Cv ii patho pharm fall 11
246
Disorders of Cardiac Disorders of Cardiac Function Function NURS 315/501 NURS 315/501 Kathryn T. Von Rueden RN, Kathryn T. Von Rueden RN, MS, FCCM MS, FCCM University of Maryland University of Maryland School of Nursing School of Nursing 1
-
Upload
dceppos -
Category
Health & Medicine
-
view
1.804 -
download
1
Transcript of Cv ii patho pharm fall 11

Disorders of Cardiac FunctionDisorders of Cardiac FunctionNURS 315/501NURS 315/501
Kathryn T. Von Rueden RN, MS, FCCMKathryn T. Von Rueden RN, MS, FCCM
University of MarylandUniversity of Maryland
School of NursingSchool of Nursing
1

2

Global Tissue OxygenationGlobal Tissue OxygenationMade Ridiculously SimpleMade Ridiculously Simple
SvO2 = 75%
25%
Venous Oxygen Delivery
ArterialOxygenDelivery
Oxygen Consumption
100%
3

Coronary Coronary CirculationCirculation
4

Cardiac Conduction SystemCardiac Conduction System
Conduction system stimulates the Conduction system stimulates the myocardium to contract & pump bloodmyocardium to contract & pump blood
Conduction system usually controls the Conduction system usually controls the rhythm of the heart.rhythm of the heart.
Heart has two conduction systemsHeart has two conduction systems One controls atrial activity One controls atrial activity One that controls ventricular activityOne that controls ventricular activity
5

Anatomy of the Conduction Anatomy of the Conduction SystemSystem
SA NodeSA Node
AV NodeAV Node
Bundle of HisBundle of His
Bundle branchesBundle branches
Purkinje fibersPurkinje fibers
Porth, 2007, Essentials of Pathophysiology, 2nd ed., Lippincott, p. 331.6

SA NodeSA Node
Pacemaker of the Pacemaker of the heartheart
Impulses originate Impulses originate herehere
Located in Located in posterior wall RAposterior wall RA
Fires at 60 -100 Fires at 60 -100 bpmbpm
7

AV NodeAV Node Connects the atria & Connects the atria &
ventricles, provides ventricles, provides one way conductionone way conduction Would beat Would beat
independentlyindependently Fires at 40 -60 bpmFires at 40 -60 bpm Can assume Can assume
pacemaker function pacemaker function if SA fails to if SA fails to dischargedischarge
8

Purkinjie FibersPurkinjie Fibers Supplies the ventriclesSupplies the ventricles Large fibers, rapid Large fibers, rapid
conduction for swift & conduction for swift & efficient ejection of efficient ejection of blood from heartblood from heart
Fire 15-40 bpmFire 15-40 bpm Assume pacemaker of Assume pacemaker of
ventricles if AV failsventricles if AV fails HR reflects intrinsic HR reflects intrinsic
firing of these structuresfiring of these structures
9

Action Potentials (AP)Action Potentials (AP)Stimulus Stimulus
excitable tissues (muscle & conduction system) excitable tissues (muscle & conduction system)
evokes an AP characterized by a sudden change evokes an AP characterized by a sudden change in voltage resulting from transient depolarization in voltage resulting from transient depolarization & then repolarization.& then repolarization.
AP’s are electrical currents involving the AP’s are electrical currents involving the movement/flow of electrically charged ions at movement/flow of electrically charged ions at level of cell membrane.level of cell membrane.
AP’s are conducted thru-out the heart, responsible AP’s are conducted thru-out the heart, responsible for initiating each cardiac contraction.for initiating each cardiac contraction.
10

SLOW SA & AV Nodes
FAST
Purkinje Fiber & Muscle
11

Cardiac Action PotentialsCardiac Action Potentials 3 types of membrane ion channels that contribute to 3 types of membrane ion channels that contribute to
voltage changes during the phases of the APvoltage changes during the phases of the AP
1.1. Fast NaFast Na++ channels channels Rapid depolarization of musclesRapid depolarization of muscles
2.2. Slow NaSlow Na++ channels channels Pacemaker activity (SA, AV)Pacemaker activity (SA, AV)
3.3. Potassium channelsPotassium channels Speedy repolarizationSpeedy repolarization
12

Three Phases of APThree Phases of AP RestingResting
Membrane is relatively Membrane is relatively permeable to Kpermeable to K++, but much , but much less so to Naless so to Na++
DepolarizationDepolarizationCell membrane becomes Cell membrane becomes
permeable to Napermeable to Na++ NaNa++ enters cell, enters cell, IC more +IC more +
RepolarizationRepolarizationOutward flow of positive Outward flow of positive
charges, mainly Kcharges, mainly K++ IC is more negativeIC is more negative Assisted by NaAssisted by Na++-K-K++ pump pump
13

Cardiac Muscle Cell FiringCardiac Muscle Cell Firing
Cells begin with a Cells begin with a negative charge: negative charge: resting membrane resting membrane potentialpotential
Calcium leakCalcium leak lets lets CaCa2+2+ diffuse in, diffuse in, making the cell more making the cell more positivepositive
Threshold potential
Resting membrane potential Calcium
leak
14

Cardiac Muscle Cell Firing (cont.)Cardiac Muscle Cell Firing (cont.) At threshold At threshold
potential, more Napotential, more Na++ channels openchannels open
NaNa++ rushes in, rushes in, making the cell making the cell very positive: very positive: depolarizationdepolarization
Action potential: Action potential: the cell responds the cell responds (e.g. by (e.g. by contracting)contracting)
Threshold potential
Resting membrane potential
Action potential
Calcium leak
15

Cardiac Muscle Cell Firing (cont.)Cardiac Muscle Cell Firing (cont.)
KK++ channels open channels open KK++ diffuses out, diffuses out,
making the cell making the cell negative again, negative again, but Cabut Ca2+2+ channels channels are still allowing are still allowing CaCa2+2+ to enter to enter
The cell remains The cell remains positive: positive: plateauplateau
Threshold potential
PLATEAU
Action potential
Calcium leak
16

Cardiac Muscle Cell Firing (cont.)Cardiac Muscle Cell Firing (cont.) During During
plateauplateau, the , the musclemuscle contracts contracts stronglystrongly
Then the CaThen the Ca2+2+ channels shut channels shut and it and it repolarizesrepolarizes
Threshold potential
PLATEAUAction potential
Calcium leak
17

Cardiac Action PotentialsCardiac Action Potentials Unlike nerve cells, cardiac cells have five phases in Unlike nerve cells, cardiac cells have five phases in
their action potentialtheir action potential Phase 4 – the resting membrane potential.Phase 4 – the resting membrane potential. Phase 0 – there is rapid depolarizationPhase 0 – there is rapid depolarization Phase 1 – there is a short repolarization (only Phase 1 – there is a short repolarization (only
observed in ventricular muscle)observed in ventricular muscle) Phase 2 – the membrane potential remains Phase 2 – the membrane potential remains
depolarized in a plateaudepolarized in a plateau Phase 3 – the membrane potential becomes Phase 3 – the membrane potential becomes
repolarized.repolarized. The characteristics of the phases are different in nodal The characteristics of the phases are different in nodal
tissues of the heart when compared with heart muscle tissues of the heart when compared with heart muscle cells or Purkinje fibers.cells or Purkinje fibers.
18

Cardiac Muscle Action PotentialCardiac Muscle Action Potential 5 Phases5 Phases
Phase 0Phase 0: : Upstroke, rapid depolarizationUpstroke, rapid depolarization
Phase 1:Phase 1: Early, short repolarizationEarly, short repolarization
Seen only in ventricular musSeen only in ventricular musclecle
Phase 2:Phase 2: Plateau phase; membrane potential Plateau phase; membrane potential
remains depolarizedremains depolarized
Phase 3:Phase 3: Final rapid repolarizationFinal rapid repolarization
Phase 4:Phase 4: Resting, Resting, diastolic repolarizationdiastolic repolarization
** Unlike nerve cells, cardiac cells ** Unlike nerve cells, cardiac cells have 5 phases in their action have 5 phases in their action
potential.potential.
19

Cardiac Muscle Cell ContractionCardiac Muscle Cell Contraction During Phase 2, the plateau, calcium ion enters the During Phase 2, the plateau, calcium ion enters the
muscle cell, causing it to contract strongly.muscle cell, causing it to contract strongly.
The strength of contraction is directly proportional to The strength of contraction is directly proportional to the number of calcium ions that enter the cell.the number of calcium ions that enter the cell.
Calcium channel opening is controlled by voltage and Calcium channel opening is controlled by voltage and by betaby beta11 receptors in the ventricular myocardium. receptors in the ventricular myocardium.
20

Lehne 5th ed Figure 47-2
Myocardium& His-Purkinje
System
SA Node &AV Node
Why are action Why are action potentials potentials important?important?
• Source of Source of dysrhythmiasdysrhythmias
• Targets of Targets of drug actiondrug action
21

Cardiac Conduction Cardiac Conduction & &
Rhythm DisordersRhythm Disorders
22

ECG: Relationship ECG: Relationship to Action Potentialto Action Potential
Electrical events recorded Electrical events recorded on ECGon ECG
Electrical events precede Electrical events precede mechanical events; mechanical events; know know what they represent!what they represent! PP QRSQRS TT
23

Lehne 5th ed Figure 47-3
Electrical event precedes mechanical event !!!
24

Porth 2007, Figure 16-12
P waveP wave
PR IntervalPR Interval
QRS complexQRS complex
T wave: T wave: RepolarizationRepolarization
25

Disorders of Cardiac Rhythm Disorders of Cardiac Rhythm and Conduction : 2 Typesand Conduction : 2 Types
1.1. Dysrhythmias (or arrhythmias)Dysrhythmias (or arrhythmias)
Term used to describe disorders of cardiac Term used to describe disorders of cardiac rhythmrhythm
Occur in healthy and non-healthyOccur in healthy and non-healthy Interfere with heart’s pumping abilityInterfere with heart’s pumping ability
2.2. Disorders of impulse conductionDisorders of impulse conduction
26

Disorders of Cardiac Rhythm Disorders of Cardiac Rhythm and Conductionand Conduction
2 types of disorders of the cardiac conduction system2 types of disorders of the cardiac conduction system1. Disorders of rhythm1. Disorders of rhythm2. Disorders of impulse conduction2. Disorders of impulse conduction
Dysrhythmias (or arrhythmias)Dysrhythmias (or arrhythmias) Term used to describe disorders of cardiac rhythmTerm used to describe disorders of cardiac rhythm Occur in healthy and non-healthyOccur in healthy and non-healthy Interfere with heart’s pumping abilityInterfere with heart’s pumping ability
27

CausesCauses
Congenital defects in conduction systemCongenital defects in conduction system Degenerative changesDegenerative changes Ischemia and MIIschemia and MI Fluid/electrolyte imbalancesFluid/electrolyte imbalances DrugsDrugs
28

Sinus Node RhythmsSinus Node RhythmsNormal Sinus RhythmNormal Sinus Rhythm
P wave precedes each QRS, RR intervals P wave precedes each QRS, RR intervals reg, rate 60-100reg, rate 60-100
Sinus BradycardiaSinus BradycardiaP before QRS, RR regular, rate P before QRS, RR regular, rate < 60, slowing of conduction thru AV < 60, slowing of conduction thru AV node (Vagal, PNS)node (Vagal, PNS)
Sinus TachycardiaSinus TachycardiaP before QRS, RR regular, P before QRS, RR regular, rate > 100. Enhancedrate > 100. Enhancedautomaticity r/t SNS activation (fever, automaticity r/t SNS activation (fever, exercise, stress)exercise, stress)
29

Lehne 5th ed Figure 47-2
Myocardium& His-Purkinje
System
SA Node &AV Node
30
Class II Antidysrhythmic

