Current Modalities for Invasive and Non Invasive Monitoring of Volume status in HF
18
11/4/13 www.medscape.com/viewarticle/765438_print www.medscape.com/viewarticle/765438_print 1/18 www.medscape.com Abstract and Introduction Abstract Heart failure (HF) represents a major health and economic burden worldwide. In spite of best current therapy, HF progresses with unpredictable episodes of deterioration that often require hospitalisation. These episodes are often preceded by accumulation or redistribution of fluid causing haemodynamic overload on the heart. Remote and telemonitoring of the HF patient, assessing symptoms and signs, thoracic impedance derived fluid status follow-up or direct haemodynamic measurements with chronic implanted devices are presently under investigation for the potential to detect impending HF decompensation early. The current evidence for volume status monitoring in HF using those novel management strategies is reviewed. Introduction Heart failure (HF) represents a major health and economic burden which is increasing with the ageing of populations around the world. In the USA, over 5.7 million people are currently estimated to live with HF. [1] In Europe, over 15 million people are estimated to have HF, and with a similar prevalence of asymptomatic left ventricular (LV) dysfunction, approximately 4% of the European population has either HF or LV dysfunction. [2] Despite advances in pharmacological and other therapies, rates for HF related hospital admission have not substantially decreased and represent a major driver for healthcare expenditure. [1] Recent data indicate that inhospital care accounts for approximately 60% of total HF costs. [3] Rehospitalisation for worsening HF predicts adverse prognosis, especially in the elderly, and is often initiated by intrathoracic fluid overload leading to symptomatic pulmonary congestion. [4 5] The vast majority of patients with acute decompensated HF (ADHF) has underlying chronic HF. Our current understanding of mechanisms contributing in ADHF is still insufficient but altered LV loading conditions and hypervolaemia are likely important contributing factors. Intrathoracic fluid accumulation frequently precedes hospital admission. Conceptually, continuous monitoring of fluid status in HF patients could aid identification of volume overload, thus providing an opportunity to intervene at an early stage and possibly avert hospital admission for ADHF. However, early clinical detection of ADHF is challenging. [6–8] Haemodynamic disturbances underlying ADHF may start weeks before the actual onset of typical HF symptoms such as fatigue, body weight gain or shortness of breath. Moreover, these are common, especially in the elderly without HF, and may be overlooked both by doctors and patients themselves. Diagnostic tools widely used in HF workup such as chest x-ray, cardiac catheterisation and conventional echocardiography are of limited use in determining the individual patient's fluid status. [7 9–11] Biomarkers in the assessment of clinical status of HF have emerged over the past two decades and are now routinely measured in various clinical settings. While the role of B type natriuretic peptide (BNP) in diagnosis as well as prognostification of HF is well established, there has been ongoing debate regarding its role as a guide to monitoring and adjustment of HF therapy. Recent meta-analyses of major randomised controlled trials (RCTs) in the field have suggested a mortality benefit in patients with monitored BNP, presumably due to enhanced use of drugs such as angiotensin converting enzyme inhibitors (ACEI) and β blockers in the cohort exhibiting biomarker increases. [12 13] Another report concluded that N terminal BNP guided HF specialist care in addition to home based nurse care was cost effective and cheaper than standard care. [14] There are conflicting data as to whether BNP guided HF care reduces rehospitalisation rates. [13 15] BNPs may not be sensitive enough tools to detect rapidly decompensating HF. In ADHF, acute changes in LV filling pressures will likely not be reflected by simultaneous changes in NPs due to their long half-lives, thus limiting their clinical utility in that setting. Furthermore, patient characteristics (ie, age, gender, body weight) may influence plasma levels of BNP and other NPs, making interpretation even more difficult. [9 10] Current Modalities for Invasive and Non- invasive Monitoring of Volume Status in Heart Failure Thomas G von Lueder, Henry Krum Heart. 2012;98(13):967-973.
-
Upload
drucsamal -
Category
Healthcare
-
view
102 -
download
1
Transcript of Current Modalities for Invasive and Non Invasive Monitoring of Volume status in HF

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 1/18
www.medscape.com
Abstract and Introduction
Abstract
Heart failure (HF) represents a major health and economic burden worldwide. In spite of best current therapy, HF
progresses with unpredictable episodes of deterioration that often require hospitalisation. These episodes are
often preceded by accumulation or redistribution of fluid causing haemodynamic overload on the heart. Remote
and telemonitoring of the HF patient, assessing symptoms and signs, thoracic impedance derived fluid status
follow-up or direct haemodynamic measurements with chronic implanted devices are presently under investigation
for the potential to detect impending HF decompensation early. The current evidence for volume status monitoring
in HF using those novel management strategies is reviewed.
Introduction
Heart failure (HF) represents a major health and economic burden which is increasing with the ageing of
populations around the world. In the USA, over 5.7 million people are currently estimated to live with HF.[1] In
Europe, over 15 million people are estimated to have HF, and with a similar prevalence of asymptomatic left
ventricular (LV) dysfunction, approximately 4% of the European population has either HF or LV dysfunction.[2]
Despite advances in pharmacological and other therapies, rates for HF related hospital admission have not
substantially decreased and represent a major driver for healthcare expenditure.[1] Recent data indicate that
inhospital care accounts for approximately 60% of total HF costs.[3] Rehospitalisation for worsening HF predicts
adverse prognosis, especially in the elderly, and is often initiated by intrathoracic fluid overload leading to
symptomatic pulmonary congestion.[4 5] The vast majority of patients with acute decompensated HF (ADHF) has
underlying chronic HF. Our current understanding of mechanisms contributing in ADHF is still insufficient but
altered LV loading conditions and hypervolaemia are likely important contributing factors. Intrathoracic fluid
accumulation frequently precedes hospital admission. Conceptually, continuous monitoring of fluid status in HF
patients could aid identification of volume overload, thus providing an opportunity to intervene at an early stage and
possibly avert hospital admission for ADHF. However, early clinical detection of ADHF is challenging.[6–8]
Haemodynamic disturbances underlying ADHF may start weeks before the actual onset of typical HF symptoms
such as fatigue, body weight gain or shortness of breath. Moreover, these are common, especially in the elderly
without HF, and may be overlooked both by doctors and patients themselves. Diagnostic tools widely used in HF
workup such as chest x-ray, cardiac catheterisation and conventional echocardiography are of limited use in
determining the individual patient's fluid status.[7 9–11]
Biomarkers in the assessment of clinical status of HF have emerged over the past two decades and are now
routinely measured in various clinical settings. While the role of B type natriuretic peptide (BNP) in diagnosis as
well as prognostification of HF is well established, there has been ongoing debate regarding its role as a guide to
monitoring and adjustment of HF therapy. Recent meta-analyses of major randomised controlled trials (RCTs) in
the field have suggested a mortality benefit in patients with monitored BNP, presumably due to enhanced use of
drugs such as angiotensin converting enzyme inhibitors (ACEI) and β blockers in the cohort exhibiting biomarker
increases.[12 13] Another report concluded that N terminal BNP guided HF specialist care in addition to home
based nurse care was cost effective and cheaper than standard care.[14] There are conflicting data as to whether
BNP guided HF care reduces rehospitalisation rates.[13 15] BNPs may not be sensitive enough tools to detect
rapidly decompensating HF. In ADHF, acute changes in LV filling pressures will likely not be reflected by
simultaneous changes in NPs due to their long half-lives, thus limiting their clinical utility in that setting.
Furthermore, patient characteristics (ie, age, gender, body weight) may influence plasma levels of BNP and other
NPs, making interpretation even more difficult.[9 10]
Current Modalities for Invasive and Non-invasive Monitoring of Volume Status in HeartFailureThomas G von Lueder, Henry Krum
Heart. 2012;98(13):967-973.

