Current Management Pleural Effusion, Empyema, Complicated ... · Current Management Pleural...
53
Current Management Pleural Effusion, Empyema, Complicated Pneumonia Update in Pediatrics Vincent Adolph, MD Pediatric Surgery July 20, 2019
Transcript of Current Management Pleural Effusion, Empyema, Complicated ... · Current Management Pleural...

Current ManagementPleural Effusion, Empyema,
Complicated Pneumonia
Update in Pediatrics
Vincent Adolph, MD
Pediatric Surgery
July 20, 2019
• No Financial Conflicts of Interest
• Thrombolytic use is off-label

• Describe the difference between pleural effusion and empyema
• Explain the role of imaging in patients with complicated pneumonia
• Explain the options for management of pleural effusion and empyema
• Know how to evaluate for parenchymal complications of pneumonia
• Evaluation / Decision making
• Antibiotic Selection
• Definitions
• Imaging
• Treatment
• Determining treatment failure
• Pulmonary Necrosis / Abscess / Pneumatocele
• Recurrent Pneumonia / Congenital Lung Lesions
• Duration of Antibiotic Therapy

• Assess Symptoms
• Resp sx, O2, fever, oral intake
• Parenchymal Process vs Pleural Disease
• Effusion vs Empyema
• Parenchymal Complications
Abscess, Necrosis, Pneumatocele

• Hypoxemia (SaO2 < 92%)
• Tachypnea (infants RR > 70 , older >50)
• Retractions, nasal flaring, grunting, etc
• Inadequate oral intake
• Other chronic conditions
• Toxic appearance
• Suspicion of Staph or group A Strep
• Failure of outpatient therapy
• Complications (effusion, empyema, abscess)
• Impending respiratory failure
• Inability to maintain sats > 92%
• Apnea or irregular respirations
• Hypotension / Refractory tachycardia
• Multi-lobar infiltrates
• Mental status changes
• Pleural disease (effusion / empyema)
• SS ds, immuno-compromise
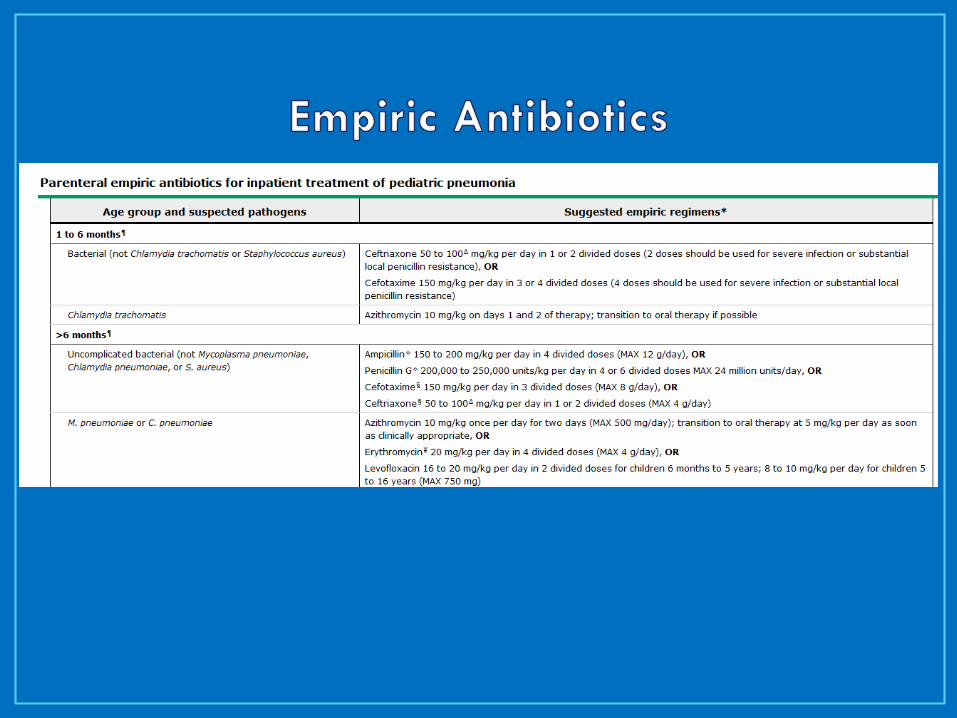
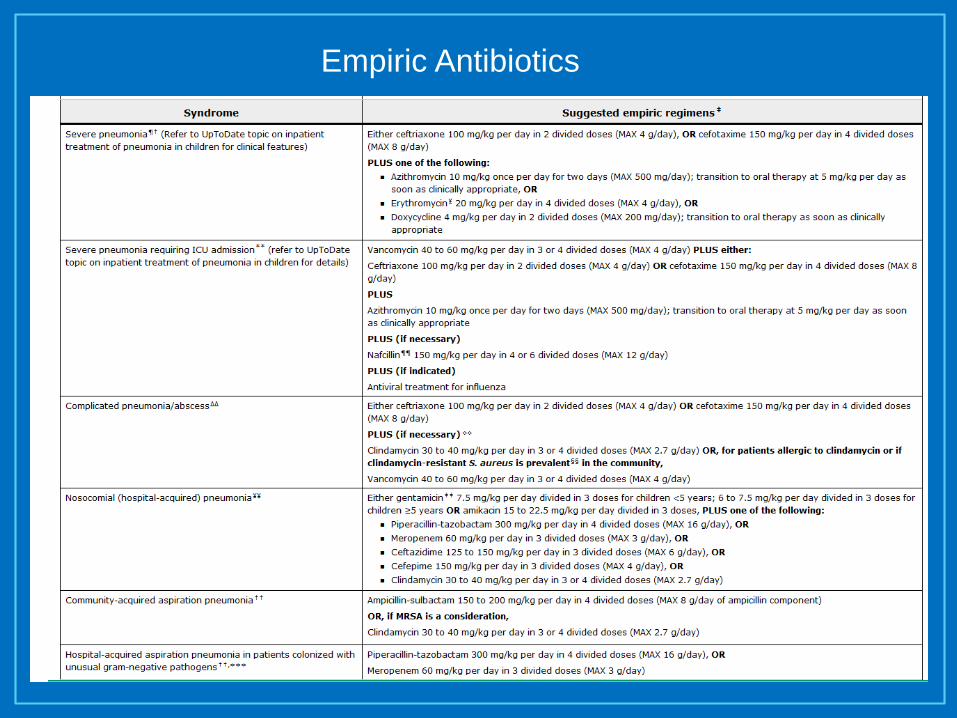
Empiric Antibiotics
• Effusion
• Transudate
• Simple, free-flowing fluid
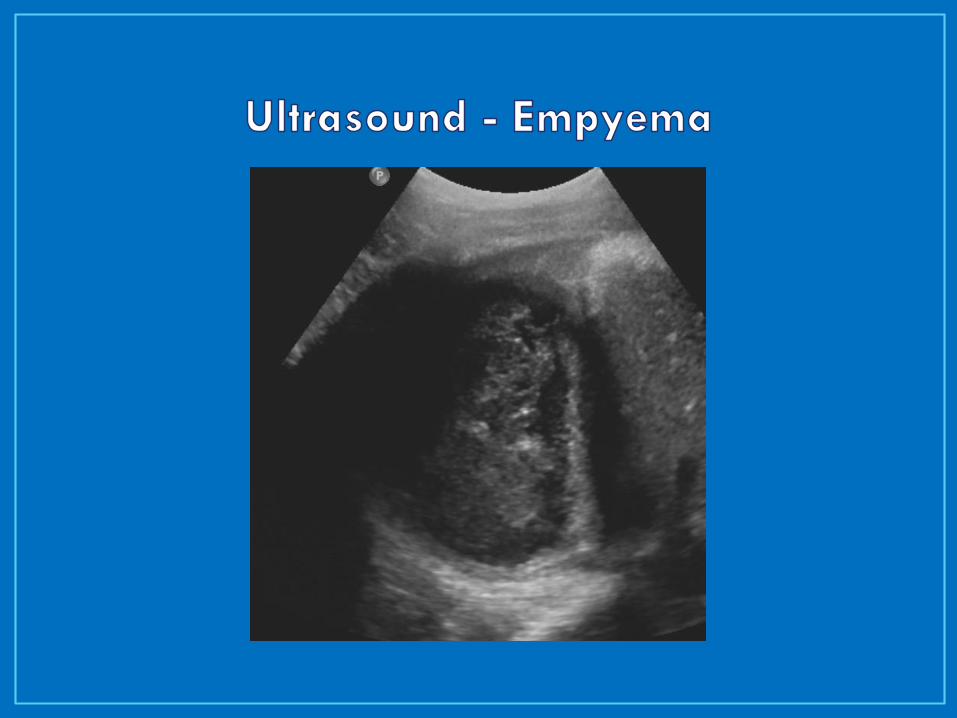
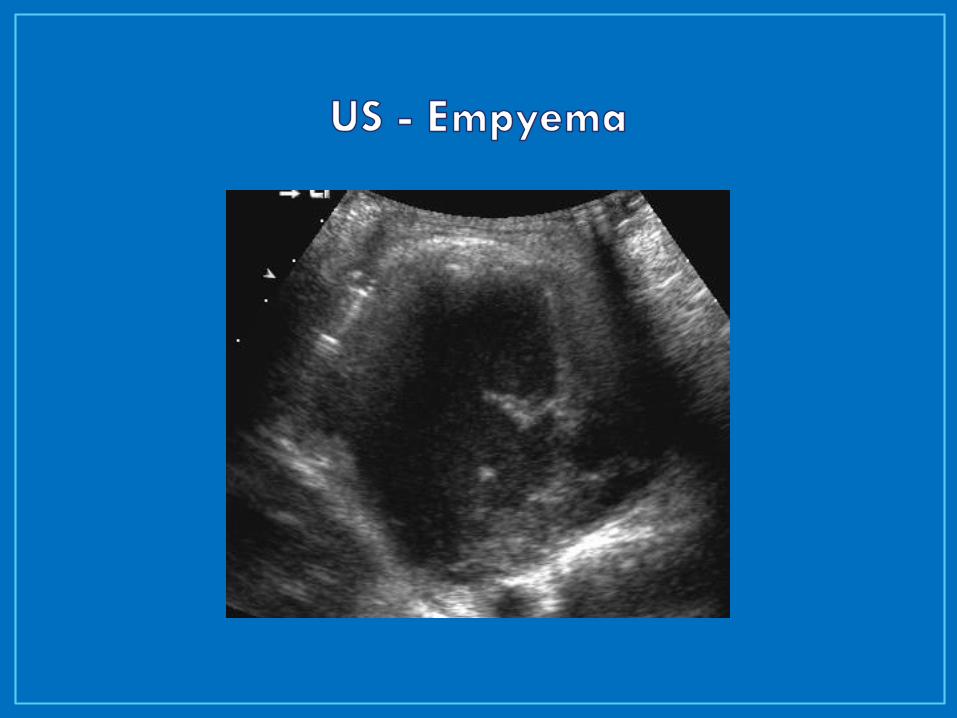
• Empyema
• Grossly purulent, WBC > 10,000 (<?)
