidural anaesthesia 1.6% 161
Hospital medication: Over-prescribed/ or never used 16-20% 162
NSAIDs 0.04% 16
Liposuction (US) — 100 deaths in the past 12 months 163
Adverse effects associated with traction, 164 ultrasound, 167 acupuncture, 168 intrathecal steroid
injections, 169 and vaccination 4, 170-172 have all been reported.---------------------------------------------------------------------------------------------------------------------------------* Adapted from Khuri et al. ** Based on an approximate calculation as follows:1 00,000 man_worldwide—all professionsX 100 average cervical manipulations per week (e.g. 2 procedures/patient visit, 50 patient visits/wk)= 10,000,000 cervical manipulations/wk= 520,000,000 per year@ .5 deaths per year (see Table 1)= mortality rate of 1:1,040,000,000 = 0.000000096%
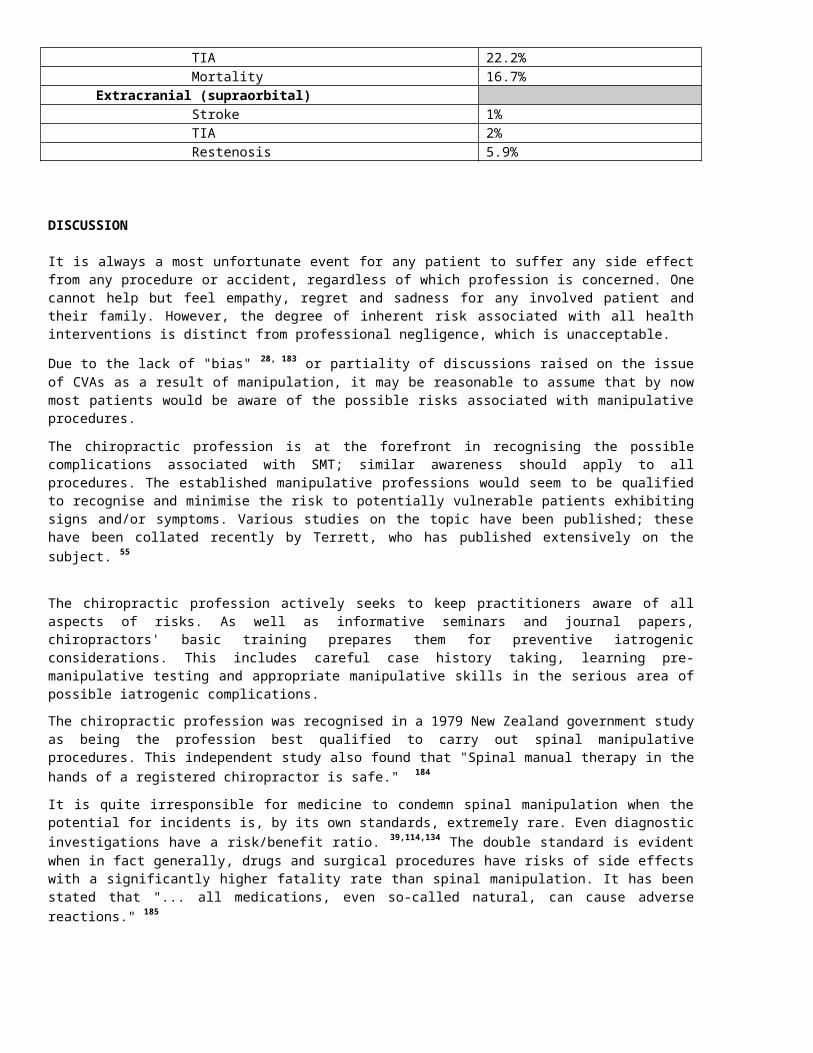
Table 8INCIDENCE OF STROKE ASSOCIATED WITH MEDICAL PROCEDURES
Australian population Deaths from stroke 1:1,639 180
Non-stroke comparisons 180
Cancer 1:565Suicide 15-24 yr/age 1 :4,000Heart disease 1:690Motor vehicle accidents 1 :3,125
Cardiopulmonary by-pass surgery 1-5:100 179
Open-heart surgery 0.3% - 5.2% 181
Coronary by-pass surgery 6.1% 34
Percutaneous transluminal angioplasty 123
IntracranialStroke 33.3%TIA 22.2%Mortality 16.7%
Extracranial (supraorbital)Stroke 1%TIA 2%Restenosis 5.9%
DISCUSSION
It is always a most unfortunate event for any patient to suffer any side effect from any procedure or accident, regardless of which profession is concerned. One cannot help but feel empathy, regret and sadness for any involved patient and their family. However, the degree of inherent risk associated with all health interventions is distinct from professional negligence, which is unacceptable.
Due to the lack of "bias" 28, 183 or partiality of discussions raised on the issue of CVAs as a result of manipulation, it may be reasonable to assume that by now most patients would be aware of the possible risks associated with manipulative procedures.
The chiropractic profession is at the forefront in recognising the possible complications associated with SMT; similar awareness should apply to all procedures. The established manipulative professions would seem to be qualified to recognise and minimise the risk to potentially vulnerable patients exhibiting signs and/or symptoms. Various studies on the topic
have been published; these have been collated recently by Terrett, who has published extensively on the subject. 55
The chiropractic profession actively seeks to keep practitioners aware of all aspects of risks. As well as informative seminars and journal papers, chiropractors' basic training prepares them for preventive iatrogenic considerations. This includes careful case history taking, learning pre-manipulative testing and appropriate manipulative skills in the serious area of possible iatrogenic complications.