Class II Antidysrhythmic Class II Antidysrhythmic Beta BlockersBeta BlockersDepress Phase 4 in depolarizationDepress Phase 4 in depolarizationNonselective: Nonselective: Carvedilol, Propranolol: Carvedilol, Propranolol:
Block beta 1 & 2 receptorsBlock beta 1 & 2 receptorsCardioselective: Cardioselective: Metropolol, Esmolol:Metropolol, Esmolol:
Block beta 1 onlyBlock beta 1 only
Mechanism of Action:Mechanism of Action:(-) Inotrope(-) Inotrope(-) Chronotrope – SLOW the heart rate!(-) Chronotrope – SLOW the heart rate!(-) Dromotrope(-) Dromotrope
31

Class II Antidysrhythmic Class II Antidysrhythmic Beta BlockersBeta Blockers
ECGECG Prolong PR & bradycardiaProlong PR & bradycardia
Pharmacotherapeutics:Pharmacotherapeutics:PSVTPSVTAnginaAnginaAMIAMIHypertension (HTN) (Hypertension (HTN) (not esmolol)not esmolol)Heart Failure (HF) Heart Failure (HF) (carvedilol, metoprolol)(carvedilol, metoprolol)
See Lehne Table 18-2 & 18-332

Beta Blocker: Adverse effectsBeta Blocker: Adverse effects
HypotensionHypotension SyncopeSyncope Precipitate HFPrecipitate HF BradycardiaBradycardia AV blockAV block Sinus arrestSinus arrest Bronchospasm Bronchospasm (non-selective beta blockers)(non-selective beta blockers) Rebound cardiac excitation Rebound cardiac excitation (if abruptly stopped)(if abruptly stopped)
33

Beta Blocker Administration Beta Blocker Administration (remember from last week)(remember from last week)
DrugDrug RouteRoute ½ Life (hrs)½ Life (hrs) IndicationIndication
EsmololEsmolol IV ONLY!IV ONLY! 0.150.15 Dysrh, anginaDysrh, angina
MetoprololMetoprolol IV, POIV, PO 3-73-7 Dysrh, angina, Dysrh, angina, AMI, HF, HTNAMI, HF, HTN
AtenololAtenolol IV, POIV, PO 6-96-9 Dysrh, angina, Dysrh, angina, AMIAMI
CarvedilolCarvedilol POPO 5-115-11 Angina, AMI, Angina, AMI, HF, HTNHF, HTN
PropanololPropanolol IV, POIV, PO 3-53-5 Dysrh, angina, Dysrh, angina, AMI, HTNAMI, HTN
34

Atrial Dysrhythmias
Atrial FibrillationAtrial Fibrillation: : Chaotic & disorganized current.Chaotic & disorganized current.Atria are depolarizing without contracting (just quivering).Atria are depolarizing without contracting (just quivering).Ventricular rhythm irregular. Ventricular rhythm irregular.
Only irregularly irregular rhythm.Only irregularly irregular rhythm.No discernable P waves.No discernable P waves.
35

A-Fib treatment: DigoxinA-Fib treatment: Digoxin
A cardiac glycoside that is used for atrial A cardiac glycoside that is used for atrial fibrillation or atrial flutter.fibrillation or atrial flutter.
Slows conduction in the AV node and Slows conduction in the AV node and thereby slows ventricular rate.thereby slows ventricular rate.
36

DigoxinDigoxinMechanism of Action:Mechanism of Action: Inhibits NaInhibits Na++-K-K++ ATPase; more intracellular calcium ATPase; more intracellular calcium
availableavailable + inotrope+ inotrope
Enhance vagal influence Enhance vagal influence (SA & AV node effect)(SA & AV node effect)
- chronotrope, - dromotrope - chronotrope, - dromotrope
Pharmacotherapeutics:Pharmacotherapeutics: Heart failureHeart failure Atrial flutterAtrial flutter
37

Lehne 6th ed Figure 47-438

Digoxin: Digoxin: PharmacokineticsPharmacokinetics
AbsorptionAbsorption 60 – 80% (tabs)60 – 80% (tabs)
70 – 85% (elixir)70 – 85% (elixir)
90 – 100% (caps)90 – 100% (caps)
MetabolismMetabolism LiverLiver
Half LifeHalf Life 5-7 DAYS to eliminate 5-7 DAYS to eliminate
& T½ 1.5 days & T½ 1.5 days
39

DigoxinDigoxinAdministration ConsiderationsAdministration Considerations PO or IV (mcg NOT mg)PO or IV (mcg NOT mg)
““Digitalization”Digitalization” IV loading doseIV loading dose
Digoxin levels (0.5 - 1.1 ng/ml)Digoxin levels (0.5 - 1.1 ng/ml) VERY narrow therapeutic rangeVERY narrow therapeutic range Digoxin immune FAB (antidote) for Digoxin immune FAB (antidote) for
toxic levels ( > 2.0 ng/ml)toxic levels ( > 2.0 ng/ml) D/C drug until toxicity resolvesD/C drug until toxicity resolves
40

Adverse effect & S/S digoxin toxicityAdverse effect & S/S digoxin toxicity
Digoxin induced dysrhythmiasDigoxin induced dysrhythmiasAll types! All types! BradycardiaBradycardiaAV block most commonAV block most commonVentricular flutter/fib most dangerousVentricular flutter/fib most dangerous
GI : Anorexia, N/V GI : Anorexia, N/V CNS: Drowsiness/weakness,CNS: Drowsiness/weakness,
Blurred vision/colored (yellow) halosBlurred vision/colored (yellow) halos
41

42

DigoxinDigoxinContraindications & PrecautionsContraindications & Precautions
ContraindicationsContraindications PrecautionsPrecautions
22ndnd/3/3rdrd degreedegree heart block heart block
V. Fib/V. TachV. Fib/V. Tach
Sick Sinus SyndromeSick Sinus Syndrome
Acute MIAcute MI
Renal insufficiencyRenal insufficiency
HypokalemiaHypokalemia
Severe pulmonary Severe pulmonary diseasedisease
43

DigoxinDigoxinAdditional ConsiderationsAdditional Considerations
Potassium levels Potassium levels
Keep in 3.5 – 5.0 mEq/L rangeKeep in 3.5 – 5.0 mEq/L range Digoxin competes with KDigoxin competes with K++ @ binding sites @ binding sites Hyperkalemia Hyperkalemia decreases digoxin effect decreases digoxin effect Diuretics may cause hypokalemia Diuretics may cause hypokalemia
digoxin toxicitydigoxin toxicity
44

DrugDrugDrug InteractionsDrug InteractionsReduce digoxin therapeutic effectReduce digoxin therapeutic effect ACE-I & ARBsACE-I & ARBs
Increase potassiumIncrease potassium
Additive digoxin effectAdditive digoxin effect SympathomimeticsSympathomimetics
Increase contractility & HRIncrease contractility & HR Increase risk of tachydysrhythmiasIncrease risk of tachydysrhythmias
Numerous interactions (Lehne Table 47-2)Numerous interactions (Lehne Table 47-2)
45

DrugDrugDrug InteractionsDrug InteractionsIncrease risk of digoxin toxicityIncrease risk of digoxin toxicity
Calcium channel blockers (verapamil)Calcium channel blockers (verapamil) Increase serum dig levelIncrease serum dig level Decrease HRDecrease HR Bradydysrhythmias or complete heart blockBradydysrhythmias or complete heart block
Diuretics may reduce potassium levelsDiuretics may reduce potassium levels Increase risk of dig-induced dysrhythmiasIncrease risk of dig-induced dysrhythmias
Herbal interactions increase metabolismHerbal interactions increase metabolism
46

Digoxin: Digoxin: Nursing ImplicationsNursing Implications
Apical pulse for 1 min. & document
Monitor ECG
Monitor potassium & dig levels
47

A-Fib, PSVT TreatmentA-Fib, PSVT TreatmentClass IV Antidysrhythmic Class IV Antidysrhythmic Calcium Channel BlockersCalcium Channel Blockers
Verapamil, diltazemVerapamil, diltazem Mechanism of Action:Mechanism of Action:
Inhibits calcium influx during Inhibits calcium influx during depolarizationdepolarization
Depresses phase 4 of depolarizationDepresses phase 4 of depolarization Prolongs phases 1 & 2 of Prolongs phases 1 & 2 of
depolarizationdepolarization
48

Lehne 5th ed Figure 47-2
Myocardium& His-Purkinje
System
SA Node &AV Node
49

Class IV Antidysrhythmic Class IV Antidysrhythmic Calcium Channel Blockers (verapamil, diltiazem)Calcium Channel Blockers (verapamil, diltiazem)
3 effects on heart3 effects on heart
1.1. Slow SA node automaticity Slow SA node automaticity slow HR slow HR
2.2. Delay AV node conduction Delay AV node conduction prolong PR prolong PR
3.3. myocardial contractility myocardial contractility CO CO
Note: same effects as Beta Blockers!!!!!Note: same effects as Beta Blockers!!!!!
PharmacotherapeuticsPharmacotherapeutics::
PSVTPSVT Atrial Fib/FlutterAtrial Fib/Flutter (slow ventricular (slow ventricular rate)rate)
Angina Angina HypertensionHypertension
Note: not effective for ventricular dysrhythmias !!Note: not effective for ventricular dysrhythmias !!50

Verapamil & DiltiazemVerapamil & DiltiazemAdverse Effects (Adverse Effects (Remember from last week)Remember from last week)
Cardiac:Cardiac:• BradycardiaBradycardia• AV blockAV block• Decreased Decreased myocardial myocardial contractility contractility decreased decreased cardiac outputcardiac output
General:General:• DizzinessDizziness• Facial FlushingFacial Flushing• HeadacheHeadache• Peripheral edemaPeripheral edema• Decreased Decreased GI motilityGI motility
51

Disorders of Atrioventricular Conduction
1st degree AV block:1st degree AV block: Slightly Slightly prolonged PR interval; prolonged PR interval; ALLALL atrial impulses atrial impulses
are conducted to ventricles; asymptomatic. are conducted to ventricles; asymptomatic.
2nd degree AV block:2nd degree AV block: Not all atrial Not all atrial impulses are conducted to ventricles, see impulses are conducted to ventricles, see some P waves, not followed by QRS. some P waves, not followed by QRS.
Can be very symptomatic. Can be very symptomatic.
3rd degree AV block =3rd degree AV block =complete AV block:complete AV block:Conduction link between atria & ventricles Conduction link between atria & ventricles lost, each controlled by independent lost, each controlled by independent pacemakers. Atria continue at their rate, pacemakers. Atria continue at their rate, ventricles contract at their rate (30-40 bpm). ventricles contract at their rate (30-40 bpm).
52

Case study: Digoxin toxicityCase study: Digoxin toxicitySerum dig level = 1.7 ng.ml Serum dig level = 1.7 ng.ml (0.5-1.1 desired)(0.5-1.1 desired)
33rdrd degree AV degree AV BlockBlock
Temporary pacemaker inserted, SR Temporary pacemaker inserted, SR 100% 100% pacedpaced
53

Complete A-V block with 100% Complete A-V block with 100% atrio-ventricular pacingatrio-ventricular pacing
54
Atrial Pacingspike
Ventricular Pacingspike
P QRS

Ventricular Dysrhythmias: More Serious!PVC:PVC: Ventricles contract prematurely. Ventricles contract prematurely. W/ a PVC, diastolic volume is insufficient for ejection of W/ a PVC, diastolic volume is insufficient for ejection of blood into arterial system. blood into arterial system. Therefore, no or weak pulse palpated. Therefore, no or weak pulse palpated. Few/day = OK, More/minute, the worse (>6). Few/day = OK, More/minute, the worse (>6). Common post MI, SNS activity, Common post MI, SNS activity, K+, hypoxia. K+, hypoxia.
V-Tachycardia: V-Tachycardia: rhythm originates below Bundle rhythm originates below Bundle of His, in ventricular muscle. Wide, tall QRS complexes. of His, in ventricular muscle. Wide, tall QRS complexes. Stops spontaneously or continue. Stops spontaneously or continue. Dangerous rhythm,Dangerous rhythm, diastolic diastolicfilling time filling time CO. Can cause CO. Can cause Cardiac ArrestCardiac Arrest
V-Fib: V-Fib: ventricle quivers but does ventricle quivers but does NOT contract! NOT contract! NO cardiac outputNO cardiac output,,and no pulses; and no pulses; Cardiac Arrest!!Cardiac Arrest!!grossly disorganized pattern.grossly disorganized pattern.
55