• pH < 7.0, LDH > 1,000, Glucose < 40
• Positive gram stain
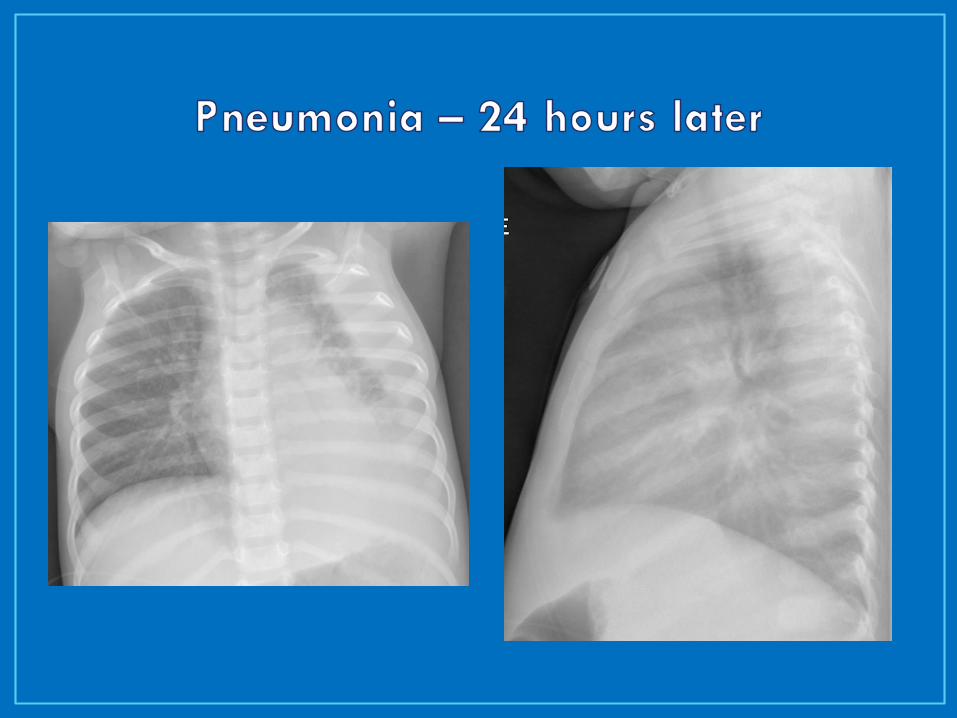
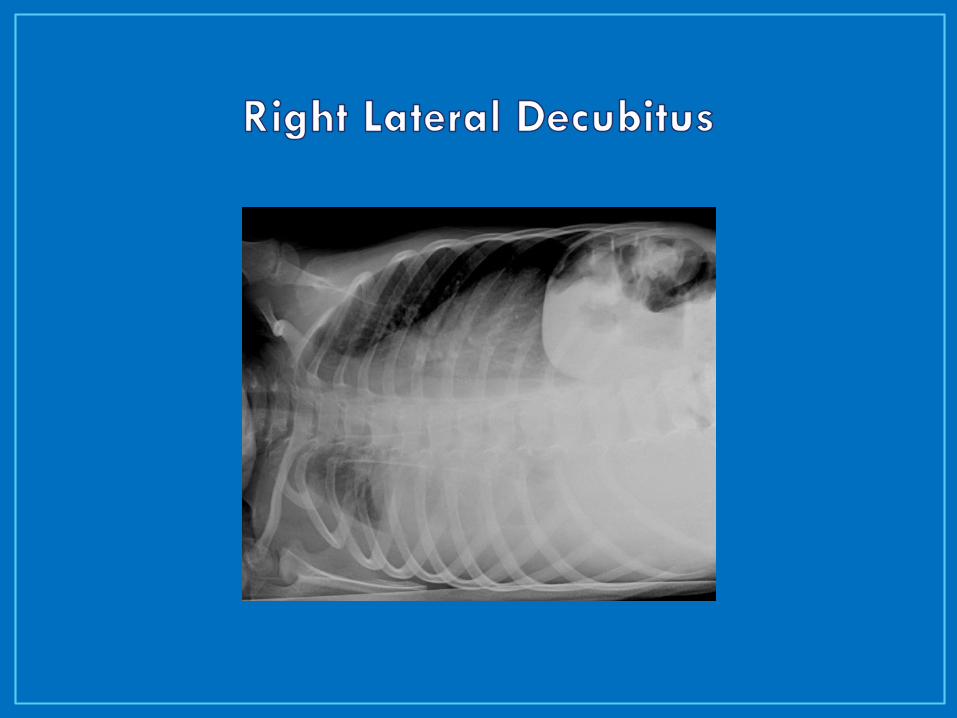
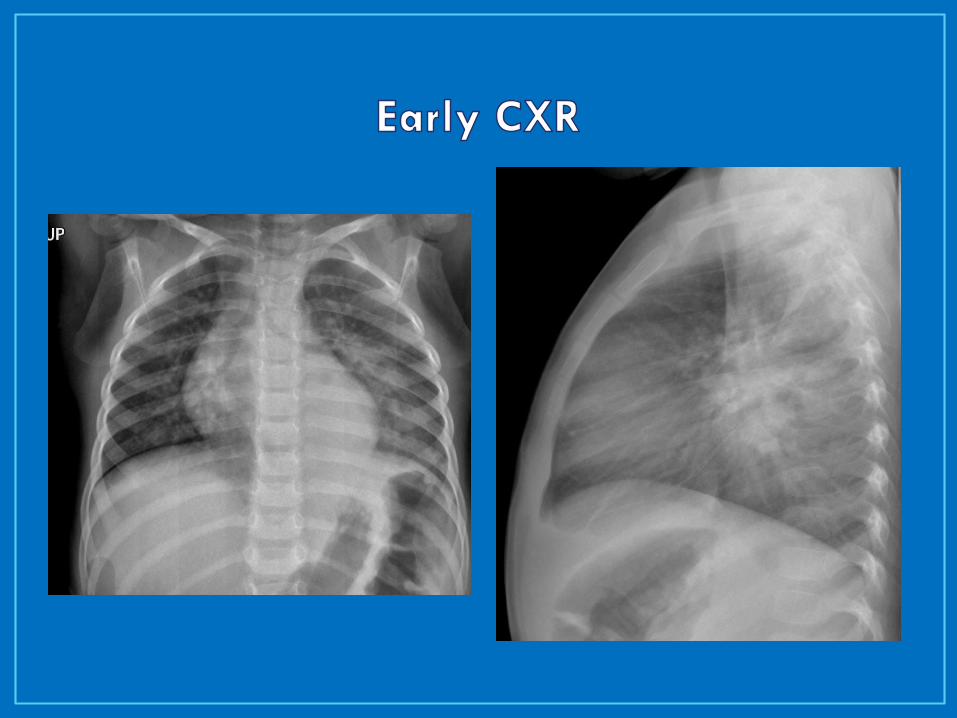
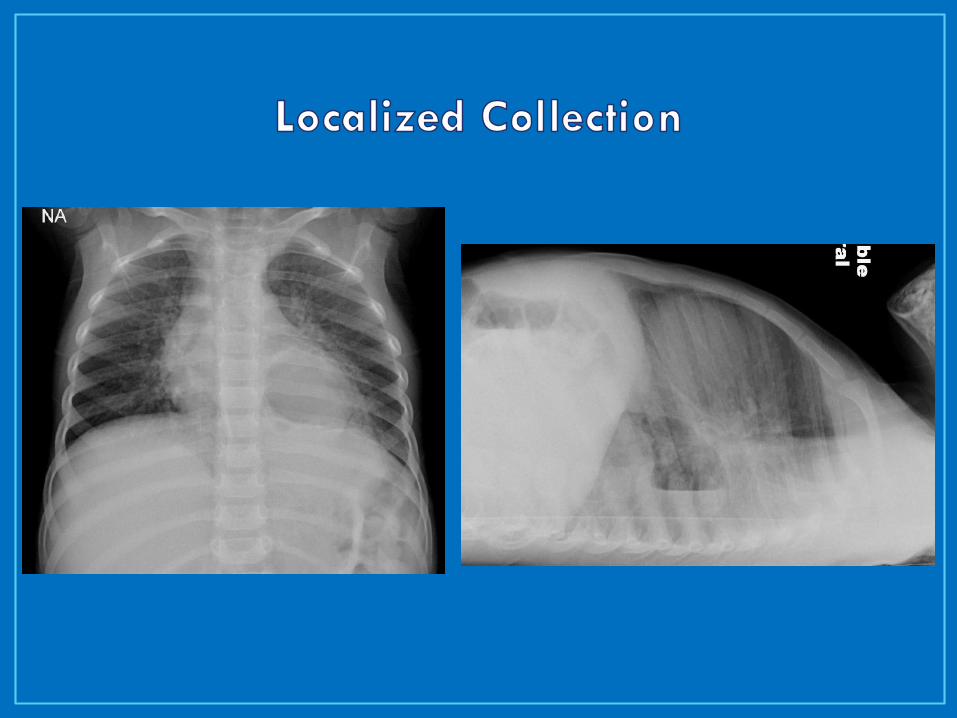