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 2/18
Therefore, novel strategies to more precisely assess and monitor fluid status in HF have been explored over recent
years. Some of those developments seem to hold promise in improving early detection of which patients will likely
be readmitted for ADHF, with the potential to intervene early. Bringing down HF hospitalisation rates may not only
improve patient quality of life but also reduce longer term clinical outcomes and alleviate the enormous HF related
cost to society.
This review seeks to summarise current knowledge on integrating fluid status monitoring into the overall
management of HF patients.
Emerging Strategies to Monitor Fluid Status in HF
Home and Telemonitoring
Given the importance of hypervolaemia in HF related events, monitoring of weight and HF specific symptoms as a
surrogate for fluid status has received considerable attention in recent years. Efforts have been made to
systematically and continuously assess fluid status associated variables either at clinical follow-ups or through
structured telephone calls. However, it has been unclear whether those strategies translate into clinical benefit.
Several recent studies have sought to establish evidence for such a benefit ( ).
Table 1. Overview of important studies of fluid monitoring in heart failure
Study N
Patient
characteristics or
key inclusion
criteria
Intervention
Follow-
up
(months)
Outcome or main findings
I. Home and remote telemonitoring
WHARF16 280
NYHA III–IV + EF
≤35%HF + HF
hospitalisation
RTM (AlereNet
system)6
No effect on rehospitalisations.
Greatly reduced mortality
HHH study17 461
NYHA II–IV + EF
≤40% + HF
hospitalisation
NTS or
NTS+RTM
strategies (3
arms)
12 Negative
HOME-HF18 182NYHA II–IV + HF
hospitalisationRTM 6
Negative, but fewer unplanned
hospitalisations
TEN-HMS19 20 426
HF symptoms +
EF ≤40% + HF
hospitalisation
RTM or NTS 8Negative, but lower 1 year
mortality by NTS and RTM
TELE-HF21 1653 HF hospitalisation RTM 6 Negative
TIM-HF22 710
NYHA II–III + EF
≤35% + HF
hospitalisation or
EF ≤25%
RTM 26 Negative
Cochrane23 8323
Meta-analysis of
25 trials (RTM,
n=2710; STS,
n=5613)
RTM and/or STS NA
Reduced mortality and HF
hospitalisations; improved QOL
(note: TIM-HF22 and TELE-HF21
not included)
II. Impedance monitoring (ICD or CRT-D)
MIDHeFT24 34NYHA III–IV + HF
eventsFeasibility study 21
Impedance inversely correlated
with PCWP

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 3/18
Maines et al 25 54NYHA II–IV + EF
24%
Case control
study12 HF hospitalisations reduced
PARTNERS-HF26 694
CRT-D + NYHA III–
IV + EF ≤35% +
QRS> 130 ms
Observational
prospective
study
12
Combined diagnostic HF
algorithm identified patients at
risk for ADHF
FAST27 156
CRT-D or ICD +
NYHA III–IV + EF
≤35%
Prospective
study18
Impedance change superior to
acute weight changes
IMPATTO28 111 HF + EF <35%Registry (no
intervention)14
Impedance data correlated with
BNP levels and
echocardiography data (E
deceleration time)
SENSE-HF29 501
Previous HF
hospitalisation
requiring
intravenous
treatment
Prospective
double blind
study
24FI had low sensitivity and PPV
for HF hospitalisation
DOT-HF30 335
NYHA II–IV + EF ≤
35% + previous HF
hospitalisation
Unblinded RCT 15
Negative. Underpowered. More
hospitalisations in intervention
group
OptiLink HF
study31 1000NYHA II-III + EF
<35%RCT 18
Ongoing. Planned inclusion,
n=1000
III. Implantable haemodynamic monitors
Permanent RV
IHM system32 32 NYHA III–IV
Observational
prospective
study
17RV pressure increases preceded
hospitalisations
COMPASS33 274
NYHA III–IV +
previous HF
hospitalisation
RVOT IHM
(CHRONICLE) all
patients; single
blinded
6Non-significant reduction of HF
events. Safety endpoints met
REDUCE-HF34 35 400
NYHA II–III +
previous HF
hospitalisation +
ICD indication
RVOT IHM
linked to ICD (all
patients)
6
Ended prematurely for lead
problems. No effects on HF
events (but underpowered)
HOMEOSTASIS36 40
NYHA III–IV +
previous HF
hospitalisation
LAP catheter
(HeartPOD) all
patients
25Increased event free survival,
lower LAP
CHAMPION37 38 550
NYHA III +
previous HF
hospitalisation
PA catheter
versus standard
care (single
blinded)
6
Reduced and shorter HF
hospitalisations, lowered PAP,
more medication changes in
intervention group
LAPTOP-HF* 730
NYHA III +
previous HF
hospitalisation
LAP catheter or
CRT-D12 Ongoing
* http://www.clinicaltrials.gov, NCT01121107.
ADHF, acute decompensated heart failure; BNP, B type natriuretic peptide; CRT-D, cardiac resynchronisation

