CURRENT CONCEPTS in peri-operative FLUID MANAGEMENT Prof. Mehdi Hasan Mumtaz.
Upload
keitria-twinsanandaCategory
view
236download
1description

Neurol Clin 25 (2007) 1209–1230
Current Concepts in Managementof Meningiomas and Schwannomas
Ashok R. Asthagiri, MDa,*,Gregory A. Helm, MD, PhDb,Jason P. Sheehan, MD, PhDb
aNational Institutes of Health/NINDS, Bethesda, MD, USAbDepartment of Neurological Surgery, University of Virginia Health Sciences Center,
P.O. Box 800212, Charlottesville, VA 22908-0212, USA
Intracranial schwannomas and tumors of the meninges have beenreported since the eighteenth century [1,2]. These extra-axial lesions lentthemselves to clinical detection by presenting overt and focal changes inappearance and function of the harboring patient. The earliest diagnosisof meningiomas during life occurred by causing hyperostotic changes tothe overlying skull. The first presumptive case of a vestibular schwannomacan be dated back to autopsy findings by Sandifort in 1777 in which hedocumented a small body adherent to the right auditory nerve, as relatedby Cushing [3]. Since their initial discovery, these often-benign lesionshave shared a parallel metamorphosis in their management. The goal ofthis article is to provide a review of the current literature surrounding themainstays of therapy for these lesions.
Meningiomas and schwannomas are the two most common extra-axialintracranial tumors in adults. Meningiomas account for approximately25% to 30.1% of all intracranial tumors diagnosed in the United States[4–7]. Data collected from the Central Brain Tumor Registry between1998 and 2002 reflect trends in meningioma demographics that have shownonly modest changes since 1990. These trends include a female age-specificincidence of 6.01 per 100,000 person-years compared with a male age-specific incidence of 2.75 per 100,000 person-years. Although the classicdescription associates these tumors with middle-aged women, it may bemisguiding because the median age at diagnosis for these tumors is 64 years
* Corresponding author.
E-mail address: [email protected] (A.R. Asthagiri).
0733-8619/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.ncl.2007.07.009 neurologic.theclinics.com

1210 ASTHAGIRI et al
and the age-specific incidence increases with each consecutive 10-year agecohort [7,8].
Intracranial nerve sheath tumors compose 8% to 10% of all intracranialtumors [7,9,10]. Schwannomas, which compose the vast majority of theselesions, are the second most common extra-axial intracranial tumor. Themale-to-female age-specific incidence ratio (1.01:1) is far less skewed thanfor meningiomas. These lesions also show a defined peak in incidence duringthe fifth and sixth decades of life [7].
Pathogenesis
Meningiomas
Tumorigenesis of meningiomas is presumed to be multifactorial and likelythe result of exogenous and endogenous factors. Among the earliest theoriesregarding their etiology was a causal relationship with head trauma, as firstsuggested by Cushing [11] in 1922 and then more assertively published in1938 [12]. Although this suggestion has been supported with isolated reportsand case-control studies, it has been refuted by others [13–17]. The seeminglyconflicting data leave us without definitive proof of a causal relationship be-tween head injury and subsequent development of intracranial meningiomas[18]. The best-proven external factor with a pathogenic role is radiation.Numerous reports have shown meningiomas to occur in treatment fields as-sociated with low doses of radiation. This concept gained wide acceptanceafter Modan and colleagues [19] reported a fourfold increase in the incidenceof meningiomas among children treated with the Kienbock-Adamson proto-col for tinea capitis, a low-dose radiation treatment protocol targeting thescalp that has since been replaced by pharmaceutic alternatives. Higher dosesof radiation have been associated with a decrease in the temporal delay todiscovery of meningiomas [20,21]. Less convincing supporting data existfor other exogenous factors including viral infection.