CXR
AP +/- decubitus (affected side down)
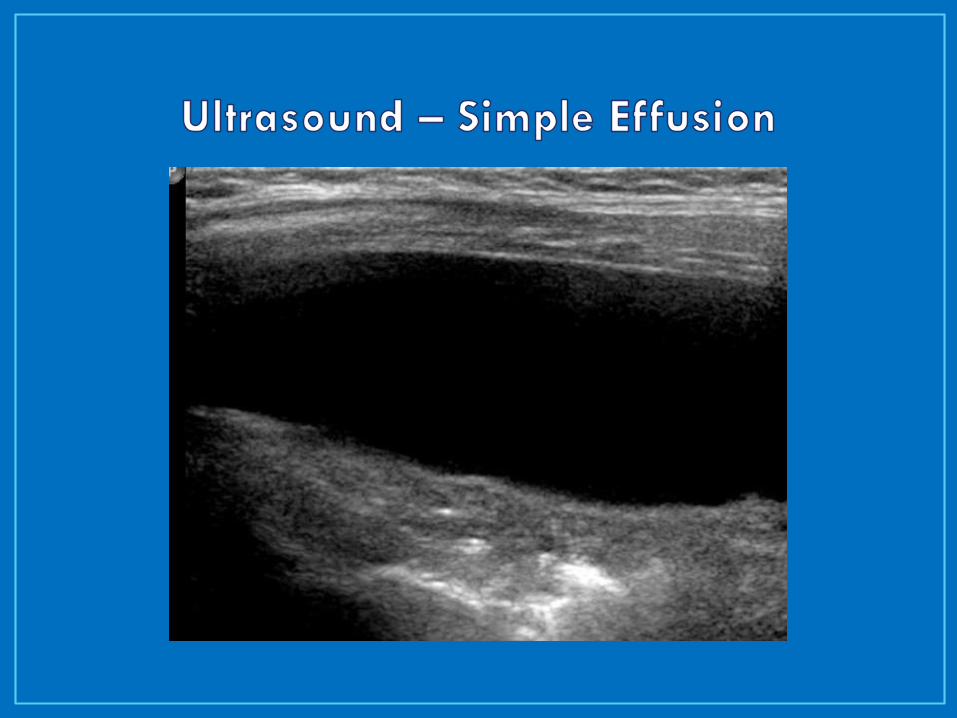
Ultrasound
Assess for pleural fluid volume / character
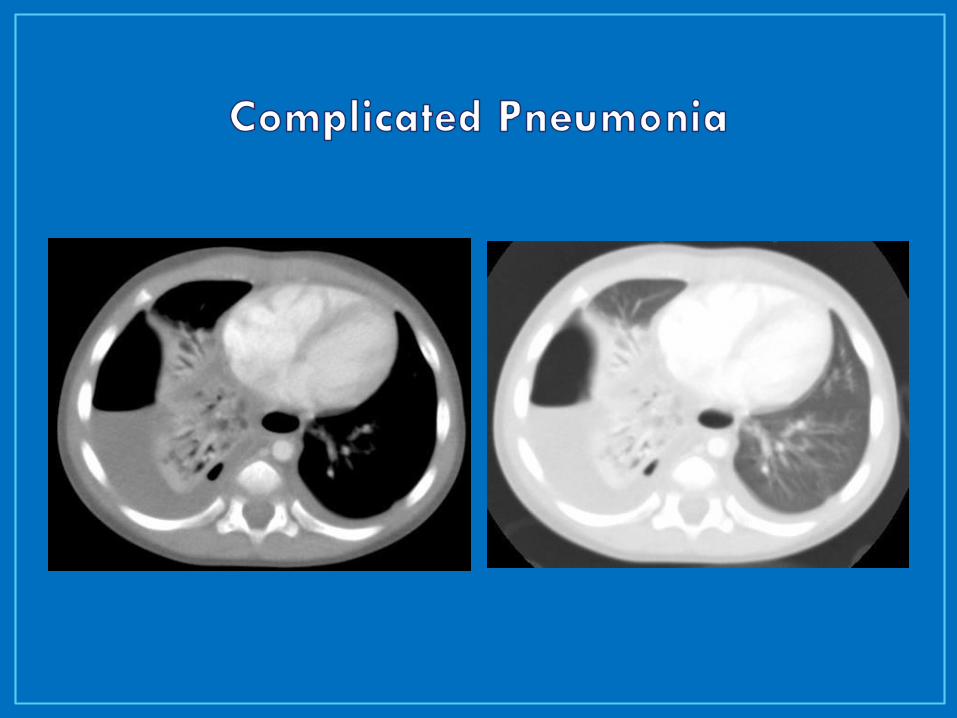
CT