The chiropractic profession was recognised in a 1979 New Zealand government study as being the profession best qualified to carry out spinal manipulative procedures. This independent study also found that "Spinal manual therapy in the hands of a registered chiropractor is safe." 184
It is quite irresponsible for medicine to condemn spinal manipulation when the potential for incidents is, by its own standards, extremely rare. Even diagnostic investigations have a risk/benefit ratio. 39,114,134 The double standard is evident when in fact generally, drugs and surgical procedures have risks of side effects with a significantly higher fatality rate than spinal manipulation. It has been stated that "... all medications, even so-called natural, can cause adverse reactions." 185
Because of medicine's self-serving publicity about SMT, discerning patients may see through what appears to be the charade of biased scaremongering. Nevertheless, the demand for qualified manipulative care continues to expand. A significant proportion of the population — almost 50% 186 of patients — actively seek an appropriate alternative approach to their health problems. One must assume this option is exercised either as a preference, a search for results, or choosing not to accede to chemical or surgical intervention.
In 1998, Wilks expressed surprise at the limited exposure of a 1987 American federal court finding that the American Medical Association "... was dishonest, untrustworthy (and) not objectively reasonable" when it acted to neutralise the competition and influence of chiropractic on the health care scene. 187 The referenced literature and media similarly appear to have been noticeably reticent on this particular issue of a single profession's (medicine's) domination of the entire health field. Strangely the media, and society in general, do not appear to want to seriously question medical philosophy, paradigm, monopolisation, efficacy, costs or procedures. 188
Medicine has adopted terms suggesting procedures have an "acceptable risk." These include "risk-adjusted mortality rates," "net clinical benefit" and "risk/benefit ratio," yet there seems a reluctance to concede the application of these terms to procedures outside the medical profession. 172 It seems that at times "such rates have been condoned" — at least in relation to dural puncture, 189 or in immunisation programs where "the benefits of preventing the disease far outweigh the risks of vaccination." 172
Lack of Government Standards or Guidelines
Regardless of the low rate of incidents in the manipulative sciences, the material reviewed warrants advocacy of further caution and awareness, with continued endeavours towards risk elimination. It is fundamental for the manipulative professions to maintain the maximum available level of recognised safety, training and education before employing their conservative manipulative procedures. 190
As mentioned, although some SMT-related accidents may be unforeseen, 28,61,191 for the vast majority there are procedures for both recognising and determining patients at risk. Essential education has been established for this purpose.
Despite the importance of public interest in standards of care, the Australian state legislatures have created a distinct anomaly through standardisation and mutual recognition of registration acts for health professions. For instance, the Victorian government's Chiropractors Registration Act and the Osteopathic Registration Act have, through an implication by considered omission, sought no standards or requirements placed upon unregistered practitioners who attempt spinal manipulation. 192 That is, any person in Victoria may carry out neck manipulation so long as he does not present himself as a chiropractor, osteopath, physiotherapist or medical practitioner.
Australian state governments do not require minimal training standards for the manipulative procedures utilised by non-registered practitioners — only for registered manipulative professionals who specialise in the field. This also allows medical practitioners to attempt to manipulate the spine, even if they have no training whatsoever in the procedures. This would seem incongruous when "protection of the public" and "standards" were two of the primary criteria for establishing registration for the manipulative professions in the first place, as would seem to be the case with all health professions. 193-195
Such a fundamental safeguard would seem even more important in health care where primary contact care practitioners are responsible for the diagnosis as well as the safe and effective management of patients' welfare and health problems. As has been indicated earlier, practitioners not formally trained or qualified in SMT have been associated with incidents of CVAs 54,111 (see Table 4).
The kind of legislative policy that currently exists would tend to support the questionable assertion that practitioners need not be qualified to render SMT, that there is relatively little concern for any danger from any SMT side-effects, or indeed, that there is any perceived danger at all.
SUMMARY
While there are some stated limitations to this type of review, a number of matters were discussed in attempting identify related issues: The rate of adverse effects, namely cerebrovascular accidents related to spinal
manipulative therapy, was shown to be extraordinarily low in the overall health care scene. The rate of SMT-related CVAs associated with the chiropractic profession is lower than for
osteopathy and medicine. Figures could not be determined for physiotherapy. In general terms, the rate of SMT-related CVA is also lower than the rate of strokes in the
general population. Morbidity and mortality rate of S MT is far lower than that suffered by patients taking
NSAIDs. There are both identifiable and unidentifiable anomalies, weaknesses, diseased states and
conditions which can influence the incidence of apoplexy in society. There is a significant percentage of spontaneous apoplexy in the general population, and
therefore, at times, such a high "natural" frequency could be confused as an SMT-related incident.
The rate of preventable drug- and surgery-related iatrogenic illness in medicine is generally far higher than for SMT, demonstrating SMT to be a safe and conservative form of intervention by comparison.
The rate of vertebrobasilar accidents associated with manipulation has been grossly exaggerated, inaccurate and sensationalised by some ill-informed sources.

SMT in the hands of a practitioner properly qualified in this specialty is shown to be a particularly safe procedure.
There appear to be medico-political overtones to the subject of SMT-related iatrogenesis.
CONCLUSIONS
This paper has attempted to identify perspectives of iatrogenesis and contrast levels of morbidity and mortality with a number of elements which may adversely affect health. In drawing such comparisons, it is worthwhile to understand where SMT is situated in relation to complications related to other forms of intervention.
