
Current workup and therapy of infantile hemangiomas
12
Current workup and therapy of infantile hemangiomas Francine Blei, MD, MBA ⁎ , Ascanio Guarini Vascular Birthmark Institute of New York, Mt. Sinai Roosevelt Hospital, New York, NY Abstract Many practitioners assume every vascular lesion is a hemangioma; then tell parents not to worry, because hemangiomas “go away” after they grow. In fact, over the past three decades, advances in the stratification of vascular lesions, identification of clinical associations and syndromic vascular anomalies, and the discovery of germline and somatic mutations accompanying certain vascular anomalies have broadened our understanding. Concomitantly, the evaluation and management of vascular anomalies have become more sophisticated, and a laissez-faire approach is often inadequate. This paper focuses on hemangiomas of infancy and is divided into two sections, Evaluation and Management, both sections including updated references to clinical and basic research and reviews supporting the discussion. © 2014 Elsevier Inc. All rights reserved. Introduction Before evaluating a patient with a vascular anomaly, it is imperative to make the appropriate diagnosis. Practitioners often use the word hemangioma loosely to describe any benign vascular lesion. A recent study using the search term “hemangioma” in PubMed showed that in 1 year (2009) more than 70% of 320 publications incorrectly used this diagnosis. 1 The accepted categorization of vascular anom- alies originally proposed by Mulliken and Glowacki 2 and later expanded by the International Society for the Study of Vascular Anomalies (ISSVA) 3 is shown in Table 1. Of note, a more comprehensive updated ISSVA classification was approved in April 2014 (issva.org). This paper focuses on the diagnoses listed in bold type in Table 1. These include infantile hemangiomas (hemangi- omas of infancy), which follow a typical pattern of postnatal growth, stabilization, then spontaneous involution, and the more recently recognized subtypes of hemangiomas: congenital hemangiomas that are present prenatally and obvious at birth, including RICH (Rapidly Involuting Congenital Hemangioma), which spontaneously improve, and NICH (Non- Involuting Congenital Hemangioma), which do not change over time. Figure 1 summarizes the typical growth curves of the three subtypes of hemangioma. RICH lesions are characterized by a circumferential halo. An additional feature distinguishing “typical hemangiomas” from congenital hemangiomas is glucose transporter 1 (GLUT-1) tissues staining. Typical hemangiomas stain positive during all growth phases, whereas congenital hemangiomas are GLUT-1 negative. 4,5 Patients with RICH-type lesions may experience high flow–related issues pre- and postnatally, 6,7 demonstrate calcifications on ultra- sound, 8,9 and/or experience a transient, self-limited hemato- logic profile similar to Kasabach-Merritt phenomenon. 10–12 After natural involution (often by 14 months of age), RICH lesions may result in redundant or atrophic skin. 10 Patients with high-flow, functional or hematologic complications may require intervention. 10,11,13 Although clinically distinct, infantile hemangioma, RICH, and NICH are thought to represent a spectrum; moreover, there are cases where patients have both infantile hemangioma and RICH or NICH, and those with RICH lesions that transformed to NICH. 14 Figures 2–10 include images of patients with the various types of hemangiomas at different stages. 15,16 ⁎ Corresponding author. Tel.: +1 212 523 8931; fax: +1 212 636 3979. E-mail address: [email protected] (F. Blei). http://dx.doi.org/10.1016/j.clindermatol.2014.02.001 0738-081X/© 2014 Elsevier Inc. All rights reserved. Clinics in Dermatology (2014) 32, 459–470
Transcript of Current workup and therapy of infantile hemangiomas

Clinics in Dermatology (2014) 32, 459–470
Current workup and therapy ofinfantile hemangiomas
Francine Blei, MD, MBA⁎, Ascanio GuariniVascular Birthmark Institute of New York, Mt. Sinai Roosevelt Hospital, New York, NY
Abstract Many practitioners assume every vascular lesion is a hemangioma; then tell parents not toworry, because hemangiomas “go away” after they grow. In fact, over the past three decades, advancesin the stratification of vascular lesions, identification of clinical associations and syndromic vascularanomalies, and the discovery of germline and somatic mutations accompanying certain vascularanomalies have broadened our understanding. Concomitantly, the evaluation and management ofvascular anomalies have become more sophisticated, and a laissez-faire approach is often inadequate.This paper focuses on hemangiomas of infancy and is divided into two sections, Evaluation andManagement, both sections including updated references to clinical and basic research and reviewssupporting the discussion.© 2014 Elsevier Inc. All rights reserved.
Introduction
Before evaluating a patient with a vascular anomaly, it isimperative to make the appropriate diagnosis. Practitionersoften use the word hemangioma loosely to describe anybenign vascular lesion. A recent study using the search term“hemangioma” in PubMed showed that in 1 year (2009)more than 70% of 320 publications incorrectly used thisdiagnosis.1 The accepted categorization of vascular anom-alies originally proposed by Mulliken and Glowacki2 andlater expanded by the International Society for the Study ofVascular Anomalies (ISSVA)3 is shown in Table 1. Of note,a more comprehensive updated ISSVA classification wasapproved in April 2014 (issva.org).
This paper focuses on the diagnoses listed in bold type inTable 1. These include infantile hemangiomas (hemangi-omas of infancy), which follow a typical pattern of postnatalgrowth, stabilization, then spontaneous involution, and themore recently recognized subtypes of hemangiomas:congenital hemangiomas that are present prenatally andobvious at birth, including RICH (Rapidly Involuting
⁎ Corresponding author. Tel.: +1 212 523 8931; fax: +1 212 636 3979.E-mail address: [email protected] (F. Blei).
http://dx.doi.org/10.1016/j.clindermatol.2014.02.0010738-081X/© 2014 Elsevier Inc. All rights reserved.
Congenital Hemangioma), which spontaneously improve,and NICH (Non- Involuting Congenital Hemangioma),which do not change over time. Figure 1 summarizes thetypical growth curves of the three subtypes of hemangioma.