Assess for parenchymal complications
IV contrast to assess for necrosis



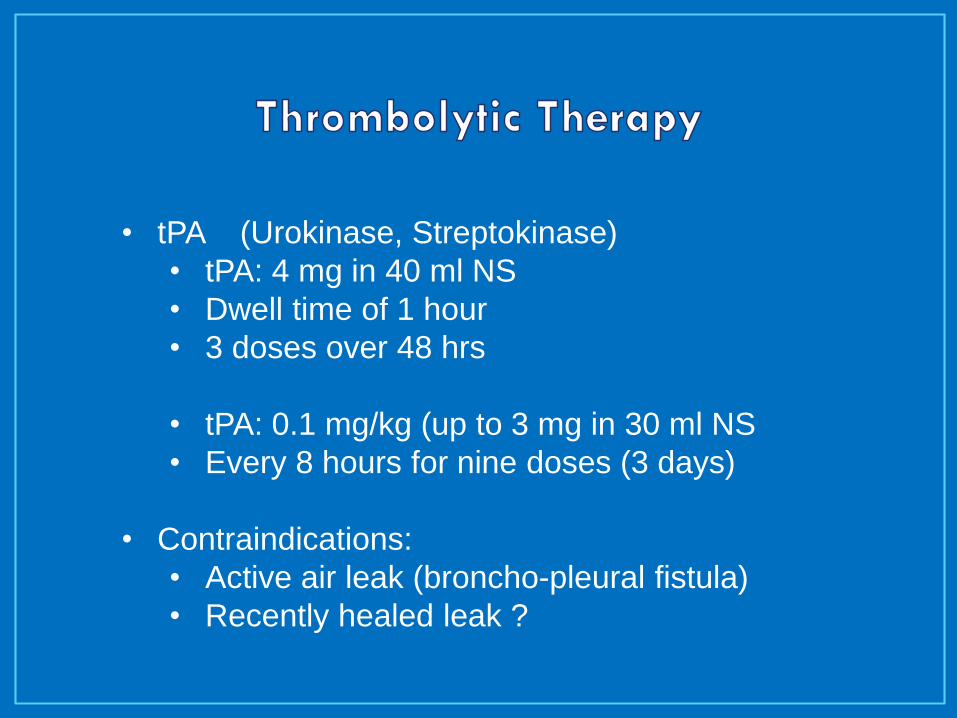
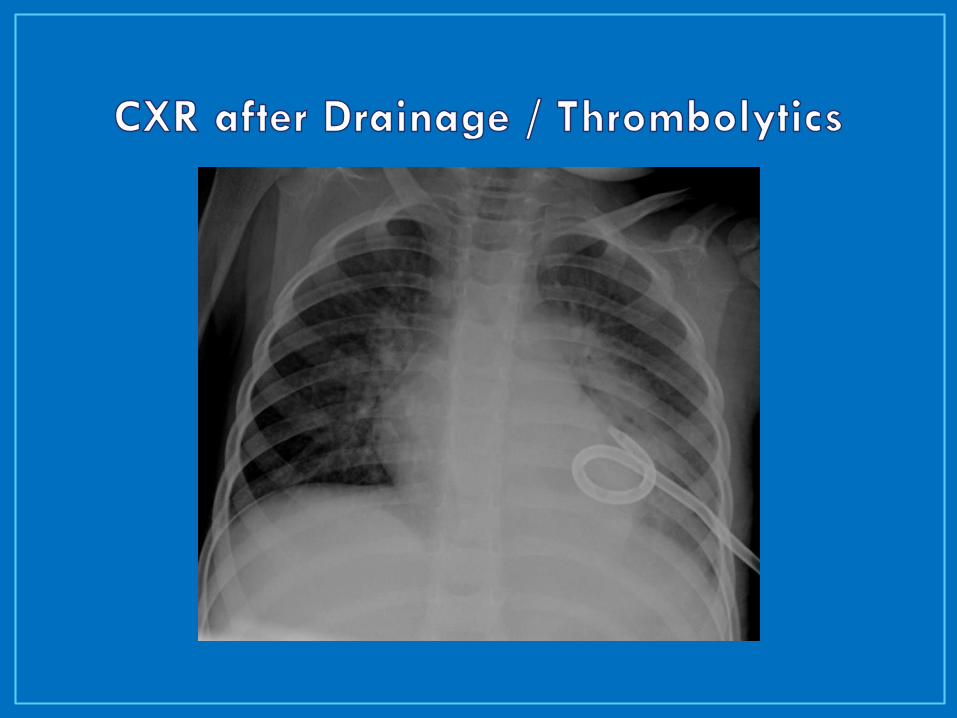
• tPA (Urokinase, Streptokinase)
• tPA: 4 mg in 40 ml NS
• Dwell time of 1 hour
• 3 doses over 48 hrs
• tPA: 0.1 mg/kg (up to 3 mg in 30 ml NS
• Every 8 hours for nine doses (3 days)
• Contraindications:
• Active air leak (broncho-pleural fistula)
• Recently healed leak ?