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 4/18
therapy device; EF, ejection fraction; FI, fluid index; HF, heart failure; ICD, cardioverter defibrillator; IHM,
implantable haemodynamic monitors; LAP, left atrial pressure; NTS, nurse telephone support; NYHA, New York
Heart Association (functional class); PA, pulmonary artery; PAP, pulmonary artery pressure; PCWP, pulmonary
capillary wedge pressure; PPV, positive predictive value; QOL, quality of life; RCT, randomised controlled trial;
RTM, remote telemonitoring; RV, right ventricular; RVOT, right ventricular outflow tract; STS, structured telephone
support.
The Weight Monitoring in HF (WHARF) trial was a large multicentre RCT of a technology based daily weight and
symptom monitoring system.[16] It included HF patients in New York Heart Association (NYHA) class III or IV.
The trial failed to meet its primary endpoint of reduced 6 month rehospitalisation rates but demonstrated a
substantial reduction in the secondary endpoint of mortality.
The Trans-European Network-Home Care Management System (TEN-HMS) study was a large scale RCT
comparing home based telemonitoring services or nurse based telephone support to usual care.[19 20] In TEN-
HMS, telemonitoring failed to meet its primary endpoints of days lost to death or hospitalisation improvements of
patient quality of life, but both interventions led to lower 1 year mortality than usual care.
A recent report by the Cochrane Review Group compared structured telephone interview and telemonitoring to
standard care.[23] That meta-analysis comprised over 8000 patients and included 11 studies (all published before
the end of 2008) which evaluated telemonitoring (total of 2710 subjects) and 16 which evaluated structured
telephone support (5613 subjects). Telemonitoring reduced all-cause mortality while structured telephone support
showed a non-significant trend. Both interventions reduced HF hospitalisations. Heterogenous protocols and the
small sample size of most of the trials included in that report warrant caution when interpreting the ascribed
benefits.
Further illustrating the limitations of pooled efficacy data, two very recent large RCTs (not included in the
aforementioned Cochrane review) have raised doubts as to the benefits of telemonitoring. First, the Telemedicine
to Improve Mortality in Heart Failure (TIM-HF) study evaluated 710 patients with NYHA class II or III HF, LV
ejection fraction (EF) ≤35% and on optimal medical therapy.[22] Using portable devices, ECG, blood pressure and
body weight measurements of the telemonitored cohort (n=354) were reviewed daily by telemedical centres. After
a mean follow-up of 26 months, telemonitoring had no significant effect on all-cause mortality, cardiovascular
death or HF hospitalisation compared with patients receiving usual care (n=356). In the even larger telemonitoring
for HF (TELE-HF) trial, 826 patients recently hospitalised for HF were randomised to daily telemonitoring by
means of a telephone based interactive voice response system collecting data on weight and symptoms, and
compared with 827 patients on standard care.[21] Data in the telemonitored cohort were reviewed by the patients'
clinicians. The primary endpoint was readmission for any reason or death from any cause within 180 days after
enrolment. Secondary endpoints included hospitalisation for HF, number of days in the hospital and number of
hospitalisations. Again, telemonitoring in TELE-HF did not improve any of these outcomes. Moreover, no subgroup
(age, gender, EF, etc) could be identified that benefitted from the intervention. Importantly, adherence to the
intervention decreased from an initial 90.2% to only 55.1% by 6 months, and almost 15% of patients never
actually used the device. There was no per protocol analysis to allow conclusions on potential benefits in those
study subjects that adhered to the intervention. TELE-HF did not report information on medication changes or on
how clinicians used information gained from telemonitoring.
In an effort to refine monitoring of fluid status associated parameters, a simple rule of thumb algorithm was
retrospectively compared with a sophisticated moving average convergence divergence algorithm to detect
abnormal weight gain in telemonitored HF patients.[20] While the moving average convergence divergence
algorithm was much more specific than the rule of thumb algorithm in detecting weight gain, overall sensitivity was
rather poor. As a significant number of episodes of worsening HF in that cohort were not associated with weight
gain at all, the authors concluded that telemonitoring of weight gain alone may be of limited use for HF
management.
Together, current evidence on home based telemonitoring strategies does not definitely point to consistent
additional benefits above standard care for HF patients.
11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 5/18
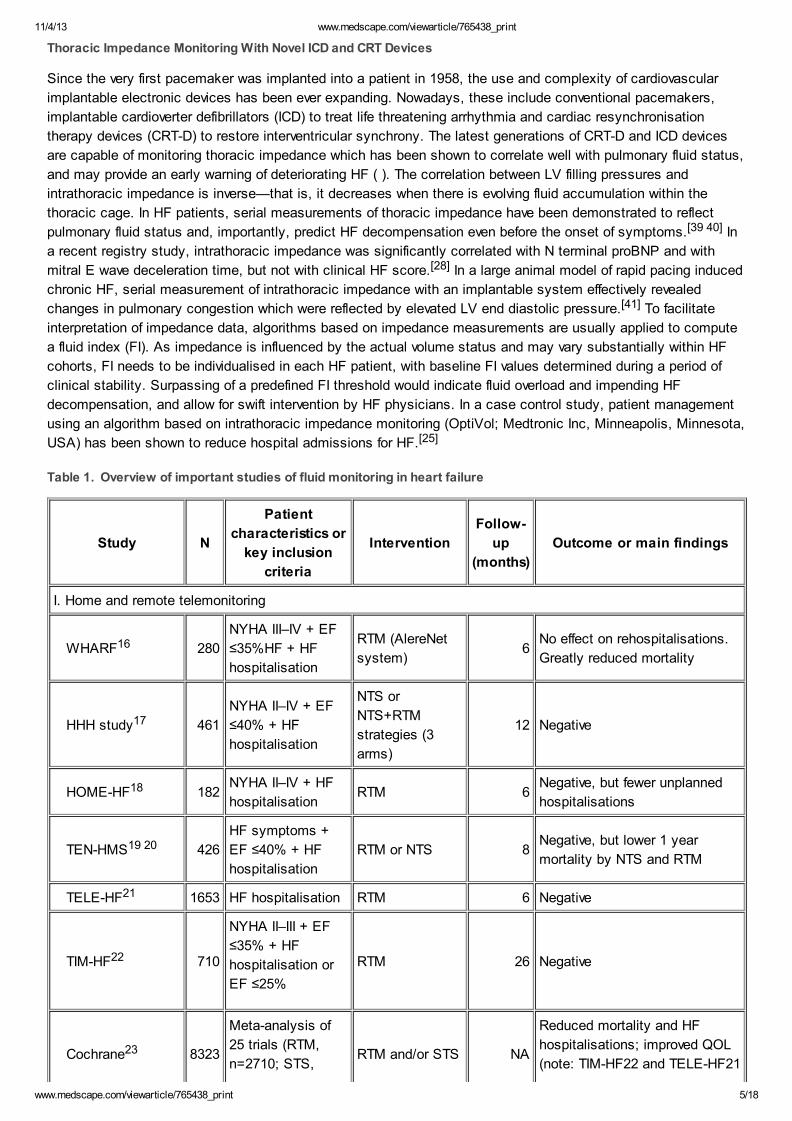
Thoracic Impedance Monitoring With Novel ICD and CRT Devices
Since the very first pacemaker was implanted into a patient in 1958, the use and complexity of cardiovascular
implantable electronic devices has been ever expanding. Nowadays, these include conventional pacemakers,
implantable cardioverter defibrillators (ICD) to treat life threatening arrhythmia and cardiac resynchronisation
therapy devices (CRT-D) to restore interventricular synchrony. The latest generations of CRT-D and ICD devices
are capable of monitoring thoracic impedance which has been shown to correlate well with pulmonary fluid status,
and may provide an early warning of deteriorating HF ( ). The correlation between LV filling pressures and
intrathoracic impedance is inverse—that is, it decreases when there is evolving fluid accumulation within the
thoracic cage. In HF patients, serial measurements of thoracic impedance have been demonstrated to reflect
pulmonary fluid status and, importantly, predict HF decompensation even before the onset of symptoms.[39 40] In
a recent registry study, intrathoracic impedance was significantly correlated with N terminal proBNP and with
mitral E wave deceleration time, but not with clinical HF score.[28] In a large animal model of rapid pacing induced
chronic HF, serial measurement of intrathoracic impedance with an implantable system effectively revealed
changes in pulmonary congestion which were reflected by elevated LV end diastolic pressure.[41] To facilitate
interpretation of impedance data, algorithms based on impedance measurements are usually applied to compute
a fluid index (FI). As impedance is influenced by the actual volume status and may vary substantially within HF
cohorts, FI needs to be individualised in each HF patient, with baseline FI values determined during a period of
clinical stability. Surpassing of a predefined FI threshold would indicate fluid overload and impending HF
decompensation, and allow for swift intervention by HF physicians. In a case control study, patient management
using an algorithm based on intrathoracic impedance monitoring (OptiVol; Medtronic Inc, Minneapolis, Minnesota,
USA) has been shown to reduce hospital admissions for HF.[25]
Table 1. Overview of important studies of fluid monitoring in heart failure
Study N
Patient
characteristics or
key inclusion
criteria
Intervention
Follow-
up
(months)
Outcome or main findings
I. Home and remote telemonitoring
WHARF16 280
NYHA III–IV + EF
≤35%HF + HF
hospitalisation
RTM (AlereNet
system)6
No effect on rehospitalisations.
Greatly reduced mortality
HHH study17 461
NYHA II–IV + EF
≤40% + HF
hospitalisation
NTS or
NTS+RTM
strategies (3
arms)
12 Negative
HOME-HF18 182NYHA II–IV + HF
hospitalisationRTM 6
Negative, but fewer unplanned
hospitalisations
TEN-HMS19 20 426
HF symptoms +
EF ≤40% + HF
hospitalisation
RTM or NTS 8Negative, but lower 1 year
mortality by NTS and RTM
TELE-HF21 1653 HF hospitalisation RTM 6 Negative
TIM-HF22 710
NYHA II–III + EF
≤35% + HF
hospitalisation or
EF ≤25%
RTM 26 Negative
Cochrane23 8323
Meta-analysis of
25 trials (RTM,
n=2710; STS,RTM and/or STS NA
Reduced mortality and HF
hospitalisations; improved QOL
(note: TIM-HF22 and TELE-HF21