It is incumbent upon practitioners of all professions to be aware of the risks involved in every type of procedure. Patients are also entitled to accurate information about the procedures that may be utilised in the course of their care. Not only do practitioners have a role in providing this information, but the scientific literature, as well as the printed and electronic popular media who report any adverse incidents must be responsible and accurate in this duty.This review of the evidence has indicated that a potential risk of catastrophic side-effects from SMT is substantially less than for any of the medical procedures or interventions listed in the tables accompanying this paper.It is submitted that as reflected in the demand for therapy, spinal manipulation has contributed significantly to the health and well-being of much of the world's population. Unsubstantiated published opinions and so-called scientific distortions of the facts are irresponsible. There are no "double-blind controlled scientific studies" which reject a reasonable degree of efficacy of spinal manipulation for appropriate mechanical back and neck conditions — indeed, quite the opposite. 196-199
In conducting this study it has been shown that the distorted impression of risk associated with cervical spinal manipulation should be cast in the proper and minimal perspective which is its due. It would be hoped that any reservations which dissuade qualified practitioners from utilising cervical spinal manipulation in appropriate situations, or dissuades patients from accepting and subsequently benefiting from such techniques, would be mitigated, and the rationale for the therapy better understood.If medicine is to assume a scientific role, it must also record accurately, fairly and without prejudice on such scientific matters concerning health and welfare. In this author's opinion, it is demonstrably wrong and scurrilous to portray SMT as a highly dangerous procedure — both in its own right, and in light of the facts concerning other procedures. It is both a judicious and propitious procedure which is safe by comparison and may perhaps explain medicine's increasing interest in adopting SMT as one of its own regimes.
As inferred by Assendelft et al., 28 it is up to the properly informed patient and practitioner to compare the risk/benefit ratio in choosing to seek relief through a particular type of intervention. To this end, conservative procedures like spinal manipulation would appear to have a distinct advantage due to there inherently low risk.Without wishing to diminish the importance and serious nature of cardiovascular incidents related to SMT, and with due recognition for continued caution for its potential, the miniscule risk which may be associated with SMT is extraordinarily low and should be encouraged and endorsed as a safe front-line health procedure.It has been suggested here that there is a relatively high incidence of CVA in the general population, that there can be a number of predisposing conditions related to CVAs, that spontaneous CVAs are relatively common, and that there can be a number of common activities associated with CVAs.
The professions who utilise spinal manipulation must strive for continued minimisation of possible SMT-related side effects — indeed, their elimination — but the facts and statistics
presented here suggest that given the nature of its considered neural influence, and with all the information in perspective, spinal manipulation in the hands of an appropriately qualified professional is both conservative and one of the safest therapeutic procedures.
ACKNOWLEDGEMENT
The author gratefully appreciates the assistance provided by Dr Damon Willmore for his input and assistance in the preparation of this paper.
REFERENCES
1. Horowitz SH. Peripheral nerve injury and causalgia secondary to routine venipuncture. Neurol 1994; 44: 962-964
2. Caswell A, editor. MIMS Annual, Australian edition.. 22nd ed. St Leonards, NSW: MediMedia Publishing, 1998
3. Anon. Readers' Q & A. Aust Med 1998; Oct 5: 18
4. Burgess MA, Mcintyre PB, Heath TC. Rethinking contradictions to vaccination. Med J Aust 1998; 68: 476-477
5. Stremple JF, Boss DS, Davis CH, McDonald GO. Comparison of post-operative mortality and morbidity in Veteran Affairs and non-federal hospitals. J Surg Res 1994; S6: 405-416 [Cited by Willmore 115]
6. Toy M-A. Vision for laser surgery loses its shine—Seeing is believing. The Age, Melbourne 1998;Nov 7: 15
7. European Carotid Surgery Trialists' Collaborative Group. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998; 351: 1379-1387
8. White WH. Strokes and net clinical benefit. Aust NZ J Med 1993; 23: 737-738
9. Terrett AGJ. Vascular accidents from cervical spine manipulation: Report of 107 cases. J Aust Chiropr Assoc 1987; 17: 15-24
10. Donnana G. Strokes to rise. The Herald Sun, Melbourne 1998; Sept 30: 26
11. Myler L. A risk assessment of cervical manipulation vs. NSAIDs for the treatment of neck pain [letter]. J Manipulative Physiol Ther 1996; 19:357
12. Terrett AGJ. Contraindications to cervical spine manipulation. In: Giles LFG, Singer KP, editors. Clinical anatomy and management of cervical spine pain. Oxford: Butterworth-Heineman, 1998: 182-210
