Cutaneous manifestations of internal diseases
113
CUTANEOUS MANIFESTATIONS OF INTERNAL DISEASES
-
date post
19-Oct-2014 -
Category
Education
-
view
1.064 -
download
0
description
Transcript of Cutaneous manifestations of internal diseases

CUTANEOUS MANIFESTATIONS OF INTERNAL DISEASES

CUTANEOUS MANIFESTATIONS
Diabetes Mellitus Thyroid disease Adrenal disease Renal Disease Liver disease Rheumatologic disease Nutritional disease

DIABETES MELLITUS
DIABETES MELLITUS
approximately 30% of patients with DM develop skin lesions at some point
Overall prevalence of cutaneous disorders does not differ between type I and type II diabeticsType I patients get more
autoimmune-type lesionsType II patients get more
cutaneous infections

DIABETES MELLITUS
Cutaneous lesions usually appear after the development of DM, but may be the first presenting sign
Four major groups of skin findings1. Skin diseases associated with DM2. Cutaneous infections3. Cutaneous manifestions of diabetic
complications 4. Skin reactions to diabetic treatment

NECROBIOSIS LIPOIDICA (NL)
NL is 3x more common in women.
NL appears earlier (mean age 22) in Type I diabetics than Type II (mean age 49.)
Appearance Begins as an oval, violaceous
patch and expands slowly. Advancing border is red. Central area turns yellowish
brown. Central area atrophies and
telangiectasia become evident. 13% of cases progress to
ulceration

NECROBIOSIS LIPOIDICA (NL)
Classically, NL occurs bilaterally on the pretibial or medial malleolar areas.
Not painful. Spontaneous
resolution occurs in 13-19% with residual scarring.

GRANULOMA ANNULARE (GA)
AppearanceRing of small, firm,
flesh-colored or red papules
If localized, most frequently found on lateral and dorsal surfaces of hands and feet
Can spontaneously regress without scarring

DIABETIC BULLAE Approximately 0.5% of diabetics
Two types have been described More frequent, non-scarring lesions
with a histologic intraepidermal split without acantholysis
Less common, occasionally hemorrhagic bullae that heal with scarring, slight atrophy, and have a histologic subepidermal split
o Trauma and microvascular disease may play a role
Appearance Painless bullae on non-inflamed
base that appear suddenly Most common on the dorsa and sides
of lower legs and feet, sometimes with similar lesions on the hands and forearms
Bullae contain clear, sterile fluid

DIABETIC BULLAE
Bullae tend to heal spontaneously in 2-5 weeks
diagnosis of exclusion DDx: bullous pemphigoid,
epidermolysis bullosa acquisita, porphyria cutanea tarda, bullous impetigo, erythema multiforme
May recur in the same or new locations

ACANTHOSIS NIGRICANS Seen in situations of insulin
resistance Besides in DM, also seen in the
following: Carcinomas, especially of the
stomach Secondary to drugs (nicotinic acid,
estrogen, or corticosteroids) Pineal tumors Other endocrine syndromes (PCOS,
acromegaly, Cushing’s disease, hypothyroidism)
Obesity
Pathogenesis it may be related to insulin
binding insulin-like growth factor receptors on keratinocytes and dermal fibroblasts, thus stimulating growth.

ACANTHOSIS NIGRICANS
AppearanceHyperpigmented,
velvety plaques in body folds, mostly axillae and neck
Can also present on groin, umbilicus, areolae, submammary areas, and on the hands

SKIN INFECTIONS IN DM
Occur in 20-50% of poorly controlled diabetics
More common in Type II May be related to Abnormal microcirculation Hypohidrosis PVD Neuropathy Decreased phagocytosis and killing activity Impaired leukocyte adherence delayed chemotaxis

CANDIDIASIS IN DIABETICS Fungal infections- most
common Candida
Candidial paronychia Inframammary
candidaGenital candida
Oral candidiasis White, curdlike material
adherent to erythematous, fissured oral commisure;
angular stomatitis

CANDIDIASIS IN DIABETICS
Initial pustules on erythematous base that become eroded and confluent

CANDIDIASIS IN DIABETICS
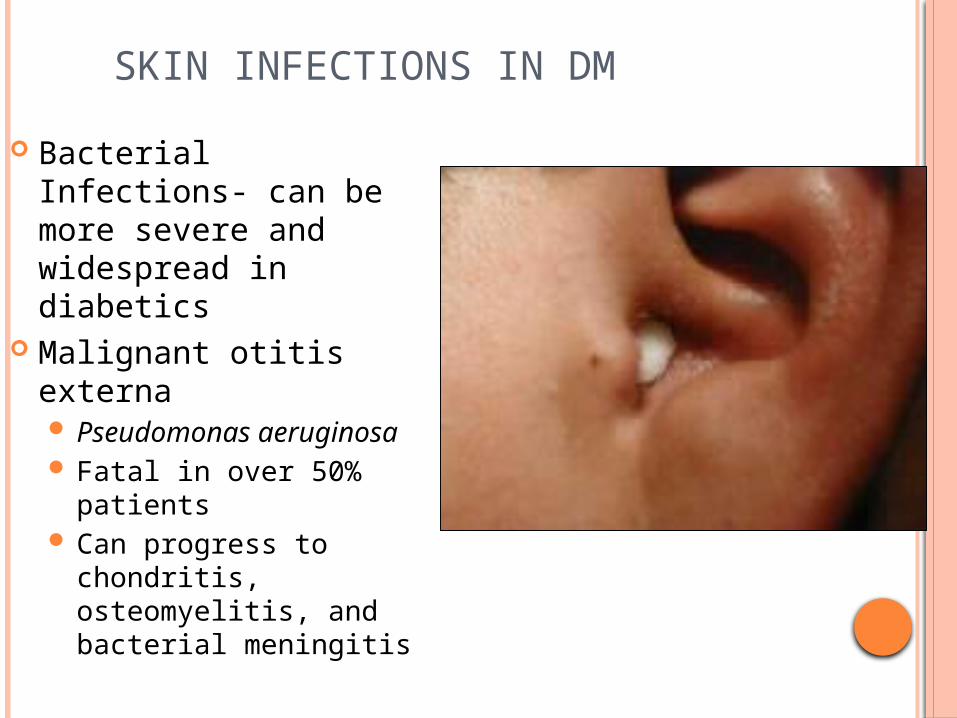
SKIN INFECTIONS IN DM
Bacterial Infections- can be more severe and widespread in diabetics
Malignant otitis externa Pseudomonas
aeruginosa Fatal in over 50%
patients Can progress to
chondritis, osteomyelitis, and bacterial meningitis

SKIN INFECTIONS IN DM
Bacterial infections in DM
Erythrasma Sharply demarcated
erythematous patches upper inner thighs,
axillae, toe web spaces, and inframammary creases
Gram positive Corynebacterium minutissimum
Identified with Wood’s light coral fluorescence
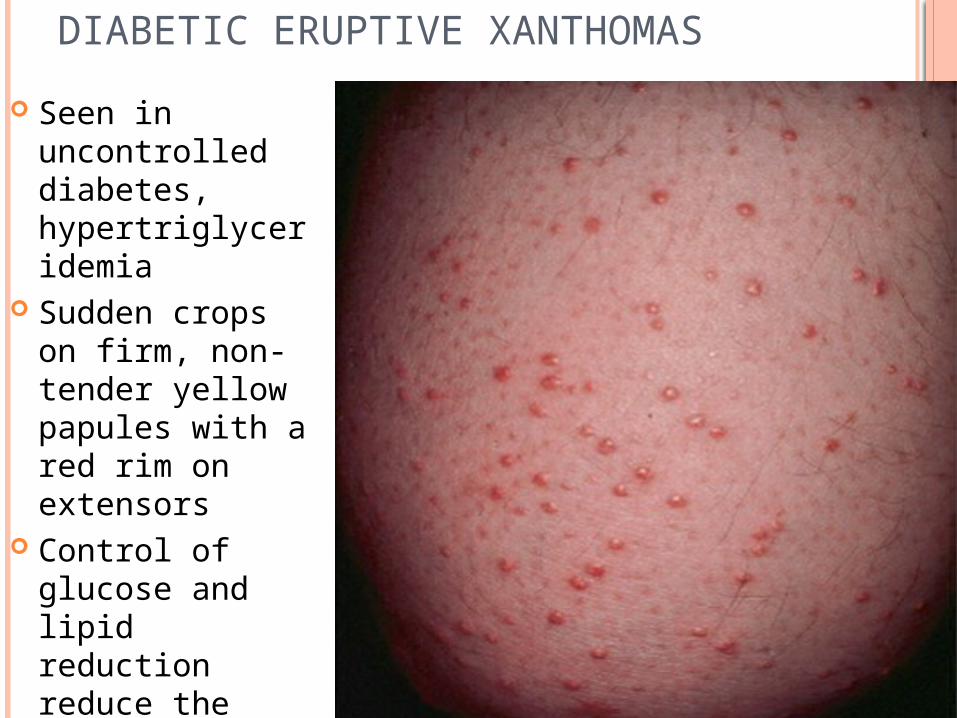
DIABETIC ERUPTIVE XANTHOMAS
Seen in uncontrolled diabetes, hypertriglyceridemia
Sudden crops on firm, non-tender yellow papules with a red rim on extensors
Control of glucose and lipid reduction reduce the lesions