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 6/18
n=5613) not included)
II. Impedance monitoring (ICD or CRT-D)
MIDHeFT24 34NYHA III–IV + HF
eventsFeasibility study 21
Impedance inversely correlated
with PCWP
Maines et al 25 54NYHA II–IV + EF
24%
Case control
study12 HF hospitalisations reduced
PARTNERS-HF26 694
CRT-D + NYHA III–
IV + EF ≤35% +
QRS> 130 ms
Observational
prospective
study
12
Combined diagnostic HF
algorithm identified patients at
risk for ADHF
FAST27 156
CRT-D or ICD +
NYHA III–IV + EF
≤35%
Prospective
study18
Impedance change superior to
acute weight changes
IMPATTO28 111 HF + EF <35%Registry (no
intervention)14
Impedance data correlated with
BNP levels and
echocardiography data (E
deceleration time)
SENSE-HF29 501
Previous HF
hospitalisation
requiring
intravenous
treatment
Prospective
double blind
study
24FI had low sensitivity and PPV
for HF hospitalisation
DOT-HF30 335
NYHA II–IV + EF ≤
35% + previous HF
hospitalisation
Unblinded RCT 15
Negative. Underpowered. More
hospitalisations in intervention
group
OptiLink HF
study31 1000NYHA II-III + EF
<35%RCT 18
Ongoing. Planned inclusion,
n=1000
III. Implantable haemodynamic monitors
Permanent RV
IHM system32 32 NYHA III–IV
Observational
prospective
study
17RV pressure increases preceded
hospitalisations
COMPASS33 274
NYHA III–IV +
previous HF
hospitalisation
RVOT IHM
(CHRONICLE) all
patients; single
blinded
6Non-significant reduction of HF
events. Safety endpoints met
REDUCE-HF34 35 400
NYHA II–III +
previous HF
hospitalisation +
ICD indication
RVOT IHM
linked to ICD (all
patients)
6
Ended prematurely for lead
problems. No effects on HF
events (but underpowered)
HOMEOSTASIS36 40
NYHA III–IV +
previous HF
hospitalisation
LAP catheter
(HeartPOD) all
patients
25Increased event free survival,
lower LAP
CHAMPION37 38 550
NYHA III +
previous HF
hospitalisation
PA catheter
versus standard
care (single
blinded)
6
Reduced and shorter HF
hospitalisations, lowered PAP,
more medication changes in
intervention group

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 7/18
LAPTOP-HF* 730 NYHA III +
previous HF
hospitalisation
LAP catheter or
CRT-D12 Ongoing
* http://www.clinicaltrials.gov, NCT01121107.
ADHF, acute decompensated heart failure; BNP, B type natriuretic peptide; CRT-D, cardiac resynchronisation
therapy device; EF, ejection fraction; FI, fluid index; HF, heart failure; ICD, cardioverter defibrillator; IHM,
implantable haemodynamic monitors; LAP, left atrial pressure; NTS, nurse telephone support; NYHA, New York
Heart Association (functional class); PA, pulmonary artery; PAP, pulmonary artery pressure; PCWP, pulmonary
capillary wedge pressure; PPV, positive predictive value; QOL, quality of life; RCT, randomised controlled trial;
RTM, remote telemonitoring; RV, right ventricular; RVOT, right ventricular outflow tract; STS, structured telephone
support.
The Medtronic Impedance in Diagnostics in HF Trial (MIDHeFT) in patients with NYHA classes III and IV HF
showed a sensitivity of 77% for FI algorithms to detect hospitalisation for fluid overload.[24] The Fluid Accumulation
Status Trial (FAST) compared serial measurements of thoracic impedance with weight changes in 156 NYHA
class II or III HF patients and implantable ICD or CRT-D, with a mean follow-up of 537 days.[27] FAST
demonstrated that impedance data were more sensitive than weight gain in predicting HF decompensation (76 vs
23%). The relatively low specificity improved when impedance data were combined with weight monitoring. The
Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients With HF
(PARTNERS-HF) study prospectively evaluated the utility of combined diagnostic algorithm including impedance
data to predict HF hospitalisations in patients with NYHA classes III and IV HF, reduced LV EF, broad QRS and
who had a CRT-D (Medtronic Inc). A total of 694 patients were followed for almost 12 months in this unblinded
observational study. The impedance based algorithm identified a cohort at high risk of experiencing a HF event
within the subsequent month.[26] Importantly, there seems to be a link between patient reported HF self-care and
the likelihood of an FI threshold crossing event.[42]
In most of these trials, the predefined FI algorithm led to a considerable number of false positive alerts and likely
increased healthcare utilisation. This lack of specificity may present an obstacle to broader implementation of the
technology into clinical practice. Current efforts to develop improved FI based algorithms demonstrated lower false
positive alerts at similar sensitivity.[43]
The recent Sensitivity of the InSync Sentry OptiVol Feature for the Prediction of HF (SENSE-HF) study was a
large prospective, multicentre, double blind study that evaluated an impedance based algorithm, OptiVol, in 501
NYHA class II and class III HF patients with CRT-D.[29] Using OptiVol, the trial showed a low sensitivity of 42%
and low positive predictive value of only 38% for future HF events. The Diagnostic Outcome Trial in HF (DOT-HF)
was a large prospective phase IV RCT designed to test whether monitoring of intrathoracic impedance (OptiVol)
could reduce morbidity and mortality in patients with chronic NYHA classes II–IV HF.[44] All study subjects were
implanted with an ICD or CRT-D capable of monitoring impedance (Medtronic Inc), and randomised to have all
device based information (including audible alerts for preset fluid threshold crossings) available to patients and
doctors (access group) or to a control group without that information.[30] The primary endpoint was a composite of
all-cause mortality and HF hospitalisation, and occurred in 48 of 168 (29%) patients in the access arm versus 33
of 167 (20%) in the control arm (p=0.063). Even if the trial was terminated early due to to low enrolment rates
(only 336 of intended 2400 subjects were included), post hoc futility analysis deemed it unlikely that better
recruitment would have changed overall outcome. The currently ongoing OptiLink-HF Study is another substantial
study in the field. Approximately 1000 patients will be required to demonstrate a 30% reduction in the primary
outcome (composite of all-cause death or cardiovascular hospitalisation).[31]
HF Management Based on Invasive Haemodynamic Monitoring
Supranormal LV filling pressures are a hallmark and one of the principal haemodynamic abnormalities in HF
decompensation. The relationship between cardiac pressures and HF events has therefore been the subject of
longstanding interest and research. Pulmonary artery catheterisation (PAC) using thermodilution/Swan Ganz
catheters has been the undisputed gold standard for invasive haemodynamic assessment. Early observational
studies and registry data including patients with ADHF or cardiogenic shock after acute myocardial infarction have

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 8/18
not been able to demonstrate beneficial effects of the use of PAC.[45–47] However, most of those reports stem
from the percutaneous coronary intervention (pre-PCI) (and pre-thrombolysis) era, and the lack of randomisation
usually meant that the most seriously ill patients (with the worst prognosis) were more likely to undergo PAC.
Accordingly, the importance of PAC in a contemporary HF setting is unclear. The Evaluation Study of Congestive
HF and Pulmonary Artery Catheterisation Effectiveness (ESCAPE) study randomised 433 patients hospitalised
with severe symptomatic HF to receive therapy guided by PAC derived haemodynamic data and clinical
assessment versus therapy based on clinical assessment alone. ESCAPE showed that addition of PAC to
clinical assessment did not affect overall mortality and hospitalisation.[48] Significantly more patients in the PAC
group (21.9 vs 11.5%) experienced an inhospital adverse event, but inhospital and 30 day mortality was not
affected by the use of PAC. In contrast with the apparent lack of benefit of PAC guided therapy in ADHF, the
relevance in chronic HF is unclear.
Implantable Continuous Haemodynamic Monitoring Devices
During the past decade, permanently implantable devices have emerged that provide accurate and timely long
term haemodynamic data ( ). Among these implantable continuous haemodynamic monitoring (ICHM) devices are
those that chronically assess pressures in the right ventricle (RV), pulmonary artery and left atrium.[32 49–51]
Table 1. Overview of important studies of fluid monitoring in heart failure
Study N
Patient
characteristics or
key inclusion
criteria
Intervention
Follow-
up
(months)
Outcome or main findings
I. Home and remote telemonitoring
WHARF16 280
NYHA III–IV + EF
≤35%HF + HF
hospitalisation
RTM (AlereNet
system)6
No effect on rehospitalisations.
Greatly reduced mortality
HHH study17 461
NYHA II–IV + EF
≤40% + HF
hospitalisation
NTS or
NTS+RTM
strategies (3
arms)
12 Negative
HOME-HF18 182NYHA II–IV + HF
hospitalisationRTM 6
Negative, but fewer unplanned
hospitalisations
TEN-HMS19 20 426
HF symptoms +
EF ≤40% + HF
hospitalisation
RTM or NTS 8Negative, but lower 1 year
mortality by NTS and RTM
TELE-HF21 1653 HF hospitalisation RTM 6 Negative
TIM-HF22 710
NYHA II–III + EF
≤35% + HF
hospitalisation or
EF ≤25%
RTM 26 Negative
Cochrane23 8323
Meta-analysis of
25 trials (RTM,
n=2710; STS,
n=5613)
RTM and/or STS NA
Reduced mortality and HF
hospitalisations; improved QOL
(note: TIM-HF22 and TELE-HF21
not included)
II. Impedance monitoring (ICD or CRT-D)
MIDHeFT24 34NYHA III–IV + HF
eventsFeasibility study 21
Impedance inversely correlated
with PCWP