13. Mas JL, Bousser MG, Hasboun D, Laplane D. Extracranial vertebral artery dissection: A review of 13 cases. Stroke 1987; 18: 1037-1047
14. Fraser RAR, Zimbler SM. Hindbrain stroke in children caused by extracranial vertebral artery trauma. Stroke 1975; 6: 153-159
15. Frumkin LP, Raloh Rw. Wallenberg's syndrome following neck manipulation. Neurol 1990; 40: 611-615

16. Dabbs V, Lauretti WJ. A risk assessment of cervical manipulation vs NSAIDs for the treatment of neck pain. J Manipulative Physiol Ther 1995; 18: 530-536
17. Cyriax J. Text-book of orthopaedic medicine. Vol 1: Diagnosis of soft tissue lesions. 4th ed. London: Cassell, 1963: 174
18. Livingstone MCP. Spinal manipulation in medical practice: A century of ignorance. Med J Aust 1968; 1: 552-555
19. Maigne R. Orthopaedic medicine: A new approach to vertebral manipulations. Springfield: Charles C. Thomas, 1972: 169
20. Jaskoviak PA. Complications arising from manipulation of the cervical spine. J Manipulative Physiol Ther 1980; 3: 213-219
21. KJougart N, Leboeuf-Yde C, Rasmussen LR. Safety in chiropractic practice. Part 1. The occurrence of cerebrovascular accidents after manipulation to the neck in Denmark from 1978-1988. J Manipulative Physiol Ther 1996; 19: 371-377
22. Shekelle PG,Adams AH, Chassin MR, Hurwitz EL, Brook RH. Spinal manipulation for back pain. Ann Intern Med 1992; 117: 590-598
23. Carey PF. A report on the occurrence of cerebral vascular accidents in chiropractic practice. J Can Chiropr Assoc 1993; 37: 104-106
24. Haynes MJ. Stroke following cervical manipulation in Perth. Chiropr J Aust 1994; 24: 42-46
25. Lauretti WJ. Spinal manipulation [letter]. J Fam Pract 1996; 43: 333-334
26. Lauretti WJ. Chiropractic complications [letter]. Neurol 1996; 46: 884
27. Michaeli A. Reported occurrence and nature of complications following manipulative physiotherapy in South Africa. Aust Physiother 1993; 39: 309-315
28. Assendelft WJJ, Bouter LM, Knipschild PG. Complications of spinal manipulation. A comprehensive review of the literature. J Fam Pract 1996; 42: 475-480
29. Tauro J. Chiropractic complications [letter]. Neurol 1996; 46: 884
30. Michaeli A. Spinal manipulation by physiotherapists in South Africa: Result of a questionnaire. Physiother 1992; 78: 673-678
31. Michaeli A. Dizziness testing of the cervical spine: Can complications of manipulations be prevented? PhysiotherTheor Pract 1991; 7: 243-250
32. Carter H. Chiropractic found to ease brain injury. Herald Sun, Melbourne 1998; Sept 30: 30
33. Carrick FR. Changes in brain function after manipulation of the cervical spine. J Manipulative Physiol Ther 1997; 20: 529-545
34. Roach GW, Kanchuger M, Mangano CM, Newman M, Nussmeier N, Wolman R, et at. Adverse cerebral outcomes after coronary bypass surgery. New Engl J Med 1996; 335: 1857-1863
35. Cooke J. Cutback on fatal arthritis drugs. Sydney Morning Herald 1992; Nov 18: 12
36. Carter H. Hopes on safer arthritis drug. Herald Sun, Melbourne 1998; Jan 6: 9
37. Woodward M. Preventing strokes. Veterans' Health. Newsletter from the Department of Veterans' Affairs, Canberra 1997; 61: 18-20
38. Anon. Causes of death in Australia, 1996. Med J Aust 1998; 169: 5
39. HankeyGJ. Transient ischaemic attacks. MedJAust 1995; 162: 260-263
40. Hart RG. Vertebral artery dissection. Neurology 1988:38: 987-989
41. Mokri B, Houser OW, Sundt AM. Idiopathic regressing anteriopathy. Ann Neurol 1977; 2: 466-472
42. Mokri B, Houser OW, Sandok BA, Pipgras DG. Spontaneous dissections of the vertebral artery. Neurol 1988; 38: 880-885
43. Mas J-L, Goeau C, Bouser M-G, Chiras J, Verret J-M, Touboul P-J. Spontaneous dissecting aneurysms of the internal carotid and vertebral arteries: Two case reports. Stroke 1985; 16: 125-129
44. Sherman DG, Hart RG, Easton JD. Abrupt change in head position and cerebral infarction. Stroke 1981; 12: 2-6
45. Schievink WI, Mokri B, O'Fallon WM. Recurrent spontaneous cervical artery dissection. New Engl J Med 1994; 330: 393-397
46. Swenson RS. Spontaneous vertebral artery dissection: A case report. J Neuromusculoskeletal Syst 1993 (1): 10-3
47. Drake M. Cricket ball death was freakish, says coroner. The Age, Melbourne 1987; June 11: 7
48. Kaufman HH, Harris JH, Spencer JA, Kopansky DR. Danger of traction during radiography for cervical trauma [letter]. JAMA 1982; 247:2369
49. Leach RA. The chiropractic theories: Principles and clinical applications. 3rd ed. Baltimore: Williams and Wilkins, 1994:285-97
50. Hope EE;-Bodensteiner JB, Barnes P. Cerebral infarction related to neck position in the adolescent. Pediatr 1983; 72:335-7
51. Husni EA, Bell\HS, Storer J. Mechanical occlusion of the vertebral artery. A new clinical concept. JAMA 1966; 196: 475-478
52. Husni EA, Storer J. The syndrome of mechanical occlusion of the vertebral artery: Further observations. Angiology 1967; 18: 106-16
53. Hardin CA, Poser CM. Rotational obstructions of the vertebral artery due to redundancy and extraluminal fascial bands. Ann Surg 1963; 158: 133-137
54. Terrett AGJ. Misuse of the literature by-medical authors in discussing spinal manipulative therapy injury. J Manipulative Physiol Ther 1995; 18: 203-210