RICH lesions are characterized by a circumferential halo.An additional feature distinguishing “typical hemangiomas”from congenital hemangiomas is glucose transporter 1(GLUT-1) tissues staining. Typical hemangiomas stainpositive during all growth phases, whereas congenitalhemangiomas are GLUT-1 negative.4,5 Patients withRICH-type lesions may experience high flow–related issuespre- and postnatally,6,7 demonstrate calcifications on ultra-sound,8,9 and/or experience a transient, self-limited hemato-logic profile similar to Kasabach-Merritt phenomenon.10–12
After natural involution (often by 14 months of age), RICHlesions may result in redundant or atrophic skin.10 Patientswith high-flow, functional or hematologic complicationsmay require intervention.10,11,13 Although clinically distinct,infantile hemangioma, RICH, and NICH are thought torepresent a spectrum; moreover, there are cases wherepatients have both infantile hemangioma and RICH orNICH, and those with RICH lesions that transformed toNICH.14 Figures 2–10 include images of patients with thevarious types of hemangiomas at different stages.15,16
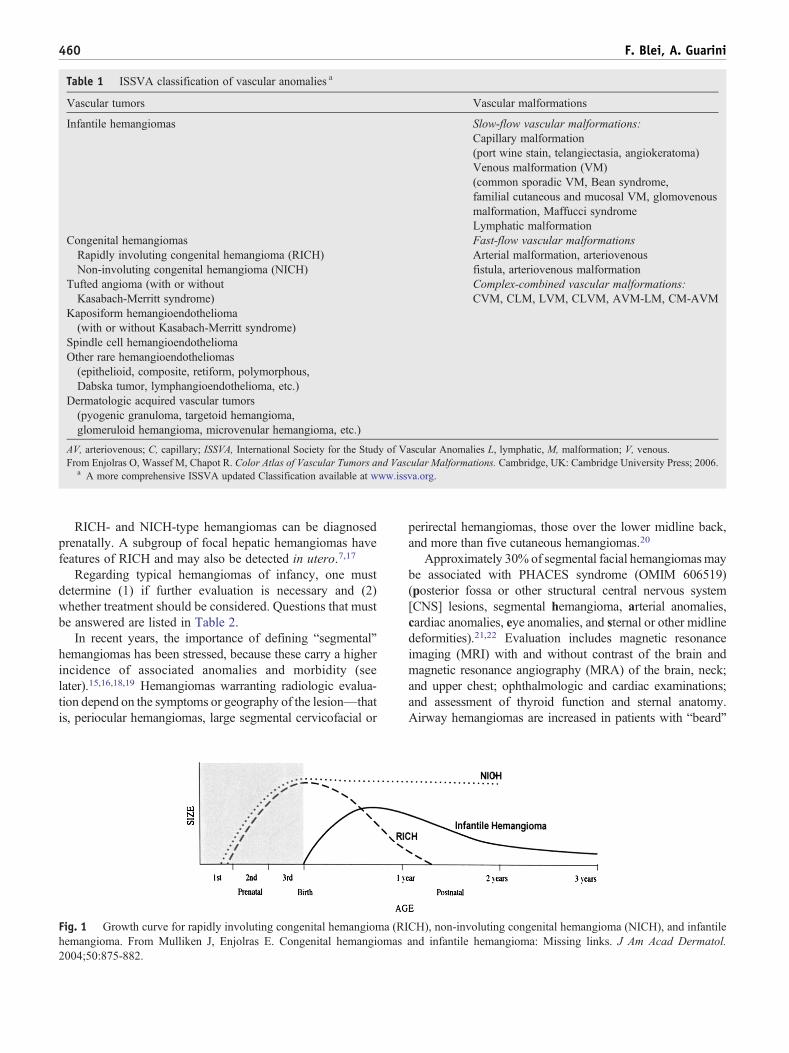
Table 1 ISSVA classification of vascular anomalies a
Vascular tumors Vascular malformations
Infantile hemangiomas Slow-flow vascular malformations:Capillary malformation(port wine stain, telangiectasia, angiokeratoma)Venous malformation (VM)(common sporadic VM, Bean syndrome,familial cutaneous and mucosal VM, glomovenousmalformation, Maffucci syndromeLymphatic malformation
Congenital hemangiomasRapidly involuting congenital hemangioma (RICH)Non-involuting congenital hemangioma (NICH)
Fast-flow vascular malformationsArterial malformation, arteriovenousfistula, arteriovenous malformation
Tufted angioma (with or withoutKasabach-Merritt syndrome)
Complex-combined vascular malformations:CVM, CLM, LVM, CLVM, AVM-LM, CM-AVM
Kaposiform hemangioendothelioma(with or without Kasabach-Merritt syndrome)
Spindle cell hemangioendotheliomaOther rare hemangioendotheliomas(epithelioid, composite, retiform, polymorphous,Dabska tumor, lymphangioendothelioma, etc.)
Dermatologic acquired vascular tumors(pyogenic granuloma, targetoid hemangioma,glomeruloid hemangioma, microvenular hemangioma, etc.)
AV, arteriovenous; C, capillary; ISSVA, International Society for the Study of Vascular Anomalies L, lymphatic, M, malformation; V, venous.From Enjolras O, Wassef M, Chapot R. Color Atlas of Vascular Tumors and Vascular Malformations. Cambridge, UK: Cambridge University Press; 2006.
a A more comprehensive ISSVA updated Classification available at www.issva.org.
460 F. Blei, A. Guarini
RICH- and NICH-type hemangiomas can be diagnosedprenatally. A subgroup of focal hepatic hemangiomas havefeatures of RICH and may also be detected in utero.7,17
Regarding typical hemangiomas of infancy, one mustdetermine (1) if further evaluation is necessary and (2)whether treatment should be considered. Questions that mustbe answered are listed in Table 2.
In recent years, the importance of defining “segmental”hemangiomas has been stressed, because these carry a higherincidence of associated anomalies and morbidity (seelater).15,16,18,19 Hemangiomas warranting radiologic evalua-tion depend on the symptoms or geography of the lesion—thatis, periocular hemangiomas, large segmental cervicofacial or
Fig. 1 Growth curve for rapidly involuting congenital hemangioma (RIhemangioma. From Mulliken J, Enjolras E. Congenital hemangiomas2004;50:875-882.
perirectal hemangiomas, those over the lower midline back,and more than five cutaneous hemangiomas.20
Approximately 30% of segmental facial hemangiomasmaybe associated with PHACES syndrome (OMIM 606519)(posterior fossa or other structural central nervous system[CNS] lesions, segmental hemangioma, arterial anomalies,cardiac anomalies, eye anomalies, and sternal or other midlinedeformities).21,22 Evaluation includes magnetic resonanceimaging (MRI) with and without contrast of the brain andmagnetic resonance angiography (MRA) of the brain, neck;and upper chest; ophthalmologic and cardiac examinations;and assessment of thyroid function and sternal anatomy.Airway hemangiomas are increased in patients with “beard”
CH), non-involuting congenital hemangioma (NICH), and infantileand infantile hemangioma: Missing links. J Am Acad Dermatol.

Fig. 2 A, Rapidly involuting congenital hemangioma (RICH) ofthe scalp, without therapy. B, RICH from Figure 8 afterspontaneous involution. C, Magnetic resonance angiogram of thehead and neck demonstrating the patient’s high-flow RICH of scalp.
ig. 3 A, Segmental hemangioma of infancy on the forearmefore therapy. B, The patient featured in Figure 1 after 1 month ofral propranolol. C, The patient featured in Figure 1 afterompletion of a 6-month course of oral propranolol.
ig. 4 A, Infant with enlarging midfacial hemangioma offancy, before any therapy. B, Same infant featured in Figure 4,fter completion of a course of oral propranolol.