AP Supine Right lateral Decubitus








48-72 hours for CT / thrombolysis
Failure to improve
Fever, Resp status, oral intake, O2 need
Re-image
Assess pleural space
Assess lung parenchyma

• Indications:
• Failure to improve with CT / thrombolytics
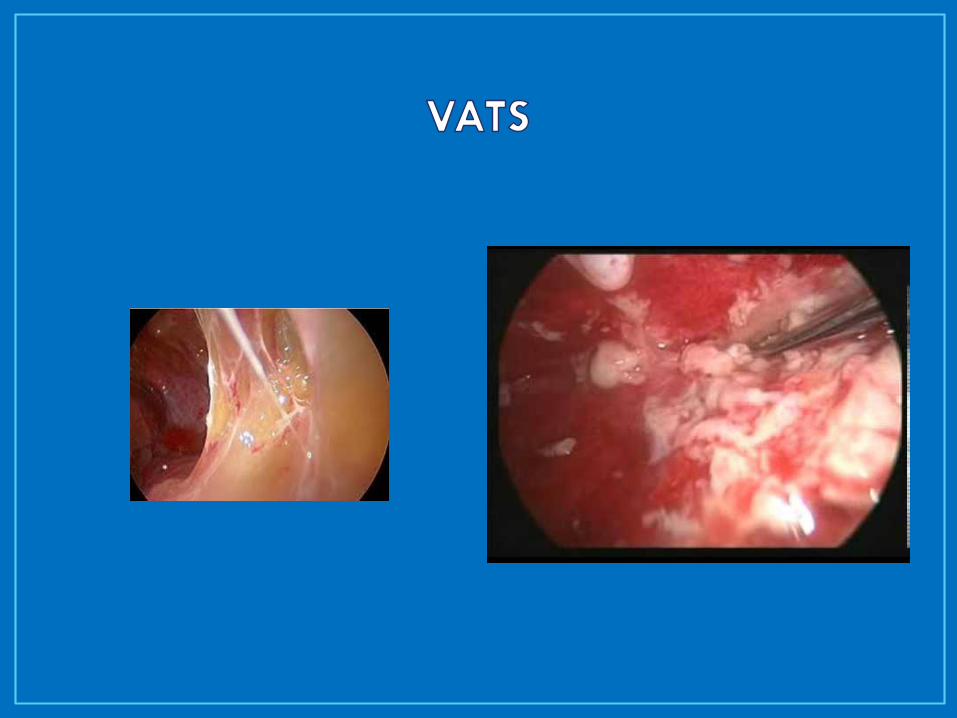
• VATS (Video-Assisted Thorascopic Surgery)
• Thorascopic debridement
• Thoracotomy
• Decortication – removal of thick fibrous pleural rind



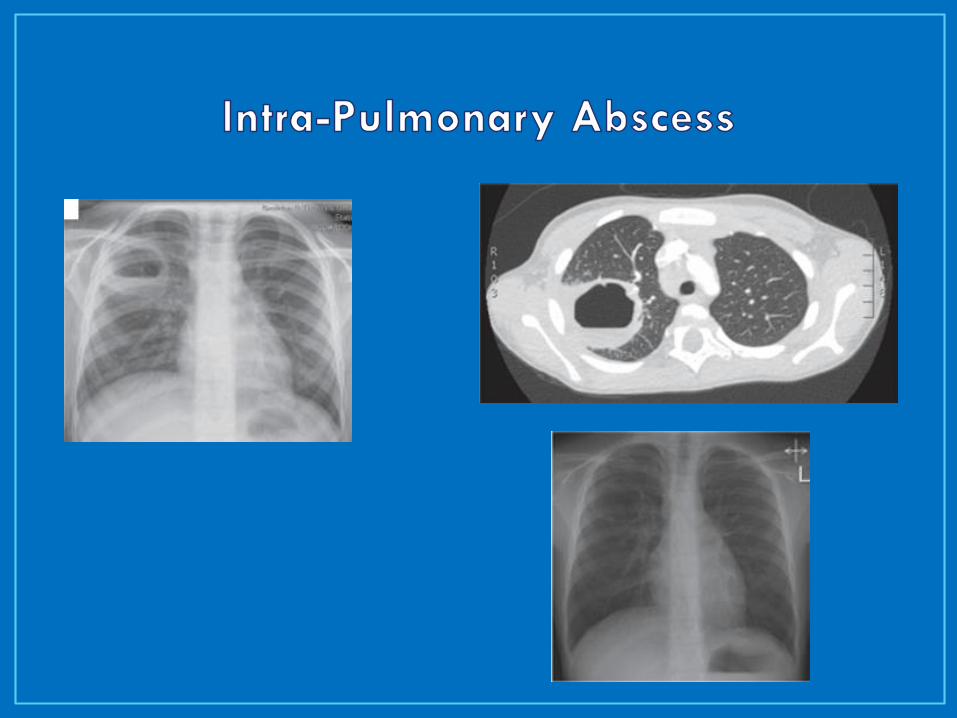
• Abscess
• Usually respond to longer course of antibiotics
• Selective aspiration / drainage
• Pneumothorax, pyo-pneumothorax
• Broncho-pleural fistula
• Pulmonary Necrosis
• Prolonged antibiotic course
• Very high risk with drainage, debridement, bx
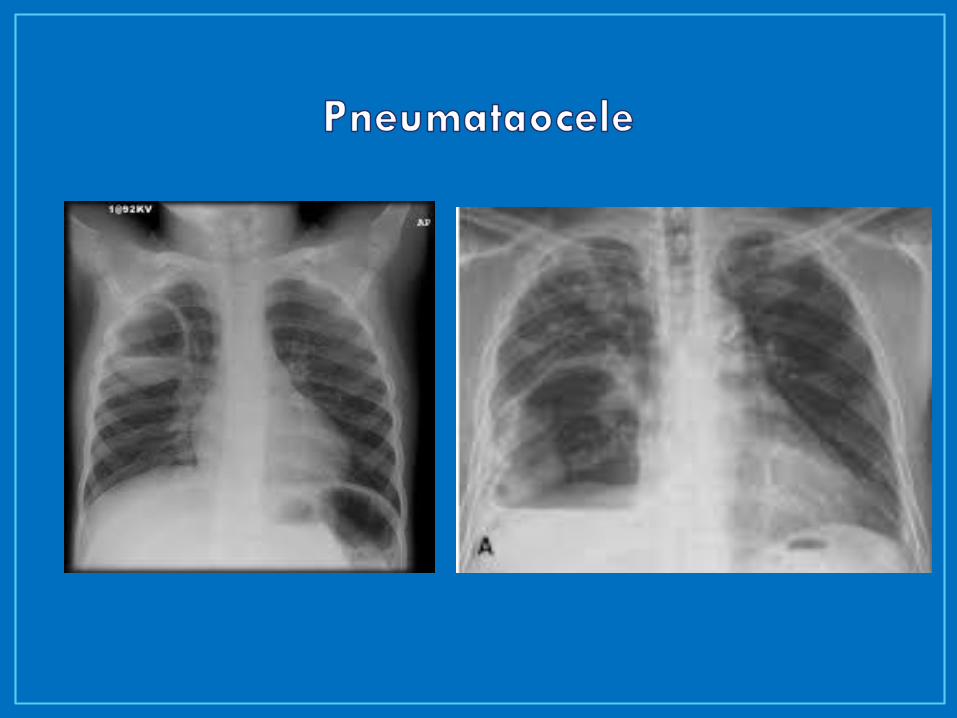