Lehne 5th ed Figure 47-2
Myocardium& His-Purkinje
System
SA Node &AV Node
56
Class I Antidysrhythmic

Class 1B: LidocaineClass 1B: Lidocaine Ventricular Dysrhthmias Ventricular Dysrhthmias
57

Class 1B: LidocaineClass 1B: Lidocaine
Effect on Heart & ECGEffect on Heart & ECG1.1. Blocks Na+ channelsBlocks Na+ channels slow conduction slow conduction
thru atria, ventricles, HIS-Purkinjethru atria, ventricles, HIS-Purkinje
2.2. Reduces automaticityReduces automaticity
3.3. Accelerates repolarization (shortens Accelerates repolarization (shortens action potential)action potential)
No anticholinergic effectNo anticholinergic effect No change in ECGNo change in ECG
58

Lidocaine: Precautions & Lidocaine: Precautions & Adverse EffectsAdverse Effects
Metabolized by LiverMetabolized by Liver Therapeutic range 1.5 – 5.0 microgm/mlTherapeutic range 1.5 – 5.0 microgm/ml Adverse CNS Effects: Adverse CNS Effects:
Drowsiness, confusion, paresthesiaDrowsiness, confusion, paresthesia Toxicity:Toxicity:
Convulsions & respiratory arrestConvulsions & respiratory arrest
59

Lidocaine: AdministrationLidocaine: Administration IV PushIV Push
50-100mg (1mg/kg)50-100mg (1mg/kg) InfusionInfusion
1-4mg/min1-4mg/minDiluted in D5WDiluted in D5W
Special Considerations: Special Considerations: Use for as short a time as possibleUse for as short a time as possibleReduce dosage in pts with liver disordersReduce dosage in pts with liver disorders
60

Class III AntidysrhythmicClass III Antidysrhythmic Potassium Channel Blockers:Potassium Channel Blockers: AmiodaroneAmiodarone ApprovedApproved for VT & VF for VT & VF Delay repolarizationDelay repolarization
Prolongs action potential & refractory periodProlongs action potential & refractory period
Increases PR & QT intervalsIncreases PR & QT intervals
Initial Initial catecholamine release catecholamine release brief exacerbation brief exacerbation of dysrhythmias of dysrhythmias
block catecholamine release block catecholamine release vasodilation / vasodilation / hypotensionhypotension
61

Lehne 5th ed Figure 47-2
Myocardium& His-Purkinje
System
SA Node &AV Node
62
Class III Antidysrhythmic

Non-Pharmacologic Non-Pharmacologic Treatment of DysrhythmiasTreatment of Dysrhythmias
CardioversionCardioversion Atrial fibAtrial fib V-tachV-tach
DefibrillationDefibrillation V-fibV-fib
63

Automated External DefibrillatorAutomated External Defibrillator Cardiac Arrest, AED “interrogates” rhythm.Cardiac Arrest, AED “interrogates” rhythm. Tells user what to do, eg “Shock Now”Tells user what to do, eg “Shock Now” Delivers shock for V-tach or V-fib.Delivers shock for V-tach or V-fib.
64

Non-Pharmacologic Non-Pharmacologic Treatment of DysrhythmiasTreatment of Dysrhythmias
Implantable Cardioverter/DefibrillatorImplantable Cardioverter/Defibrillator Like a pacemakerLike a pacemaker Monitors & analyzes rhythmMonitors & analyzes rhythm Delivers shock to terminate V-tach, V-fibDelivers shock to terminate V-tach, V-fib
Radiofrequency Catheter AblationRadiofrequency Catheter Ablation Cardiac cath & electrophysiologic testCardiac cath & electrophysiologic test Identify cardiac tissue site which causes Identify cardiac tissue site which causes
dysrhythmiadysrhythmia RF energy delivered to destroy the tissue RF energy delivered to destroy the tissue
(remember, you can’t pace meatloaf)(remember, you can’t pace meatloaf)
65

Antidysrhythmic Drugs: SummaryAntidysrhythmic Drugs: Summary
Class IClass I Depress phase 0 in depolarizationDepress phase 0 in depolarizationBlock sodium channelsBlock sodium channels
Class IIClass IIDepress phase 4 in depolarizationDepress phase 4 in depolarizationBlock beta 1 & 2 adrenergic receptorsBlock beta 1 & 2 adrenergic receptors
HRHR Contractility Contractility
66

Class IIIClass IIIProlong phase 3 (repolarization)Prolong phase 3 (repolarization)
Class IVClass IVDepresses phase 4 depolarizationDepresses phase 4 depolarizationProlongs phases 1 & 2 repolarizationProlongs phases 1 & 2 repolarization
Antidysrhythmic Drugs: SummaryAntidysrhythmic Drugs: Summary
67

Management of Management of Cardiac DysrhythmiasCardiac Dysrhythmias
REMEMBER:REMEMBER:Many drugs used to treat dysrhythmias Many drugs used to treat dysrhythmias
also may worsen them also may worsen them or cause new ones!or cause new ones!
68

Coronary Heart Disease Coronary Heart Disease & &
Acute Myocardial InfarctionAcute Myocardial Infarction(MI or AMI)(MI or AMI)
69

Coronary CirculationCoronary Circulation Two main coronary Two main coronary
arteries arise from arteries arise from coronary sinus (above coronary sinus (above aortic valve)aortic valve)
Primary factor Primary factor responsible for perfusion responsible for perfusion coronary arteries is BP coronary arteries is BP in aortain aorta
s aortic pressure -> s aortic pressure -> s coronary blood flow s coronary blood flow
70

LVLV
Coronary CirculationCoronary Circulation
71

72

Ischemic Heart DiseaseIschemic Heart Disease
a.k.a Coronary Heart Disease a.k.a Coronary Heart Disease a.k.a Coronary Artery Diseasea.k.a Coronary Artery Disease
AnginaAnginaMyocardial InfarctionMyocardial Infarction
73

Coronary Heart DiseaseCoronary Heart Disease
Heart disease caused by impaired coronary blood Heart disease caused by impaired coronary blood flow (atherosclerosis)flow (atherosclerosis)
Cause angina, dysrhythmias, conduction defects, Cause angina, dysrhythmias, conduction defects, heart failure, sudden death, myocardial infarction heart failure, sudden death, myocardial infarction (“heart attack”)(“heart attack”)
If blood flow is temporarily inadequate (due to If blood flow is temporarily inadequate (due to increased oxygen demand), ischemia produces increased oxygen demand), ischemia produces pain (angina).pain (angina).
Myocardial Infarction is myocardial cell/tissue Myocardial Infarction is myocardial cell/tissue death due to oxygen starvationdeath due to oxygen starvation
74

Assessment of Coronary Assessment of Coronary Blood FlowBlood Flow ECGECG Exercise Stress TestingExercise Stress Testing Pharmacologic Stress TestingPharmacologic Stress Testing Nuclear ImagingNuclear Imaging Cardiac Catheterization /Coronary Cardiac Catheterization /Coronary
angiographyangiography
75

Collateral CirculationCollateral Circulation
With gradual occlusion of large coronary With gradual occlusion of large coronary vessels, the smaller collateral vessels vessels, the smaller collateral vessels in size in size and provide alternative channels for blood and provide alternative channels for blood flowflow
One of the reasons CHD does not produce One of the reasons CHD does not produce symptoms until it is far advanced is that the symptoms until it is far advanced is that the collateral channels develop at the same time collateral channels develop at the same time the atherosclerotic changes are occurring.the atherosclerotic changes are occurring.
76

77
Collateral Circulation
77

Pathogenesis of CAD: Pathogenesis of CAD: AtherosclerosisAtherosclerosis Most common cause of CADMost common cause of CAD Plaque disruption is most frequent Plaque disruption is most frequent
cause of MI, sudden deathcause of MI, sudden death Can affect one or all 3 major coronary Can affect one or all 3 major coronary
arteries/branchesarteries/branches
78

PlaquePlaque Plaques typically do not occlude the whole Plaques typically do not occlude the whole
coronary artery but produce a narrowing that coronary artery but produce a narrowing that restricts blood flow.restricts blood flow. In times of increased oxygen demand, such as with In times of increased oxygen demand, such as with
exercise, the restricted blood flow may produce exercise, the restricted blood flow may produce ischemia in cells supplied by that artery.ischemia in cells supplied by that artery.
This produces the pain of angina.This produces the pain of angina. A plaque may become unstable and rupture, A plaque may become unstable and rupture,
causing a clot to form which may completely causing a clot to form which may completely occlude the artery.occlude the artery. Occlusion of the artery causes death of the cardiac Occlusion of the artery causes death of the cardiac
cells downstream that are supplied by that artery.cells downstream that are supplied by that artery. When the cells die, that is an infarction – hence the When the cells die, that is an infarction – hence the
name name myocardial infarction.myocardial infarction.79

Atherosclerosis in Coronary ArteryAtherosclerosis in Coronary ArteryPlaque rupture & disruption of atheromaPlaque rupture & disruption of atheroma lipid core/contents exposed to bloodlipid core/contents exposed to blood
platelet aggregationplatelet aggregationcoagulation cascade coagulation cascade
fibrin clotfibrin clot
thrombosis, vasospasm thrombosis, vasospasm
myocardial ischemiamyocardial ischemia Coronary arteries unable to supply blood to Coronary arteries unable to supply blood to
meet metabolic demands of the heartmeet metabolic demands of the heart
80

Review of Terms Related to CHDReview of Terms Related to CHD Angina:Angina: symptomatic paroxysmal chest pain or symptomatic paroxysmal chest pain or
pressure sensation associated with transient pressure sensation associated with transient myocardial ischemiamyocardial ischemia
Stable angina:Stable angina: Occurs with exertion or stress Occurs with exertion or stress Variant or vasospastic angina:Variant or vasospastic angina: Occurs during rest or Occurs during rest or
with minimal activity (nocturnal, Prinzmetal’s)with minimal activity (nocturnal, Prinzmetal’s) Silent myocardial ischemiaSilent myocardial ischemia: Occurs in the absence of : Occurs in the absence of
anginal painanginal pain Unstable anginaUnstable angina: Symptoms at rest lasting >20 mins., : Symptoms at rest lasting >20 mins.,
marked limitations of ordinary activity (walking 1–2 marked limitations of ordinary activity (walking 1–2 blocks, climbing a flight of stairs), recent acceleration in blocks, climbing a flight of stairs), recent acceleration in anginal signsanginal signs
AMI:AMI: Acute myocardial infarction (STEMI or NSTEMI) Acute myocardial infarction (STEMI or NSTEMI) 81

82

83

84

85

Plaque RupturePlaque Rupture SpontaneousSpontaneous
SNS activation SNS activation BP, BP, HR, HR, contraction contraction Triggering event (stress: emotional, physical)Triggering event (stress: emotional, physical)
DiurnalDiurnal First hour of arisingFirst hour of arising SNS “surge” on arisingSNS “surge” on arising
SNS major playerSNS major player Beta-adrenergic blockersBeta-adrenergic blockers
86

““Severe” coronary stenosis and vulnerable Severe” coronary stenosis and vulnerable plaques co-existplaques co-exist
Califf, Atlas of Heart Diseases 200187

Ischemia, Injury, & Infarction Ischemia, Injury, & Infarction
3 Zones of Damage3 Zones of Damage
Infarction = NecrosisInfarction = Necrosis-MI, dead cells-MI, dead cells
InjuryInjury-some recovery possible-some recovery possible
IschemiaIschemia- full recovery possible- full recovery possible
88