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 9/18
Maines et al 25 54NYHA II–IV + EF
24%
Case control
study12 HF hospitalisations reduced
PARTNERS-HF26 694
CRT-D + NYHA III–
IV + EF ≤35% +
QRS> 130 ms
Observational
prospective
study
12
Combined diagnostic HF
algorithm identified patients at
risk for ADHF
FAST27 156
CRT-D or ICD +
NYHA III–IV + EF
≤35%
Prospective
study18
Impedance change superior to
acute weight changes
IMPATTO28 111 HF + EF <35%Registry (no
intervention)14
Impedance data correlated with
BNP levels and
echocardiography data (E
deceleration time)
SENSE-HF29 501
Previous HF
hospitalisation
requiring
intravenous
treatment
Prospective
double blind
study
24FI had low sensitivity and PPV
for HF hospitalisation
DOT-HF30 335
NYHA II–IV + EF ≤
35% + previous HF
hospitalisation
Unblinded RCT 15
Negative. Underpowered. More
hospitalisations in intervention
group
OptiLink HF
study31 1000NYHA II-III + EF
<35%RCT 18
Ongoing. Planned inclusion,
n=1000
III. Implantable haemodynamic monitors
Permanent RV
IHM system32 32 NYHA III–IV
Observational
prospective
study
17RV pressure increases preceded
hospitalisations
COMPASS33 274
NYHA III–IV +
previous HF
hospitalisation
RVOT IHM
(CHRONICLE) all
patients; single
blinded
6Non-significant reduction of HF
events. Safety endpoints met
REDUCE-HF34 35 400
NYHA II–III +
previous HF
hospitalisation +
ICD indication
RVOT IHM
linked to ICD (all
patients)
6
Ended prematurely for lead
problems. No effects on HF
events (but underpowered)
HOMEOSTASIS36 40
NYHA III–IV +
previous HF
hospitalisation
LAP catheter
(HeartPOD) all
patients
25Increased event free survival,
lower LAP
CHAMPION37 38 550
NYHA III +
previous HF
hospitalisation
PA catheter
versus standard
care (single
blinded)
6
Reduced and shorter HF
hospitalisations, lowered PAP,
more medication changes in
intervention group
LAPTOP-HF* 730
NYHA III +
previous HF
hospitalisation
LAP catheter or
CRT-D12 Ongoing
* http://www.clinicaltrials.gov, NCT01121107.
ADHF, acute decompensated heart failure; BNP, B type natriuretic peptide; CRT-D, cardiac resynchronisation

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 10/18
therapy device; EF, ejection fraction; FI, fluid index; HF, heart failure; ICD, cardioverter defibrillator; IHM,
implantable haemodynamic monitors; LAP, left atrial pressure; NTS, nurse telephone support; NYHA, New York
Heart Association (functional class); PA, pulmonary artery; PAP, pulmonary artery pressure; PCWP, pulmonary
capillary wedge pressure; PPV, positive predictive value; QOL, quality of life; RCT, randomised controlled trial;
RTM, remote telemonitoring; RV, right ventricular; RVOT, right ventricular outflow tract; STS, structured telephone
support.
Right Ventricular Pressure Monitoring In a feasibility study, 32 patients with HF received a permanent RV
ICHM system (Chronicle; Medtronic Inc) similar to a single lead RV pacemaker. The ICHM delivered accurate RV
pressure data over time that correlated well with LV filling pressures obtained from conventional PAC.[49] In this
cohort, hospitalisations before using ICHM data for clinical management averaged 1.08 per patient year and
decreased to 0.47 per patient year (57% reduction; p<0.01) after integration of RV pressure data into the follow-
up.[32] The subsequent landmark Chronicle Offers Management to Patients with Advanced Signs and Symptoms
of HF (COMPASS) trial sought to establish whether integration of RV ICHM derived pressures would reduce HF
morbidity.[33] COMPASS was a prospective, multicentre, randomised, single blind, parallel controlled trial and
included 274 NYHA class III/IV HF patients with a previous HF hospitalisation, all of whom were implanted with
the same ICHM as above. Subjects were randomised to an ICHM guided HF management strategy or control
group follow-up without ICHM data available. ICHM guided HF management in COMPASS did not reduce HF
related events compared with standard care which was probably the reason why the Food and Drug
Administration has not thus far approved the technology.[33 52] This surprising lack of efficacy deserves further
discussion. Sample size calculations were based on an event rate of at least 1.2 per 6 patient months in the
control group to show a 30% reduction in HF related events with 80% power. The trial, however, reported an event
rate as low as 0.85 per 6 patient months in the control group, being further (non-significantly) reduced by 21% to
0.67 in the intervention group. It is noteworthy that the HF event rate in the control group decreased from 1.8 per 6
patient months (ie, by over 50%) after enrolment, probably driven by the very tight follow-up (at almost weekly
intervals) which seems unrealistic to achieve in daily clinical practice.[53] Even if technically underpowered to meet
its efficacy endpoints, COMPASS provided novel important insights into the pathophysiological changes during
decompensation in patients with HF with reduced and preserved EF.[52] Pressure increases preceded HF related
events by 3–4 weeks, and interestingly, no significant body weight changes were found in relation to HF events.
Data on medication changes in relation to ICHM data are yet to be published and will further our understanding of
HF management guided by RV haemodynamics. Very recently, the Reducing Decompensation Events Utilising
Intracardiac Pressures in Patients with Chronic HF (REDUCE-HF) trial was halted with only 400 of the planned
1300 patients enrolled, due to problems with the pressure sensor leads seen in earlier studies.[34] The HF event
rate was even lower than in COMPASS, probably due to a healthier patient cohort ( ), and the device had not led
to reduced hospitalisation or other HF events when it was stopped.[35]
Table 1. Overview of important studies of fluid monitoring in heart failure
Study N
Patient
characteristics or
key inclusion
criteria
Intervention
Follow-
up
(months)
Outcome or main findings
I. Home and remote telemonitoring
WHARF16 280
NYHA III–IV + EF
≤35%HF + HF
hospitalisation
RTM (AlereNet
system)6
No effect on rehospitalisations.
Greatly reduced mortality
HHH study17 461
NYHA II–IV + EF
≤40% + HF
hospitalisation
NTS or
NTS+RTM
strategies (3
arms)
12 Negative
HOME-HF18 182
NYHA II–IV + HF
hospitalisation RTM 6
Negative, but fewer unplanned
hospitalisations

