Current Practice Patterns and Recent Trends in Breast Biopsy Among Radiologists and Surgeons
3
Current Practice Patterns and Recent Trends in Breast Biopsy Among Radiologists and Surgeons David C. Levin, MD ab , Vijay M. Rao, MD a , Andrea J. Frangos, MS a , Laurence Parker, PhD a , Jonathan H. Sunshine, PhD c Purpose: To ascertain the relative roles of radiologists and surgeons in breast biopsy. Methods and Materials: The Nationwide Medicare Physician Supplier Procedure Summary Master Files for 1999 to 2004 were used to study the 4 Current Procedural Terminology ® , Fourth Edition, codes for breast biopsy. Using the Medicare specialty codes, physician providers were categorized as radiologists, surgeons, or others. Procedure volumes for each of the 3 groups were tabulated for each year of the study, and trends were assessed. Results: Between 1999 and 2004, the breast biopsy utilization rate per 100,000 Medicare beneficiaries increased by 43%. In 2004, a total of 144,697 breast biopsies were performed, of which 124,423 (86%) were done with imaging guidance. From 1999 to 2004, procedure volume increased by 101% among radiologists, compared with 32% among surgeons. By 2004, radiologists performed 63% of all breast biopsies, compared with 32% by surgeons and 5% by others. Within the 2 codes that are specific for the use of imaging guidance, radiologists performed 72%. Conclusions: Radiologists predominate in breast biopsies, and their role has gotten progressively stronger in recent years. Key Words: Breast biopsy, breast imaging, medical economics, diagnostic radiology, radiology, radiologists, socioeconomics issues J Am Coll Radiol 2006;3:707-709. Copyright © 2006 American College of Radiology The introduction of percutaneous, image-guided inter- ventional procedures often produces conflict with sur- geons or other specialists who had been previously accus- tomed to using open surgical procedures to achieve the same ends and who sometimes view the new approaches as threats to their practice. Breast biopsy is an example of this situation. In recent years, percutaneous breast biopsy using stereotactic mammographic techniques or ultra- sound guidance have replaced many open surgical biop- sies, and surgeons have espoused these new approaches [1-3]. Our purpose in this investigation was to determine what proportions of these procedures are performed by radiologists, surgeons, and other physicians, as well as to ascertain recent trends in their utilization. MATERIALS AND METHODS We used the nationwide Centers for Medicare and Medic- aid Services Physician Supplier Procedure Summary Master Files for the period from 1999 to 2004. These databases cover all Medicare fee-for-service beneficiaries, but not those enrolled in health maintenance organizations (12.4% in 2004). For every Current Procedural Terminology 4th ed, (CPT-4) ® code, the Physician Supplier Procedure Sum- mary Master Files provide information on the volume of services performed nationwide each year in the Medicare fee-for-service population, the specialties of the provider physicians, and other useful information, such as reimburse- ments paid, place of service, region of the country, and so on. We studied the 4 CPT-4 ® surgical procedure codes used to submit claims for breast biopsies, two of which use imaging guidance and two of which do not. These codes a Department of Radiology, Thomas Jefferson University Hospital and Jeffer- son Medical College, Philadelphia, Pa. b HealthHelp, Inc., Houston, Tex. c American College of Radiology, Reston, Va. Corresponding author and reprints: David C. Levin, MD, Thomas Jeffer- son University Hospital, Department of Radiology, Main 1090, Philadelphia, PA 19107;e-mail: [email protected]. This study was supported in part by a grant from Berlex Laboratories, Montville, NJ. © 2006 American College of Radiology 0091-2182/06/$32.00 ● DOI 10.1016/j.jacr.2006.03.025 707
Transcript of Current Practice Patterns and Recent Trends in Breast Biopsy Among Radiologists and Surgeons

Tvgtsatuss[
a
sb
c
sP
M
©0
Current Practice Patterns and RecentTrends in Breast Biopsy Among
Radiologists and SurgeonsDavid C. Levin, MDab, Vijay M. Rao, MDa, Andrea J. Frangos, MSa,
Laurence Parker, PhDa, Jonathan H. Sunshine, PhDc
Purpose: To ascertain the relative roles of radiologists and surgeons in breast biopsy.
Methods and Materials: The Nationwide Medicare Physician Supplier Procedure Summary Master Filesfor 1999 to 2004 were used to study the 4 Current Procedural Terminology®, Fourth Edition, codes for breastbiopsy. Using the Medicare specialty codes, physician providers were categorized as radiologists, surgeons, orothers. Procedure volumes for each of the 3 groups were tabulated for each year of the study, and trends wereassessed.