Endogenous factors involved in tumorigenesis include molecular alter-ations found in meningiomas and the ambiguous role of endogenous hor-mones in tumor development. Meningiomas were among the first solidtumors evaluated by cytogenetics. They were found to have a chromosomalaberration on the long arm of chromosome 22 in 50% to 72% of cases,which involved the tumor suppressor NF2 gene loci in up to 60% of spo-radic meningiomas [22–25]. The presence of the NF2 gene product, schwan-nomin/merlin, in 26% of one series, confirms the lack of universal deletionand underscores the notion that non-NF2 mechanisms are also important[26,27]. Of interest, the absence in reduction of NF2 protein levels may beas high as 72% in some histologic subtypes of meningiomas [28]. Otherchromosomal aberrations and genetic abnormalities, including the loss ofother tumor suppressor genes (DAL-1, CDKN2A), oncogene activation,and telomerase reactivation, are being implicated in the tumorigenesis of

1211MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
meningiomas and the progression toward malignant behavior with accrualof these changes [26].
An almost 2:1 female preponderance of meningiomas reported in the lit-erature and a strong association with breast cancer led to initial interest inthe role of sex hormones in the development and progression of meningio-mas. Investigation has revealed that tumors expressing progesteronereceptors behave in a more benign clinical fashion and are less likely torecur. Tumors expressing estrogen receptor or lacking progesterone receptorexpression display more frequent genotypic alterations and karyotypeabnormalities consistent with more aggressive meningiomas [29,30].Although the use of steroid hormone receptor antagonists as targets oftherapy was initially successful in mice experiments and promising to a lim-ited potential in humans, it now seems less promising after no benefit wasseen in a double-blinded, placebo-controlled phase III study [30,31].
Schwannomas
Schwannomas are slow-growing peripheral nerve sheath tumors that arisedistal to the oligodendroglial–Schwann cell myelination transition. Our un-derstanding of these lesions’ pathogenesis has been forwarded by the evalua-tion of the molecular and genetic changes found in neurofibromatosis 2(NF2). The NF2 gene was localized to chromosome 22q12 through geneticlinkage analysis [32]. Subsequent genetic and physical mapping led to the dis-covery of theNF2 gene by two independent groups in 1993 [33,34]. This regionof DNA encodes a 595–amino acid protein product termed ‘‘merlin’’ (formoesin-ezrin-radixin-like protein) or schwannomin, and it functions as a tu-mor suppressor. Mutations of the NF2 gene have been found not only inschwannomas associated with NF2 but also in sporadic cases [35–37]. Exten-sive screening of vestibular schwannomas, however, has not yielded a univer-sal detection of mutations of the NF2 gene locus, suggesting that additionalmechanisms for inactivation of the tumor suppressor may exist [38].
Clinical presentation
Meningiomas
Meningiomas are among the most diverse of all intracranial lesions, pre-senting with a vast assortment of symptoms, diagnostic imaging results, andhistology. The duplicitous nature of these lesions and their ability to mimicdiagnostic identifying features of other intracranial pathology have garneredrespectful monikers such as the ‘‘great masquerader.’’ Meningiomas origi-nate from arachnoid (meningothelial) cap cells, which in general are associ-ated with regions containing the trilamellar meninges. Lesions occurring inobscure locations such as the ventricular system can thus be explained by thepresence of these cap cells within the tela choroidea. The most commonlocations of meningiomas, in descending order of frequency, are convexity

1212 ASTHAGIRI et al
(19%–34%), parasagittal (18%–25%), sphenoid and middle cranial fossa(17%–25%), frontal base (10%) and posterior fossa (9%–15%), cerebellarconvexity (5%), cerebellopontine angle (2%–4%), intraventricular (1%–5%), and clivus (!1%) [20,39–41].
Meningiomas present in one of four ways, determined by size and locationof the tumor [42,43]. With the advent of CT/MRI diagnostic capabilities, me-ningiomas are being discovered more frequently in an incidental fashion. In-deed, meningiomas represent the most common incidentally detectedintracranial neoplasm, accounting for one third of such tumors [39,44]. Tenpercent of patients present in this manner, typically asymptomatic withslow or no tumor growth; however, one study of 40 patients revealed tumorgrowth in 33% and found 10% of patients became symptomatic [44,45]. Thesecond group, accounting for upwards of 50% of patients, may present due todisruption of cortical electrophysiology and present with seizures. Meningio-mas may also cause general symptoms of raised intracranial pressure, directlythrough tumor size and indirectly through associated hemorrhage, edema,obstructive hydrocephalus, and dural venous sinus obstruction. Finally, thesetumors may cause neurologic deficits because of neural compression. Theclinical presentation in these patients is determined by tumor location andsize. Typical clinical presentations have been extensively described in the lit-erature, the most common of which are outlined in Table 1.