55. Terrett AGJ. Vertebrobasilar stroke following manipulation. West Des Moines, IA: National Chiropractic Mutual Insurance Company, 1996
56. McKechnie B. Manipulative vascular accidents in proper perspective. Part I: Dynamic Chiropr 1994; 12 (16): 25, 37. ~ and ~ Part II: Dynamic Chiropr 1994; 12 (18): 28-9
57. Silverstein A, Present DH. Cerebrovascular occlusions in relatively young patients with regional enteritis. JAMA 1971; 215: 976-977
58. Nelson J, Barron MM, Riggs JE, Gutmann L, Schochet S. Cerebral vasculitis and ulcerative colitis. Neurol 1986; 36: 719-721
59. Yassinger S, Adelman R, Cantor D, Halsted CH, Bolt RJ. Association of inflammatory bowel disease and large vascular lesions. Gastroenterol 1976; 71: 844-846
60. Sturzenegger M. Headache and neck pain: The warning symptoms of vertebral artery dissection. Headache 1994; 34: 187-193
61. Fogelholm R, Karli P. 'Iatrogenic' brain stem infarction. A complication of x-ray examination of the cervical spine and following posterior tamponade of the nose. Eur Neurol 1975; 12: 6-12
62. Yang PJ, Latack JT, Gabrielsen TO, Knake JE, Gebarski SS, Chandler, et al. Rotational vertebral artery occlusion at C 1-C2. Stroke 1985; 6: 98-100
63. Zimmerman AW, Kumar AJ, Gadoth N, Hodges FJ. Traumatic vertebrobasilar occlusive disease in childhood. Neurol 1978; 28: 185-188
64. Hamann G, Haass A, Kujat C, Felber S, Strittmatter M, Schimrgk, ef al. Cervicocephalic artery dissections due to chiropractic manipulations [letter]. Lancet 1993; 341 : 764-765
65. Weintraub MI. Beauty .Parlour stroke syndrome: Report of five cases. JAMA 1993; 269: 2085-2086
66. Yates PO. Birth trauma to the vertebral arteries. Arch Dis Child 1959; 34: 431-436
67. Dorey RSA, Mayne V. Break-dancing injuries [letter]: Med J Aust 1986; 144: 610-611
68. McBride DO, Lehman CP, Mangiardi JR. Break-dancing neck. New Engl J Med 1985; 312: 186
69. Leung AK. Hazards of breakdancing. NY State J Med 1984; 84: 592
70. Nagler W. Vertebral obstruction by hyperextension of the neck: A report of three cases. Arch Phys Med Rehabil 1973; 54: 237-240
71. Pryse-Phillips W. Infarction of the medulla and cervical cord after fitness exercises. Stroke 1989; 20: 292-294
72. Schneider RC, Schemm GW. Vertebral artery insufficiency in acute and chronic spinal trauma. J Neurosurg 1961; 18: 348-360
73. Weinstein SM, Cantu RC. Cerebral stroke in a semi-pro football player: A case report. Med Sci Sports Exerc 1991; 23: 1119-1121. [Cited by Terrett 12]
74. Marks RL, Freed MM. Non-penetrating injuries of the neck and cerebrovascular accident. Arch Neurol 1973; 28: 412-414
75. Boldrey E, Maas L, Miller E. The role of allantoid compression in the etiology of internal carotid thrombosis. J Neurosurg 1956; 13: 127-139
76. Nwokolo N, Bateman DE. Stroke after a visit to the hairdresser. Lancet 1997; 350: 866
77. Brown BStJ, Tallow WFT. Radiographic studies of the vertebral arteries in cadavers: Effects of posture and traction on the head. Radiol 1963; 81: 80-88
78. Oh VMS. Brain infarction and neck callisthenics. Lancet 1993; 342: 739-740
79. Tettenborn B, Caplan LR, Sloan MA, Estrol CJ, Pessin MS, DeWitt LD, et al. Post-operative brainstem and cerebellar infarcts. Neurol 1993; 43: 471-477
80. Okawara S, Nibbelink D. Vertebral artery occlusion following hyperextension and rotation of the head. Stroke 1974; 5: 640-642
81. Fritz VU, Malon A, Tuch P. Neck manipulation causing stroke. S Afr Med J 1984; 66: 844-846
82. Wagner M, Kitzerow E, Taitel A. Vertebral artery insufficiency. Arch Surg 1963; 87: 885-886
83. Tallow WIT, Bammer HG. Syndrome of vertebral artery compression. Neurol 1957; 7: 331-340
84. Grossman RI, Davis KR. Positional occlusion of the vertebral artery: A rare cause of embolic stroke. Neuroradiol 1982; 23: 227-230
85. Norman RA, Grodin MA. Injuries from break-dancing. Am Fam Physician 1984; 4: 109-112
86. Gascoemsio PJ, Leurauos L. Injury caused by break-dancing. JAMA 1984; 252: 3367
87. Biousse V, Chabriat H, Awarenco P. Roller-coaster-induced vertebral artery dissection (letter]. Lancet 1995; 346: 767
88. Bo-Abbas Y, Bolton CF. Roller-coaster headache. New Engl J Med 1995; 332: 1585
89. Brain L. Some unsolved problems of cervical spondylosis. Br Med J 1963; 1: 771-777
90. CookJW, SansteadJK. Wallenberg's syndrome following self-induced manipulation. Neurol 1995; 41: 1495-1496
91. Schellhas KP, Latchaw RE, Wendling LR, Gold HA. Vertebrobasilar injuries following cervical manipulation. JAMA 1980; 244: 1450-1453
92. Tramo MJ, Hainline B, Petito F, Lee B, Caronna J. Vertebral artery injury and cerebellar stroke while swimming: Case report. Stroke 1985; 16: 1039-1042
93. Mourad J-J, Giererd X, Safar M. Carotid artery dissection after a prolonged telephhone call [letter]. New Engl J Med 1997; 333: 516
94. Klein RA, Snyder RD, Schwartz HJ. Lateral medullary syndrome in a child: Arteriographic conformation of vertebral artery occlusion. JAMA 1976; 235: 940-941
95. Easton JD, Sherman DG. Cervical manipulation and stroke. Stroke 1977; 8: 594-597
96. Simeone FA, Goldberg HI. Thrombosis of the vertebral artery from hyperextension injury to the neck. Case report. J Neurosurg 1968; 29: 540-544