DIABETIC DERMOPATHY AKA “shin spots” or
pigmented pretibial papules
Most common cutaneous manifestation of diabetes
Benign asymptomatic red brown macules on shins
No treatment needed

CUTANEOUS MANIFESTATIONS OF DIABETIC COMPLICATIONS: FOOT ULCERS Peripheral neuropathy leads to unnoticed trauma Vascular complications may lead to ulcers and
complicate ulcer healing Risk of amputation goes up 8x once these develop

CUTANEOUS REACTIONS TO DIABETIC TREATMENT
Insulin Allergy may be local or systemic and
usually occurs within the first month of therapy Erythematous or urticarial pruritic
nodules at the site of injection Lipoatrophy can also occur
Circumscribed depressed areas of skin at the insulin injection site 6-24 months after starting insulin
More common in women and children
Lipohypertrophy can also occur Soft dermal nodules that resemble
lipomas at sites of frequent injection May be a response to the lipogenic
action of insulin Treat and prevent by rotating sites of
injection
CUTANEOUS REACTIONS TO DIABETIC TREATMENT-ORAL HYPOGLYCEMICS
Most rxns are associated with the first-generation
sulfonylureas (chlorpropamide and tolbutamide)
1-5% of patients on these drugs will develop skin
rxns during the first 2 months of treatment
Most commonly, they present with
maculopapular eruptions that resolve despite
continuation of the drug.

THYROID DISEASES
Graves disease
Hyperthyroidism
Hypothyroidism

THYROID HORMONE AND THE SKIN
Thyroid hormone plays a pivotal role in the
growth and formation of hair and sebum
production.
Thyroid hormone stimulates epidermal
oxygen consumption, protein synthesis,
mitosis, and determination of epidermal
thickness.
There is increased cutaneous blood flow and
peripheral vasodilation.

HYPERTHYROIDISM AND THE SKIN Skin is usually warm, moist, and smooth(best assessed on the inner aspect of arm and
over the chest) Facial flushing Palmar erythema Hyperpigmentation, esp. creases of palms and soles(buccal pigementation doesn’t occur) hair is fine and friable, hair loss may be excessive History of early graying Hyperhydrosis, particularly of palms and soles
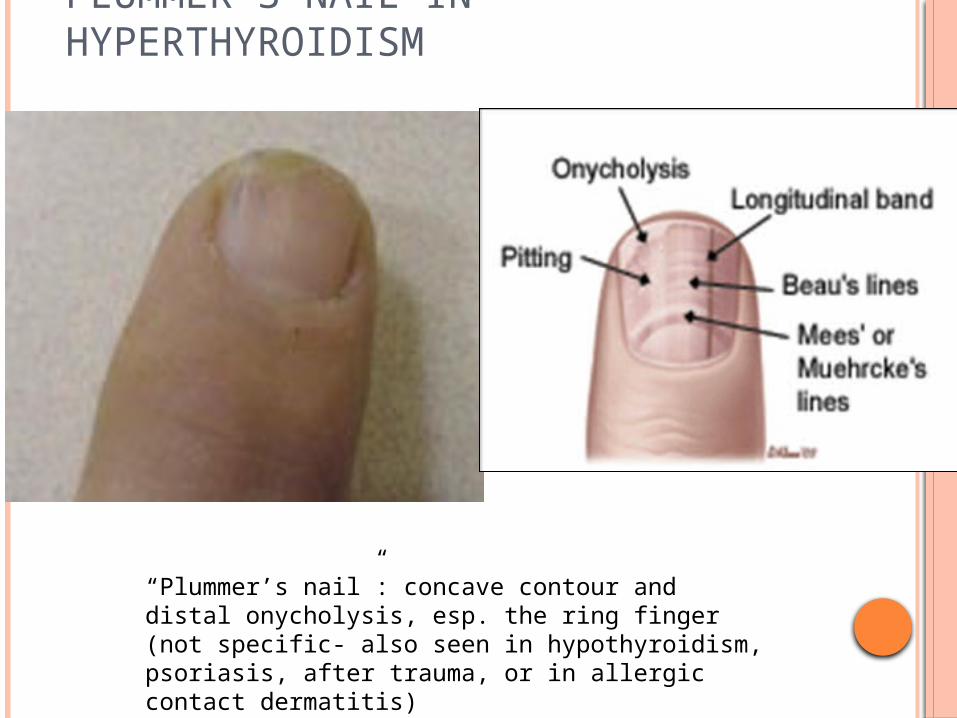
PLUMMER’S NAIL IN HYPERTHYROIDISM
“Plummer’s nail”: concave contour and distal onycholysis, esp. the ring finger (not specific- also seen in hypothyroidism, psoriasis, after trauma, or in allergic contact dermatitis)

SCLEROMYXEDEMA IN HYPERTHYROIDISM
Numerous firm white, yellow, or pink papules on face, trunk, axillae, and extremities Lesions result from accumulation of
hyaluronic acid in the dermis, accompanied by large fibrocytes
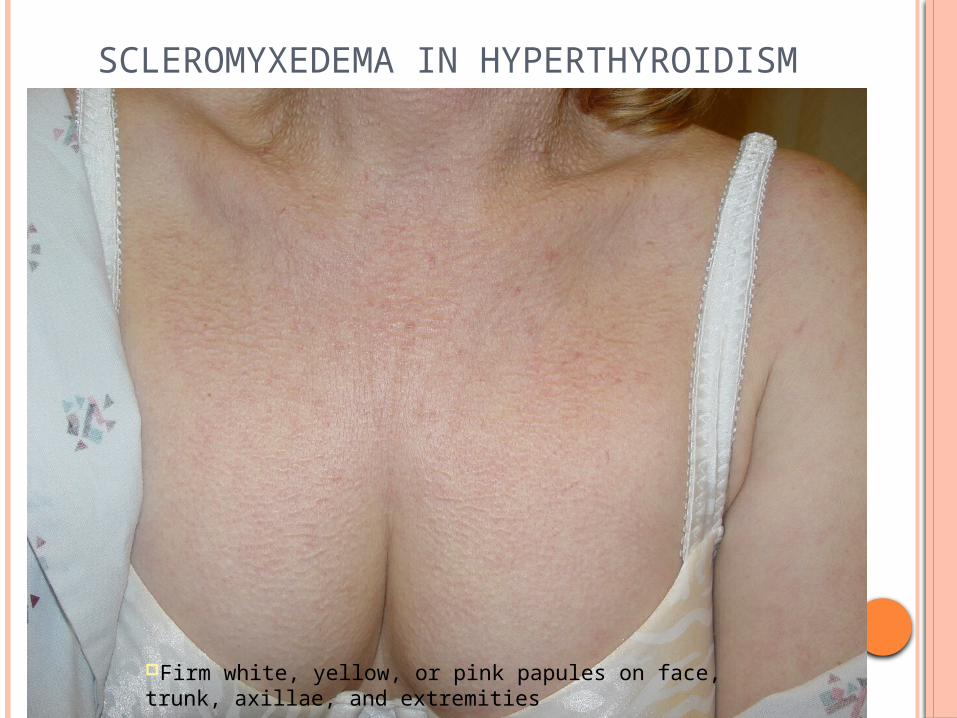
SCLEROMYXEDEMA IN HYPERTHYROIDISM
Firm white, yellow, or pink papules on face, trunk, axillae, and extremities