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 11/18
TEN-HMS19 20 426
HF symptoms +
EF ≤40% + HF
hospitalisation
RTM or NTS 8Negative, but lower 1 year
mortality by NTS and RTM
TELE-HF21 1653 HF hospitalisation RTM 6 Negative
TIM-HF22 710
NYHA II–III + EF
≤35% + HF
hospitalisation or
EF ≤25%
RTM 26 Negative
Cochrane23 8323
Meta-analysis of
25 trials (RTM,
n=2710; STS,
n=5613)
RTM and/or STS NA
Reduced mortality and HF
hospitalisations; improved QOL
(note: TIM-HF22 and TELE-HF21
not included)
II. Impedance monitoring (ICD or CRT-D)
MIDHeFT24 34NYHA III–IV + HF
eventsFeasibility study 21
Impedance inversely correlated
with PCWP
Maines et al 25 54NYHA II–IV + EF
24%
Case control
study12 HF hospitalisations reduced
PARTNERS-HF26 694
CRT-D + NYHA III–
IV + EF ≤35% +
QRS> 130 ms
Observational
prospective
study
12
Combined diagnostic HF
algorithm identified patients at
risk for ADHF
FAST27 156
CRT-D or ICD +
NYHA III–IV + EF
≤35%
Prospective
study18
Impedance change superior to
acute weight changes
IMPATTO28 111 HF + EF <35%Registry (no
intervention)14
Impedance data correlated with
BNP levels and
echocardiography data (E
deceleration time)
SENSE-HF29 501
Previous HF
hospitalisation
requiring
intravenous
treatment
Prospective
double blind
study
24FI had low sensitivity and PPV
for HF hospitalisation
DOT-HF30 335
NYHA II–IV + EF ≤
35% + previous HF
hospitalisationUnblinded RCT 15
Negative. Underpowered. More
hospitalisations in intervention
group
OptiLink HF
study31 1000NYHA II-III + EF
<35%RCT 18
Ongoing. Planned inclusion,
n=1000
III. Implantable haemodynamic monitors
Permanent RV
IHM system32 32 NYHA III–IV
Observational
prospective
study
17RV pressure increases preceded
hospitalisations
COMPASS33 274
NYHA III–IV +
previous HF
hospitalisation
RVOT IHM
(CHRONICLE) all
patients; single
blinded
6Non-significant reduction of HF
events. Safety endpoints met

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 12/18
REDUCE-HF34 35 400
NYHA II–III +
previous HF
hospitalisation +
ICD indication
RVOT IHM
linked to ICD (all
patients)
6
Ended prematurely for lead
problems. No effects on HF
events (but underpowered)
HOMEOSTASIS36 40
NYHA III–IV +
previous HF
hospitalisation
LAP catheter
(HeartPOD) all
patients
25Increased event free survival,
lower LAP
CHAMPION37 38 550
NYHA III +
previous HF
hospitalisation
PA catheter
versus standard
care (single
blinded)
6
Reduced and shorter HF
hospitalisations, lowered PAP,
more medication changes in
intervention group
LAPTOP-HF* 730
NYHA III +
previous HF
hospitalisation
LAP catheter or
CRT-D12 Ongoing
* http://www.clinicaltrials.gov, NCT01121107.
ADHF, acute decompensated heart failure; BNP, B type natriuretic peptide; CRT-D, cardiac resynchronisation
therapy device; EF, ejection fraction; FI, fluid index; HF, heart failure; ICD, cardioverter defibrillator; IHM,
implantable haemodynamic monitors; LAP, left atrial pressure; NTS, nurse telephone support; NYHA, New York
Heart Association (functional class); PA, pulmonary artery; PAP, pulmonary artery pressure; PCWP, pulmonary
capillary wedge pressure; PPV, positive predictive value; QOL, quality of life; RCT, randomised controlled trial;
RTM, remote telemonitoring; RV, right ventricular; RVOT, right ventricular outflow tract; STS, structured telephone
support.
Left Atrial Pressure Monitoring A different approach to assess cardiac filling pressures is by implantation of a
left atrial pressure (LAP) sensing system. HeartPOD (St Jude Medical Inc, Minneapolis, Minnesota, USA) was
the first implantable LAP sensor to be reported.[51] Similar to the RV ICHM system, HeartPOD consists of a
small, pulse generator-like coil antenna and a lead carrying a septal anchor fixation system with a distal sensing
diaphragm. The lead is implanted percutaneously and advanced across the atrial septum with the sensor
depicting LAP signals. HeartPOD was previously shown to provide accurate and stable measurements in keeping
with simultaneously obtained pulmonary capillary wedge pressure.[50] In the recently published
Haemodynamically Guided Home Self-Therapy in Severe HF Patients (HOMEOSTASIS) trial, 40 ambulatory
patients in HF NYHA classes III and IV and a HF hospitalisation requiring intravenous therapy during the past 12
months underwent percutaneous implantation of the HeartPOD system.[36] The study design was observational
and prospective, with a follow-up of 25±19 (range 1–63) months. LAP was read twice daily, and both patients and
clinicians were blinded to the LAP data the first 3 months after implantation. HF therapy was thereafter guided by
LAP readings. HeartPOD derived LAP correlated highly with pulmonary capillary wedge pressure measured at 3
and 12 months (r=0.98, average difference of Hg) under various loading conditions, and no important device
0.8±4.0 mm related safety issues were raised. HOMEOSTASIS demonstrated encouraging significant reductions
of LAP together with improvements in NYHA class and EF. Importantly, LAP guided management led to
significant increases in β blocker and ACEI/angiotensin receptor blocker (ARB) use, as well as reduced use of
diuretics. Subsequently, an additional 44 patients were implanted with HeartPOD. Recently published 48 month
follow-up data in a total of 84 patients witnessed good long term sensor performance.[54] The ongoing LAP
Monitoring to Optimise HF Therapy trial (LAPTOP-HF; http://www.clinicaltrials.gov, NCT01121107; planned
enrolment 730 patients) using HeartPOD or a similar LAP sensor combined with CRT-D ('Promote LAP') will
evaluate whether HF related events are reduced in patients who are managed with the LAP management system
versus those who receive the current standard of care.
Pulmonary Artery Pressure Monitoring A different device making use of ambulatory haemodynamic
parameters is an implantable pulmonary artery sensor (CardioMEMS, Atlanta, Georgia, USA). The CardioMEMS
sensor is a small yet ingenious device that is deployed in a distal pulmonary artery branch during routine right
heart catheterisation, and delivers continuous pulmonary artery pressure (PAP) data.[55] An apparent advantage
over other ICHM devices is its small size and the lack of need for batteries or leads. The device was evaluated in

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 13/18
the CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III HF
Patients (CHAMPION) trial.[37] CHAMPION was a prospective, randomised, single blinded trial in patients with
NYHA class III HF, irrespective of LV EF, and a previous hospital admission for HF. All patients were implanted
with the ICHM device and then randomised to PAP guided therapy (n=270) or standard care (n=280). The primary
efficacy endpoint was HF related events at 6 months, with pressure sensor failure and ICHM related complications
as safety endpoints. After a mean follow-up of 15 months, in spite of a very low HF event rate (0.44 per 6 patient
months in the standard care cohort), haemodynamic guided HF therapy substantially reduced HF related
hospitalisations (to 0.31 per 6 patient months), significantly reduced PAP and improved quality of life. Integration
of PAP data also led to significantly greater medication use. It is remarkable that background medical therapy at
baseline was very good with over 90% and almost 80% of patients using β blockers and ACEI/ARBs, respectively,
and furthermore, that patients with reduced versus preserved EF benefitted equally. The specific medication
changes by which the encouraging results of the CHAMPION trial were achieved deserve further discussion.[56]
PAP guided HF therapy led to significantly greater utilisation of nitrates, ACEI/ARBs and β blockers.[38] Diuretics
were frequently adjusted, but not differently between groups. Extending positive signals from previous smaller,
mostly observational, studies, CHAMPION was the first randomised trial sufficiently powered to detect and
demonstrate effects on clinically meaningful endpoints.
Discussion
With the advent of technology allowing continuous monitoring of fluid status signals, early identification of
pulmonary fluid accumulation in HF patients has moved within reach. Several devices have provided evidence that
integration of fluid status is clinically feasible, with some encouraging results regarding endpoints.
First, remote or telemonitoring of HF symptoms integrating changes in body weight as a surrogate of fluid status
has been extensively studied in recent trials. Even if some of the trials have suffered from low adherence to
intervention, overall results have not demonstrated substantial benefit over and above standard HF care. Newer
data indicate that body weight changes in HF patients are likely not sensitive (nor specific) enough signals to
permit early identification of impending HF decompensation. This may be partly explained by fluid redistribution
(not retention) which has been recently proposed as an important contributory mechanism.[57]
A different fluid monitoring concept is based on serial measurements of intrathoracic impedance, exploiting its
inverse correlation with lung water content. A number of currently available CRT-D and ICD devices are capable of
providing valid impedance derived fluid indexes. As indications for CRT-D and ICD devices in clinical HF care are
ever expanding, additional fluid status signals could be obtained at 'no extra cost'. Ongoing large scale clinical
trials seek to establish whether HF management incorporating impedance data is superior to standard care.
Non-invasive impedance monitoring using impedance cardiography (ICG) may be suitable for patients who would
not otherwise be considered for receiving an implantable device but more definitive outcome data are required to
support their use in HF management.
Directly measured haemodynamic parameters as markers of intracardiac filling pressures constitute another
promising avenue in fluid status monitoring, and a number of different devices are the subject of ongoing
investigation.
Recent data support the potential for this approach in reducing HF related events even in cohorts with low event
rates that already receive state of the art care. Few studies have included HF patients with preserved EF, which
account for approximately half of ADHF hospitalisations.[58] Data from CHAMPION and COMPASS studies point
to a similar benefit for HF patients with preserved versus reduced EF.[33 37 38]
While the field advances rapidly, a number of issues remain to be resolved. Obviously, fluid status monitoring in
HF by itself does not alter outcomes. In the clinic, decompensated HF and hypervolaemia are most frequently
treated by increasing use of diuretics and/or vasodilators. Diuretic overuse might induce postural symptoms and
azotaemia, and may be harmful in the long term.[59] We still do not know from several published trials whether
knowledge of fluid status data actually led to medication changes; specifically, to enhanced use of drugs known
to reduce morbidity and mortality in HF. The medical community needs to learn what specific medication changes