Schwannomas
These typically benign tumors may be encountered incidentally but morecommonly present to clinical attention secondary to neurologic dysfunctionfrom local mass effect. Some tumors may display a more profound globalneurologic effect when cerebrospinal fluid dynamics are altered. Intracranialschwannomas, like their spinal counterparts, show a predilection forinvolvement of the sensory division of nerves. In order of decreasing fre-quency, schwannomas arise most commonly from the vestibular componentof the eighth nerve (O90%), sensory division of the trigeminal nerve (0.8%–8%), facial nerve (1.9%), nerves of the jugular foramen (2.9%–4%), hypo-glossal nerve, extraocular nerves, and the olfactory nerve [46–50]. Because oftheir intimate relationship with regional cranial nerves, brainstem, and cer-ebellum, schwannomas may become symptomatic even as relatively smalltumors. Conversely, their slow growth rates may mask the insidiousprogression of neurologic deficits, allow neural elements to deform withouta direct loss of function, or both. Typical clinical presentations of intracra-nial schwannomas are reviewed in Table 2.
Treatment
In the interests of brevity, the microsurgical and radiosurgical treatmentresults for meningiomas and vestibular schwannomas are discussed the

1213MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
following sections. These approaches and the associated results can be gen-erally translated to other more rare tumors such as facial or trigeminalschwannomas.
Microsurgical management
There is today nothing in the whole realm of surgery more gratifying than
the successful removal of a meningioma with subsequent perfect functionalrecovery. dHarvey Cushing [11]
Surgical resection of acoustic neuromas and meningiomas has been themainstay of treatment. Several compelling arguments favor surgery: (1) seem-ingly difficult tumors can sometimes be removed safely; (2) surgery securesa tissue diagnosisdoccasionally, a tumor thought to be a meningioma on im-aging is determined to be a different lesion; and (3) most meningiomas andacoustic neuromas are benign tumors, and a ‘‘cure’’ can be achieved by
Table 1
Meningioma location and associated typical clinical presentations
Meningioma Location Clinical presentation
Parasagittal and falcine Anterior one third
Middle one third
Posterior one third
Headache and mental status changes
Jacksonian seizures and progressive
hemiparesis
Headache, visual symptoms, seizures, or
mental status changes
Spenoid wing Lateral/pterional
Middle one third
(alar)
Medial (clinoidal)
Similar to convexity tumors
Hemiparesis/dysphasia
Visual acuity/field disturbance due to
optic nerve compression, proptosis,
cranial nerve dysfunction (III, IV, V,
VI)
Olfactory groove Foster Kennedy syndrome (anosmia,
ipsilateral optic atrophy with
contralateral papilledema), frontal lobe
syndromes/mental status changes,
urinary incontinence, seizure
Tuberculum sella/suprasellar Visual acuity/field disturbance, anosmia,
hydrocephalus, endocrinologic
syndromes
Cavernous sinus Cranial nerve deficits (III, IV, V, VI)
Cerebellopontine angle Hearing loss, facial pain/numbness/
weakness/spasm, headaches, cerebellar
signs
Foramen magnum Unilateral cervical pain, extremity motor
and sensory loss (clockwise
involvement), cold and clumsy hands
with intrinsic hand atrophy
Petroclival Hearing loss, vertigo, tinnitus, facial pain,
cranial nerve deficits (V, VI, VII, VII)

1214 ASTHAGIRI et al
complete resection. Advanced microsurgical and skull-based techniques haveled to reduced morbidity and more thorough resections of meningiomas andacoustic neuromas. Despite these advances, gross total resections cannot al-ways be accomplished without placing the patient at significant risk of mor-bidity and mortality. The goal of surgery should always be to preserve thequality of the patient’s life, even if it means leaving residual tumor.