461Workup and therapy of infantile hemangiomas
(mandibular; see Figure 11) distribution cutaneous hemangi-omas (segment 3).15,23,24 Patients with recurrent and progres-sive stridor may have subglottic hemangioma. Conclusivediagnosis is achieved with bronchoscopy and direct visuali-zation of the airway.
Hemangiomas in the lower midline of the back may beassociated with congenital renal, sacral, lower part ofthe spine, or genitourinary anomalies and should beevaluated.25–28 LUMBAR syndrome (lower body hemangi-oma and other cutaneous defects, urogenital anomalies,ulceration, myelopathy, bony deformities, anorectal mal-formations, arterial anomalies, and renal anomalies) andPELVIS syndrome (perineal hemangioma, external genitaliamalformations, lipomyelomeningocele, vesicorenal abnor-malities, imperforate anus, and skin tag) describe a spectrum
Fboc
Fina

Fig. 5 Large untreated and disfiguring hemangioma of infancyon the breast wall.
ig. 7 A and B, Hemangioma of infancy on the left eyelid in anfant before and after therapy with propranolol.
462 F. Blei, A. Guarini
of potential clustering clinical features seen in conjunctionwith segmental perineal hemangiomas.26,29–31 de Graaf et alhave proposed an algorithm for evaluation of lumbosacraland perianal infantile hemangioma (Figure 12).
Periocular hemangiomas
Patients with periocular hemangiomas are at risk forblepharoptosis, amblyopia, strabismus, proptosis, refractiveerrors, optic nerve compression, and anisotropia. Patients withPHACESmay also have retinopathy, cataracts, glaucoma, andoptic nerve or iris abnormalities.32 Early evaluation andfollow-up by regular serial cycloplegic refraction by a pediatricophthalmologist able to perform retinoscopy of preverbalchildren is essential to prevent or minimize visual sequelae.One study showed an increased risk of amblyopia in periocularhemangiomas greater than1 cm in diameter and in diffusesegmental hemangiomas.33 These findings are potentiallyreversible with early institution of treatment.34
Hemangiomatosis
Infants with multiple small cutaneous hemangiomas maypredict parenchymal hemangiomatosis (CNS, eye, pancreas,gastrointestinal tract, lungs), most notably hepatic hemangi-omas. Hepatic hemangiomas represent a special category.Screening with abdominal ultrasound is recommended for
Fig. 6 Involuted hemangioma of infancy is reported to haveredundant tissue and fibrofatty tissue deposition.
Fin
patients younger than 6 months of age with five or morecutaneous hemangiomas because one study showed thatthese patients with were more likely to have hepatichemangiomas.20 If hepatic hemangiomas are noted, labora-tory and cardiac evaluation should ensue. Hepatic heman-giomas may be focal, multifocal, and diffuse. Patients withdiffuse and multifocal hepatic hemangiomas should haveprompt thyroid function screening because they are at risk forconsumptive hypothyroidism as a result of elaboration oftype 3 iodothyronine deiodinase activity in the hemangiomatissue causing a “consumptive hypothyroidism.”35,36 Analgorithm for evaluation and management of hepatichemangiomas of infancy has been developed.37 Prenataldiagnosis of hemangiomas is possible for RICH and NICHlesions. In one study, one third of patients with focal hepatichemangiomas (which have clinical and radiologic features ofRICH) were detected prenatally.36
Miscellaneous issues
Large bulky hemangiomas and hemangiomas in certainanatomic locations (eg, parotid) may be transiently
Fig. 8 End-stage enlargement of an eyelid hemangioma ofinfancy that was untreated.

Fig. 9 Untreated lower lip hemangioma of infancy causingenlargement and distortion.
Table 2 Questions to aid in determination of risk ofcomplications in infantile hemangiomas
1. What is the location of the hemangioma, age of the patient,and size of the lesion?
2. Is the hemangioma superficial, subcutaneous, or combined?3. How large is it?4. Is it focal or segmental?5. Is it single or are there multiple lesions?6. Are there any associated or impending symptoms (ie, stridor,ptosis, ulceration, bleeding, high-flow state, functionalimitation, etc.)?
463Workup and therapy of infantile hemangiomas
associated with high flow.38,39 These hemangiomas have athrill or bruit on examination; if present, cardiac evaluation iswarranted to assess for a high-output state, which maynecessitate therapy. Hemangiomas disposed to ulcerationoccur over pressure points (eg, back) and in mucosal(perineum, lip) or intertriginous areas.40 Meticulous localcare as well as adjunctive therapies are indicated (see later).Biopsy is usually not necessary for hemangiomas; however,not every vascular lesion in an infant is benign. Vascularlesions warranting biopsy generally do not behave as “typical”hemangiomas, RICH or NICH. If a lesion is firm, has anunusual appearance, or is found to have radiologic features ofconcern, biopsy should be performed for prompt diagnosis.Mimickers of hemangiomas include but are not limited torhabdomyosarcoma, neuroblastoma, myobfibroma, fibrosar-coma, glioma, hemangiopericytoma, and leukemia.41–51 Anatypical history or physical examination or a fixed, nonmotilefirm mass should alert the practitioner to obtain histologicconfirmation of the diagnosis.
Table 3 summarizes clinical issues warranting furtherevaluation in patients with hemangiomas.
Management
Early referral is essential to prevent unwanted morbidityand enable timely evaluation. Specialists to better define theextent of concern and work in concert to begin therapy mustpromptly evaluate patients with vision- or airway-threateninghemangiomas. Initiating therapy may abrogate more com-plicated interventions or surgery in the future.
Flash lamp pulsed dye laser treatment can be effective inearly-stage hemangiomas to prevent outward growth52–56
Fig. 10 Ulcerated hemangioma of infancy.
with sequential treatments during the proliferative phase.Laser-associated scarring and pigment and contour changescan occur; however, these complications can be minimizedwith current laser technologies.53,57 Laser treatment mayalso be useful after involution, to remove telangiectasias(pulsed dye), or to smooth contour irregularities (Fraxel;Solta Medical, Inc., Hayward, CA).