Results: Between 1999 and 2004, the breast biopsy utilization rate per 100,000 Medicare beneficiariesincreased by 43%. In 2004, a total of 144,697 breast biopsies were performed, of which 124,423 (86%) weredone with imaging guidance. From 1999 to 2004, procedure volume increased by 101% among radiologists,compared with 32% among surgeons. By 2004, radiologists performed 63% of all breast biopsies, comparedwith 32% by surgeons and 5% by others. Within the 2 codes that are specific for the use of imaging guidance,radiologists performed 72%.
Conclusions: Radiologists predominate in breast biopsies, and their role has gotten progressively stronger inrecent years.
Key Words: Breast biopsy, breast imaging, medical economics, diagnostic radiology, radiology, radiologists,socioeconomics issues
J Am Coll Radiol 2006;3:707-709. Copyright © 2006 American College of Radiology
wra
M
WaFce2(msfpmou
he introduction of percutaneous, image-guided inter-entional procedures often produces conflict with sur-eons or other specialists who had been previously accus-omed to using open surgical procedures to achieve theame ends and who sometimes view the new approachess threats to their practice. Breast biopsy is an example ofhis situation. In recent years, percutaneous breast biopsysing stereotactic mammographic techniques or ultra-ound guidance have replaced many open surgical biop-ies, and surgeons have espoused these new approaches1-3]. Our purpose in this investigation was to determine
Department of Radiology, Thomas Jefferson University Hospital and Jeffer-on Medical College, Philadelphia, Pa.
HealthHelp, Inc., Houston, Tex.
American College of Radiology, Reston, Va.
Corresponding author and reprints: David C. Levin, MD, Thomas Jeffer-on University Hospital, Department of Radiology, Main 1090, Philadelphia,A 19107;e-mail: [email protected].
This study was supported in part by a grant from Berlex Laboratories,
iontville, NJ.2006 American College of Radiology091-2182/06/$32.00 ● DOI 10.1016/j.jacr.2006.03.025
hat proportions of these procedures are performed byadiologists, surgeons, and other physicians, as well as toscertain recent trends in their utilization.
ATERIALS AND METHODS
e used the nationwide Centers for Medicare and Medic-id Services Physician Supplier Procedure Summary Masteriles for the period from 1999 to 2004. These databasesover all Medicare fee-for-service beneficiaries, but not thosenrolled in health maintenance organizations (12.4% in004). For every Current Procedural Terminology 4th ed,CPT-4)® code, the Physician Supplier Procedure Sum-ary Master Files provide information on the volume of
ervices performed nationwide each year in the Medicareee-for-service population, the specialties of the providerhysicians, and other useful information, such as reimburse-ents paid, place of service, region of the country, and so
n. We studied the 4 CPT-4® surgical procedure codessed to submit claims for breast biopsies, two of which use
maging guidance and two of which do not. These codes
707

aatgpcdfs1(
vOctpc
v1pcb
f
R
Tngi
a6aTfaifipgrssdpo
ac8gamggw
D
Twb
n.
708 Journal of the American College of Radiology/Vol. 3 No. 9 September 2006
nd their descriptors are shown in Table 1. The codes do notllow differentiation between biopsies performed with ul-rasound guidance and those using stereotactic mammo-raphic guidance. The corresponding supervision and inter-retation codes that are used in conjunction with surgicalodes were not tabulated, because that would have led toouble-counting procedures. We also did not include codesor fine needle aspiration (10021 and 10022), completeurgical excision of breast lesions (19120, 19125, and9126), or preoperative needle localization procedures19290 and 19291).
Using Medicare’s 108 physician specialty codes, pro-iders were classified as radiologists, surgeons, or others.ne of Medicare’s “specialty” codes is for a multispe-
ialty group practice, but with this code, it is not possibleo determine the specialty of the physician who actuallyrovided a service. In this study, claims from multispe-ialty groups were included in the “other” category.
Procedure volumes were tabulated for each of the 3 pro-ider groups, and utilization trend lines were plotted from999 to 2004. The overall utilization rate of breast biopsyer 100,000 Medicare fee-for-service beneficiaries was cal-ulated by dividing the number of procedures by the num-er of hundreds of thousands of beneficiaries each year.
All analyses were conducted using SAS version 9.1.3or Windows (SAS Institute Inc., Cary, NC).