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 14/18
produced results superior to standard care, as recently reported for the CHAMPION study.[38 56] Next, exactly
how were the fluid status data translated into treatment decisions? Given the multitude of monitoring devices,
unifying guidelines for intervention thresholds need to be established. We also need to learn more about managing
ADHF presenting without concomitant weight gain, where volume redistribution rather than overload may be the
pathophysiological abnormality. Finally, perhaps previous expectations of the devices to reduce risk in the range
20–30% have simply been too optimistic, given the very low event rates in some of the reported HF cohorts.
Nevertheless, despite these ongoing issues, device based fluid status monitoring appears to represent a novel and
promising tool in the management of HF.
References
1. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statisticsd2011 update: a report from
the American Heart Association. Circulation 2011;123: e18–209.
2. Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC guidelines for the diagnosis and treatment of acute
and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart
failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure
Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM).
Eur J Heart Fail 2008;10:933–89.
3. Braunschweig F, Cowie MR, Auricchio A. What are the costs of heart failure? Europace 2011;13(Suppl
2):ii13–17.
4. Pulignano G, Del Sindaco D, Tavazzi L, et al. Clinical features and outcomes of elderly outpatients with
heart failure followed up in hospital cardiology units: data from a large nationwide cardiology database (IN-
CHF Registry). Am Heart J 2002;143:45–55.
5. Blackledge HM, Tomlinson J, Squire IB. Prognosis for patients newly admitted to hospital with heart failure:
survival trends in 12 220 index admissions in Leicestershire 1993–2001. Heart 2003;89:615–20.
6. Stevenson LW, Perloff JK. The limited reliability of physical signs for estimating hemodynamics in chronic
heart failure. JAMA 1989;261:884–8.
7. Mahdyoon H, Klein R, Eyler W, et al. Radiographic pulmonary congestion in endstage congestive heart
failure. Am J Cardiol 1989;63:625–7.
8. Friedman MM. Older adults' symptoms and their duration before hospitalization for heart failure. Heart Lung
1997;26:169–76.
9. Dokainish H, Zoghbi WA, Lakkis NM, et al. Optimal noninvasive assessment of left ventricular filling
pressures: a comparison of tissue Doppler echocardiography and Btype natriuretic peptide in patients with
pulmonary artery catheters. Circulation 2004;109:2432–9.
10. Daniels LB, Clopton P, Bhalla V, et al. How obesity affects the cut-points for B-type natriuretic peptide in
the diagnosis of acute heart failure. Results from the Breathing Not Properly Multinational Study. Am Heart
J 2006;151:999–1005.
11. Chakko S, Woska D, Martinez H, et al. Clinical, radiographic, and hemodynamic correlations in chronic
congestive heart failure: conflicting results may lead to inappropriate care. Am J Med 1991;90:353–9.
12. Felker GM, Hasselblad V, Hernandez AF, et al. Biomarker-guided therapy in chronic heart failure: a meta-
analysis of randomized controlled trials. Am Heart J 2009;158:422–30.
13. Porapakkham P, Zimmet H, Billah B, et al. B-type natriuretic peptide-guided heart failure therapy: a meta-
analysis. Arch Intern Med 2010;170:507–14.