Medical therapy has been administered topically, intrale-sionally, and systemically. Until 2008, oral corticosteroidswere the first-line therapy for proliferating hemangiomasrequiring medical treatment. Steroids have been supercededby propranolol, a nonselective beta blocker, serendipitouslydiscovered as a treatment for proliferating infantile heman-giomas.58 Subsequently, more than 200 papers have beenpublished describing clinical efficacy (in most studies) forvarious types of hemangiomas, including periocular, airway,ulcerated, and hepatic hemangiomas.59–70 Studies that havereported purported mechanisms of action are summarized inTable 4.71–76 There is no uniform protocol for drug-relatedpretreatment evaluation and monitoring.77 Potential adverseeffects of propranolol include cool extremities, gastrointes-tinal symptoms, hypotension, nocturnal restlessness, reactive
ig. 11 Segmental pattern of distribution of facial hemangiomas.rom Haggstrom A, Lammer EJ, Schneider RA, Marcucio R,rieden IJ. Patterns of infantile hemangiomas: New clues toemangioma pathogenesis and embryonic facial development.ediatrics 2006;117:699.
FFFhP

Fig. 12 Diagnostic approach of lumbosacral and perianal infantile hemangioma (IH). LUMBAR, Lower body IH and other skin defects,urogenital anomalies and ulceration, myelopathy, bony deformities, anorectal malformations, arterial anomalies, and renal anomalies; MRI,magnetic resonance imaging. From de Graaf M, Pasmans SG, van Drooge AM, et al. Associated anomalies and diagnostic approach inlumbosacral and perineal haemangiomas: Case report and review of the literature. J Plast Reconstr Aesthet Surg. 2012;66:e26-28.
464 F. Blei, A. Guarini
airways, and bradycardia, with rare but significant reports ofhypoglycemia.22,63,78,79 The medication should be heldduring intercurrent illnesses associated with diminishedoral intake or respiratory symptoms, as well as before anyprocedures for which the child will be fasting.80 Alternative
Table 3 Hemangiomas: Clinical issues meriting evaluation
Clinical finding Recomm
HemangiomatosisN5 cutaneous hemangiomas
Ultrasou
Segmental facial hemangioma EvaluatehemangiMRA brCardiac,Evaluatisternal aThyroidMRA evPerioculMRI +/-
Cutaneous hemangiomas in “beard” distribution EvaluatiParaspinal midline hemangiomas Ultrasou
for occuanogenit
Thrill or bruit, or both, associated with hemangioma CardiacTorticollis, flexure contracture PhysicalDelayed milestones CNS/PH
CNS, central nervous system; MRA, magnetic resonance angiography; MRI, ma
selective beta blockers may obviate these concerns; however,further studies are needed. Topical beta blockers (eg, timololmaleate gel-forming solution; Alcon Laboratories, FortWorth, TX) may hinder growth and expedite involution ofsmall superficial hemangiomas.81–84
ended evaluation
nd evaluation for parenchymal hemangiomas
for PHACES—MRI +/- contrast for orbitaloma ± posterior fossa malformationain, neck to thoracic aortaophthalmologic evaluationson for midline abnormality—supraumbilical raphe,tresia, cleft palate, thyroid abnormalityfunction evaluationaluation of craniocervical vessels for anomalyar hemangiomacontrast of orbit ophthalmologic evaluationon for airway hemangioma, especially if presenting with stridornd (if younger than 6 months old) or MRI to evaluatelt spinalal dysraphism ± underlying vascular lesion orourinary anomalyevaluation and echo to rule out diastolic reversal of flow of aortatherapyACE-related issue, hearing assessment
gnetic resonance imaging.

Table 4 Propranolol: Potential mechanism of action
Proposed mechanism of action Reference
Early vasoconstriction (decreased nitrous oxide)Angiogenesis inhibition (interference with vascular endothelialgrowth factor [VEGF]– and bFGF-induced endothelial cell proliferation)Apoptosis induction
Storch et al, 201095
G/G phase cell cycle arrestInhibition of VEGF-induced tyrosine phosphorylation of VEGF-R-2
Lamy et al, 201296
Inhibition of endothelial progenitor cell homing Zou et al, 201271
Hastens adipogenesis in hemangioma stem cellsTriggers apoptosis of hemangioma endothelial cells
Wong et al, 201273
Endothelial cell type independentBlockade of endothelial cell proliferation, migration, and multiple functions
Stiles et al 201274
Inhibition of inhibit hemangioma endothelial cell proliferation and induction of apoptosisDose-dependent VEGF expression downregulation
Ji et al, 201297
Inhibition of angiotensin-converting enzyme and angiotensinII receptor 2, resulting in decreased ATII and VEGF
Itinteang et al, 201198
Inhibition of hemangioma emangioma of he Hadaschik et al, 201275
Inhibition of hemangioma endothelial nitric oxide synthase Dai et al, 201299
Hypoxia inducible factor (HIF-1 alpha)–related inhibition of VEGF-A Chim et al, 201272
Targeting hemangioma endothelial cell pericytes Boscolo et al 201376
465Workup and therapy of infantile hemangiomas
Various combinations of local and systemic therapies forulcerated hemangiomas are included in the reviews notedearlier. Topical or systemic antibiotics may be necessary forsuperinfected ulcerated hemangiomas. Additionally, analge-sics, hemostatic agents for bleeding, hydrocolloid gels toexpedite healing, and topical beta blockers may be used.Recombinant platelet-derived growth factor is efficaciousfor ulcerated hemangiomas,85,86 although a “black box”warning restricts its use because of an increasedincidence of malignancy when used for diabetic ulcers.(http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm094968.htm).
Older remedies include topical imiquimod87,88; subcuta-neous interferon, which had a side effect of spastic diplegiain about 10% of children89; and intravenous vincristine.90
Preliminary results suggest beta-blocker therapy providesefficacy with a safety profile superior to older agents.
Controversies in management of subglottic hemangiomasinclude surgery (submucous resection); laser (CO2 versuspotassium titanyl phosphate [KTP]); oral propranolol; steroids(intralesional versus systemic); and interferon-alpha (IFN-α)or tracheotomy, or both. CO2 or KTP laser may be helpful fornoncircumferential subglottic hemangiomas.91
Table 5 summarizes current studies focused on treatment orevaluation of patients with hemangiomas of infancy Table 6.
Surgery
Surgical excision for hemangiomas is indicated in theproliferative stage if there are symptoms not controllable byother means (eg, bleeding, amblyopia, astigmatism) or incertain anatomic locations (eg, early excision of large scalp
hemangiomas benefit from greater laxity of the infantscalp).92 Large scalp, forehead, nasal tip, and auricularhemangiomas generally require surgical intervention at somepoint.93,94 Indications for and timing of surgery forhemangiomas remain controversial.
References
1. Hassanein AH, Mulliken JB, Fishman SJ, Greene AK. Evaluation ofterminology for vascular anomalies in current literature. Plast ReconstrSurg. 2011;127:347-351.
2. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations ininfants and children: A classification based on endothelial character-istics. Plast Reconstr Surg. 1982;69:412-422.
3. Enjolras O, Wassef M, Chapot R. Color Atlas of Vascular Tumors andVascular Malformations. Cambridge, UK: Cambridge University Press.2006.