97. Grinker RR, Guy Cc. Sprain of cervical spine causing thrombosis of anterior spinal artery.

JAMA 1927; 88: 1140-1142
98. Hanus SH, Homer TD, Harter DH. Vertebral artery occlusion complicating yoga exercises. Arch Neurol 1977; 34: 574-575
99. Berger JR, Sheremata WA. Persistent neurological deficit precipitated by hot bath test in multiple sclerosis. JAMA 1983; 249: 1751-1752
100. Davis FA. Neurological deficits following the Hot Bath Test in multiple sclerosis. JAMA 1985;
253: 203
101. De Fabio RP. Manipulation of the cervical spine: Risks and benefits. Phys Ther 1998; 79: 50-65
102. Winterstein JF. Spinal manipulation [letter]. J Fam Pract 1996; 43: 333
103. Michaeli A. Reported occurrence and nature of complications following manipulative physiotherapy in South Africa. Aust Physiother 1993; 39 (4): 309-315
104. Parker PJ, Wallis WE, Wilson JL. Vertebral artery occlusion following manipulation of the neck. NZ Med J 1978; 88: 441-443
105. Lyness SS, Wagman AD. Neurological deficit following cervical manipulation. Surg Neurol 1974; 2: 121-124
106. Danesmend TK, Hewer RL, Bradshaw JR. Acute brain stem stroke during neck manipulation. Br Med J 1984; 288: 189
107. Cooper G. Osteopathic manipulation resulting in damage to spinal cord. Br Med J 1985; 291:
1538-1541
108. Tauro J Chiropractic complications (letter]. Neurol 1996; 46: 884
109. Ford FR, Clark D. Thrombosis of the basilar artery with softenings in the cerebellum and brain stem due to manipulation of the neck. Bull Johns Hopkins Hosp 1956; 98: 37-42
110. Rothrock JF, Hesselink JR, Teacher TM. Vertebral artery occlusion and stroke from cervical self- manipulation. Neurol 1995; 41 : 1496-1497
111. Bohm J. Cervicocephalic artery dissections due to chiropractic manipulations (letter]. Lancet 1993;
341: 1214
112. Terrett AGJ. Personal communication, August 1998
113. Khuri SF, Daley J, Henderson W, Hur K, Gibbbs JO, Barbour G, el at. Risk adjustment of the post-operative mortality rate for the comparison assessment of the quality of surgical care. Results of the National Veterans Affairs surgical risk study. J Am Coli Surg 1997; 185: 315-340
114. Steel K, Gertman PM, Crescenzi C,Anderson J. Iatrogenic illness on a general medical service at a university hospital. New Engl J Med 1981; 304: 638-642 Cited in: Iatrogenic Illness: How frequently does it occur? [extracts]. Mod Med Aust 1982; July: 51
115. Willmore D. You're in safe hands: The relative risks of chiropractic care. Unpublished
research 1998
116. Steiner CA, Bass EB, Talamini MA, Pitt HA, Steinberg EP. Surgical rates and operative mortality for open and laparoscopic cholecystectomy in Maryland. New Engl J Med 1994; 330: 403-408 (cited by Willmore 115)
117. Stolke D, Sollman WP, Seifert V. Intra-and post-operative complications in lumbar disc surgery. Spine 1989; 14: 56-58
118. Bedell SE, Deitz DC, Leeman D, Delbanco TL. Incidence and characteristics of preventable iatrogenic cardiac arrests. JAMA 1991; 265: 2815-2820
119. Bellestra-Lopez C, Vallet-Fernandez J, Catarci M, Bastida-Vila X, Nieto-Martinez B. Iatrogenic perforations of the esophagus. Int Surg 1993; 78: 28-31 (cited by McKechnie 55)
120. Kardaun JW, White LR, Shaffer WO Acute complications in patients with surgical treatment of lumbar herniated disc. J Spinal Disorders 1990; 3 (1): 30-38
121. Bouillet R. Treatment of sciatica. A comparative survey of complications of surgical treatment and nucleolysis with chymopapain. Clin Orthop Rel Res 1990; 251: 144-152
122. Deyo RA, Cherkin DC, Loeser JD, Bigos SJ, Ciol MA. Morbidity and mortality in association with operations on the lumbar spine. J Bone Jt Surg 1992; 74-A: 5536-5543
123. Volk EE, Prayson RA, Perl J. Autopsy findings of fatal complications of posterior cerebral circulation angioplasty. Arch Path Lab Med 1997; 121: 738-740
124. Shapiro S, Slone D, Lewis GP, Jick H. Fatal drug reactions among medical patients. JAMA 1971; 216: 467-472
125. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients. A meta-analysis of prospective studies. JAMA 1998; 279: 1200-1205
126. Borda IT. Assessment of adverse reactions within a drug surveillance program. JAMA 1968; 205 (9): 99-101
127. Wang RIH, Terry Lc. Adverse drug reactions in a veterans administration hospital. J Clin Pharmacol 1971; 11: 14-18
128. Porter J, Jick H. Drug-related deaths among medical inpatients. JAMA 1977; 237: 879-881
129. East KL, Parsons BJ, Starr M, Brien JE. The incidence of drug-related problems as a cause of hospital admissions in children. Med J Aust 1998; 169: 356-359