SCLEROMYXEDEMA IN HYPERTHYROIDISM
Firm white, yellow, or pink papules on face, trunk, axillae, and extremities

GRAVES’ DERMOPATHY
Pretibial myxedema (0.5-4% of patients)
Late manifestation, accompanied by ophthalmopathy in 99%. Presentation varies from “peau
d’orange” appearance to extensive infiltration.
Most often, bilateral, asymmetric, raised, firm plaques or nodules varying from pink to brown, sometimes with woody induration
Can appear anywhere (arms, shoulders, head).
Histologically, the process involves dermal accumalation of hyaluronic acid.
Pathogenesis :pretibial fibroblasts are the target for antithyroid antibodies
T cells may be interacting with a dermal antigen similar to a thyroid autoantigen, with cytokines subsequently activating fibroblasts to secrete hyalouronic acid.
Can treat with topical steroids, intralesional steroids, IV pulse steroids, or IVIG
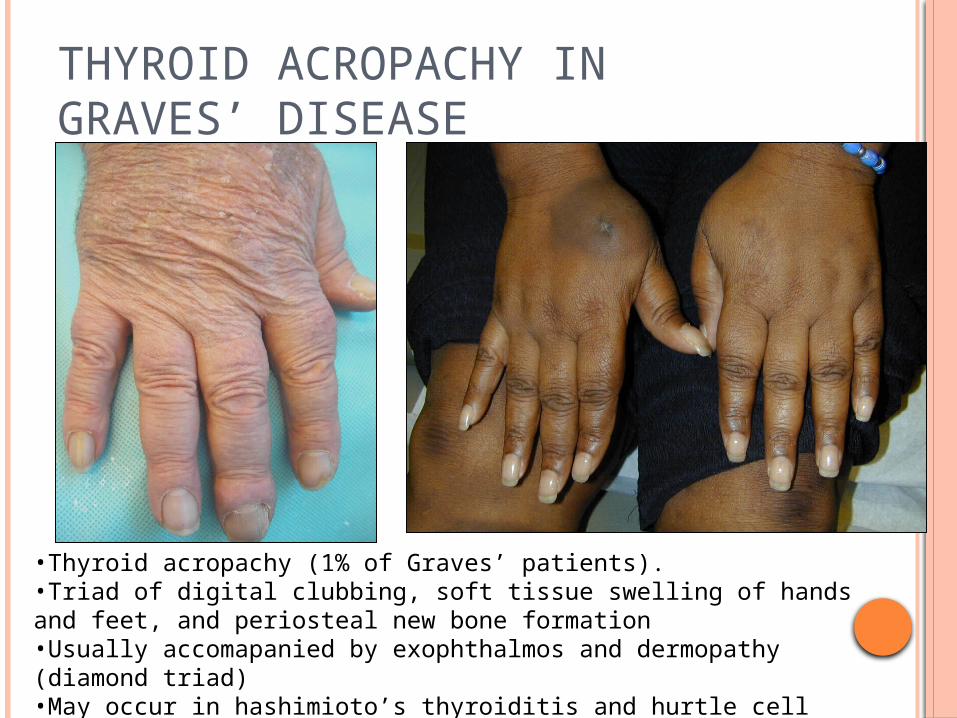
THYROID ACROPACHY IN GRAVES’ DISEASE
•Thyroid acropachy (1% of Graves’ patients).•Triad of digital clubbing, soft tissue swelling of hands and feet, and periosteal new bone formation•Usually accomapanied by exophthalmos and dermopathy (diamond triad)•May occur in hashimioto’s thyroiditis and hurtle cell adenocarcinoma.

HYPOTHYROIDISM AND THE SKIN
Skin is cool, dry, and pale. Pallor results from cutaneous
vasoconstriction and increased deposition of water and mucopolysaccharides in the dermis, which alter the refraction of light
Hypohydrosis may lead to palmoplantar keratoderma (possibly along with reduced epidermal steroid synthesis)
Carotenemia (from decreased hepatic conversion of beta carotene to Vit A) gives skin yellowish hue (palms, soles, +nasolabial folds)
Hair: dry, brittle, coarse; partial alopecia Loss of hair from lateral 1/3 of eyebrows
(lateral superciliary madarosis) Hertog’s sign
Hair growth slows down, the proportion of telogen hair is increased.
These changes normalise with normalization of thyroid hormone levels.

HYPOTHYROIDISM AND THE SKIN Nails are brittle, grow slowly, purpura Easy bruising Wound healing is impaired. Diminished levels of clotting factors may manifest
as purpura.

HYPOTHYROIDISM FACIES WITH GENERALIZED MYXEDEMA
Generalized myxedema Characteristic skin sign
Occurs as a result of deposition of PAS-positive dermal acid mucopolysaccharides (esp. hyaluronic acid and chondroitin sulfate) in the skin
Skin is non-pitting, with a firm waxy appearance
Characteristic facies: swollen lips, broad nose, macroglossia, and puffy eyelids
Also apparent on the dorsa of hands and feet and in the supraclavicular fossa
Carpal tunnel syndrome and facila nerve palsy may occur owing to nerve entrapment

CONGENITAL HYPOTHYROIDISM (CRETINISM)
Myxodema Yellowing (carotenemia or prolonged jaundice) Pronounced clavicular fat pad Coarse, dry, brittle hair with patchy alopecia Persistent, long, lanugo hair on the upper back,
shoulders, and extremities Hypothermia Reflex peripheral vasoconstriction may
accentuate cutis marmorata Poor nail growth Delayed eruption of deciduous teeth Retardation of mental and physical development Delayed milestones

Thyroid replacement therapy rapidly reverses many of the cutaneous features of hypothyroidism, with gradual disappeaarance of excessive dermal mucopolysaccharides.

ASSOCIATION BETWEEN CUTANEOUS AND THYROID DISEASE
Vitiligo (higher levels of antithyroid
peroxidase, antithyroid microsome, anti-TSH) Connective tissue diseases
Dermatomyositis, SLE, scleroderma, polymyositis, sjogren’s syndrome.
Generalised granuloma annulare, reticular erythematous mucinosis Chronic urticaria Melasma Chronic mucocutaneous
candidiasis MEN syndromes
Patients with idiopathic chronic urticaria and/or angiodema should therefore be screened for thyroid autoimmunity

ASSOCIATION BETWEEN CUTANEOUS AND THYROID DISEASE CONTD.
ALOPECIA AREATA
Rapid onset of total hair loss in a sharply defined, usually round, area
Regrowth begins in 1 to 3 months and may be followed by loss in the same or other areas

ASSOCIATION BETWEEN CUTANEOUS AND THYROID DISEASE CONTD.
Pemphigus foliaceus
Herpes gestationisBullous pemphigoidDermatitis herpetiformis
Pemphigus vulgaris

ADRENAL DISEASE
Addison’s diseaseHypercortism

ADRENAL INSUFFICIENCY
Increased stimulation of melanocortin-2 receptor by ACTH itself
Pigmentation is maximal over photoexposed areas, mucuos membranes, palmar creases, areas subject to friction, genitalia, areola, axillae, perineum as well as in scars.
Nails-longitudinal melanonychia

HYPERCORTISM
Truncal obesity Buffalo hump Moon facies Slender limbs Cutaneous atrophy and
telangiectasias Fragility with purpura Poor wound healing Acneform eruptions Hirsuitism Cigarette paper like
wrinkling of skin on dorsum of hands(liddle’s sign)
Livid, purplish straie on abdomen, breasts, proximal part of limbs

RENAL DISEASES Signs of ESRD Signs associated with dialysis Signs in renal transplant patients

CUTANEOUS MANIFESTATIONS OF UREMIA Xerosis Pruritus Pigmentary alteration Nail Changes Hair Changes Acquired perforating disorder Bullous disease of dialysis Calcinosis cutis (metastatic) Calciphylaxis Nephrogenic systemic fibrosis

XEROSIS Most common cutaneous abnormality
Is predominantly seen over the extensor surfaces of the forearms, legs and thighs.
The abdomen and chest may show fine scaling Hypervitaminosis A, reduction in size of eccrine sweat glands,
high dose diuretic regimens are some of the causes of xerosis