4. North PE, Waner M, James CA, Mizeracki A, Frieden IJ, Mihm Jr MC.Congenital nonprogressive hemangioma: A distinct clinicopathologic entityunlike infantile hemangioma. Arch Dermatol. 2001;137:1607-1620.
5. Berenguer B, Mulliken JB, Enjolras O, et al. Rapidly involutingcongenital hemangioma: Clinical and histopathologic features. PediatrDev Pathol. 2003;6:495-510.
6. Konez O, Burrows PE, Mulliken JB, Fishman SJ, Kozakewich HP.Angiographic features of rapidly involuting congenital hemangioma(RICH). Pediatr Radiol. 2003;33:15-19.
7. Elia D, Garel C, Enjolras O, et al. Prenatal imaging findings in rapidlyinvoluting congenital hemangioma of the skull. Ultrasound ObstetGynecol. 2008;31:572-575.
8. Rogers M, Lam A, Fischer G. Sonographic findings in a series ofrapidly involuting congenital hemangiomas (RICH). Pediatr Dermatol.2002;19:5-11.
9. Gorincour G, Kokta V, Rypens F, Garel L, Powell J, Dubois J. Imagingcharacteristics of two subtypes of congenital hemangiomas: Rapidlyinvoluting congenital hemangiomas and non-involuting congenitalhemangiomas. Pediatr Radiol. 2005;35:1178-1185.

466 F. Blei, A. Guarini
10. Boon LM, Enjolras O, Mulliken JB. Congenital hemangioma: Evidenceof accelerated involution. J Pediatr. 1996;128:329-335.
11. Baselga E, Cordisco MR, Garzon M, Lee MT, Alomar A, Blei F.Rapidly involuting congenital haemangioma associated with transientthrombocytopenia and coagulopathy: A case series. Br J Dermatol.2008;158:1363-1370.
12. Rangwala S,Wysong A, TollefsonMM,Khuu P, Benjamin LT, BrucknerAL. Rapidly involuting congenital hemangioma associated with pro-found, transient thrombocytopenia. Pediatr Dermatol. 2014;31:402-404.
13. Weitz NA, Lauren CT, Starc TJ, et al. Congenital cutaneoushemangioma causing cardiac failure: A case report and review of theliterature. Pediatr Dermatol. 2013;30:e180-e190.
14. Mulliken JB, Enjolras O. Congenital hemangiomas and infantilehemangioma: Missing links. J Am Acad Dermatol. 2004;50:875-882.
15. Waner M, North PE, Scherer KA, Frieden IJ, Waner A, Mihm Jr MC.The nonrandom distribution of facial hemangiomas. Arch Dermatol.2003;139:869-875.
16. Haggstrom AN, Lammer EJ, Schneider RA, Marcucio R, Frieden IJ.Patterns of infantile hemangiomas: New clues to hemangioma pathogen-esis and embryonic facial development. Pediatrics. 2006;117:698-703.
17. Fadell II MF, Jones BV, Adams DM. Prenatal diagnosis and postnatalfollow-up of rapidly involuting congenital hemangioma (RICH).Pediatr Radiol. 2011;41:1057-1060.
18. Haggstrom AN, Drolet BA, Baselga E, et al. Prospective study ofinfantile hemangiomas: Clinical characteristics predicting complica-tions and treatment. Pediatrics. 2006;118:882-887.
19. Metry DW, Haggstrom AN, Drolet BA, et al. A prospective study ofPHACE syndrome in infantile hemangiomas: Demographic features,clinical findings, and complications.Am JMedGenet A. 2006;140:975-986.
20. Horii KA, Drolet BA, Frieden IJ, et al. Prospective study of thefrequency of hepatic hemangiomas in infants with multiple cutaneousinfantile hemangiomas. Pediatr Dermatol. 2011;28:245-253.
21. Metry D, Heyer G, Hess C, et al. Consensus statement on diagnosticcriteria for PHACE syndrome. Pediatrics. 2009;124:1447-1456.
22. Haggstrom AN, Garzon MC, Baselga E, et al. Risk for PHACEsyndrome in infants with large facial hemangiomas. Pediatrics.2010;126:e418-e426.
23. Orlow SJ, Isakoff MS, Blei F. Increased risk of symptomatichemangiomas of the airway in association with cutaneous hemangi-omas in a "beard" distribution. J Pediatr. 1997;131:643-646.
24. Durr ML, Meyer AK, Huoh KC, Frieden IJ, Rosbe KW. Airwayhemangiomas in PHACE syndrome. Laryngoscope. 2012;122:2323-2329.
25. Goldberg NS, Hebert AA, Esterly NB. Sacral hemangiomas andmultiple congenital abnormalities. Arch Dermatol. 1986;122:684-687.
26. Girard C, Bigorre M, Guillot B, Bessis D. PELVIS Syndrome. ArchDermatol. 2006;142:884-888.
27. Drolet BA, Chamlin SL, Garzon MC, et al. Prospective study of spinalanomalies in children with infantile hemangiomas of the lumbosacralskin. J Pediatr. 2010;157:789-794.
28. Stockman A, Boralevi F, Taieb A, Leaute-Labreze C. SACRALsyndrome: Spinal dysraphism, anogenital, cutaneous, renal and urologicanomalies, associated with an angioma of lumbosacral localization.Dermatology. 2007;214:40-45.
29. Frade F, Kadlub N, Soupre V, et al. PELVIS or LUMBAR syndrome:The same entity. Two case reports. Arch Pediatr. 2012;19:55-58.
30. Iacobas I, Burrows PE, Frieden IJ, et al. LUMBAR: Association betweencutaneous infantile hemangiomas of the lower body and regionalcongenital anomalies. J Pediatr. 2010;157:795-801. [e791-797].
31. de Graaf M, Pasmans SG, van Drooge AM, et al. Associated anomaliesand diagnostic approach in lumbosacral and perineal haemangiomas:Case report and review of the literature. J Plast Reconstr Aesthet Surg.2012;66:e26-e28.
32. Kronenberg A, Blei F, Ceisler E, Steele M, Furlan L, Kodsi S. Ocularand systemic manifestations of PHACES (Posterior fossa malforma-tions, Hemangiomas, Arterial anomalies, Cardiac defects and coarcta-tion of the Aorta, Eye abnormalities, and Sternal abnormalities orventral developmental defects) syndrome. J AAPOS. 2005;9:169-173.
33. Schwartz SR, Blei F, Ceisler E, Steele M, Furlan L, Kodsi S. Riskfactors for amblyopia in children with capillary hemangiomas of theeyelids and orbit. J AAPOS. 2006;10:262-268.
34. Schwartz SR, Kodsi SR, Blei F, Ceisler E, Steele M, Furlan L.Treatment of capillary hemangiomas causing refractive and occlusionalamblyopia. J AAPOS. 2007;11:577-583.