Zones of Tissue DamageZones of Tissue Damage
Goal is to limit the area of Goal is to limit the area of necrosis (infarction) !necrosis (infarction) !
• Necrotic myocardial cells Necrotic myocardial cells are gradually replaced with are gradually replaced with scar tissue scar tissue • Scar tissue cannot contract Scar tissue cannot contract or conduct action potentialsor conduct action potentials
89

An Acute MI (AMI) Leaves Behind an An Acute MI (AMI) Leaves Behind an Area of Yellow NecrosisArea of Yellow Necrosis
90

Pathologic ChangesPathologic Changes
Ischemic areas cease to function within Ischemic areas cease to function within minutesminutes
Irreversible damage/death to myocardial cells Irreversible damage/death to myocardial cells occurs within 20-40 minutesoccurs within 20-40 minutes
Early reperfusion (20min) after onset of Early reperfusion (20min) after onset of ischemia can prevent necrosis, prevent further ischemia can prevent necrosis, prevent further ischemia and necrosisischemia and necrosis
91

Pathologic Changes Pathologic Changes
Extent of infarct depends on :Extent of infarct depends on : locationlocation extent of occlusion extent of occlusion amount of heart tissue supplied by amount of heart tissue supplied by
vessel, duration of occlusionvessel, duration of occlusion metabolic needs of the affected tissuemetabolic needs of the affected tissue extent of collateral circulationextent of collateral circulation
92

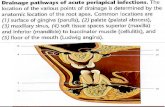
Pathologic Pathologic ChangesChanges
Transmural infarctTransmural infarctFull thickness of ventricular Full thickness of ventricular
wall, wall, Occurs with obstruction of a Occurs with obstruction of a
single artery; single artery; May involve RV, LV and/or IV May involve RV, LV and/or IV
septumseptum Subendocardial infarctSubendocardial infarct
Involve inner 1/3 to 1/2 Involve inner 1/3 to 1/2 ventricular wall, ventricular wall,
May occur with severely May occur with severely narrowed arteries or with narrowed arteries or with occlusion of a very small occlusion of a very small arteryartery
Porth, 2007, Essential of Pathophysiology, 2nd ed., Lippincott, p. 328.
93

94

Chest Pain AssessmentChest Pain Assessment
P - ProvocationP - Provocation Q - QualityQ - Quality R – Region/RadiationR – Region/Radiation S - SeverityS - Severity T – TimingT – Timing
95

Categories (PQRST)Categories (PQRST) Angina that occurs with stress Angina that occurs with stress
(physical/emotional)(physical/emotional)Relieved within minutes by Relieved within minutes by
rest or NTG?rest or NTG? Angina that occurs with restAngina that occurs with rest Is of new onsetIs of new onset Increasing intensityIncreasing intensity
risk risk forforMIMI
96

97

Stable AnginaStable Angina Fixed coronary obstructionFixed coronary obstruction 0022 Demand Demand 0 022 supply supply pain pain
Physical/emotional stress, coldPhysical/emotional stress, cold Provoked by stressorProvoked by stressor
Relieved with rest/NTGRelieved with rest/NTG Not everyone with CHD has anginaNot everyone with CHD has angina
Sedentary lifestyle (couch potatoes), Sedentary lifestyle (couch potatoes), development of collateral circulation, development of collateral circulation, altered perception painaltered perception pain
98

Usual distribution of pain Less common sites of pain distribution
Typically precordial, substernalAnginaAngina
99

Variant or Vasospastic AnginaVariant or Vasospastic Angina ““Prinzmetal’s angina”Prinzmetal’s angina” Due to coronary artery spasms Due to coronary artery spasms Occurs during rest or with minimal exertion, frequently Occurs during rest or with minimal exertion, frequently
nocturnalnocturnal Mechanism uncertainMechanism uncertain
?SNS activation, VSM Ca?SNS activation, VSM Ca++++ channel dysfunction, channel dysfunction, imbalance of endothelial cell vasodilating/constricting imbalance of endothelial cell vasodilating/constricting substancessubstances
Dysrhythmias can occurDysrhythmias can occur Person usually aware; High risk sudden deathPerson usually aware; High risk sudden death
100

Hamon M and Hamon M. N Engl J Med 2006;355:2236
A 38-year-old man was scheduled to undergo invasive coronary angiography after cardiac scintigraphy revealed silent ischemia of the anterior myocardial wall
Variant or Vasospastic AnginaVariant or Vasospastic Angina
101

Acute Coronary Syndrome (ACS)Acute Coronary Syndrome (ACS)
NSTEMI STEMI
Unstable or ruptured plaque
102

Acute Coronary Syndrome (ACS)Acute Coronary Syndrome (ACS)
103

Unstable AnginaUnstable Angina
Clinical syndrome of myocardial ischemia Clinical syndrome of myocardial ischemia ranging between stable angina and MIranging between stable angina and MI
Usually d/t atherosclerotic plaque disruption, Usually d/t atherosclerotic plaque disruption, plt aggregationplt aggregation
Three presentationsThree presentations
1.1. Symptoms at rest (> 20 minutes)Symptoms at rest (> 20 minutes)
2.2. Severe, frank pain, new onset (< 1month)Severe, frank pain, new onset (< 1month)
3.3. More severe, prolonged, or frequentMore severe, prolonged, or frequent
104

Porth, 2007, Essentials of Pathophysiology, 2nd ed., Lippincott, p. 392. 105

Acute Coronary Syndrome (ACS)Acute Coronary Syndrome (ACS)
106

ST Segment ElevationST Segment Elevation ST segment elevations ST segment elevations
are indicative of are indicative of myocardial damage or myocardial damage or ischemia.ischemia.
It may take some time It may take some time (minutes to hours) for (minutes to hours) for the changes to show the changes to show up, and they may not up, and they may not be present in all EKG be present in all EKG leads.leads.
Porth, 2007, Essentials of Pathophysiology, 2nd ed.,
Lippincott, p. 394.
107

ECG : STEMI vs NSTEMIECG : STEMI vs NSTEMI
108

Non ST Segment Elevation Myocardial InfarctionNon ST Segment Elevation Myocardial Infarction (NSTEMI)(NSTEMI)
How is this different from unstable angina or STEMI?How is this different from unstable angina or STEMI?
Unstable anginaUnstable angina, plaque disruption but no thrombus , plaque disruption but no thrombus or occlusion of the coronary artery, therefore no or occlusion of the coronary artery, therefore no myocardial cell death (no MI).myocardial cell death (no MI).
NSTEMINSTEMI, a thrombus partially occludes a coronary , a thrombus partially occludes a coronary artery. Depending on the degree of occlusion and artery. Depending on the degree of occlusion and oxygen demand of downstream heart cells, there may oxygen demand of downstream heart cells, there may be myocardial cell death (an MI) but insufficient to be myocardial cell death (an MI) but insufficient to produce ST segment elevations.produce ST segment elevations.
109

Porth, 2007, Essentials of Pathophysiology, 2nd ed., Lippincott, p. 392. 110

ST Segment Elevation MIST Segment Elevation MI
Characterized by ischemia of cardiac tissueCharacterized by ischemia of cardiac tissue Area of infarction is determined by the Area of infarction is determined by the
coronary artery that is affected and by its coronary artery that is affected and by its distribution of blood flowdistribution of blood flow40-50% of time - LAD40-50% of time - LAD30-40% of time - RCA30-40% of time - RCA15-20% of time - LCA15-20% of time - LCA
111

Porth, 2007, Essentials of Pathophysiology, 2nd ed., Lippincott, p. 392. 112

Diagnosis CHD and MIDiagnosis CHD and MI
Good history & identification of risk Good history & identification of risk factorsfactors
R/O Other causes of CP, eg GERDR/O Other causes of CP, eg GERD ECGECG Serum myocardial markersSerum myocardial markers Stress testing Stress testing Cardiac catheterizationCardiac catheterization
113

““Classic” Manifestations of MIClassic” Manifestations of MI Abrupt onset or progression of unstable, Abrupt onset or progression of unstable,
non-ST elevationnon-ST elevation Pain is severe, crushing, “someone sitting Pain is severe, crushing, “someone sitting
on my chest”on my chest” Radiates to left arm, jaw, neckRadiates to left arm, jaw, neck MI pain is prolonged, not relieved by rest MI pain is prolonged, not relieved by rest
and/or NTG (unlike angina)and/or NTG (unlike angina) N/V, SNS activation N/V, SNS activation HR, HR, RR, RR,
diaphoresis, cool/clammy skindiaphoresis, cool/clammy skin114

ECG ChangesECG Changes T wave inversionT wave inversion ST segment elevationST segment elevation Abnormal Q waveAbnormal Q wave
(may not appear immediately)(may not appear immediately)
Changes can occur over Changes can occur over time, depending on time, depending on duration of ischemia duration of ischemia (extent & location)(extent & location)
Changes may not be Changes may not be present in all leads – take present in all leads – take 12-lead EKG12-lead EKG
115

ST SegmentsST Segments 11stst to change during to change during
ischemia or MI ischemia or MI because myocardial because myocardial repolarization is repolarization is altered.altered.
Ischemia reduces Ischemia reduces membrane potential membrane potential and shorten duration and shorten duration of AP in ischemic of AP in ischemic area.area.
116

Abnormal Q WavesAbnormal Q Waves
Develop because there is no Develop because there is no depolarizing current conduction depolarizing current conduction from necrotic tissuefrom necrotic tissue
May not appear immediatelyMay not appear immediately Diagnostic of MIDiagnostic of MI Q waves are permanent after MIQ waves are permanent after MI
117

Serum Markers for Ischemia & MISerum Markers for Ischemia & MI Necrotic cells release intracellular enzymes Necrotic cells release intracellular enzymes
into blood streaminto blood stream Measure these in blood, larger the number, Measure these in blood, larger the number,
the larger the amount of necrotic tissuethe larger the amount of necrotic tissueCK-MB CK-MB (Creatine-kinase-myocardial bands)(Creatine-kinase-myocardial bands)TroponinTroponinC-reactive ProteinC-reactive Protein
118

CK-MBCK-MB
CK normal in all muscle cells, has 3 CK normal in all muscle cells, has 3 isoenzymes BB, MM, MBisoenzymes BB, MM, MB
CK-MB Creatine kinase -myocardial CK-MB Creatine kinase -myocardial bands is cardiac specificbands is cardiac specific
Elevated within 8 hours after MIElevated within 8 hours after MI Returns to normal in 2-3 daysReturns to normal in 2-3 days Nl ~ 24-195 IU/LNl ~ 24-195 IU/L
119

Troponin Troponin (TnC, TnI, TnT)(TnC, TnI, TnT) Part of the actin-myosin filamentPart of the actin-myosin filament Rises within 3 hours after MIRises within 3 hours after MI Remains elevated 3-4 days, & up to 10 daysRemains elevated 3-4 days, & up to 10 days Diagnostic of MI; No change with ischemiaDiagnostic of MI; No change with ischemia Nl ~ 0.4 ng/mlNl ~ 0.4 ng/ml
120

C-Reactive Protein (CRP)C-Reactive Protein (CRP)
Marker of chronic inflammationMarker of chronic inflammation Maybe a marker of riskMaybe a marker of risk Identifies people before they are Identifies people before they are
symptomaticsymptomatic May guide preventative therapy in future May guide preventative therapy in future
121

Cardiac MarkersCardiac Markers
Hr 1 2 3 4 5 6 7 8 9 10 11 12 Day 2 3 4 5
Troponin
CK-MB
122

NSTEMINSTEMIUnstable anginaUnstable angina
No ECG No ECG ssElevation of serum Elevation of serum
markersmarkers
Unstable AnginaUnstable AnginaPain is severePain is severe
No ECG No ECG ssNo change in markersNo change in markers
ACSACS
No ST ElevationNo ST Elevation STEMISTEMI
123

124

ACS Case Presentation 1 68 yr male; 3 mos. h/o progressive chest pain; day of adm, with minimal exertion
Risk factors: Smoking; HTN; cholesterol; diabetes
Physical exam: normal
ECG: sinus rhythm; no ST or T-wave abnormalities
Biochemical markers at 10 hours: CK = 58; CKMB = <1 ng/ml; Tn= 0.31 ng/ml
Not an MI !! 125