UREMIC PRURITUS Incidence is 50-90% Usually on forarms, back
Cutaneous manifestations of
pruritus include excoriations,
prurigo nodularis and lichen
simplex chronicus
Decreased transepidermal elimination of pruritogenic factors
Hyperparathyroidism Hypercalcemia Hyperphosphatemia Elevated histamine levels
Topical Moisturizing creams Capsaicino Physical treatments UVB light parathyroidectomyo Systemic medications Sedating Antihistamines Cholestyramine Alternative strategies Acupuncture homeopathy

PIGMENTARY CHANGES PURPURA/ECHHYMOSIS
Pallor – Anemia Yellow hue – Carotenoids and
nitrogenous pigments (urochromes) in the skin.
Brown-black Hyperpigmentation - Sunexposed areas can be attributed to retention of
chromogens and deposition of melanin in the basal layer and superficial dermis due to failure of kidney to excrete beta-melanocyte stimulating hormone
Sunscreens, sun avoidance measures and clothing are advised for these pigmentary changes.
Defects in primary hemostasis like increased vascular fragility
Abnormal platelet function Use of heparin during
dialysis are the main causes of abnormal bleeding in these patients
Dialysis treatment partially corrects these changes
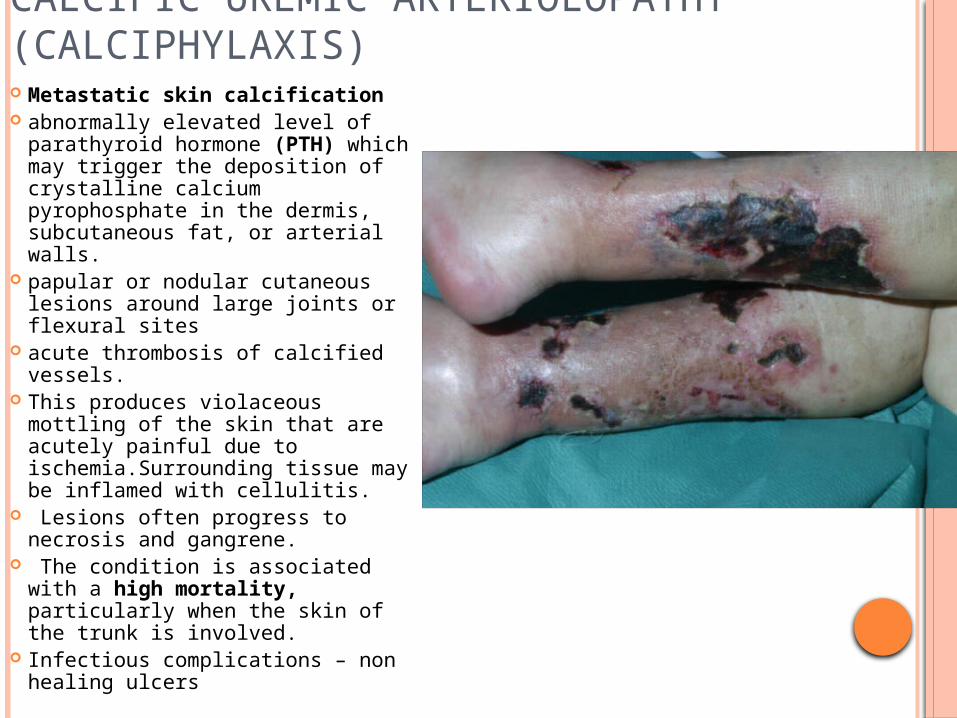
CALCIFIC UREMIC ARTERIOLOPATHY (CALCIPHYLAXIS) Metastatic skin calcification abnormally elevated level of
parathyroid hormone (PTH) which may trigger the deposition of crystalline calcium pyrophosphate in the dermis, subcutaneous fat, or arterial walls.
papular or nodular cutaneous lesions around large joints or flexural sites
acute thrombosis of calcified vessels.
This produces violaceous mottling of the skin that are acutely painful due to ischemia.Surrounding tissue may be inflamed with cellulitis.
Lesions often progress to necrosis and gangrene.
The condition is associated with a high mortality, particularly when the skin of the trunk is involved.
Infectious complications – non healing ulcers

ACQUIRED PERFORATING DERMATOSIS ( APD ) Hyperpigmented papules,
up to 1 cm in diameter, with a central keratinous plug in patients of CRF.
The exclusive feature of the perforating disorders is the trans-epidermal elimination of altered dermal substances.
The changes are significantly more prevalent in diabetic patients
Excessive scratching + diabetic vasculopathy - dermal necrosis- eliminated through the epidermis
The extensor surfaces of the limbs are more commonly affected but the trunk and face may be involved.
oDistinct from primary perforating disordersKyrle’s diseaseElastosis Perforans serpiginosaPerforating folliculitisReactive perforating collagenosis
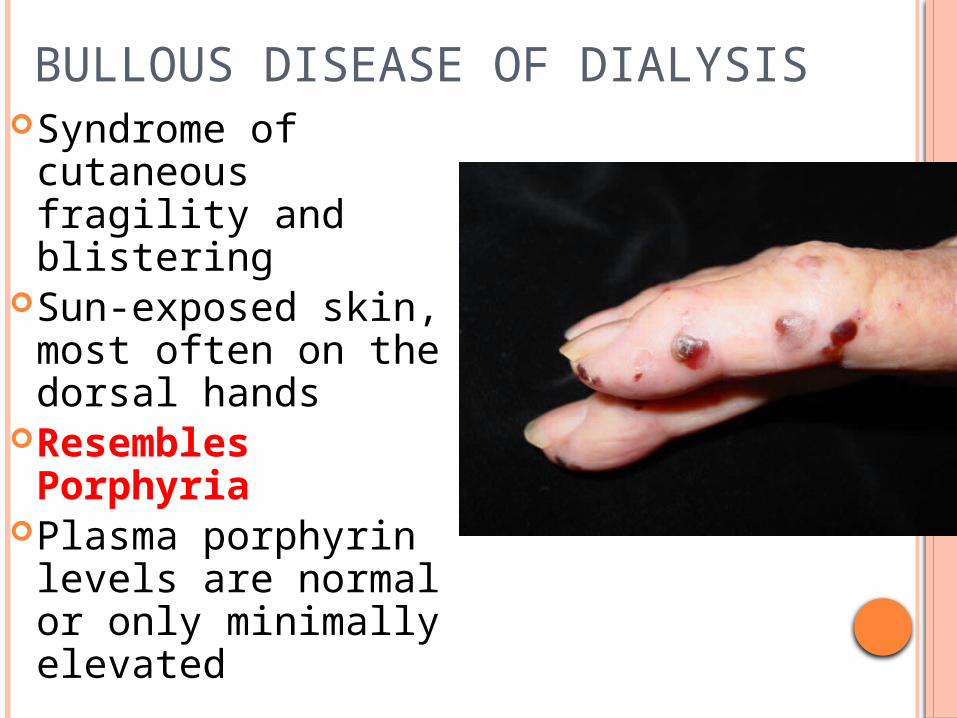
BULLOUS DISEASE OF DIALYSIS
Syndrome of cutaneous fragility and blistering
Sun-exposed skin, most often on the dorsal hands
Resembles Porphyria
Plasma porphyrin levels are normal or only minimally elevated

NEPHROGENIC FIBROSING DERMOPATHY (NFD)
Scleroderma like fibrosing skin condition
Typically, symmetrical skin plaques with a peau d’orange surface and advancing ameboid edges develop on limbs and trunk sparing the head and neck.
Nodules and contractures can be seen in patients with disease of long duration.
Skin biopsy-marked fibrosis

UREMIC FROST Was a frequent in the pre-
dialysis era blood urea nitrogen level of
more than 250-300 mg/dl. The concentration of urea
in sweat is increased and, after evaporation, there is a deposition of urea crystals on the skin surface.
The frost consists of a white or yellowish coating of urea crystals on the beard area and other parts of the face, neck and on the trunk.