Microsurgery results
MeningiomasThe measures used to review operative results in meningioma surgery in-
clude radiographic parameters (including recurrence rates) and clinical-based outcomes of morbidity and mortality. In 1957, Simpson [51]retrospectively reviewed the postoperative course of 265 patients who hadmeningiomas, 55 of whom experienced recurrences (21%). A recurrencerate of 9% was seen in patients who had a grade I excision, a recurrencerate of 19% was seen for grade II excisions, 29% for grade III, and 44%for grade IV (Table 3). The extent of surgical resection is the most importantfactor in the prevention of recurrence.
Although complete resection is generically the fundamental goal in sur-gery for these benign lesions, deliberate incomplete resection is often
Table 3
Simpson’s classification of the extent of resection of intracranial meningiomas
Grade Extent of resection Recurrence rate
I Gross total resection of tumor, dural attachments, and
abnormal bone
9%
II Gross total resection of tumor, coagulation of dural
attachments
19%
III Gross total resection of tumor without resection or coagulation
of dural attachments or its extradural extensions
29%
IV Partial resection of tumor 44%
V Simple decompression
From Simpson D. The recurrence of intracranial meningiomas after surgical treatment.
J Neurol Neurosurg Psychiatry 1957;20(1):22–39; with permission.
Table 2
Intracranial schwannomas: typical clinical presentation
Schwannoma Clinical presentation
Vestibular Unilateral sensory hearing loss, tinnitus, disequilibrium
Trigeminal Trigeminal nerve dysfunction (numbness, pain), headache, diplopia,
hearing loss/tinnitus
Facial Hearing loss, facial paralysis (may be acute), facial pain, hemifacial
spasm, tinnitus, vertigo
Jugular foramen Cranial nerve palsies (IX, X, XI)
Accessory nerve Chronic neck and shoulder pain, muscle spasms
Hypoglossal Headache, cranial nerve dysfunction (IX, X, XI), limb weakness

1215MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
undertaken to minimize associated morbidity. This practice is especially truewith regard to petroclival, clinoidal, and tentorial-based tumors to reducerelated cranial nerve morbidity, and in posterior parasagittal lesions with in-complete obstruction of the superior sagittal sinus to preserve its patency.Inherent to this, recurrence rates of these tumors are higher; the highestrecurrence rates (O20%) are found in patients who have sphenoid wing me-ningiomas, followed by those who have parasagittal meningiomas (8%–24%) and suprasellar meningiomas (5%–10%) [41]. These findings showthat the site of tumor origin and its operative accessibility may limit the po-tential for complete resection and thus serve as a secondary factor influenc-ing recurrence rate [52,53]. Other factors that correlate with an increasedrecurrence rate include histopathologic findings of increased mitosis, focalnecrosis, nuclear pleomorphism, prominent nucleoli, syncytial tumors, andthe presence of brain invasion [54–56]. These findings (except brain inva-sion) have been incorporated into the World Health Organization classifica-tion of meningiomas and denote changes toward malignancy.
The surgical morbidity and mortality associated with resection of theselesions has dramatically decreased since initial undertakings at the turn ofthe twentieth century. This decrease has been a result of improved diagnos-tic imaging, introduction of microsurgical techniques and image guidance,and better perioperative critical/medical care. Even in the best hands,however, mortality rates remain at 1% to 14% [57–62]. Factors that increasemortality include poor preoperative clinical condition, compressive symp-toms from tumor, old age, incomplete tumor removal, pulmonary embo-lism, and intracranial hemorrhage [58].