Management of Management of Angina & CHD/AMIAngina & CHD/AMI
Goals: Goals: • Prevent or minimize infarctionPrevent or minimize infarction• Increase oxygen supply to myocardiumIncrease oxygen supply to myocardium• Decrease metabolic (oxygen) demandsDecrease metabolic (oxygen) demands• Symptom reliefSymptom relief
126

Management of Management of Angina & CHD/AMIAngina & CHD/AMI
TreatmentTreatment Non-pharmacologic: Percutaneous Non-pharmacologic: Percutaneous Coronary Intervention (PCI), life style Coronary Intervention (PCI), life style modificationsmodifications Pharmacologic: anti-platelet drugs, Pharmacologic: anti-platelet drugs, beta blockers, nitratesbeta blockers, nitrates
127

Acute Management: ReperfusionAcute Management: Reperfusion PTCA/PCIPTCA/PCI
ASAPASAPWith or without With or without
thrombolyticsthrombolyticsOften includes Often includes
placement of a placement of a stentstent
CABGCABG
•ThrombolyticsThrombolytics- Tissue plasminogen - Tissue plasminogen activator (t-PA)activator (t-PA)
- Streptokinase- Streptokinase
- Urokinase- Urokinase
- Reteplase Reteplase (modification of t-PA)(modification of t-PA)
128

ReperfusionReperfusion
McCance 5th Ed, 2006 Figure 30-2129

Reperfusion – Balloon Angioplasty, Reperfusion – Balloon Angioplasty, Possibly with StentingPossibly with Stenting
Copyright © 2005 Nucleus Communications, Inc. All rights reserved. www.nucleusinc.com
http://www.orbusneich.com/patients/genous/treatment/stenting/?PHPSESSID=d3bf5eb0eed5f6a353d73c
130

Complication of PCIComplication of PCI
N Engl J Med 2011;364:453-64.131

Administration of Thrombolytic Administration of Thrombolytic Therapy Must be Done PromptlyTherapy Must be Done Promptly
Giugliano & Braunwald, Circulation 2003;108;2828-2830
IRA = infarct-related artery
132

PCI (angioplasty ± stenting) must be PCI (angioplasty ± stenting) must be done promptlydone promptly
Nallamothu B et al. N Engl J Med 2007;357:1631-1638 133

Emergency Pain ReliefEmergency Pain Relief
Morphine SulfateMorphine Sulfate VenodilationVenodilation
Reduces preload & cardiac workReduces preload & cardiac work ““Modest” arterial vasodilationModest” arterial vasodilation
Reduces afterload & cardiac workReduces afterload & cardiac work
134

NitroglycerinNitroglycerinAnginaAnginaAcute myocardial infarctionAcute myocardial infarction
Mechanism of Action:Mechanism of Action:Prevents vasospasm of coronary arteriesPrevents vasospasm of coronary arteriesVenodilator Venodilator Decreases preload Decreases preload
Decreases LVEDV Decreases LVEDV
Decreases cardiac Decreases cardiac workwork
135

NitroglycerinNitroglycerin
Purpose/OnsetPurpose/Onset AdministrationAdministration DurationDuration
SLSL Acute anginaAcute angina
1 – 3 min1 – 3 min
0.3 – 0.6 mg 0.3 – 0.6 mg prnprn
30 - 60 30 - 60 minmin
IVIV Acute, unstable Acute, unstable
1-3 min1-3 min
5 microgm/min 5 microgm/min then increasethen increase
Special tubingSpecial tubing Glass bottlesGlass bottles Increased Increased
tolerancetolerance
3 - 5 min3 - 5 min
Lehne, 2006 Tables 50-3 and 50-4136

NitroglycerinNitroglycerinPharmacokineticsPharmacokinetics
• Metabolized in the liver• Excreted by liver & kidneys• Use with caution in patients with liver
or kidney disease• Onset & duration of action administration route dependent
137

NitroglycerinNitroglycerin
ContraindicationsContraindications Severe hypotensionSevere hypotension Increased ICPIncreased ICP Cerebral hemorrhageCerebral hemorrhage Severe anemiaSevere anemia
138

Nitroglycerin Nitroglycerin DrugDrugDrug InteractionsDrug Interactions AlcoholAlcohol
SEVERE hypotension; CV collapseSEVERE hypotension; CV collapse HeparinHeparin
Decreased anticoagulationDecreased anticoagulation LithiumLithium
Possible lithium toxicityPossible lithium toxicity FentanylFentanyl
SEVERE hypotension; Increased fluid SEVERE hypotension; Increased fluid requirementsrequirements
139

Chronic HD & Angina ManagementChronic HD & Angina Management NitratesNitrates Beta BlockersBeta Blockers Calcium channel Calcium channel
blockersblockers
140

Nitrates: Chronic AnginaNitrates: Chronic AnginaPurpose/OnsetPurpose/Onset AdministrationAdministration DurationDuration
OralOral
Isosorbide Isosorbide dinitratedinitrate
Sustained txSustained txPrevent stable Prevent stable
anginaangina
20 - 45 min20 - 45 min
2.5 - 6.5 mg 2.5 - 6.5 mg
1 – 4 x daily1 – 4 x daily
3 - 8 hrs3 - 8 hrs
TransdermalTransdermal
NitroglycerineNitroglycerine
Sustained txSustained txPrevent stable Prevent stable
anginaangina
20 – 60 min20 – 60 min
Patch 1 / dayPatch 1 / day
Ointment Ointment
1-2 in., 4-6 hrs1-2 in., 4-6 hrs Avoid Avoid tolerance tolerance
(PM respite)(PM respite)
2 – 24 hrs2 – 24 hrs
Lehne, 2006 Tables 50-3 and 50-4141

Nitroglycerin Nitroglycerin Patient/Family EducationPatient/Family Education
SLSL Tabs between cheek/lip & gumTabs between cheek/lip & gum Don’t swallowDon’t swallow 1 tab q 5 min x 3, Call 911 if chest pain continues1 tab q 5 min x 3, Call 911 if chest pain continues
NO ALCOHOL!NO ALCOHOL! Slow position changes; orthostatic hypotensionSlow position changes; orthostatic hypotension Headaches are not uncommonHeadaches are not uncommon Check expiration date on tabletsCheck expiration date on tablets
142

Angina ProphylaxisAngina Prophylaxis
““Medical management” of symptomatic coronary Medical management” of symptomatic coronary artery disease (stable angina) has been shown to have artery disease (stable angina) has been shown to have similar outcomes when compared with interventions similar outcomes when compared with interventions such as balloon angioplasty with stenting.such as balloon angioplasty with stenting.
Most stents are actually not FDA approved for stable Most stents are actually not FDA approved for stable angina.angina. They are indicated for acute coronary syndromes They are indicated for acute coronary syndromes
(to be covered in a few minutes).(to be covered in a few minutes).
143

Beta-adrenergic Blocking AgentsBeta-adrenergic Blocking Agents Manage stable angina (not vasospastic)Manage stable angina (not vasospastic) Block beta-1 receptorsBlock beta-1 receptors
Negative inotropeNegative inotrope Negative chronotropeNegative chronotrope Negative dromotropeNegative dromotrope
reduce myocardial oxygen demandreduce myocardial oxygen demand Prevent Sudden Death!Prevent Sudden Death!
More on these later……More on these later……
144

Calcium Channel BlockersCalcium Channel Blockers
Verapamil, diltiazem, nifedipineVerapamil, diltiazem, nifedipine Manage stable & vasospastic anginaManage stable & vasospastic angina Block calcium entry into cellBlock calcium entry into cell
Arterial vasodilationArterial vasodilation Decreases heart rate (SA node firing, AV Decreases heart rate (SA node firing, AV
node conduction)node conduction) Negative intotropeNegative intotrope
reduce myocardial oxygen demandreduce myocardial oxygen demand
145

Anti-platelet drugsAnti-platelet drugsAspirin, Aspirin,
clopidorel (Plavix), clopidorel (Plavix), IIb,IIIa inhibitors (Repro)IIb,IIIa inhibitors (Repro)
Decrease platelet Decrease platelet aggregation aggregation
Prevent thrombus Prevent thrombus formationformation
AnticoagulantsAnticoagulants
Heparin, warfarinHeparin, warfarin
Reduce fibrin Reduce fibrin production production
Suppress clottingSuppress clotting
OPEN!OPEN!Keep arteriesKeep arteries
146

Kumar (2003)
IIb-IIIa Inhibitors Abciximab (RePro@)Alter Platelet Aggregation
- Onset 2 hours
- Duration 48 hours
- Infuse with filter147

Anti-platelet & Anticoagulant DrugsAnti-platelet & Anticoagulant Drugs
Contraindications Contraindications Active bleedingActive bleedingCVA w/i 2 yrsCVA w/i 2 yrsGI/GU bleedingGI/GU bleeding
w/i 6 weeksw/i 6 weeks
ThrombocytopeniaThrombocytopeniaAneurysmAneurysmIntracranial neoplasmIntracranial neoplasm
Major side effectMajor side effect BLEEDINGBLEEDING Intracranial, Intracranial,
retroperitoneal, retroperitoneal, hematemesishematemesis
LabsLabs PT/INR, PTT, PT/INR, PTT,
Activated clotting Activated clotting Time (ACT), Time (ACT), platelet countplatelet count
148

You having an MI ??You having an MI ??
149

Which of the following is present in Which of the following is present in stable angina?stable angina?
An uns
table
pla
que
A ruptu
red p
laque
A sta
ble p
laqu
e
A pla
que with
a th
ro...
25%25%25%25%
1.1. An unstable plaque.An unstable plaque.
2.2. A ruptured plaqueA ruptured plaque
3.3. A stable plaqueA stable plaque
4.4. A plaque with a A plaque with a thrombus.thrombus.
150

Which of the following is Which of the following is diagnosticdiagnostic of an acute myocardial infarction?of an acute myocardial infarction?
ST s
egm
ent e
le...
Incr
ease
d ser
u...
Chest
pai
n at r
est
Incr
ease
d C-re
activ
e p.
..
25% 25%25%25%
1.1. ST segment elevationST segment elevation
2.2. Increased serum CK-MB Increased serum CK-MB
3.3. Increased serum troponinsIncreased serum troponins
4.4. Increased C-reactive Increased C-reactive proteinprotein
151

Management of unstable angina or acute Management of unstable angina or acute myocardial infarction must include myocardial infarction must include interventions/medications that:interventions/medications that:
Incr
ease
oxy
ge...
Dec
reas
e th
e o...
Rel
ieve
the
sy...
All
of the
abo...
25% 25%25%25%1.1. Increase oxygen supply Increase oxygen supply to the myocardium to the myocardium
2.2. Decrease the oxygen Decrease the oxygen demands of the demands of the myocardium myocardium
3.3. Relieve the symptomsRelieve the symptoms
4.4. All of the above All of the above
152

Need a break?Need a break?
153

Heart FailureHeart Failure
154

Heart FailureHeart Failure Failure of the heart to function as a pumpFailure of the heart to function as a pump Normally pumping ability adjusts to body Normally pumping ability adjusts to body
needs for Oneeds for O22
Cardiac ReserveCardiac Reserve Ability to Ability to CO during CO during need need Athletes have large cardiac reserveAthletes have large cardiac reserve HF pts (and elderly) have poor cardiac HF pts (and elderly) have poor cardiac
reserve reserve
155

Heart FailureHeart Failure
HF involves interplay between 2 factors:HF involves interplay between 2 factors:1.1. Inability of failing heart to maintain Inability of failing heart to maintain
sufficient CO to support body functionssufficient CO to support body functions
2.2. Recruitment ( and subsequent failure) of Recruitment ( and subsequent failure) of compensatory mechanisms designed to compensatory mechanisms designed to maintain cardiac reservemaintain cardiac reserve
156