NAIL CHANGES Lindsay's nails (half and half nails,
prevalence 30-50 %) Others
Koilonychia Subungual hyperkeratosis Onycholysis Mees’ lines Muehrcke’s lines Splinter hemorrhages Beaus lines
Proximal half opaque white
Normal to red brown distal half


Yellow nail syndrome (YNS) is triad of yellow nails, lymphedema, and respiratory tract involvement

HAIR ABNORMALITIES
Sparse body hair and diffuse alopecia with dry, lusterless hair
Decreased secretion of sebumChronic telogen effluvium Drugs – Heparin / Statins /
Antihypertensives

CUTANEOUS MANIFESTATIONS IN PTS ON DIALYSIS
Diffuse hyperpigmentation
Accelerated cutaneous aging
Actinic elastosis Excessive wrinkling of neck(
cutis rhomboidalis nuchae) Telangiectasiaso Skin infections common
DERMATOLOGIC DISORDERS ASSOCIATED WITH RENAL TRANSPLANTATION.
Drugs – Steroids, ImmunosuppresantsInfections Severe herpes zoster Viral warts and condylomata accuminata are more common
later Pityriasis versicolor commonest fungal infection Candidal infections Malignancies Kaposi sarcoma- oral cavity, limbs, trunk; associated with edema SCC> BCC Younger age, multiple, extracephalic, HP features of HPV
infection, spindle cell morphology is more common
Transplant patients should be counselled on minimizing UV light exposure, regular sunscreen use, self screening for skin lesions
LIVER DISEASE
Chronic liver disease
Hepatitis B,C
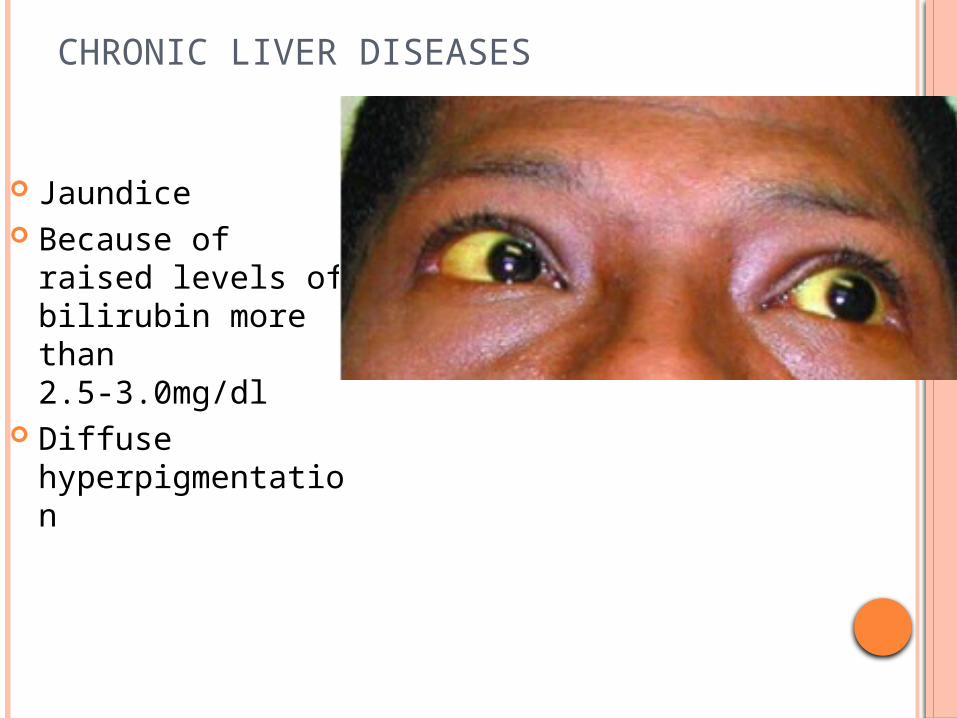
CHRONIC LIVER DISEASES
Jaundice Because of raised
levels of bilirubin more than 2.5-3.0mg/dl
Diffuse hyperpigmentation

SPIDER ANGIOMAS/ SPIDER NEVUS/NEVUS ARANEUS Pinhead to upto 2mm Mostly on skin drained by
superior vena cava Central arteriole visible as a red,
flat or slightly elevated point surrounded by multiple, small and tortuous radiating capillaries
Commoner in alcoholic cirrhosis Presence may indicate an
increased risk of bleeding from oesophageal varices
Abundant cutaneous spider angiomata –clinical marker of hepatopulmonary syndrome, where circulatory and gas-exchange abnormalities in lungs occur secondary to advanced CLD.

CHRONIC LIVER DISEASES Palmar erythema Exaggerated mottling or a well
defined hypothenar erythema that later spreads to fingers and rest of the palm
gynaecomastia(Because of hyperestrogenemia)
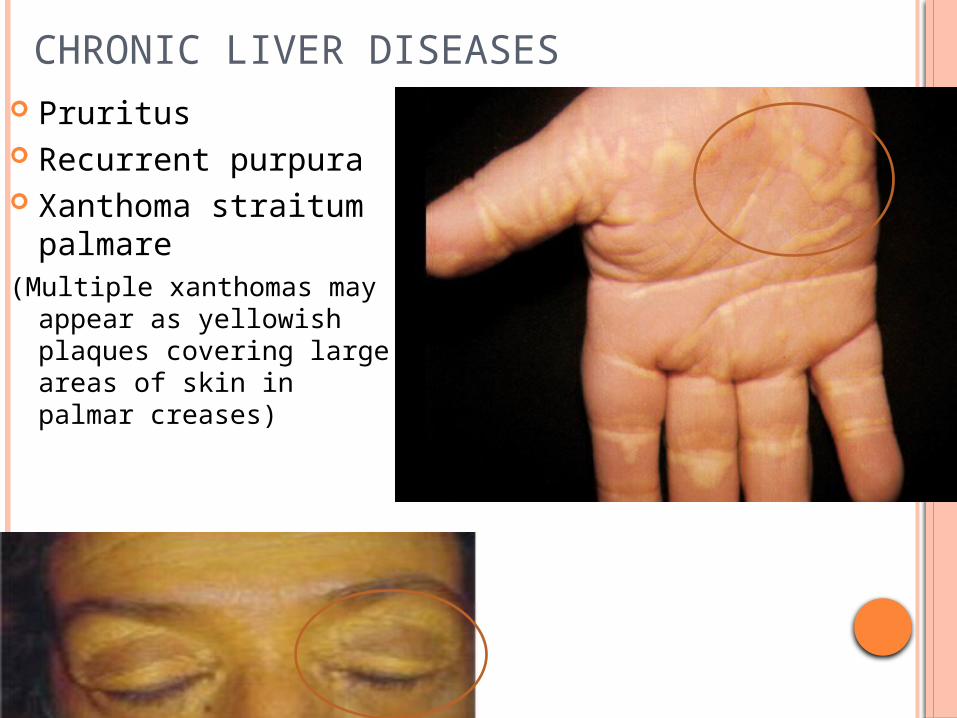
CHRONIC LIVER DISEASES Pruritus Recurrent purpura Xanthoma straitum
palmare(Multiple xanthomas may
appear as yellowish plaques covering large areas of skin in palmar creases)

CHRONIC LIVER DISEASES
Ascites leads to striae distensae
dupuytren's contracture

CHRONIC LIVER DISEASES
Clubbing Longitudinal ridging Thickening Brittleness Total leuconychia terry’s nails (whitening of the
entire nail plate except for a narrow pink band distally)
Muehrcke’s nails(multiple parallel
transverse white bands Terry’s nails
Muehrcke’s nails
clubbing