35. Huang SA, Tu HM, Harney JW, et al. Severe hypothyroidism caused bytype 3 iodothyronine deiodinase in infantile hemangiomas. N Engl JMed. 2000;343:185-189.
36. Kulungowski AM, Alomari AI, Chawla A, Christison-Lagay ER,Fishman SJ. Lessons from a liver hemangioma registry: Subtypeclassification. J Pediatr Surg. 2012;47:165-170.
37. Christison-Lagay ER, Burrows PE, Alomari A, et al. Hepatichemangiomas: Subtype classification and development of a clinicalpractice algorithm and registry. J Pediatr Surg. 2007;42:62-67.[discussion 67–68].
38. Blei F, Rutkowski M. Transiently arterialized hemangiomas: Relevantclinical and cardiac issues. Lymphat Res Biol. 2003;1:317-320.
39. Rutkowski M, Blei F. The role of pediatric cardiology in themanagement of hemangiomas. Lymphat Res Biol. 2005;3:260-262.
40. Chamlin SL,HaggstromAN,DroletBA, et al.Multicenter prospective studyof ulcerated hemangiomas. J Pediatr. 2007;151:684-689. [689 e681].
41. Boon LM, Fishman SJ, Lund DP, Mulliken JB. Congenital fibrosar-coma masquerading as congenital hemangioma: Report of two cases.J Pediatr Surg. 1995;30:1378-1381.
42. Asgari M, Rubin BP, Hornung RL. Neonate with a fibrosarcoma andconsumptive coagulopathy. J Am Acad Dermatol. 2004;50(2 Suppl):S23-S25.
43. Yan AC, Chamlin SL, Liang MG, et al. Congenital infantilefibrosarcoma: A masquerader of ulcerated hemangioma. PediatrDermatol. 2006;23:330-334.
44. Al-Mubarak L, Al-Khenaizan S. A wolf in sheep's disguise:Rhabdomyosarcoma misdiagnosed as infantile hemangioma. J CutanMed Surg. 2009;13:276-279.
45. Requena C, Miranda L, Canete A, et al. Congenital fibrosarcomasimulating congenital hemangioma. Pediatr Dermatol. 2008;25:141-144.
46. Frieden IJ, Rogers M, Garzon MC. Conditions masquerading asinfantile haemangioma: Part 2. Australas J Dermatol. 2009;50:153-168. [quiz 169–170].
47. Hassanein AH, Fishman SJ, Mulliken JB, et al. Metastatic neuroblastomamimicking infantile hemangioma. J Pediatr Surg. 2010;45:2045-2049.
48. Megarbane H, Doz F, Manach Y, et al. Neonatal rhabdomyosarcomamisdiagnosed as a congenital hemangioma. Pediatr Dermatol.2011;28:299-301.
49. AssenYJ,MadernGC, deLaat PC, denHollander JC,OranjeAP.Rhabdoidtumor mimicking hemangioma. Pediatr Dermatol. 2011;28:295-298.
50. Behnke NM, Patel M, Davidson T, Arkader A. Orthopaedic case of themonth: Rapidly progressive shoulder soft tissue mass in an 8-week-oldgirl. Clin Orthop Relat Res. 2011;469:624-629.
51. Jain D, Kohli K. Congenital infantile fibrosarcoma: A clinical mimickerof hemangioma. Cutis. 2012;89:61-64.
52. Kono T, Sakurai H, Groff WF, et al. Comparison study of a traditionalpulsed dye laser versus a long-pulsed dye laser in the treatment of earlychildhood hemangiomas. Lasers Surg Med. 2006;38:112-115.
53. Admani S, Krakowski AC, Nelson JS, Eichenfield LF, Friedlander SF.Beneficial effects of early pulsed dye laser therapy in individuals withinfantile hemangiomas. Dermatol Surg. 2012;38:1732-1738.
54. Bruscino N, Bonan P, Cannarozzo G, Moretti S, Lotti T, Campolmi P.Laser use in infantile hemangiomas, when and how. Dermatol Ther.2012;25:314-321.
55. Tay YK, Tan SK. Treatment of infantile hemangiomas with the 595-nmpulsed dye laser using different pulse widths in an Asian population.Lasers Surg Med. 2012;44:93-96.
56. Geronemus RG. Commentary: Beneficial effects of early pulsed dyelaser therapy in patients with infantile hemangiomas. Dermatol Surg.2012;38:1739-1740.

467Workup and therapy of infantile hemangiomas
57. Witman PM, Wagner AM, Scherer K, Waner M, Frieden IJ.Complications following pulsed dye laser treatment of superficialhemangiomas. Lasers Surg Med. 2006;38:116-123.
58. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, Boralevi F,Thambo JB, Taieb A. Propranolol for severe hemangiomas of infancy.N Engl J Med. 2008;358:2649-2651.
59. Buckmiller LM, Munson PD, Dyamenahalli U, Dai Y, Richter GT.Propranolol for infantile hemangiomas: Early experience at a tertiaryvascular anomalies center. Laryngoscope. 2010;120:676-681.
60. Bertrand J, Sammour R, McCuaig C, et al. Propranolol in the treatmentof problematic infantile hemangioma: Review of 35 consecutive patientsfrom a vascular anomalies clinic. J Cutan Med Surg. 2012;16:317-323.
61. Gan LQ, Ni SL, Tan Q, Wang H. A retrospective study of propranololtherapy in 109 infants with infantile hemangioma. Pediatr Dermatol.2013;30:270-272.
62. Haider KM, Plager DA, Neely DE, Eikenberry J, Haggstrom A.Outpatient treatment of periocular infantile hemangiomas with oralpropranolol. J AAPOS. 2010;14:251-256.
63. Hermans DJ, Bauland CG, Zweegers J, van Beynum IM, van derVleuten CJ. Propranolol in a case series of 174 complicated infantilehaemangioma patients: Indications, safety and future directions. Br JDermatol. 2013;168:837-843.
64. Leboulanger N, Fayoux P, Teissier N, et al. Propranolol in thetherapeutic strategy of infantile laryngotracheal hemangioma: Apreliminary retrospective study of French experience. Int J PediatrOtorhinolaryngol. 2010;74:1254-1257.
65. Mazereeuw-Hautier J, Hoeger PH, Benlahrech S, et al. Efficacy ofpropranolol in hepatic infantile hemangiomas with diffuse neonatalhemangiomatosis. J Pediatr. 2010;157:340-342.
66. Missoi TG, Lueder GT, Gilbertson K, Bayliss SJ. Oral propranolol fortreatment of periocular infantile hemangiomas. Arch Ophthalmol.2011;129:899-903.