Morbidity associated with meningioma surgery has been cataloged andcritically reviewed and should be clustered into two broad categories. Thelow-risk group includes tumors that provide an easy corridor for accessand that are spatially removed from cranial nerves, brainstem, and vitalcerebrovascular anatomy. Examples of such tumors include cerebral andcerebellar convexity tumors, lateral- and middle-third sphenoid wing me-ningiomas, and anterior-third parasagittal and falcine meningiomas. Inmost cases, convexity meningiomas are amenable to complete resectionand improved operative mortality rates [63,64]. Neurologic sequelae asso-ciated with these resections typically manifest secondary to compromiseof adjacent cerebrovascular structures, immediate postoperative edema,and epilepsy [57]. In one study, convexity meningioma recurrence-freerates at 5, 10, and 15 years were 93%, 80%, and 68%, respectively[65]. Several investigators have reported low mortality rates (0%–3%)and morbidity manifesting as permanent neurologic deficit in 10% of pa-tients [66–68]. Similarly, relatively low rates of postoperative-increasedmorbidity can be found with anterior-third parasagittal and falcinemeningiomas.
The high-risk group of meningiomas includes tumors of the skull base,tentorial-based tumors, foramen magnum meningiomas, and parasagittal

1216 ASTHAGIRI et al
lesions associated with the middle third of the superior sagittal sinus. Basaltumors are often intimately associated with cranial nerves and proximal ce-rebral vessels, thereby making the approach to these lesions a formidablechallenge. With resection of skull-base tumors, permanent neurologic deficitascribed to cranial nerve dysfunction has been reported in a wide range(18%–86%) [69]. The highest of these complication rates is typically associ-ated with petroclival or cavernous sinus meningiomas, especially in cases inwhich a complete resection is performed [70–72]. Subtotal resection for de-compression, even with tumors of the cavernous sinus, can be performedsafely, although recurrence rates are naturally higher.
Schwannomas (vestibular)The first reported surgical removal of a vestibular schwannoma was per-
formed by Sir Charles Ballance [73] in 1894. Although alive and well overa decade later, the patient suffered ipsilateral facial paralysis and numbness,two neurologic sequelae that were not uncommon during initial undertak-ings for removal of these tumors. During this time period, Dandy [74] re-ported the operative mortality to be 67% to 84%. Through improvedsurgical methodology and technique, Cushing was able to markedly de-crease the mortality rates associated with operative management of these le-sions, thereby ushering neurosurgeons and neuro-otologists into the modernera of surgery for acoustic neuromas. Since that time, the introduction of theoperating microscope, more sensitive diagnostic imaging, and intraoperativefacial and cochlear monitoring has steadily reduced the morbidity and mor-tality associated with resection of these lesions. In a meta-analysis of 16studies including 5005 patients undergoing microsurgery for sporadic unilat-eral vestibular schwannomas, it was reported that tumor resection was com-plete in 96% of cases, with a mortality rate of 0.63%. The most commonnon-neurologic complication was cerebrospinal fluid leak, which occurredin 6.0% of patients [75].
With an expectant small mortality and major morbidity rate, the morecommon end points for evaluation of a successful surgery have turned topreservation of facial nerve function and auditory function. In 1985, Houseand Brackmann [76] developed what has become the most widely acceptedmeasurement of facial nerve function (Table 4). Detailed evaluation of indi-vidual large series shows that preservation of facial nerve function is in-versely proportional to tumor size. Indeed, when evaluating facial nervepreservation after resection of intracanalicular lesions alone, multiple stud-ies have reported 100% postoperative grade I House-Brackmann function[77–81]. Resection of small tumors (!2.0 cm), medium-sized tumors (2.0–3.9 cm), and large tumors (O4.0 cm) was respectively associated witha 95% to 97%, a 61% to 73%, and a 28% to 57% preservation of gradeI to II House-Brackmann function [82–84]. In reviewing the relative ratesof facial nerve dysfunction, the suboccipital and translabyrinthine ap-proaches afford comparable and excellent results compared with the middle

1217MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
fossa approach in which increased manipulation of the superiorly locatedfacial nerve in the internal auditory canal may account for a higher riskto facial nerve function [84–86].