HEPATITIS C
Porphyria Cutanea Tarda
Lichen Planus
Necrolytic acral erythema

PORPHYRIA CUTANEA TARDA Vesicles and bullae
on sun-exposed areas, scarring with milia
Hypertrichosis Fragile skin with
sclerodermoid changes
Anti HCV antibodies found in upto 2/3rd of cases of these patients
HCV serology should be a part of routine investigative work up in patients with PCT
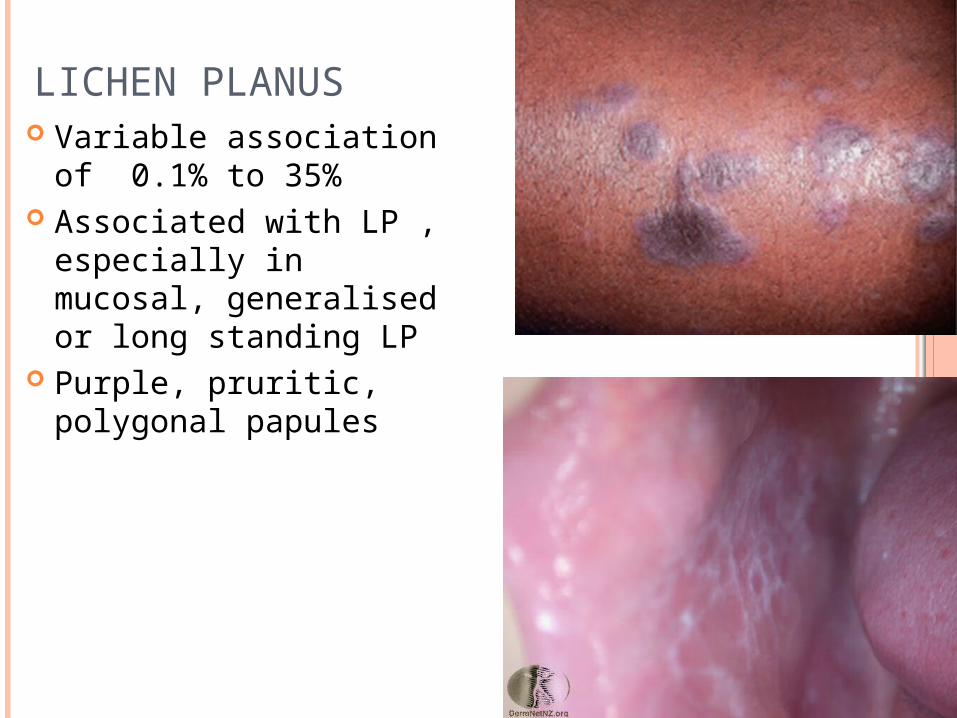
LICHEN PLANUS Variable association of
0.1% to 35% Associated with LP ,
especially in mucosal, generalised or long standing LP
Purple, pruritic, polygonal papules

NECROLYTIC ACRAL ERYTHEMA
Starts as erythematous papules and sometimes blisters that coalesce into well-circumscribed dusky areas with scaling and erosions.
Hyperkeratotic surface develops in older lesions
Mc site- drsal surface of feet-great toes
Spares periorificial areas-d/f with other necrolytic erythemas such as necrolytic migratory erythemas and zinc deficiency

HEPATITIS B About 30% may
have Urticaria or present a serum sickness like picture (because of circulating immune complexes)
Associated with 5-7% cases of Polyarteritis nodosa
Classical PAN Renal vasculitis
present ANCA negative

SYSTEMIC LUPUS ERYTHEMATOSUS

SYSTEMIC LUPUS ERYTHEMATOSUS
Malar erythema Discoid plaques or psoriasiform
erythroderma Photosensitivity, alopecia and mucosal ulcers Raynaud’s phenomenon Periungual erythema

MALAR ERYTHEMA
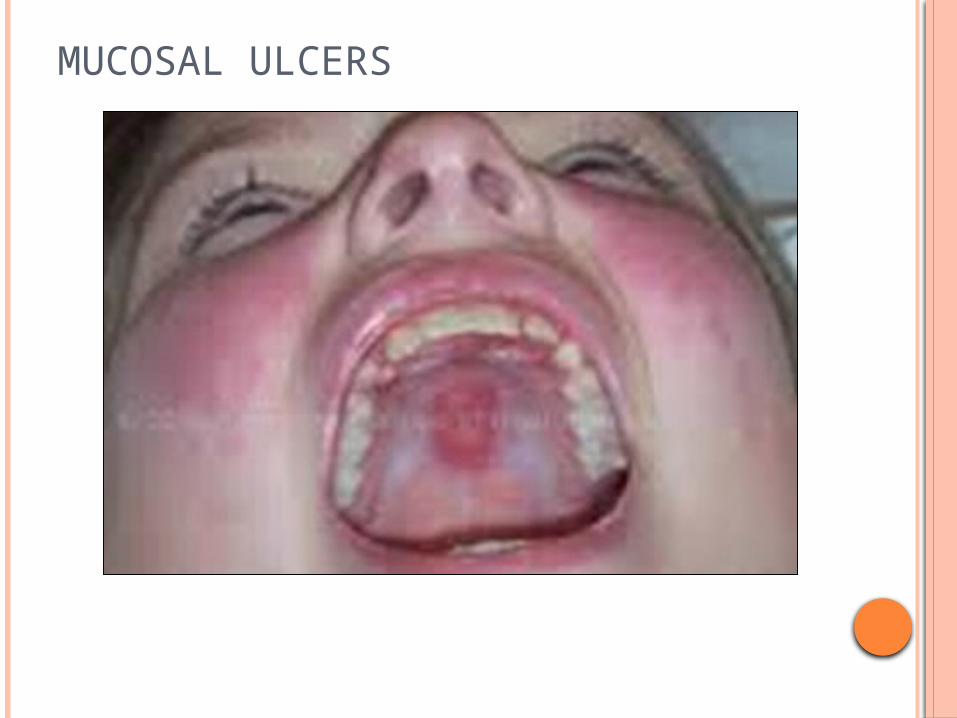
MUCOSAL ULCERS

ALOPECIA

ANNULAR PSORIASIFORM MACULES AND PATCHES

ANNULAR PSORIASIFORM MACULES AND PATCHES

ANNULAR PSORIASIFORM MACULES AND PATCHES

Periungual erythema
DERMATOMYOSITIS

HELIOTROPE RASH IN DERMATOMYOSITIS
Heliotrope rash (violaceous erythema) of periorbital skin

DERMATOMYOSITIS
Shawl sign

DERMATOMYOSITIS-HOLSTER SIGN

SYSTEMIC SCLEROSIS

Major criteria:
Proximal Scleroderma : Symmetrical thickening, tightening, induration of skin of
digits and
dorsal hands; may affect entire extremity and involve face
and torso Minor criteria: 1. Sclerodactyly: skin changes (above) limited to digits 2. Digital pitted scars or loss of finger pad soft tissue 3. bibasilar pulmonary fibrosis
Diagnosis requires 1 major or 2 minor criteria
CRITERIA FOR DIAGNOSIS: SYSTEMIC SCLEROSIS

Sclerodactyly
SCLERODACTLY

SCLERODERMATOUS PLAQUES
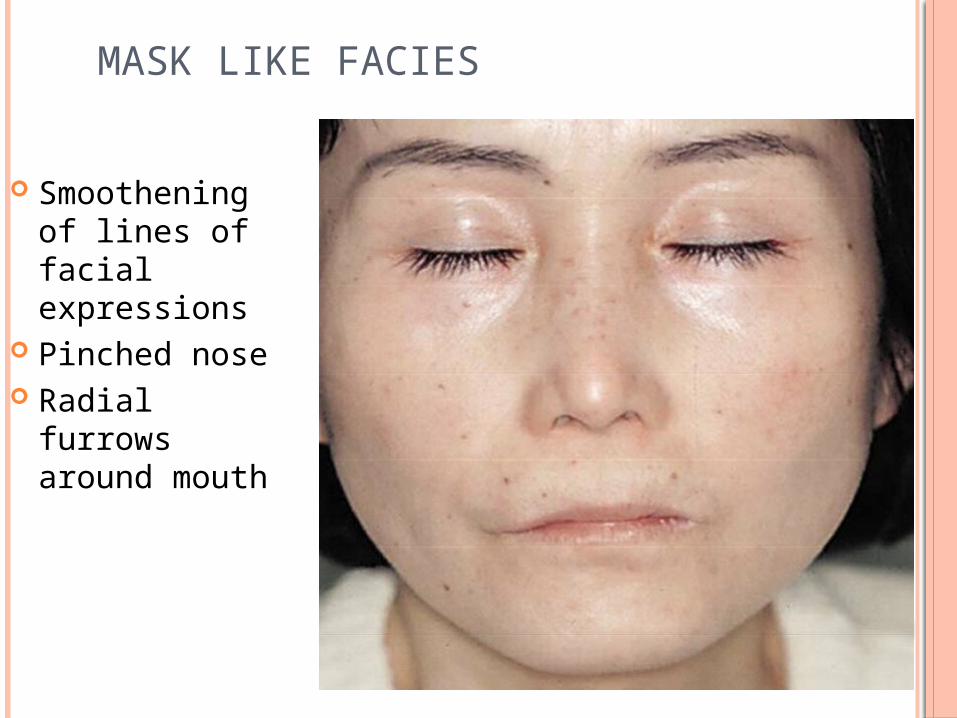
bird-like facies MASK LIKE FACIES
Smoothening of lines of facial expressions
Pinched nose Radial furrows
around mouth