• Pneumatocele



• Recurrent Pneumonia in same lobe
• Pneumatocele
• Congenital Pulmonary Malformations
• CCAM
• (Congenital Cystic Adenomatoid Malformation)
• Sequestration
• Intrapulmonary
• Extrapulmonary
• Bronchogenic Cysts

Uncomplicated Pneumonia
One week after fever resolves
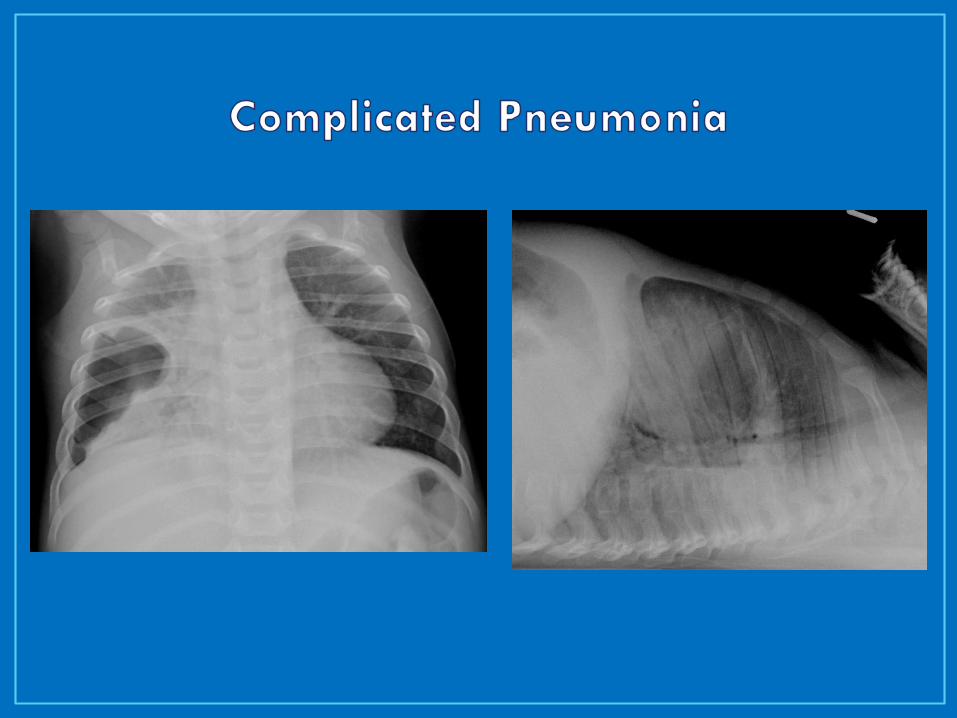
Complicated Pneumonia
Empyema:
7-10 days after CT out, clinically well, afebrile
Abscess/ Necrosis:
10-14 days after resolution – minimum
Some recommend 2-4 weeks
• Describe the difference between pleural effusion and empyema
• Explain the role of imaging in patients with complicated pneumonia
• Explain the options for management of pleural effusion and empyema
• Know how to evaluate for parenchymal complications of pneumonia