130. Phillips DP, Christenfeld N, Glynn LM. Increase in US medication error deaths between 1983 and 1993. Lancet 1998; 351 : 643-644
131. Stamouly JP, Pollack MM. Iatrogenic illnesses in pediatric critical care. Crit Care Med 1990; 18: 1248-1251 (cited by McKechnie 55)
132. Trunet P, Le Gall J-R, Lhoste F, Regnier B, Saiilard Y, Carlet J, et al. The role of iatrogenic disease in admissions to intensive care. JAMA 1980; 244: 2617-2620
133. King M. Preventing deep venous thrombosis in hospitalised patients. Am Fam Physician 1994; 49: 1389-1396

134. Roebuck DJ. Diagnostic imaging: Reversing the focus [letter]. Med J Aust 1995; 162: 275
135. D'Espaignet ET. Trends in Australian mortality. In: Diseases of the circulatory system: 1950-1991. Canberra: Australian Government Publishing Service, 1994:49-64
136. Abraham B, d'Espaignet ET, Stevenson C. Australian health trends 1995. Canberra: Australian Institute of Health and Welfare, 1995: 34-47
137. Anon. Colorectal cancer. Med J Aust 1998; 169: 5
138. Heywood J, Carson A. Lightning sparks bushfire havoc across state. The Age, Melbourne 1998; Dee 26:3
139. Maharaj JC, Cameron D. Increase in spinal injury among rugby union players in Fiji [letter]. Med J Aust1998; 168: 418
140. Anon. Break a leg. Med J Aust 1998; 169: 442 (citing Occup Environ Med 1998; 55: 585-593)
141. Trinca H. Work accidents kill 11 a week. The Age, Melbourne 1998; Dee 7: 5 (citing a National Occupational Health and Safety Commission Survey 1988-1992)
142. Rotem TR, Lawson JS, Wilson SF, Engel S, Rutkowski SB, Aisbett CW Severe cervical spinal cord injuries related to rugby union and league football in New South Wales, 1984-1996. Med J Aust 1998; 168: 379-381
143. Wilson SF, Atkin PA, Totem T, Lawson J. Spinal cord injuries have fallen in rugby union players in New South Wales [letter]. Br Med J 1996; 313: 1550
144. Pearn J. Reducing brain damage in boxers [letter]. Med J Aust 1998; 168: 418
145. Day RO, Rowett D, Roughhead EE. Towards the safer use of non steroidal anti-inflammatory drugs. J Qual Clin Pract 1999; 19: 51-53
146. Blower AL, Armstrong CP Ulcer perforation in the elderly and non steroidal anti-inflammatory drugs. Lancet 1986; 1 : 971
147. Tuchin P. Manual therapy carries low risk. Aust Doctor 1997; Feb 7: 5
148. Laxenaire MC, Moneret-Vautrin DA, WatkinsJ. Diagnosis and causes of anaphalactoid anaesthetic reactions. Anaesth 1983; 38: 147-148
149. Sponseller PD, Cohen MS, Nachemson AL, Hall JE, Wohl EB. Results of surgical treatment of adults with idiopathic scoliosis. J Bone Jt Surg 1987; 69-A: 667-675
150. Tettenborn B, Caplan LR, Sloan MA, Estol CJ, Pessin MS, DeWitt LD, et al. Post-operative brainstem and cerebellar infarcts. Neurol 1993; 43: 471-477
151. Law JD, Lehman RAW, Kirsch WM. Re-operation after lumbar intervertebral disc surgery. J Neurosurg 1978; 48: 259-263
152. Waddell G, Kummel EG, Lotto WN, Graham JD , Hall H, McCulough JA. Failed lumbar disc surgery and repeat surgery following industrial injuries. J Bone Jt Surg 1979; 61-A: 201-207
153. Gomes JA, Roth SH, Zeeh J, Bruyn GAW, Woods EM, Geis GS. Double-blind comparison of efficacy and gastroduodenal safety of diclofenac/misoprostol, piroxicam, and
naproxen in the treatment of osteoarthritis. Ann Rheum Dis 1993; 52: 881-885
154. Tress B, Lau L. Depo-Medrol and facet joint injections Australasian Radiol 1991; 35: 291
155. Melmon KL. Preventable drug reactions--causes and cures. New Engl J Med 1971; 284: 1361-1368
156. Lally G. Cause for concern. Herald Sun, Melbourne 1998; July 7: 5
157. Auchincloss S. Facts a casualty in medicine. Onus on doctors to keep up to date with research. Aust Doctor 1998; Oct 23: 27
158. Seagroat V, Tan HS, Goldacre M, Bulstrode C, Nugent I, Gill L. Elective total hip replacement: Incidence, emergency readmission rate, and post-operative mortality. Br Med J 1991; 330: 1431-1435
159. Dow S. Vaccination report needles GPs. The Age, Melbourne, 1995; Mar 11
160. Lee A. Doctors fooled by lab reports: A Survey. The Age, Melbourne circa 1978
161. MacArthur C, Lewis M, Knox EG. Accidental dural puncture in obstetric patients and long term symptoms. Br Med J 1993; 306: 883-885
162. Miller BM. Hospital drug error rate 'seriously high'. The Age, Melbourne 1979; Oct 2
163. Marshall D. Liposuction warning. Quoted in The Herald Sun, Melbourne 1998; Sept 30: 26
164. Horsley M, Taylor TK, Sorby WA. Traction induced rupture of an extracranial vertebral artery aneurysm associated with neurofibromatosis: A case report. Spine 1997; 22: 225-227