Periungual erythema and hemorrhage NAIL FOLD CHANGES
Periungual erythema and hemorrhage

GASTROINTESTINAL DISEASES

HENOCH-SCHÖNLEIN PURPURA
vasculitis with arthritis, abdominal pain, and
hematuria
mainly affects children
often follows streptococcal infection
In the skin, the disease causes palpable purpura
(small hemorrhages)
chronic kidney disease- loss of small amounts of
blood and protein in the urine

Henoch-Schönlein purpura

Henoch-Schönlein purpura
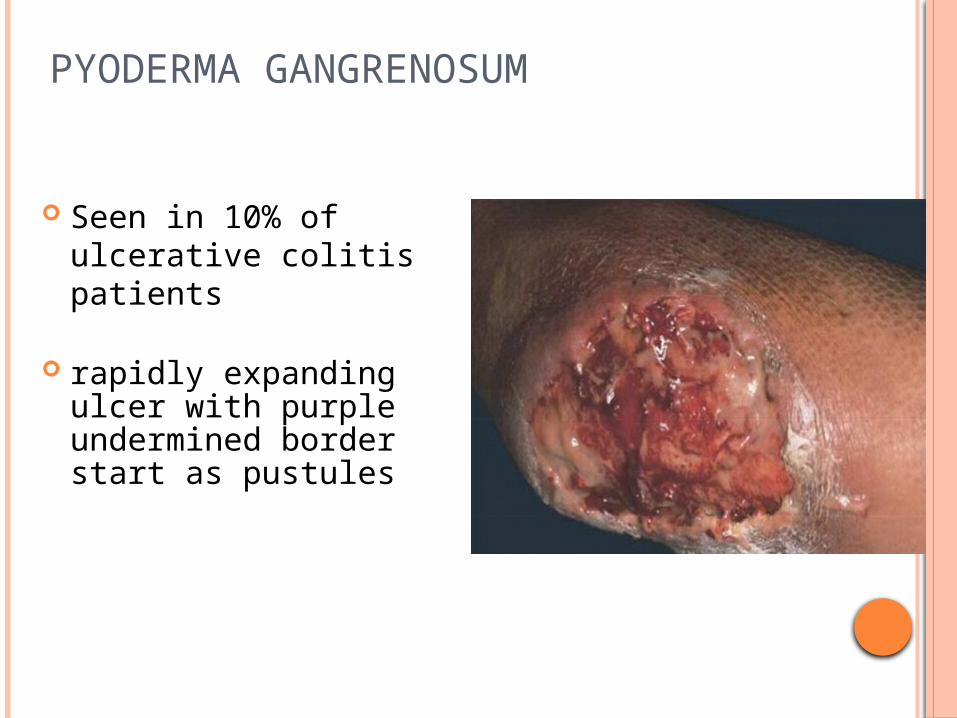
PYODERMA GANGRENOSUM
Seen in 10% of ulcerative colitis patients
rapidly expanding ulcer with purple undermined border start as pustules

SWEET’S SYNDROME
Erythematous tender papules,nodules and plaques with marked lesional edema resulting in pseudovesiculation
May occur in pts with inflammatory bowel disease, UC
CARDIAC DISEASES

CYANOSIS
Capillary concentration of reduced Hb is more than 4g/Dl.
Best observed in fulorescent lightening
Most prominent in areas with thin vascular surfaces
Oral mucosa Lips Earlobes Nail beds Palms and soles in children

CYANOSIS May be Central (decreased arterial oxygen saturation) Congenital heart disease Impaired pulmonary function Tongue is the most reliable site for detecting cyanosis. Peripheral (owing to poor blood flow) Cold exposure Peripheral vascular disease Congestive heart failure Polycytemia Oral mucosa is often spared in peripheral cyanosiso Mixed Pulmonary odema Cardiogenic shock

CLUBBING
Increase in the angle between the proximal nail fold and the nail plate (Lovibond’s angle)
Due to connective tissue proliferation between the nail matrix and the underlying distal phalanx
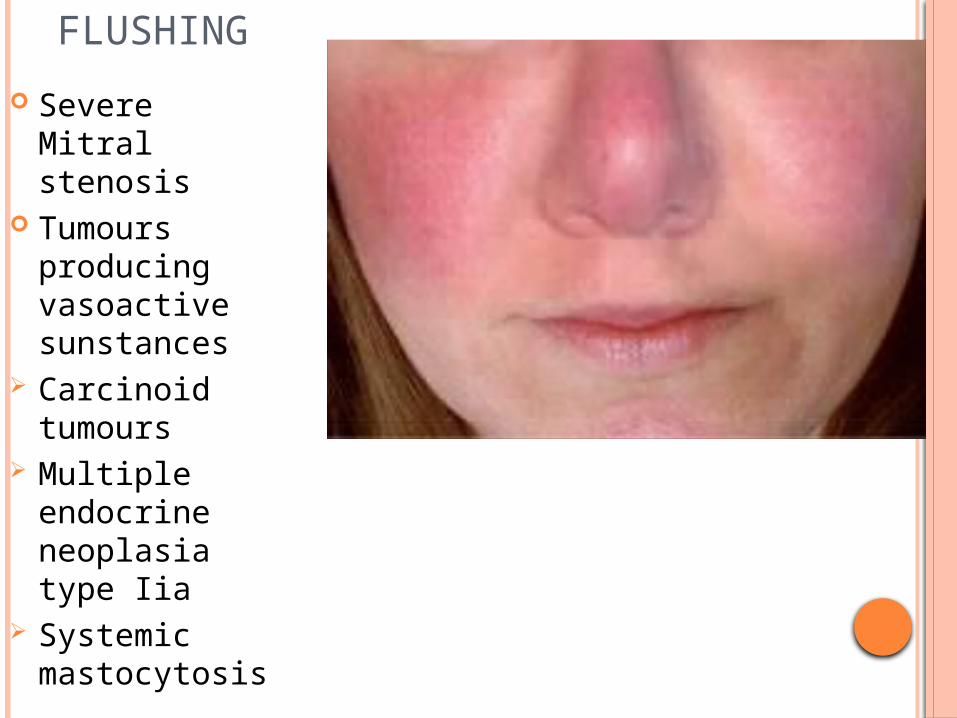
FLUSHING
Severe Mitral stenosis
Tumours producing vasoactive sunstances
Carcinoid tumours
Multiple endocrine neoplasia type Iia
Systemic mastocytosis

CUTANEOUS ASSOCIATIONS OF CORONARY ARTERY DISEASE
Xanthomas: localized lipid infiltrates in the dermis or tendons.
Indicative of abnormal lipid profile and risk of coronary artery disease

INFECTIVE ENDOCARDITIS
Subungual splinter hemorrhages
1-2mm brown streaks under the finger/toe nails
Proximal appearance has more diagnostic value
Petechiae Osler’s nodes tender purpuric nodules on
the finger pads and toes) Janeway lesions nontender purpuric macules
of the palms and soles

RHEUMATIC FEVER Subcutaneous
nodules: Extensor aspect of elbows and
knees Exclusively seen in pts of
rheumatic carditis
Erythema marginatum Seen in 10% pts of
rheumatic fever Dull red ,flat or palpable,
discrete or confluent, annular lesions on the trunk, esp the abdomen and proximal parts of the extremities
CUTANEOUS SIGNS INDICATIVE OF INTERNAL DISEASES
oErythema nodosumoAcanthosis nigricansoPyoderma gangrenosumoAcquired ichthyosisoGeneralised pruritus without an eruption

Erythema Nodosum
Due to panniculitis
(inflammation of the
subcutaneous fat)
deep, firm, and tender
reddish-blue nodules, 1-5 cm
diameter
Most commonly at calves
and shins