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 15/18
14. Adlbrecht C, Huelsmann M, Berger R, et al. Cost analysis and cost-effectiveness of NT-proBNP-guided
heart failure specialist care in addition to home-based nurse care. Eur J Clin Invest 2011;41:315–22.
15. Berger R, Moertl D, Peter S, et al. N-terminal pro-B-type natriuretic peptide-guided, intensive patient
management in addition to multidisciplinary care in chronic heart failure a 3-arm, prospective, randomized
pilot study. J Am Coll Cardiol 2010;55:645–53.
16. Goldberg LR, Piette JD, Walsh MN, et al. Randomized trial of a daily electronic home monitoring system in
patients with advanced heart failure: the Weight Monitoring in Heart Failure (WHARF) trial. Am Heart J
2003;146:705–12.
17. Mortara A, Pinna GD, Johnson P, et al. Home telemonitoring in heart failure patients: the HHH study
(Home or Hospital in Heart Failure). Eur J Heart Fail 2009;11:312–18.
18. Dar O, Riley J, Chapman C, et al. A randomized trial of home telemonitoring in a typical elderly heart
failure population in North West London: results of the Home-HF study. Eur J Heart Fail 2009;11:319–25.
19. Cleland JG, Louis AA, Rigby AS, et al. Noninvasive home telemonitoring for patients with heart failure at
high risk of recurrent admission and death: the Trans-European Network-Home-Care Management System
(TEN-HMS) study. J Am Coll Cardiol 2005;45:1654–64.
20. Zhang J, Goode KM, Cuddihy PE, et al. Predicting hospitalization due to worsening heart failure using daily
weight measurement: analysis of the Trans-European Network-Home-Care Management System (TEN-
HMS) study. Eur J Heart Fail 2009;11:420–7.
21. Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure. N Engl J Med
2010;363:2301–9.
22. Koehler F, Winkler S, Schieber M, et al. Impact of remote telemedical management on mortality and
hospitalizations in ambulatory patients with chronic heart failure: the telemedical interventional monitoring
in heart failure study. Circulation 2011;123:1873–80.
23. Inglis SC, Clark RA, McAlister FA, et al. Structured telephone support or telemonitoring programmes for
patients with chronic heart failure. Cochrane Database Syst Rev 2010;8:CD007228.
24. Yu CM, Wang L, Chau E, et al. Intrathoracic impedance monitoring in patients with heart failure: correlation
with fluid status and feasibility of early warning preceding hospitalization. Circulation 2005;112:841–8.
25. Maines M, Catanzariti D, Cemin C, et al. Usefulness of intrathoracic fluids accumulation monitoring with an
implantable biventricular defibrillator in reducing hospitalizations in patients with heart failure: a case-control
study. J Interv Card Electrophysiol 2007;19:201–7.
26. Whellan DJ, Ousdigian KT, Al-Khatib SM, et al. Combined heart failure device diagnostics identify patients
at higher risk of subsequent heart failure hospitalizations: results from PARTNERS HF (Program to Access
and Review Trending Information and Evaluate Correlation to Symptoms in Patients With Heart Failure)
study. J Am Coll Cardiol 2010;55:1803–10.
27. Abraham WT, Compton S, Haas G, et al. Intrathoracic impedance vs daily weight monitoring for predicting
worsening heart failure events: results of the Fluid Accumulation Status Trial (FAST). Congest Heart Fail
2011;17:51–5.
28. Tomasi L, Zanotto G, Zanolla L, et al. Physiopathologic correlates of intrathoracic impedance in chronic
heart failure patients. Pacing Clin Electrophysiol 2011;34:407–13.
29. Conraads VM, Tavazzi L, Santini M, et al. Sensitivity and positive predictive value of implantable
intrathoracic impedance monitoring as a predictor of heart failure hospitalizations: the SENSE-HF trial. Eur
11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 16/18
Heart J 2011;32:2266–73.
30. van Veldhuisen DJ, Braunschweig F, Conraads V, et al. Intrathoracic impedance monitoring, audible
patient alerts, and outcome in patients with heart failure. Circulation 2011;124:1719–26.
31. Brachmann J, Bohm M, Rybak K, et al. Fluid status monitoring with a wireless network to reduce
cardiovascular-related hospitalizations and mortality in heart failure: rationale and design of the OptiLink HF
Study (Optimization of Heart Failure Management using OptiVol Fluid Status Monitoring and CareLink).
Eur J Heart Fail 2011;13:796–804.
32. Adamson PB, Magalski A, Braunschweig F, et al. Ongoing right ventricular hemodynamics in heart failure:
clinical value of measurements derived from an implantable monitoring system. J Am Coll Cardiol
2003;41:565–71.
33. Bourge RC, Abraham WT, Adamson PB, et al. Randomized controlled trial of an implantable continuous
hemodynamic monitor in patients with advanced heart failure: the COMPASS-HF study. J Am Coll Cardiol
2008;51:1073–9.
34. Adamson PB, Conti JB, Smith AL, et al. Reducing events in patients with chronic heart failure (REDUCEhf)
study design: continuous hemodynamic monitoring with an implantable defibrillator. Clin Cardiol
2007;30:567–75.
35. Adamson PB, Gold MR, Bourge RC, et al. Reducing decompensation events utilizing intracardiac
pressures in patients with chronic HF (REDUCEhf). J Card Fail 2010;16:913.
36. Ritzema J, Troughton R, Melton I, et al. Physician-directed patient self-management of left atrial pressure
in advanced chronic heart failure. Circulation 2010;121:1086–95.
37. Abraham WT, Adamson PB, Bourge RC, et al. Wireless pulmonary artery haemodynamic monitoring in
chronic heart failure: a randomised controlled trial. Lancet 2011;377:658–66.
38. Costanzo MR, Abraham WT, Adamson PB, et al. Medical management guided by pulmonary artery
pressures in NYHA functional class III heart failure patients. J Card Fail 2011;17:S93.
39. Vollmann D, Nagele H, Schauerte P, et al. Clinical utility of intrathoracic impedance monitoring to alert
patients with an implanted device of deteriorating chronic heart failure. Eur Heart J 2007;28:1835–40.
40. Ypenburg C, Bax JJ, van der Wall EE, et al. Intrathoracic impedance monitoring to predict decompensated
heart failure. Am J Cardiol 2007;99:554–7.
41. Wang L, Lahtinen S, Lentz L, et al. Feasibility of using an implantable system to measure thoracic
congestion in an ambulatory chronic heart failure canine model. Pacing Clin Electrophysiol 2005;28:404–
11.
42. Rathman LD, Lee CS, Sarkar S, et al. A critical link between heart failure self-care and intrathoracic
impedance. J Cardiovasc Nurs 2011;26:E20–6.
43. Sarkar S, Hettrick DA, Koehler J, et al. Improved algorithm to detect fluid accumulation via intrathoracic
impedance monitoring in heart failure patients with implantable devices. J Card Fail 2011;17:569–76.
44. Braunschweig F, Ford I, Conraads V, et al. Can monitoring of intrathoracic impedance reduce morbidity
and mortality in patients with chronic heart failure? Rationale and design of the Diagnostic Outcome Trial in
Heart Failure (DOT-HF). Eur J Heart Fail 2008;10:907–16.
45. Gore JM, Goldberg RJ, Spodick DH, et al. A community-wide assessment of the use of pulmonary artery
catheters in patients with acute myocardial infarction. Chest 1987;92:721–7.

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 17/18
Contributors Both TGVL and HK contributed to the paper. TGVL drafted and wrote the manuscript. HK helped draft themanuscript and revised its content.
Funding TGVL is supported by a post-doctoral research grant from South-Eastern Norwegian Health Authorities.
Provenance and peer review Commissioned; not externally peer reviewed.
Heart. 2012;98(13):967-973. © 2012 BMJ Publishing Group Ltd & British Cardiovascular Society
46. Zion MM, Balkin J, Rosenmann D, et al. Use of pulmonary artery catheters in patients with acute
myocardial infarction. Analysis of experience in 5,841 patients in the SPRINT Registry. SPRINT Study
Group. Chest 1990;98:1331–5.
47. Connors AF Jr, Speroff T, Dawson NV, et al. The effectiveness of right heart catheterization in the initial
care of critically ill patients. SUPPORT Investigators. JAMA 1996;276:889–97.
48. Binanay C, Califf RM, Hasselblad V, et al. Evaluation study of congestive heart failure and pulmonary artery
catheterization effectiveness: the ESCAPE trial. JAMA 2005;294:1625–33.
49. Magalski A, Adamson P, Gadler F, et al. Continuous ambulatory right heart pressure measurements with
an implantable hemodynamic monitor: a multicenter, 12-month follow-up study of patients with chronic
heart failure. J Card Fail 2002;8:63–70.
50. Ritzema J, Melton IC, Richards AM, et al. Direct left atrial pressure monitoring in ambulatory heart failure
patients: initial experience with a new permanent implantable device. Circulation 2007;116:2952–9.
51. Walton AS, Krum H. The Heartpod implantable heart failure therapy system. Heart Lung Circ
2005;14(Suppl 2):S31–3.
52. Zile MR, Bennett TD, St John Sutton M, et al. Transition from chronic compensated to acute
decompensated heart failure: pathophysiological insights obtained from continuous monitoring of
intracardiac pressures. Circulation 2008;118:1433–41.
53. Teerlink JR. Learning the points of COMPASS-HF: assessing implantable hemodynamic monitoring in
heart failure patients. J Am Coll Cardiol 2008;51:1080–2.
54. Troughton RW, Ritzema J, Eigler NL, et al. Direct left atrial pressure monitoring in severe heart failure:
long-term sensor performance. J Cardiovasc Transl Res 2011;4:3–13.
55. Adamson PB, Abraham WT, Aaron M, et al. CHAMPION trial rationale and design: the long-term safety
and clinical efficacy of a wireless pulmonary artery pressure monitoring system. J Card Fail 2011;17:3–10.
56. Krum H. Telemonitoring of fluid status in heart failure: CHAMPION. Lancet 2011;377:616–18.
57. Fallick C, Sobotka PA, Dunlap ME. Sympathetically mediated changes in capacitance: redistribution of
the venous reservoir as a cause of decompensation. Circ Heart Fail 2011;4:669–75.
58. Yancy CW, Lopatin M, Stevenson LW, et al. Clinical presentation, management, and in-hospital outcomes
of patients admitted with acute decompensated heart failure with preserved systolic function: a report from
the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol
2006;47:76–84.
59. Ahmed A, Husain A, Love TE, et al. Heart failure, chronic diuretic use, and increase in mortality and
hospitalization: an observational study using propensity score methods. Eur Heart J 2006;27:1431–9.

11/4/13 www.medscape.com/viewarticle/765438_print
www.medscape.com/viewarticle/765438_print 18/18