Cardiac OutputCardiac Output
Stroke Stroke VolumeVolume
Heart Heart RateRate
PreloadPreload
LVEDVLVEDV
AfterloadAfterload
SVRSVR
ContractilityContractility
LVSWI LVSWI
Determinant of Cardiac OutputDeterminant of Cardiac Output
157

SV
Contractility
CO
O2 to Organs
Trigger Compensatory
Mechanisms
Blood volumeVascular resistance
Cardiac work
HF
158

Vicious Cycle of Heart FailureVicious Cycle of Heart Failure
Lehne, 2009, Pharmacology for Nursing Care, 7th ed., Elsevier, p. 518 159

Compensatory Mechanisms Compensatory Mechanisms Maintain Vital Organ PerfusionMaintain Vital Organ Perfusion
Compensated heart failureCompensated heart failureShort term useShort term use
Decompensated heart failureDecompensated heart failureCompensatory mechanisms no longer Compensatory mechanisms no longer
effectiveeffectiveCompensatory mechanisms become Compensatory mechanisms become
detrimentaldetrimental
160

Compensatory MechanismsCompensatory Mechanisms Frank Starling mechanismFrank Starling mechanism Increased SNS activityIncreased SNS activity
HR, HR, preload d/t alpha receptor stimulation preload d/t alpha receptor stimulation Renin-angiotensin-aldosterone systemRenin-angiotensin-aldosterone system Atrial natriuretic peptideAtrial natriuretic peptide
Hormone release from atrial cells in response to Hormone release from atrial cells in response to stretch. stretch. Promotes diuresis.Promotes diuresis.
Myocardial HypertrophyMyocardial Hypertrophy in number of contractile elements in myocardial cells to in number of contractile elements in myocardial cells to
contractile performance contractile performance
161

162

163

Causes of CHFCauses of CHFImpaired Cardiac FunctionImpaired Cardiac Function Excess Work DemandsExcess Work Demands
Myocardial DiseaseMyocardial Disease Increased PressureIncreased Pressure
CardiomyopathyCardiomyopathy Systemic hypertensionSystemic hypertension
Myocardial infarctionMyocardial infarction Pulmonary hypertensionPulmonary hypertension
Coronary artery diseaseCoronary artery disease Coarctation of aortaCoarctation of aorta
MyocardititsMyocarditits Increased Volume WorkIncreased Volume Work
Cardiac Valve DiseaseCardiac Valve Disease A-V shuntA-V shunt
Congenital Heart DefectsCongenital Heart Defects Excessive administration Excessive administration of IV fluidsof IV fluids
164

Heart FailureHeart Failure Pulmonary and/or systemic venous congestionPulmonary and/or systemic venous congestion Described asDescribed as
Systolic vs diastolic failureSystolic vs diastolic failure Right vs left sided failureRight vs left sided failure
165

Systolic DysfunctionSystolic Dysfunction
Impaired ejectionImpaired ejection
cardiac contractilitycardiac contractility CO CO
Conditions that Conditions that contractility: contractility:ischemic heart disease,ischemic heart disease, preload, preload, afterload afterload
Symptoms mainly result of Symptoms mainly result of COCO “ “forward” flowforward” flow
Porth 2005 28-4
EF
167

Diastolic DysfunctionDiastolic Dysfunction
Porth 2005 28-4
Impaired fillingImpaired filling
LV Filling LV Filling CO CO
Conditions that cause diastolic Conditions that cause diastolic dysfunction: conditions that restrict dysfunction: conditions that restrict diastolic fillingdiastolic filling
- MV stenosis- MV stenosis- - ventricular hypertrophy ventricular hypertrophy- Delay diastolic relaxation (aging)- Delay diastolic relaxation (aging)
EF
168

“Backward”
“Forward”
170

Right Heart Failure (RHF) fluid fluid accumulation in accumulation in systemic venous systemsystemic venous system venous congestion venous congestion peripheral edemaperipheral edema
CausesCauses::Pulmonic valve stenosis Pulmonic valve stenosis or regurgitationor regurgitationRV infarctionRV infarctionCardiomyopathyCardiomyopathyPEPE (or anything else (or anything else PVR)PVR)
Cor Pulmonale:Cor Pulmonale: RHF RHF caused by lung diseasecaused by lung disease
Signs &Symptoms:
171

Left Heart Failure (LHF)
PathophysiologyPathophysiology::
COCO LA & LV EDV & LA & LV EDV & pulmonary pressure pulmonary pressure eventually pulmonary eventually pulmonary edema.edema.
CausesCauses::
Acute MIAcute MIHypertensionHypertensionCardiomyopathyCardiomyopathyMV stenosis/regurgitationMV stenosis/regurgitation
Signs & Symptoms
• Renal dysfunction
172

BNP: B-Type natriuretic peptideBNP: B-Type natriuretic peptide Synthesized in myocardium Synthesized in myocardium
of ventriclesof ventricles Released in response to Released in response to
ventricular dilation & ventricular dilation & overloadoverload
Normal ~ 1-30 picogms/mlNormal ~ 1-30 picogms/ml Normally increases with Normally increases with
age, renal failure, age, renal failure, B-Blockers, diureticsB-Blockers, diuretics
173

BNP in BNP in Heart FailureHeart Failure
• DiagnosisDiagnosis BNP < 100, used to rule out new HF BNP < 100, used to rule out new HF Higher levels associated with more myocardial Higher levels associated with more myocardial
damagedamage
• Prognosis and guiding therapyPrognosis and guiding therapy Increased risk of death or readmission, Increased risk of death or readmission,
independent of clinical findingsindependent of clinical findings Relevant changes in level and role for Relevant changes in level and role for
determining treatmentdetermining treatment
174

HF ClassificationsHF ClassificationsACC/AHAACC/AHA NYHA Functional ClassNYHA Functional Class
AA High Risk; no structural High Risk; no structural disease or symptomsdisease or symptoms
BB Structural disease; no Structural disease; no symptomssymptoms
II Asymptomatic Asymptomatic
CC Structural disease with Structural disease with symptomssymptoms
IIII Symptomatic w/ moderate Symptomatic w/ moderate exertionexertion
IIIIII Symptomatic w/ minimal Symptomatic w/ minimal exertionexertion
DD Advanced structural Advanced structural disease; severe symptoms; disease; severe symptoms; invasive tx neededinvasive tx needed
IVIV Symptomatic at rest Symptomatic at rest
175

Heart Failure ManagementHeart Failure ManagementGOALSGOALS
1. Reduce myocardial restructuring / remodeling1. Reduce myocardial restructuring / remodeling ACE-I, ARB, beta blockers ACE-I, ARB, beta blockers
2. Reduce/minimize symptoms 2. Reduce/minimize symptoms improve quality of life!!!improve quality of life!!! diuretics, digoxindiuretics, digoxin
3. Improve contractility 3. Improve contractility increase CO, vital organ perfusionincrease CO, vital organ perfusion dobutamine, digoxindobutamine, digoxin
176

Diuretics Preload
Vasodilators Afterload
177

Diuretic TherapyDiuretic Therapy
Furosemide (Lasix)Furosemide (Lasix) Ascending loop of Ascending loop of
HenleHenle Block Na+ & Cl- Block Na+ & Cl-
reabsorption reabsorption prevent water prevent water reabsorptionreabsorption
Rapid onsetRapid onset PO 60 minPO 60 min IV 5 minIV 5 min
Lehne 2007, Fig 40-2178

Loop Diuretics Adverse EffectsLoop Diuretics Adverse Effects HypotensionHypotension
Volume lossVolume lossVenodilationVenodilation
HypokalemiaHypokalemiaVentricular dysrythmiasVentricular dysrythmiasIncrease risk of dig toxicityIncrease risk of dig toxicity
HyponatremiaHyponatremia HypochloremiaHypochloremia
179

Afterload Reduction in HFAfterload Reduction in HFVasodilationVasodilation - - Decrease resistance to ventricular Decrease resistance to ventricular ejection of blood ejection of blood- Improves forward blood flow- Improves forward blood flow- Reduce cardiac workload- Reduce cardiac workload- Reduce compensatory myocardial - Reduce compensatory myocardial remodeling remodeling
180

Angiotensin Converting Enzyme Angiotensin Converting Enzyme Inhibitors (ACE-I)Inhibitors (ACE-I)
(captopril, lisinopril, enalipril)(captopril, lisinopril, enalipril)
Mechanism of ActionMechanism of ActionInhibit angiotensin I conversion to angiotensin IIInhibit angiotensin I conversion to angiotensin II
Prevents vasoconstrictionPrevents vasoconstriction Dilate arterioles (Dilate arterioles ( afterload) afterload)
Decreases aldosterone release (Decreases aldosterone release ( preload) preload)
181

Angiotensin II Receptor Blockers Angiotensin II Receptor Blockers (ARBs)(ARBs)
(valsartan)(valsartan)
Mechanism of ActionMechanism of ActionBlocks actions of angiotensin II at its receptorBlocks actions of angiotensin II at its receptor
Aldosterone release Aldosterone release Dilate arterioles Dilate arterioles
Na & HNa & H22O excretionO excretion AfterloadAfterload
PreloadPreload
182

ALLALL Heart Failure Patients Heart Failure Patients SHOULD BE ONSHOULD BE ON
an ACE-I or ARB !!!!!!!!an ACE-I or ARB !!!!!!!!
American College of Cardiologists, American College of Cardiologists,
TJC, NQF, AHRQTJC, NQF, AHRQ
183

Beta blockers and HFBeta blockers and HF
Selective use due to negative inotropic effectSelective use due to negative inotropic effect Decrease contractility and afterload Decrease contractility and afterload reduce reduce
cardiac re-modelingcardiac re-modeling Cardioselective beta blockers have been Cardioselective beta blockers have been
shown to improve morbidity & mortalityshown to improve morbidity & mortality Ex. metoprolol (Ex. metoprolol (beta)beta), bisoprolol (, bisoprolol (beta)beta), ,
carvedilol carvedilol (alpha & beta blocker) (alpha & beta blocker)
184

Digoxin: Considerations in HFDigoxin: Considerations in HF Increases intracellular calcium concentration Increases intracellular calcium concentration
improves contractility improves contractility PLUSPLUS slows heart rate slows heart rate
Provides symptom reliefProvides symptom relief Treatment should begin with low doses (≤ 0.125 Treatment should begin with low doses (≤ 0.125
mg/d), esp. in elderly, women or kidney diseasemg/d), esp. in elderly, women or kidney disease Serum concentrations 0.5–0.9 ng/mL Serum concentrations 0.5–0.9 ng/mL Risk factors for digoxin toxicity (≥ 1 ng/mL): old Risk factors for digoxin toxicity (≥ 1 ng/mL): old
age, female sex, high serum creatinine, use of age, female sex, high serum creatinine, use of non– potassium-sparing diuretics non– potassium-sparing diuretics
ACE-I & ARBs ACE-I & ARBs Reduce digoxin therapeutic effect Reduce digoxin therapeutic effect
185

Aldosterone receptor blockerAldosterone receptor blocker (spironolactone [Aldactone])(spironolactone [Aldactone])Advanced HF, symptomatic despite ACE-I, dig, Advanced HF, symptomatic despite ACE-I, dig,
etc.etc.Blocks aldosterone receptors & actionsBlocks aldosterone receptors & actionsBenefits in HFBenefits in HF reduces cardiac remodelingreduces cardiac remodeling decreased sympathetic NS activation decreased sympathetic NS activation
Positive inotropic agents: Positive inotropic agents: more on these latermore on these later
186

The renin-angiotensin-aldosterone system contributes to The renin-angiotensin-aldosterone system contributes to worsening of heart failure and myocardial remodeling. worsening of heart failure and myocardial remodeling. Appropriate management includes administration of Appropriate management includes administration of ______ which targets this system.______ which targets this system.
25% 25%25%25%
1.1. Calcium channel Calcium channel blocker blocker
2.2. Angiotensin Angiotensin converting enzyme converting enzyme inhibitor inhibitor
3.3. Diuretic Diuretic
4.4. DigoxinDigoxin187