67. Naouri M, Schill T, Maruani A, Bross F, Lorette G, Rossler J.Successful treatment of ulcerated haemangioma with propranolol. J EurAcad Dermatol Venereol. 2010;24:1109-1112.
68. Betlloch-Mas I, Martinez-Miravete MT, Martin de Lara AI, Lucas-Costa A, Selva-Otalaurruchi J. Outpatient treatment of infantilehemangiomas with propranolol: A prospective study. Actas Dermosi-filiogr. 2012;103:806-815.
69. Rosbe KW, Suh KY, Meyer AK, Maguiness SM, Frieden IJ.Propranolol in the management of airway infantile hemangiomas.Arch Otolaryngol Head Neck Surg. 2010;136:658-665.
70. Vlastarakos PV, Papacharalampous GX, Chrysostomou M, et al.Propranolol is an effective treatment for airway haemangiomas: Acritical analysis and meta-analysis of published interventional studies.Acta Otorhinolaryngol Ital. 2012;32:213-221.
71. Zou HX, Jia J, Zhang WF, Sun ZJ, Zhao YF. Propranolol inhibitsendothelial progenitor cell homing: A possible treatment mechanism ofinfantile hemangioma. Cardiovasc Pathol. 2013;22:203-210.
72. Chim H, Armijo BS, Miller E, Gliniak C, Serret MA, Gosain AK.Propranolol induces regression of hemangioma cells through HIF-1alpha-mediated inhibition of VEGF-A. Ann Surg. 2012;256:146-156.
73. Wong A, Hardy KL, Kitajewski AM, Shawber CJ, Kitajewski JK, WuJK. Propranolol accelerates adipogenesis in hemangioma stem cells andcauses apoptosis of hemangioma endothelial cells. Plast Reconstr Surg.2012;130:1012-1021.
74. Stiles J, Amaya C, Pham R, et al. Propranolol treatment of infantilehemangioma endothelial cells: A molecular analysis. Exp Ther Med.2012;4:594-604.
75. Hadaschik E, Scheiba N, Engstner M, Flux K. High levels of beta2-adrenoceptors are expressed in infantile capillary hemangiomas andmay mediate the therapeutic effect of propranolol. J Cutan Pathol.2012;39:881-883.
76. Boscolo E, Mulliken JB, Bischoff J. Pericytes from infantilehemangioma display proangiogenic properties and dysregulatedangiopoietin-1. Arterioscler Thromb Vasc Biol. 2013;33:501-509.
77. Drolet BA, Frommelt PC, Chamlin SL, et al. Initiation and Use ofPropranolol for Infantile Hemangioma: Report of a ConsensusConference. Pediatrics. 2013;131:128-140.
78. Bonifazi E, Acquafredda A, Milano A, Montagna O, Laforgia N. Severehypoglycemia during successful treatment of diffuse hemangiomatosiswith propranolol. Pediatr Dermatol. 2010;27:195-196.
79. Breur JM, de Graaf M, Breugem CC, Pasmans SG. Hypoglycemia as aresult of propranolol during treatment of infantile hemangioma: A casereport. Pediatr Dermatol. 2011;28:169-171.
80. Allford MA, Brown JL. Case report: Intraoperative hypoglycaemia in achild treated with propranolol following a short preoperative fast. Eur JAnaesthesiol. 2011;28:71-72.
81. Pope E, Chakkittakandiyil A. Topical timolol gel for infantilehemangiomas: A pilot study. Arch Dermatol. 2010;146:564-565.
82. Guo S, Ni N. Topical treatment for capillary hemangioma of the eyelidusing beta-blocker solution. Arch Ophthalmol. 2010;128:255-256.
83. Chakkittakandiyil A, Phillips R, Frieden IJ, et al. Timolol maleate 0.5%or 0.1% gel-forming solution for infantile hemangiomas: A retrospec-tive, multicenter, cohort study. Pediatr Dermatol. 2012;29:28-31.
84. Chambers CB, Katowitz WR, Katowitz JA, Binenbaum G. A controlledstudy of topical 0.25% timolol maleate gel for the treatment ofcutaneous infantile capillary hemangiomas. Ophthal Plast ReconstrSurg. 2012;28:103-106.
85. Sugarman JL, Mauro TM, Frieden IJ. Treatment of an ulceratedhemangioma with recombinant platelet-derived growth factor. ArchDermatol. 2002;138:314-316.
86. Metz BJ, Rubenstein MC, Levy ML, Metry DW. Response ofulcerated perineal hemangiomas of infancy to becaplermin gel, arecombinant human platelet-derived growth factor. Arch Dermatol.2004;140:867-870.
87. Ho NT, Lansang P, Pope E. Topical imiquimod in the treatment of infantilehemangiomas: A retrospective study. J Am Acad Dermatol. 2007;56:63-68.
88. McCuaig CC, Dubois J, Powell J, et al. A phase II, open-label study ofthe efficacy and safety of imiquimod in the treatment of superficial andmixed infantile hemangioma. Pediatr Dermatol. 2009;26:203-212.
89. Ezekowitz RA,Mulliken JB, Folkman J. Interferon alfa-2 a therapy for life-threatening hemangiomas of infancy.NEngl JMed. 1992;326:1456-1463.
90. Fawcett SL, Grant I, Hall PN, Kelsall AW, Nicholson JC. Vincristine asa treatment for a large haemangioma threatening vital functions. Br JPlast Surg. 2004;57:168-171.
91. Balakrishnan K, Perkins JA. Management of airway hemangiomas.Expert Rev Respir Med. 2010;4:455-462.
92. Spector JA, Blei F, Zide BM. Early surgical intervention forproliferating hemangiomas of the scalp: Indications and outcomes.Plast Reconstr Surg. 2008;122:457-462.
93. Daramola OO, Chun RH, Nash JJ, et al. Surgical treatment of infantilehemangioma in a multidisciplinary vascular anomalies clinic. Int JPediatr Otorhinolaryngol. 2011;75:1271-1274.
94. Daramola OO, Chun RH, Kerschner JE. Surgical management ofauricular infantile hemangiomas. Arch Otolaryngol Head Neck Surg.2012;138:72-75.
95. Storch CH, Hoeger PH. Propranolol for infantile haemangiomas: Insightsinto themolecularmechanisms of action.Br JDermatol. 2010;163:269-274.
96. Lamy S, Lachambre MP, Lord-Dufour S, Beliveau R. Propranololsuppresses angiogenesis in vitro: Inhibition of proliferation, migration, anddifferentiation of endothelial cells. Vascul Pharmacol. 2010;53:200-208.
97. Ji Y, Li K, Xiao X, Zheng S, Xu T, Chen S. Effects of propranolol onthe proliferation and apoptosis of hemangioma-derived endothelialcells. J Pediatr Surg. 2012;47:2216-2223.