Causes of Erythema Nodosum
Idiopathic
Bacterial
Fungal
Viral
Drugs
Systemic diseases
About 20% of cases
Streptococci, TB, leprosy, Yersinia, Mycoplasma, Rickettsia
Coccidioidomycosis
Cat-scratch fever
Sulphonamides, oral contraceptives
Inflammatory bowel disease, sarcoidosis, Behçet’s disease, malignancy (rare)
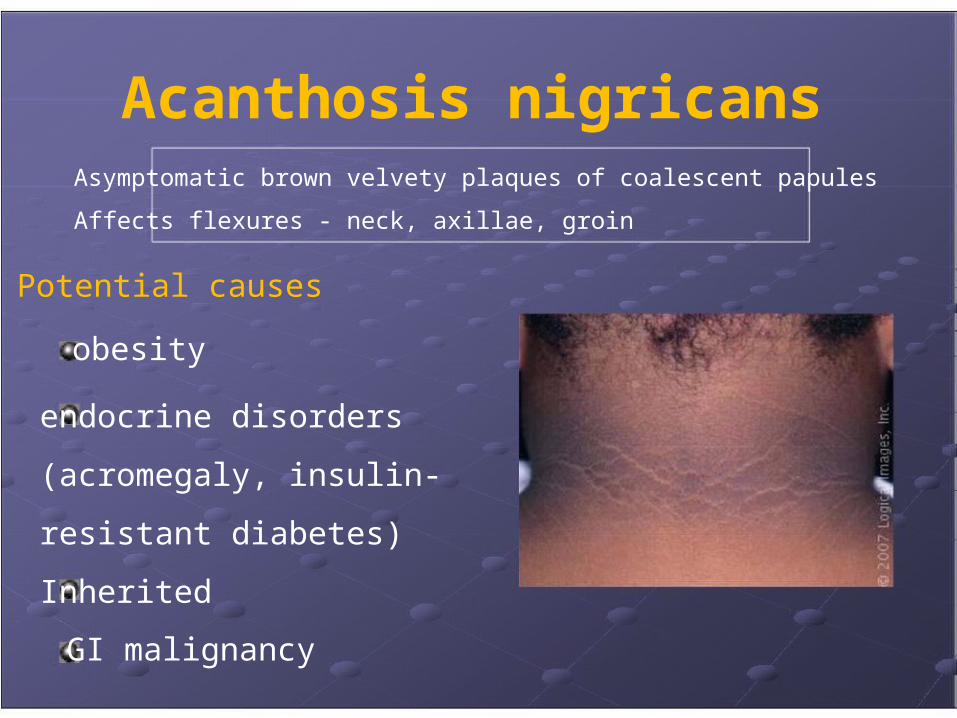
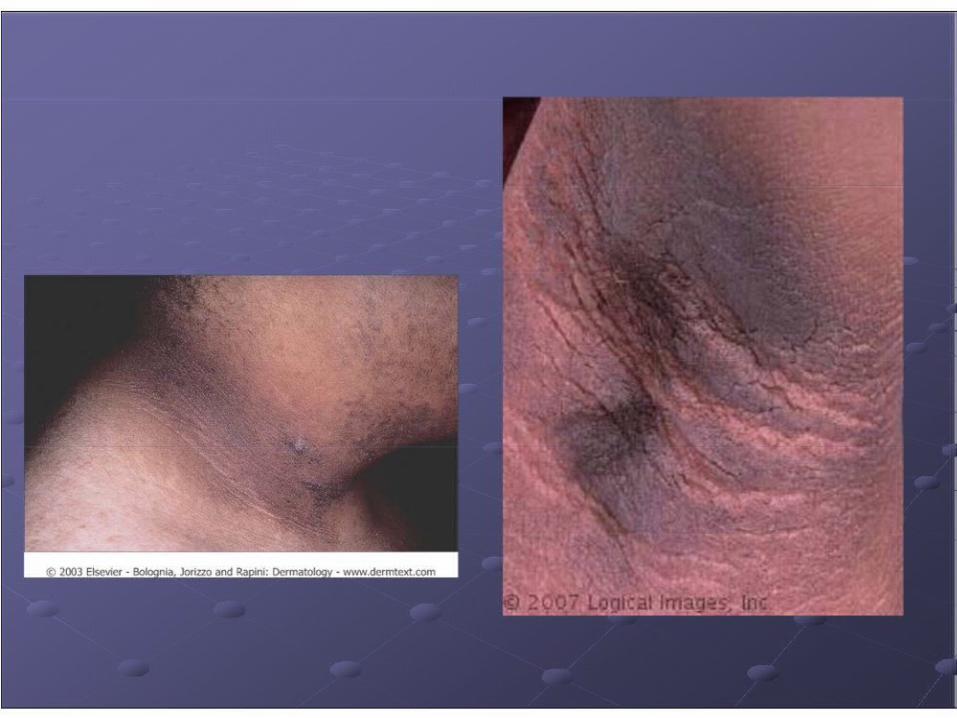
Acanthosis nigricans Asymptomatic brown velvety plaques of coalescent papules
Affects flexures - neck, axillae, groin
Potential causes
obesity
endocrine disorders
(acromegaly, insulin-
resistant diabetes)
Inherited
GI malignancy
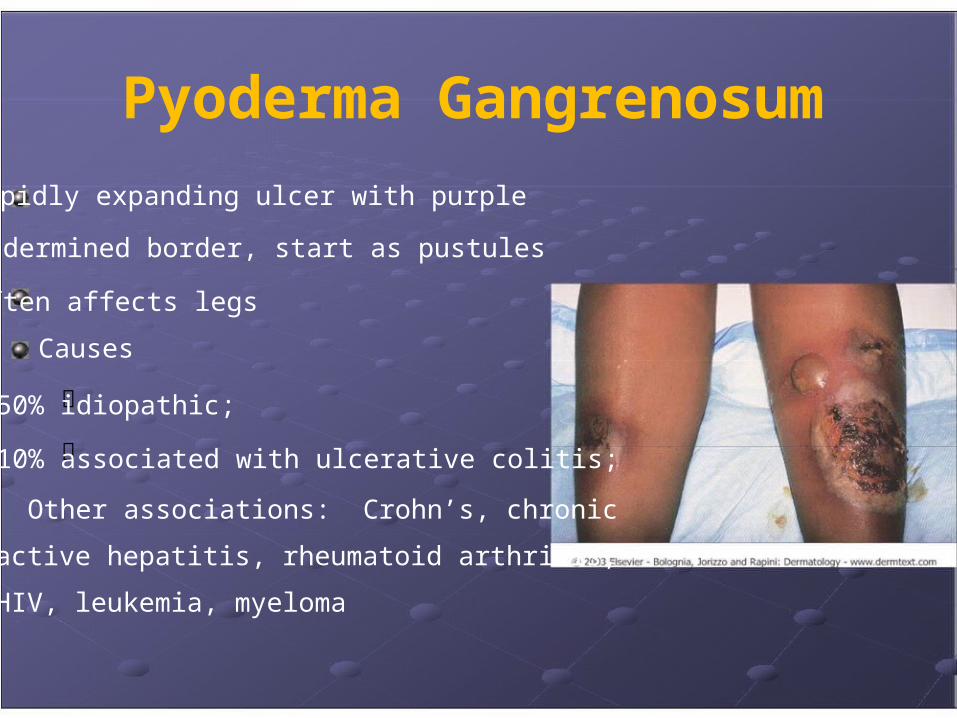
Pyoderma Gangrenosum
rapidly expanding ulcer with purple
undermined border, start as pustules
Often affects legs
Causes
50% idiopathic;
10% associated with ulcerative colitis;
Other associations: Crohn’s, chronic
active hepatitis, rheumatoid arthritis,
HIV, leukemia, myeloma

ACQUIRED ICHTHYOSIS If develops in
adulthood, consider:
underlying
malignancy (e.g.
Hodgkin’s disease),
essential fatty acid
deficiency (e.g. due to
malabsorption from
intestinal by-pass or
from lipid lowering
drugs)

Generalized pruritus without an eruption
Causes: Idiopathic (‘senile’)
Iron deficiency
Liver disease
Malignancy (e.g. Hodgkin’s lymphoma)
Neurological disorders
Polycythemia
Renal failure
Thyroid dysfunction

THANK YOU