Similarly, the importance of preservation of serviceable ipsilateral hear-ing has become paramount. The translabyrinthine approach, through itsdestruction of the otic capsule, is not compatible with hearing preserva-tion [85]. Resection of purely intracanalicular tumors is associated witha 57% to 82% preservation of ipsilateral serviceable auditory function[77,79]. Risk to serviceable auditory function is directly related to tumorsize. In 1988, Gardner and Robertson [87] compiled results of multipleoperative series and found hearing preservation in 131 of 394 patients,athough only 5 of these patients had tumors larger than 3 cm. Subse-quent studies have reported retention of functional ipsilateral hearing in29% to 60% of cases, primarily with tumors less than 3 cm, and a precip-itous decline in hearing preservation rates in cases with larger tumors[78,79,88,89]. The objective criteria for the designation of serviceablehearing vary between these studies and may account for the disparityin rates of hearing preservation.
Table 4
House-Brackmann scale for assessment of facial nerve function
Grade Function Gross Motion
I Normal facial
function
II Mild dysfunction � Slight weakness
noticeable on close
inspection
� May have slight
synkinesis
� At rest, normal
symmetry and tone
� Forehead: moderate-to-
good function
� Eye: complete closure
with minimal effort
� Mouth: slight asymmetry
III Moderate
dysfunction
� Obvious but not
disfiguring difference
between the two sides
� Noticeable but not severe
synkinesis, contracture,
or hemifacial spasm
� At rest, normal
symmetry and tone
� Forehead: slight-to-
moderate movement
� Eye: complete closure
with effort
� Mouth: slightly weak
with maximum effort
IV Moderately severe
dysfunction
� Obvious weakness and/
or disfiguring asymmetry
� At rest, normal
symmetry and tone
� Forehead: none
� Eye: incomplete closure
� Mouth: asymmetric with
maximum effort
V Severe dysfunction � Only barely perceptible
motion
� At rest, asymmetry
� Forehead: none
� Eye: incomplete closure
� Mouth: slight movement
VI Total paralysis � No movement � No movement
From House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck
Surg 1985;93(2):146–7; with permission.

1218 ASTHAGIRI et al
Radiosurgical management
Radiosurgery may be used for patients who have recurrent or residual tu-mors or as a primary treatment in patients unwilling or unable to undergosurgery and who possess a lesion with the typical imaging characteristics ofan acoustic neuroma or meningioma. Radiosurgery for meningiomas is usu-ally performed with the gamma knife. Occasionally, modified linear accela-rators or proton beam can be used. Patients who have atypical findings onMRI or CT should undergo surgery to obtain a histologic diagnosis. Thispractice is critical because when gamma knife radiosurgery (GKRS) isused to treat tumors on imaging characteristics alone, the risk of an incor-rect diagnosis may be as high as 2% [90].
Location plays a pivotal role in the selection of the appropriate treatmentmodality. Convexity meningiomas are usually treated with open surgerybecause they are amenable to complete resection. Acoustic neuromas,skull-base (including cavernous sinus and petroclival) and parasagittalmeningiomas, on the other hand, are ideal lesions for radiosurgery due totheir anatomy and associated surgical morbidity and mortality.
Residual tumor attached to still-patent vascular or neural structures canbe targeted using radiosurgery, allowing less radical microsurgical resectionand a lower incidence of morbidity. For radiosurgery, a distance of at least 3to 4 mm between the tumor and the optic apparatus is ideal. With thin-cutstereotactic planning MRI and shielding, radiosurgery can be used to treatlesions within 2 mm of the optic apparatus. The authors tend to favor earlytreatment of acoustic neuromas or skull-base meningiomas rather thana ‘‘watch and wait’’ approach because of the favorable benefit-to-risk profileof GKRS.