165. Gruenberg MF, Rechtine R, Chrin AM, Sola CA, Ortulan EG. Overdistraction of cervical spine injuries with the use of skull traction: A report of 2 cases. J Trauma 1997; 42: 1152-1156
166. Simmers TA, Bekkenk MW, Vidakovic-Vukic M. Internal jugular vein thrombosis after cervical traction. J Intern Med 1997; 241 : 333-335
167. Ter Haar G. Safety of diagnostic ultrasound [commentary]. Br J Radiol 1996; 69: 1083-1085
168. Norheim AJ, Fonnebo V. Adverse effects of acupuncture [letter]. Lancet 1995; 345: 1576
169. Rochel J. Steroid-induced arachnoiditis. Med J Aust 1984; 140, 281-284
170. Chen RT, De Stefano F. Vaccine adverse events: Causal or coincidental? Lancet 1998; 351: 611-612
171. Brown MA, Bertouch JV. Rheumatic complications of influenza vaccination. Aust NZ Med J 1994; 24: 572-573
172. Duclos P, Bentsi-Enchill A. Risks and benefits of immunisation. Current Thoughts. Curr Ther 1994; April: 17-28
173. Knipschild P. Viewpoint: Searching for alternatives: Loser pays. Lancet 1993;
341: 135-137
174. Smith R. Where is the wisdom...? The poverty of medical evidence. Br Med J 1991; 303: 798-799
175. Leeder SR. Health for all by the year 2000: Educational, empirical and ethical responsibilities for the medical profession. Med J Aust 1985; 142: 551-555
176. Moore TJ, Psaty BM, Furberg CD. Time to act on drug safety. JAMA 1998; 279: 1571-1573
177. Turner JA, Ersek M, Herron L, Haselkorn J, Kent J, Ciol MA, et al. Patient outcomes after lumbar spinal fusions. JAMA 1992; 268: 907-911
178. International classification of diseases. Manual of the international statistical classification of diseases, injuries and causes of death. 9th rev 1975. Vol. 2 Alphabetical index. Geneva: World Health Organisation, 1978
179. Rankin JM, Silbert PL, Ydava OP, Hankey GJ, Stewart-Wynne EG. Mechanisms of stroke complicating cardiopulmonary bypass surgery. Aust NZ J Med 1994; 24: 154-160
180. Rollins A. Health messages being heeded. Australian snapshot: Richer, healthier, cleverer. The Age, Melbourne 1998; June 4: 8,9 (citing Australian Bureau of Statistics 1996 survey of social trends)
181. Tettenborn G, Caplan LR, Sloan MA, Estol CJ, Pessin MS, DeWitt LD, et at. Post-operative brainstem and cerebellar infarcts. Neurology 1993; 43: 471-477 (citing Shaw)
182. Nachemson A. Low back pain. Are orthopedic surgeons missing the boat? Acta Orthop Scand 1993; 64 (1): 1-2
183. Haldeman S. Chiropractic complications [letter]. Neurol 1996; 46: 885
184. Ingliss BD, Fraser B, Penfold BR. Chiropractic in New Zealand. Report of the Commission of Inquiry. Wellington: Government Printer, 1979: 3
185. Anon. Readers Q & A. Aust Med 1998; Oct5: 18
186. Maclennan AH, Wilson DH, Taylor AW. Prevalence and cost of alternative medicine in Australia. Lancet 1996; 347: 569-573
187. Wilke C. Team: The key to success. Today's Chiropr 1998; 27 (4): 12-14
188. Rondberg TA. Under the influence of modern medicine. Chandler, AZ: The Chiropractic Journal, 1998
189. Reynolds F. Dural puncture and headache. Br Med J 1993; 306: 874-875
190. Brewer GE, Hogan-Casey P. Rotational head movements and their relationship to stroke: The role of the chiropractic physician. Chiropr Tech 1990; 2: 188-190
191. Johnson DW, Whiting G, Pender MP. Cervical self manipulation and stroke. Med J Aust 1993;
158: 290
192. The Chiropractors Registration Act of Victoria 1996
193. van den Heuvel S. ACT moves for chiropractors. Canberra Times 1973; July 11
194. O'Neill A. Danger and safety in medicines. Soc Sci Med 1994; 34: 497-507
195. Carter M. Review of registration for health practitioners. Health Department of Victoria 1987; i, ii, 58
196. Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. Scientific monograph of the Quebec task force on whiplash associated disorders: Redefining 'whiplash' and its management. Spine 1995; 20 (8S): S1-73
197. Bigos S, Bowyer 0, Braen G, Brown K, Deyo R, Haldeman S, et al., editors. Acute low back problems in adults. Clinical practice guideline No. 14. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, U.S. Department of Health and Human Services, 1994: AHCPR publication No (PHS) 95-0642
198. Manga P, Angus D, Papdopoulos C, Swan W, editors. The effectiveness and cost-effectiveness of chiropractic management of low-back pain. A report to the Ministry of Health, Government of Ontario, Canada, 1993
199. Aker PD, Gross AR, Peloso P. Conservative management of mechanical neck pain: A systematic overview and meta-analysis. Br Med J 1996; 313: 1291-1296