98. Itinteang T, Brasch HD, Tan ST, Day DJ. Expression of components ofthe renin-angiotensin system in proliferating infantile haemangiomamay account for the propranolol-induced accelerated involution. J PlastReconstr Aesthet Surg. 2011;64:759-765.
99. Dai Y, Hou F, Buckmiller L, et al. Decreased eNOS protein expressionin involuting and propranolol-treated hemangiomas. Arch OtolaryngolHead Neck Surg. 2012;138:177-182.

Table 5 Clinical trials for hemangiomas
Title of study Site ClinicalTrials.govidentifier:
Details
Efficacy and Safety of Propranolol Versus Acebutololon the Proliferative Phase of Infantile HemangiomaSingle BlindPhase 3
University Hospital,Montpellier, France
NCT01743885 Up to 6 months oldPrimary outcome measure: Hemangioma size(visual analog scale) older than 3 months
Propranolol Vs Prednisolone forSymptomatic HemangiomasPhase 2Single BlindRandomized
Children's Research Institute(Children's National Medical Center)
NCT00967226 Up to 5 months oldPrimary outcome measure:
• Reduction in hemangioma sizeNadolol for Proliferating InfantileHemangiomas (active, not recruiting)Phase 2
The Hospital for Sick Children NCT01010308 1 month to 1 year oldPrimary outcome measure:• At least 75% improvement in hemangioma size
Topical Timolol for SuperficialInfantile HemangiomaPhase 3Randomized
Mahidol UniversityBangkok, Thailand
NCT01685398 Up to 2 years oldEfficacy of the topical 0.5% timololmaleate solution vs placeboHemangioma size (visual analog scale)
Open-label, Uncontrolled Studyof the Off Label Use ofPropranolol for Infancy Hemangiomas toIdentify Side EffectsActive, Not recruiting
Hannover Medical SchoolGermany
NCT01211080 1 month to 8 month oldOral propranolol +/- concomitant(cryotherapy, or laser)Primary outcome:CosmesisAdverse events
Study in Infants With Infantile Hemangioma toCompare Propranolol Gel to PlaceboActive, not recruitingPhase 2Randomized
Pierre Fabre Dermatology NCT01512173 Primary outcome measure:
• Complete/nearly complete resolution ofthe infantile hemangioma at week12 compared with baseline
Comparative Study of theUse of Beta Blocker and OralCorticosteroid in the Treatment ofInfantile HemangiomaPhase 2
University of Sao Paulo, Brazil NCT01072045 Up to 2 years oldPrimary outcome measure:
• Reduction on tumor volume
468F.
Blei,A.
Guarini

Timolol Option for UlceratedHemangiomas (TOUCH Trial)Phase 2Randomized
Children's Hospital of Philadelphia NCT01408056 1 month to 8 months oldTimolol vs mupirocinPrimary outcome measure:
• Time to wound reepithelization at 3 monthsStudy to Demonstrate the Efficacy andSafety of Propranolol Oral Solution inInfants with Proliferating Infantile HemangiomasRequiring Systemic Therapy (HEMANGIOL)Active, not recruitingPhase 2 PropranololPhase 3 PlaceboDouble Blind
Pierre Fabre Dermatology NCT01056341 Compare four regimens of propranolol(1 or 3 mg/kg/day for 3 or 6 months)to placebo (double blind).Primary outcome measure:
• Complete/nearly complete resolutionof the target Infantile hemangioma at week24 compared with baseline
Longitudinal Study of Neurologic,Cognitive, and RadiologicOutcomes of PHACE SyndromeObservational
Medical College of Wisconsin NCT01018082 4-6 years old with PHACEPrimary outcome measure:
• Define functional and neurodevelopmentaloutcome of PHACE syndrome, and identifypotential biomarkers predictive of progressivevasculopathy, ischemic stroke, andneurodevelopmental impairment
Hemangioma Growth During the First 6 Months of LifeActive, not recruitingObservational
University of California, San Francisco NCT00911781 3 months to 5 yearsretrospective review of serial photographsof hemangiomas
Airway Vascular LesionsActive, not recruiting
University of Arkansas NCT00866827 Determine protocols for treatment of airwayvascular malformation and to evaluate resultsfrom treatment of these lesions
Genetic Analysis of PHACE Syndrome(Hemangioma with Other Congenital Anomalies)Observational
Medical College of Wisconsin NCT01016756 Primary outcome measures:
• Establish a DNA and tissue bank• Determine candidate genes for PHACE
syndrome using a genome-wide approachA Prospective Longitudinal Study to IdentifyBiomarkers in Children with HemangiomasObservational
The Ohio State UniversityNationwide Children's Hospital
NCT01598116 Up to 5 months oldUrine collection and ultrasonography (of hemangioma)
Optical Tomographic Imaging ofInfantile Hemangiomas
Columbia University NCT01673971 Initial visit up to 2 months of ageHandheld wireless device usingdiffuse optical imaging (DOI), measuring hemangiomablood flow; correlate with clinical findings
469Workup
andtherapy
ofinfantile
hemangiom
as

Table 6 Internet Resources for Patients and Physicians
Program Website
About Face http://www.aboutfaceinternational.org
Arkansas Children’s HospitalVascular AnomaliesProgram
http://www.birthmarks.org
Boston Children’s HospitalVascular AnomaliesProgram
http://www.childrenshospital.org/clinicalservices/Site1964/mainpageS1964P0.html
Children’s Hospital ofWisconsin VascularAnomalies Program
http://www.chw.org/display/PPF/DocID/36150/router.asp
Cincinnati Children’s HospitalVascular AnomaliesProgram
http://www.cincinnatichildrens.org/service/h/hemangioma/default
Genetics Home Reference http://ghr.nlm.nih.govInternational Society for theStudy of VascularAnomalies
http://www.issva.org
Medline Plus www.medlineplus.govNational Organization for RareDiseases
http://www.rarediseases.org
National Organization ofVascular Anomalies
http://www.novanews.org
Seattle Children’s’ HospitalVascular AnomaliesProgram
http://www.seattlechildrens.org/clinics-programs/vascular-anomalies
UCSF Vascular AnomaliesProgram
http://www.bvac.ucsf.edu
Vascular Birthmark Instituteof New York
http://www.vbiny.org
Vascular BirthmarkFoundation
http://birthmark.org
470 F. Blei, A. Guarini


![InfantileHemangiomasMasqueradingas …strawberry-colorednodule,whiledeeporbitalhemangiomas typically present as a fluctuant, compressible bluish mass [2]. Infantile hemangiomas are](https://static.fdocuments.in/doc/165x107/6103541b09e789301341c088/infantilehemangiomasmasqueradingas-strawberry-colorednodulewhiledeeporbitalhemangiomas.jpg)