Radiosurgery results
MeningiomasNeuroimaging outcomes. The authors have treated more than 300 meningi-omas at the University of Virginia since 1989. The most recent evaluation ofthe authors’ material included 206 patients who had meningiomas treatedwith GKRS, with a follow-up of 1 to 6 years. This evaluation included142 patients treated for residual disease and 64 patients treated withGKRS primarily. Tumor volume ranged from 1 to 32 cm3. These patientsreceived an average of 38 Gy maximum dose (range, 20–60 Gy) and anaverage margin dose of 14 Gy (range, 10–20 Gy). Radiographic follow-upwas available for 151 patients. Of the evaluated patients, 94 (63%) showeda tumor volume decrease of at least 15% and 40 (26%) showed no change insize, corresponding to an 89% tumor control rate. Tumor growth was notedin 17 patients (11%). The authors now have long-term follow-up (10–21years) of 31 meningiomas treated with GKRS. Two thirds of these tumorshave shrunk significantly or remained stable. Among these tumors are those

1219MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
in which only the vascular supply for the tumor (ie, the nutritive vessel) wastargeted. Such targeting has resulted in significant tumor shrinkage andlasting effect, even in the long-term.
The results of other centers are similar (Table 5) [90–101]. The Universityof Pittsburgh group recently reported long-term results in 85 patients whosemeningiomas were treated with GKRS.With a median follow-up of 10 years,they reported that 53% of the tumors decreased in size and 40% were stablein size, corresponding to a 93% tumor control rate [102]. Kreil and col-leagues [103], with a median follow-up of 7.9 years, similarly reported on200 patients treated with GKRS for meningiomas and found that 56.5%of meningiomas demonstrated a decreased volume and 42.5% showed stabletumor volumes. Pollock and colleagues [104] compared the efficacy of GKRSwith that of microsurgery for the treatment of meningiomas that had an av-erage diameter less than 35 mm. They concluded that progression-free sur-vival after radiosurgery is equivalent to that after resection of a Simpsongrade 1 tumor and was superior to that after Simpson grade 2, 3, or 4 resec-tions, confirming the efficacy of GKRS, especially in tumors in which grosstotal resection is difficult to achieve due to anatomic constraints.
Atypical and malignant meningioma outcomes. Atypical and malignant me-ningiomas usually demonstrate recurrence and aggressive growth regardlessof the treatment modality (ie, extirpation, radiosurgery, or radiation ther-apy). Although GKRS appears to work very well for typical meningiomas,
Table 5
Outcome of radiosurgery for meningiomas
Size
Author (year)
[Reference] N
Follow-up
(mo)
Decrease
(%)
Stable
(%)
Increase
(%)
Complications
(%)
Improved
(%)
Kondziolka et al
(1991) [97]
50 12–36 54 38 2 6 d
Pendl et al (1997) [98] 97 48 39 56 5 5 d
Liscak et al (1999) [94] 67 2–60 52 48 0 4 36
Roche et al (2000) [93] 80 12–79 31 64 5 4 26
Lee et al (2002) [99] 159 2–145 34 60 6 7 29
Nicolato et al
(2002) [91]
122 O12 61 36 3 3 d
Roche et al (2003) [92] 32 28–188 12 88 d 6 41
Kondziolka (2003) [102] 85 120 53 40 7 6 d
Flickinger et al
(2003) [90]
219 2–164 d d 3 5 d
Liscak et al (2004) [100] 176 36 73 25 2 15.5 63
Kreil et al (2005) [103] 200 60–144 57 42 2 3 42
Malik et al (2005) [106] 277 39 d d 12 3–7 d
Pollock (2005) [101] 49 58 59 41 d 24 53
Steiner & Sheehana 151 6–252 63 26 11 0 8
Abbreviation: d, n/a.a Unpublished data from the author’s series.

1220 ASTHAGIRI et al
the results for atypical and malignant meningiomas are less favorable. Ina study from the University of Pittsburgh, Harris and colleagues [105] re-ported 5-year progression-free survival rates of 83% and 72% for atypicaland malignant meningiomas, respectively. Malik and colleagues [106] re-ported less favorable results, reporting 5-year actuarial control rates of49% in atypical meningiomas and 0% in malignant meningiomas. Ojemannand colleagues’ [107] results were similar to those of Malik and colleagues[106]; they reported a 5-year progression-free survival rate of 26% in pa-tients who had malignant meningiomas treated with GKRS, although out-comes were better in smaller tumors and in young patients. Survival rates, asopposed to control rates, have also been reported for patients after GKRSof atypical and malignant meningiomas. Five-year overall survival ratesvary between 59% and 76% in patients who have atypical meningiomasand between 0% and 59% in patients who have malignant meningiomas[105,107,108].