ESULTS
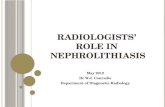
able 2 shows, for each year from 1999 to 2004, theumber of breast biopsies performed by radiologists, sur-eons, and others. The trends are illustrated graphicallyn Figure 1. The overall volume of biopsy procedures of
Table 1. CPT®-4 codes and descriptorsCode19100 Biopsy of breast; percutaneous, needle19101 Biopsy of breast; open, incisional19102 Biopsy of breast; percutaneous, needle19103 Biopsy of breast; percutaneous, automa
imaging guidance
Note: CPT®-4 � Current Procedural Terminology®, Fourth Editio
Table 2. Number of breast biopsies in the Medicare1999 2000 2001 20
Radiologists 45,143 52,042 62,357 74,Surgeons 35,410 37,192 40,904 43,Others 9,367 10,264 12,347 9,Total 89,929 99,498 115,608 128,
Note: “Others” include multispecialty groups, in which the spec
physicians aside from radiologists and surgeons.ll types rose from 89,929 in 1999 to 144,697 in 2004, a1% increase. However, part of this was accounted for byn increase in the number in the Medicare beneficiaries.he overall utilization rate per 100,000 (which corrects
or fluctuations in population size) of procedures withinll 4 codes rose from 268 in 1999 to 383 in 2004, anncrease of 43%. Among surgeons, the rate increasedrom 106 to 123 (�16%); among radiologists, the ratencreased from 135 to 241 (�79%). From 1999 to 2004,rocedure volume increased by 101% among radiolo-ists, compared with 32% among surgeons. In 1999,adiologists had performed 50% of breast biopsies andurgeons had performed 39%. By 2004, radiologists’hare had increased to 63%, while surgeons’ share hadeclined to 32%. The sharp divergence in accrual of newrocedures by radiologists and surgeons is clearly dem-nstrated in Figure 1.
Procedure volume in the 2 nonimaging codes (19100nd 19101) increased slightly from 1999 to 2000 but de-lined steadily thereafter. By 2004, a total of 124,423, or6% of all breast biopsies, were performed with imaginguidance (codes 19102 and 19103). These codes do notllow differentiation between procedures using stereotacticammographic localization and those using ultrasound
uidance. Among the 124,423 biopsies done with imaginguidance in 2004, radiologists performed 89,493 (72%),hereas surgeons performed 29,815 (24%).
ISCUSSION
he results of this study are encouraging for radiologistsho perform breast imaging. The rate at which breastiopsies are performed in the Medicare population is
escriptorre, not using imaging guidance
re, using imaging guidancevacuum assisted or rotating biopsy device, using
opulation2003 2004 % Change, 1999–2004
8 83,177 90,933 �1014 44,407 46,632 �328 7,305 7,132 –240 134,889 144,697 �61
of the physician provider cannot be determined, and all other
Dco
coted
p0297677440
ialty

iTobnpo1twm
t
pmsiecooa
bAosprct
R
1
2
3
Fosc
Levin et al/Practice Patterns and Recent Trends in Breast Biopsy 709
ncreasing (an increase of 43% between 1999 and 2004).he rate is increasing much more rapidly among radiol-gists than among surgeons (79% vs 16%, respectively,etween 1999 and 2004). The vast majority (86%) areow done with imaging guidance. In 2004, radiologistserformed 63% of all breast biopsy procedures and 72%f those performed with imaging guidance. Between999 and 2004, the accrual of new volume was substan-ially greater among radiologists than among surgeons,ith the result that by 2004, radiologists performed al-ost twice as many breast biopsies as surgeons.A limitation of our study is the fact that it covered only
010,00020,00030,00040,00050,00060,00070,00080,00090,000
100,000
1999 2000 2001 2002 2003 2004
radiolsurgeonsothers
ig 1. Volume of breast biopsies per year for radiol-gists (radiol), surgeons, and others. The vertical axishows procedure volume per year within the Medi-are fee-for-service population.
he Medicare population. However, it is unlikely that
ractice patterns would be greatly different in the com-ercially insured population. Another limitation is that
ome operative procedures begun by surgeons with thentent to do only incisional biopsies may instead havended up as complete excisions of the lesions. Such pro-edures would likely have been billed using codes for thepen surgical excision of a breast lesion (19120, 19125,r 19126). These codes do not allow the identification ofn initial intent to do only a biopsy.
In conclusion, the role of radiologists in percutaneousreast biopsy is strong and seems to be getting stronger.lthough one hears anecdotes of conflicts between radi-logists and surgeons over these procedures, it does noteem to pose a threat on a broad scale to breast imagingractices. Radiology trainees who are contemplating ca-eers in breast imaging can feel confident that they willontinue to have a major role in breast interventions inhe future.
EFERENCES
. Rubio IT, Henry-Tillman R, Klimberg VS. Surgical use of breast ultra-sound. Surg Clin North Am 2003;83:771-88.
. Nurko J, Edwards MJ. Image-guided breast surgery. Am J Surg 2005;190:221-7.
. White RR, Halperin TJ, Olson JA Jr, Soo MS, Bentley RC, Seigler HF.Impact of core-needle breast biopsy on the surgical management of mam-
mographic abnormalities. Ann Surg 2001;233:769-77.