A patient has severe mitral stenosis which greatly limits blood A patient has severe mitral stenosis which greatly limits blood flow between the left atrium and the left ventricle. This flow between the left atrium and the left ventricle. This condition may produce heart failure due to which of the condition may produce heart failure due to which of the following?following?
Systo
lic d
ysfu
nctio
n
Diast
olic d
ysfu
nctio
n
50%50%
1.1. Systolic dysfunctionSystolic dysfunction
2.2. Diastolic dysfunctionDiastolic dysfunction
188

A patient is newly diagnosed with heart failure. A patient is newly diagnosed with heart failure. Which of the following drugs should Which of the following drugs should alwaysalways be be prescribed?prescribed?
A bet
a blo
cker
A cal
cium
chan
nel b
l...
A diu
retic
An ACE in
hibito
r or A
RB
25%25%25%25%1.1. A beta blockerA beta blocker
2.2. A calcium channel A calcium channel blockerblocker
3.3. A diureticA diuretic
4.4. An ACE inhibitor An ACE inhibitor or ARBor ARB
189

Disorders of Heart ValvesDisorders of Heart Valves
191

Valvular Heart DiseaseValvular Heart Disease Function of the valves is to ensure Function of the valves is to ensure
unidirectionalunidirectional flow of blood in the heart flow of blood in the heart
Dysfunction of valves Dysfunction of valves Narrowing of valve openingNarrowing of valve opening does notdoes not openopen properly = properly = StenosisStenosis Distortion of the valve Distortion of the valve does not does not closeclose properly =properly =RegurgitationRegurgitation
192

StenosisStenosis Valve does not open Valve does not open
properlyproperly resistance to blood flow resistance to blood flow
thru valvethru valve volume & work of the volume & work of the
chamber that empties thru chamber that empties thru narrowed valvenarrowed valve Ex. LA for mitral Ex. LA for mitral
stenosisstenosis Produces distention in one Produces distention in one
chamber & impaired chamber & impaired filling in anotherfilling in another
193

RegurgitationRegurgitation Valve does not close Valve does not close
properlyproperly Permits backflow to occur Permits backflow to occur
when valve should be when valve should be closedclosed Ex. Blood flows back Ex. Blood flows back
into LV during diastole into LV during diastole when aortic valve should when aortic valve should be closedbe closed
Produces distention & Produces distention & work demands on ejecting work demands on ejecting chamber chamber
194

195
Mitral Valve ProlapseMitral Valve Prolapse 2-7% of the population2-7% of the population Most asymptomaticMost asymptomatic Usually unknown cause, Usually unknown cause,
although can be associated although can be associated with a variety of conditionswith a variety of conditions
Palpations (awareness of the Palpations (awareness of the heartbeat) and dysrhythmias heartbeat) and dysrhythmias are common.are common. Dysrhythmias may Dysrhythmias may
produce light-headedness produce light-headedness or fainting.or fainting.
Mitral regurgitation may Mitral regurgitation may necessitate valve repair or necessitate valve repair or replacement.replacement.
Sudden death is rare.Sudden death is rare.
Porth, 2007, Essentials of Pathophysiology, 2nd ed., Lippincott, p. 407.
195

Valvular Heart DiseaseValvular Heart Disease Valve defects are Valve defects are
characterized by heart characterized by heart murmurs resulting from murmurs resulting from turbulent flow thru valveturbulent flow thru valve
Dysfunction d/tDysfunction d/t Congenital, trauma, Congenital, trauma,
ischemia, age, inflammationischemia, age, inflammation Any valve can be involvedAny valve can be involved Aortic & mitral most Aortic & mitral most
commoncommon
196

Diagram in Handout- Use it to figure out murmurs &Problems with blood flow d/t valvular defects!
197

Mitral StenosisMitral Stenosis Incomplete opening of MV Incomplete opening of MV
during diastole during diastole LA distention LA distention
& impaired LV filling& impaired LV filling Resistance thru MV Resistance thru MV LA dilates LA dilates LA pressures LA pressures pulmonary vasculaturepulmonary vasculature pulmonary congestion & pulmonary congestion & HTNHTN Symptoms of Symptoms of CO occur with CO occur with
exertion, or exertion, or HR ( HR (diastolic diastolic filling time)filling time)
198

Mitral Stenosis: Signs & SymptomsMitral Stenosis: Signs & SymptomsWhen would you hear a murmur?
DIASTOLE
199

Mitral Valve RegurgitationMitral Valve Regurgitation Incomplete closure of MVIncomplete closure of MV During systole, part of LV SV During systole, part of LV SV
goes forward into aorta & goes forward into aorta & regurgitant blood flows back regurgitant blood flows back into LA into LA
Result Result CO &/or pulmonary CO &/or pulmonary congestioncongestion
LV enlarges d/t LV enlarges d/t LVEDV LVEDV LA dilates d/t extra volumeLA dilates d/t extra volume Murmur heard during ????Murmur heard during ????
200

Mitral Valve RegurgitationMitral Valve Regurgitation AcuteAcute
forward SV, forward SV, regurgitant SV regurgitant SV LAP LAP pulmonary edema pulmonary edema
Occur with MI, infective endocarditisOccur with MI, infective endocarditis ChronicChronic
Well tolerated, asymptomatic, until LV Well tolerated, asymptomatic, until LV function becomes impaired function becomes impaired
forward SV, forward SV, regurgitant SV regurgitant SV LAP LAP pulmonary edema pulmonary edema
201

Mitral Valve RegurgitationMitral Valve RegurgitationManagementManagement Acute Acute
Improve forward flow with vasodilator, Improve forward flow with vasodilator, eg nitroprussideeg nitroprusside
MV repair, reconstruction, replacementMV repair, reconstruction, replacement ChronicChronic
MV repair, reconstruction, replacementMV repair, reconstruction, replacement
202

Aortic Valve StenosisAortic Valve Stenosis resistance to ejection of resistance to ejection of
blood from LV into aortablood from LV into aorta resistance resistance work of LV work of LV
& & volume of blood ejected volume of blood ejected into systemic circulationinto systemic circulation
ManifestationsManifestations R/T R/T SV SV Hypotension, syncope, Hypotension, syncope,
angina, fatigue, angina, fatigue, HR HR (takes longer to eject (takes longer to eject volume)volume)
203

Aortic Valve RegurgitationAortic Valve Regurgitation Incompetent AoV Incompetent AoV backflow of blood to LV backflow of blood to LV
during diastole during diastole LV volume d/t LA & LV volume d/t LA &
blood leaking back thru blood leaking back thru incompetent valveincompetent valve
Turbulent flow across Turbulent flow across AV during diastole AV during diastole high pitched blowing high pitched blowing sound sound
204

Aortic Valve RegurgitationAortic Valve Regurgitation
AcuteAcuteSudden uncompensated Sudden uncompensated LVEDP LVEDP
pulmonary edema & pulmonary edema & CO CO sympathetic stimulation sympathetic stimulation peripheral vasoconstriction peripheral vasoconstriction afterload afterload CO CO
ChronicChronic Compensated for a whileCompensated for a while
205

Valve Disease Summary
206

Which of the following might Which of the following might produce pulmonary edema?produce pulmonary edema?
Mitr
al s
tenosi
s
Pumon
ic s
tenosi
s
Tricusp
id s
tenosi
s
Tricusp
id re
gurgita
tion
25%25%25%25%
1.1. Mitral stenosisMitral stenosis
2.2. Pulmonic stenosisPulmonic stenosis
3.3. Tricuspid stenosisTricuspid stenosis
4.4. Tricuspid Tricuspid regurgitationregurgitation
207

Kathryn !!!
Pleeeaaase!Release the students!
Mmmm…excellent!
208

Shock:Shock:The rude unhinging of the The rude unhinging of the
machinery of life!machinery of life!
209

ShockShock Adequate perfusion of body tissues depends on:Adequate perfusion of body tissues depends on:
Functioning heart to pump 0Functioning heart to pump 022 into systemic circulation into systemic circulation A vascular system to transport OA vascular system to transport O22 to tissues to tissues Sufficient amount of blood/OSufficient amount of blood/O22
Tissues able to extract OTissues able to extract O22, nutrients from blood, nutrients from blood ShockShock is a condition in which is a condition in which
OO22 & energy supply to tissues is not adequate to meet & energy supply to tissues is not adequate to meet demandsdemands
210

Shock Shock Impairment of cellular metabolismImpairment of cellular metabolism
Impairment of Impairment of oxygen useoxygen use Aerobic to Aerobic to
anaerobic anaerobic metabolismmetabolism
Impairment of Impairment of glucose useglucose use Impaired Impaired
glucose delivery glucose delivery or impaired or impaired glucose uptakeglucose uptake
211

Global Tissue OxygenationGlobal Tissue OxygenationMade Ridiculously SimpleMade Ridiculously Simple
SvO2 = 75%
25%
Venous Oxygen Delivery
ArterialOxygenDelivery
Oxygen Consumption
100%
212

Aerobic Metabolism Anaerobic Metabolism
36 molecules ATP36 molecules ATP 2 molecules ATP2 molecules ATP
Supports normal Supports normal cell functioncell function
Eventual Eventual cell dysfunctioncell dysfunction
213

4 Types of Circulatory Shock4 Types of Circulatory Shock1.1. HypovolemicHypovolemic
Diminished blood volume Diminished blood volume inadequate inadequate filling of vascular compartmentfilling of vascular compartment
Loss of whole blood/plasma, extracellular fluidLoss of whole blood/plasma, extracellular fluid
2.2. CardiogenicCardiogenic Failure of the heart to function as a pumpFailure of the heart to function as a pump
3.3. ObstructiveObstructive Mechanical barrier to blood flow in circulationMechanical barrier to blood flow in circulation
PE, cardiac tamponadePE, cardiac tamponade
4.4. DistributiveDistributive Enlargement of vascular compartmentEnlargement of vascular compartment
214

Compensatory MechanismsCompensatory MechanismsSympathetic Nervous SystemSympathetic Nervous System Heart rateHeart rate Respiratory rateRespiratory rate GlycolysisGlycolysis Urine outputUrine output Blood flow to internal organsBlood flow to internal organs PeristalsisPeristalsis Cool skinCool skin DiaphoresisDiaphoresis
215

216

217

CardiogenicCardiogenicShockShock
218

PreloadPreload
SVSV
Restore Cardiac Pump Restore Cardiac Pump Ventricular ContractilityVentricular Contractility
Positive Inotropic AgentsPositive Inotropic Agents
DepressedDepressed
NormalNormal
EnhancedEnhanced
219

Enhance ContractilityEnhance ContractilityBeta –1 Effect, increase contractilityBeta –1 Effect, increase contractility EpinephrineEpinephrine DobutamineDobutamine DopamineDopamine
AdministrationAdministration Correct hypovolemia 1Correct hypovolemia 1stst !! !! Use infusion pumpUse infusion pump Central venous catheter (CVC) preferred routeCentral venous catheter (CVC) preferred route
220

DobutamineDobutamineBeta-1 selective adrenergic agonistBeta-1 selective adrenergic agonist First line to increase cardiac outputFirst line to increase cardiac output
Increase contractility & HR via beta-1Increase contractility & HR via beta-1 Typical dose 2.5 – 10 microgm/kg/minTypical dose 2.5 – 10 microgm/kg/min
Adverse EffectsAdverse Effects DysrhythmiasDysrhythmias
When possible give via central venous catheter (CVC) When possible give via central venous catheter (CVC) !!!!
221

EpinephrineEpinephrineNon-selective adrenergic agonistNon-selective adrenergic agonist First line in cardiac arrest & anaphylaxisFirst line in cardiac arrest & anaphylaxis
Increase contractility & HR via beta-1Increase contractility & HR via beta-1 Vasoconstriction via alpha-1Vasoconstriction via alpha-1 Bronchodilation via beta-2Bronchodilation via beta-2
Adverse EffectsAdverse Effects DysrhythmiasDysrhythmias AnginaAngina Hyperglycemia in diabeticsHyperglycemia in diabetics Necrosis w/ extravasation Necrosis w/ extravasation Give via CVC!!Give via CVC!!
222

EpinephrineEpinephrineCardiac ArrestCardiac Arrest IV Push IV Push
Pre-filled syringePre-filled syringe Intracardiac Intracardiac
Pre-filled syringePre-filled syringe
w/ really long needle!w/ really long needle!
IV infusionIV infusion Increase contractilityIncrease contractility
223

Cardiogenic Shock
Vasodilators Afterload
224

Afterload Manipulation: Restore Afterload Manipulation: Restore perfusion or Decrease Work of Heartperfusion or Decrease Work of Heart
Systemic Vascular Resistance (SVR)
Vasopressors SV & CO BP & perfusion pressure
SVRSVR
VasodilatorsVasodilators SV& CO SV& CO
BP & work of heartBP & work of heart
SVSV
SVRSVR
225

Sodium Nitroprusside (Nipride)Sodium Nitroprusside (Nipride)
Arterial vasodilatorArterial vasodilator reduces resistance to LV ejectionreduces resistance to LV ejection Improves forward flow & increases SV Improves forward flow & increases SV reduces “backward” pressure in the reduces “backward” pressure in the pulmonary pulmonary
vasculature vasculature decrease pulmonary congestiondecrease pulmonary congestion
Also used in acute mitral regurgitation & Also used in acute mitral regurgitation & hypertensive emergencieshypertensive emergencies
226

Hypovolemic ShockHypovolemic Shock
Acute loss of 15-20% of blood volumeAcute loss of 15-20% of blood volume Characterized by Characterized by blood volume blood volume inadequate inadequate
filling of the vascular compartment filling of the vascular compartment
venous return to right heartvenous return to right heart
preloadpreload
SV SV CO CO
02 delivery to tissues02 delivery to tissues
227

HypovolemicHypovolemicShockShock
228

Clinical ManifestationsClinical Manifestations Mild Mild
HR, HR, BP, cool extremitiesBP, cool extremities Moderate Moderate
HR >100, sBP~90, Restless, diaphoretic, HR >100, sBP~90, Restless, diaphoretic, oliguriaoliguria
Severe Severe HR >120, BP<60, cold extremities, HR >120, BP<60, cold extremities, LOC LOC
229

Frank-Starling Curve:Frank-Starling Curve:PreloadPreload
SVSV
LVEDVLVEDV
LV dysfunctionLV dysfunction
HypovolemiaHypovolemia
NormalNormal
230

Restore Intravascular VolumeRestore Intravascular Volume
Crystalloid InfusionCrystalloid Infusion Isotonic Fluids Isotonic Fluids
0.9% NaCl 0.9% NaCl
(“Normal Saline”)(“Normal Saline”) Plasmalyte (pH 7.40)Plasmalyte (pH 7.40) Ringers LactateRingers Lactate
Colloid Infusion “Volume Expander”
• Albumin• Hetastarch (Hespan)
231

Stop Intravascular Volume Loss Stop Intravascular Volume Loss &/or DIC&/or DIC
Blood productsBlood productsPlatelets Platelets plug the holes plug the holesFresh frozen plasma (Fresh frozen plasma (FFP)FFP)
correct coagscorrect coags
Restore Oxygen Carrying CapacityRestore Oxygen Carrying Capacity– PRBC replace lost boxcars
– Erythropoietin
232

Distributive SDistributive ShockhockLoss of vessel tone, enlargement of vascular Loss of vessel tone, enlargement of vascular
compartment, displacement of vascular compartment, displacement of vascular volume away from heart & central circulationvolume away from heart & central circulation
Loss of sympathetic tone (Loss of sympathetic tone (neurogenic SCIneurogenic SCI)) Presence of vasodilating substances in blood Presence of vasodilating substances in blood
((anaphylactic shockanaphylactic shock)) Presence of inflammatory mediators in blood Presence of inflammatory mediators in blood
((septic shockseptic shock))
233

Septic ShockSeptic Shock Associated with severe infection and the systemic Associated with severe infection and the systemic
response to the infection.response to the infection. Gram negative organisms most common Gram negative organisms most common Mechanisms related to mediators of inflammatory Mechanisms related to mediators of inflammatory
response response VasodilationVasodilation capillary permeabilitycapillary permeability
Endotoxins induce tissue damage by activating Endotoxins induce tissue damage by activating coagulation cascadecoagulation cascade
Manifests as fever, vasodilationManifests as fever, vasodilation
234

235

Septic shockSeptic shockEndotoxin & inflammatory mediator release Endotoxin & inflammatory mediator release
Vasodilation Vasodilation Decrease preload Decrease preload Increase cardiac outputIncrease cardiac output
Capillary “leakage” Capillary “leakage” Edema Edema
Coagulopathies Coagulopathies Disseminated Disseminated Intravascular Coagulation Intravascular Coagulation (DIC)(DIC)
236

What is SIRS?What is SIRS?Systemic Inflammatory Response SyndromeSystemic Inflammatory Response SyndromeOften a precursor to sepsis!Often a precursor to sepsis!
Clinical response arising from a nonspecific insult.Clinical response arising from a nonspecific insult.
SIRS criteria includes 2 or more of the following:SIRS criteria includes 2 or more of the following: Temperature Temperature >> 38 38C or C or << 36 36CC Heart Rate Heart Rate >> 90 beats/min 90 beats/min Respiration Respiration >> 20 breaths/min 20 breaths/min WBC WBC >> 12,000/mm 12,000/mm33, < 4,000/mm, < 4,000/mm33 or >10% or >10%
immature cells (bands)immature cells (bands) PaCOPaCO22 < 32mm Hg < 32mm Hg
237

Continuum of SContinuum of Sepsisepsis
SIRS with a suspected or confirmed infx
SepsisSepsisSIRSSIRS Septic Septic ShockShock
≥2 of the following:Temp: >38°C or <36°CH R: >90 beats/minResps: >20/minWBC : >12,000/mm3, or < 4,000/mm3
1992 Consensus Conf Bone et al. Chest. 1992;101:1644-1654.; 2001 SCCM/ESICM/ACCP/TS/SIS International Sepsis Definition Conference. Crit Care Med 2003 31(4):1250-1256.
Sepsis
+ Hypotension despite fluid
+ perfusion abnormalities+ MODS (>1 organ failure, inability to maintain homeostasis w/o tx)
Severe Severe SepsisSepsis
Sepsis +
> 1 organ dysfunction
238

Sepsis Resuscitation BundleSepsis Resuscitation Bundlewithin 1within 1stst hour of recognition hour of recognition
Obtain serum lactateObtain serum lactate Blood cultures (percutaneous) prior to antibioticsBlood cultures (percutaneous) prior to antibiotics AntibioticsAntibiotics Initiate BP, CVP & ScvO2 monitoringInitiate BP, CVP & ScvO2 monitoring If CVP If CVP << 8 mmHg, Hypotension &/or Lactate >4 8 mmHg, Hypotension &/or Lactate >4
Start:Start:
1000ml crystalloid over 30 min.1000ml crystalloid over 30 min.
Vasopressor if no response to fluidVasopressor if no response to fluid
(Clinically important but not on exam)(Clinically important but not on exam)Dellinger P, et al: Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis Dellinger P, et al: Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis
and Septic Shock 2008. and Septic Shock 2008. Crit Care MedCrit Care Med. 2008;36(1):296-327. 2008;36(1):296-327239

Sepsis Resuscitation BundleSepsis Resuscitation Bundlewithin 1within 1stst 6 hours of recognition 6 hours of recognition
PRBC for Hgb < 7 g/dl, target 7-9 g/dlPRBC for Hgb < 7 g/dl, target 7-9 g/dl Fluid to keep CVP Fluid to keep CVP >> 8 mmHg 8 mmHg MAP MAP >> 65 mmHg 65 mmHg
Crystalloid; Vasopressor if no response to fluidCrystalloid; Vasopressor if no response to fluid ScvO2 ScvO2 >> 70 % 70 %
Dobutamine; RBC if Hct < 30%Dobutamine; RBC if Hct < 30% Transfer to ICUTransfer to ICU
(Clinically important but not on exam)(Clinically important but not on exam)
Dellinger P, et al: Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis Dellinger P, et al: Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2008. and Septic Shock 2008. Crit Care MedCrit Care Med. 2008;36(1):296-327. 2008;36(1):296-327
240

Catecholamines: Adrenergic AgonistsCatecholamines: Adrenergic Agonists
Alpha 1Alpha 1 Beta 1Beta 1 Beta 2Beta 2 DopamineDopamine
VasoconstrictVasoconstrict CardiacCardiac
stimulationstimulation
BronchodilateBronchodilate Renal artery Renal artery dilationdilation
Phenylephrine
Epinephrine
Norepinephrine (Levophed)
Dobutamine
Dopamine Dopamine Dopamine
241

Complications of ShockComplications of Shock““Shock not only stops the machinery, but it wrecks the Shock not only stops the machinery, but it wrecks the
machinery” (Wiggers)machinery” (Wiggers) Many body systems are “wrecked” by shockMany body systems are “wrecked” by shock ComplicationsComplications
Acute respiratory failure/respiratory distress syndromeAcute respiratory failure/respiratory distress syndrome Acute renal failureAcute renal failure GI bleedingGI bleeding Disseminated intravascular coagulationDisseminated intravascular coagulation Multiple organ dysfunction syndromeMultiple organ dysfunction syndrome
242

Cardiac OutputCardiac Output
Stroke Stroke VolumeVolume
Heart Heart RateRate
PreloadPreload AfterloadAfterload
ContractilityContractility
Management of Shock: Oxygen DeliveryManagement of Shock: Oxygen Delivery
SaO2 & HgbSaO2 & Hgb XX
Reverse the causative factor(s)Reverse the causative factor(s)Restore perfusion to cells, tissues, organsRestore perfusion to cells, tissues, organs
243

Global Tissue OxygenationGlobal Tissue OxygenationMade Ridiculously SimpleMade Ridiculously Simple
SvO2 = 75%
25%
Venous Oxygen Delivery
ArterialOxygenDelivery
Oxygen Consumption
100%
244

Appropriate treatment of Appropriate treatment of hypotension related to cardiogenic hypotension related to cardiogenic shock includes:shock includes:
Volu
me
infu
sio...
Vas
opres
sor (
e...
Posi
tive
inotr.
..
Incr
easi
ng hea
...
25% 25%25%25%1.1. Volume infusionVolume infusion
2.2. Vasopressor (eg Vasopressor (eg levophed)levophed)
3.3. Positive inotrope (eg Positive inotrope (eg dobutamine)dobutamine)
4.4. Increasing heart rate Increasing heart rate (eg atropine)(eg atropine)
245

Appropriate treatment of Appropriate treatment of hypotension related to hypovolemic hypotension related to hypovolemic shock includes:shock includes:
Volu
me
infu
sio...
Vas
opres
sor (
e...
Posi
tive
inotr.
..
Incr
easi
ng hea
...
25% 25%25%25%
1.1. Volume infusionVolume infusion
2.2. Vasopressor (eg Vasopressor (eg levophed)levophed)
3.3. Positive inotrope Positive inotrope (eg dobutamine)(eg dobutamine)
4.4. Increasing heart Increasing heart rate (eg atropine)rate (eg atropine)
246

Which of the following will produce Which of the following will produce cold extremities?cold extremities?
Cardi
ogenic
sho
ck
Anaphyl
actic
sho
ck
Septic
shock
Obstru
ctiv
e sh
ock
25%25%25%25%
1.1. Cardiogenic shockCardiogenic shock
2.2. Anaphylactic Anaphylactic shockshock
3.3. Septic shockSeptic shock
4.4. Spinal shockSpinal shock
247

SaO2/HbSaO2/Hb
COCO
O2 Utilization
Extraction & VO2
O2 Utilization
Extraction & VO2
VenousReturnSvOSvO22
O2 Delivery
248

Questions?Questions?
249