Radiation-induced meningioma outcomes. It is well known that fractionatedradiation therapy can induce meningiomas. The incidence of radiation-induced tumors following fractionated radiation therapy is 1.9% in 20 years.Some centers (including the authors’) have had limited yet favorable earlyexperience with radiosurgical treatment of radiation-induced tumors. Forexample, the Mayo Clinic group recently reported a 100% 5-year localtumor control rate for 16 patients who had radiation-induced tumors[109]. The median follow-up from the Mayo Clinic report was only 40.2months. Although it is too early to know whether such an approach is pru-dent, the concept of treating radiation-induced meningiomas with radiosur-gery may have some interesting implications regarding the pathogenesis ofintracranial tumors.
Clinical outcomes following radiosurgery. Many patients who present formanagement of meningiomas, especially skull-base lesions, present withneurologic deficits such as cranial nerve dysfunction. It is therefore impor-tant not only to evaluate outcomes with respect to tumor control but alsoclinical outcomes. GKRS is regularly reported to be associated with im-proved cranial nerve function after treatment of skull-base meningiomas.Pollock and Stafford [110], for example, reported that 12 of 38 patientswho presented with cranial neuropathies associated with cavernous sinusmeningiomas had improvement in cranial nerve function on follow-up.Roche and colleagues [93] also reported on clinical outcomes in patientswho had cavernous sinus meningiomas treated with GKRS. They reportedthat 23 of 54 patients who had oculomotor palsies improved or completelyrecovered and that 7 of 13 patients who had trigeminal neuralgia improvedor completely recovered. Roche and colleagues [92] reported similar successin GKRS-treated petroclival meningiomas: 13 of 32 patients treated withGKRS for petroclival meningiomas had clinical improvement in cranial

1221MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
nerve dysfunction. Kreil and colleagues [103] reported that 96% of patientswho had skull-base meningiomas treated with GKRS had improved or sta-ble neurologic status, with improvement noted in a broad range of areas in-cluding vision and other cranial nerve functions, hemiparesis, ataxia, vertigo,seizures, and exophthalmus.
Vestibular schwannomasNeuroimaging outcomes. At the University of Virginia’s Lars LeksellGamma Knife center, the authors and colleagues have treated 400 patientswho had vestibular schwannomas. One hundred fifty-three of these patientswho had greater than 12 months’ follow-up have been reported [111].Radiosurgery was the primary treatment for 96 patients and the adjuvanttreatment (following microsurgery) in 57 patients. The volume of the treatedtumors ranged from 0.02 to 18.3 cm3.
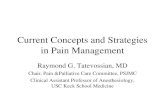
Of the patients treated primarily with GKRS, 81% (78 patients) experi-enced a decrease in tumor size (Fig. 1), 12% had no change, and 6% hadan increase in size. Among the 78 patients who had decreased tumor size,the decrease was greater than 50% in 20 patients. It is the authors’ policyto not consider decreases in volume of less than 15% as significant. Radio-logic follow-up for these patients ranged from 1 to 10 years.
Of the 57 patients treated with GKRS after microsurgery, 65% obtaineda decrease in tumor size, 25% had no change, and 10% had an increase intumor size. Among the 37 patients who had a decrease in the size of theirtumors, the decrease was greater than 50% in 12 patients. The outcome interms of postradiosurgical volume reduction in patients who had prior mi-crosurgery is worse compared with the outcome in those who were treatedprimarily with radiosurgery. This difference is likely a result of the increaseddifficulty with accurate targeting in those who underwent prior microsur-gery. Of note, although the authors’ experience with treating large vestibularschwannomas is small (n ¼ 19), they have observed a 95% tumor controlrate in these patients following radiosurgery. Other centers report similarrates (89%–100%) of tumor control (ie, no change or a decrease in thesize of the tumor) in patients (Table 6) [111–118].
The Karolinska group included evaluation of radiographic changes otherthan size [116]. The most common change was loss of central enhancementwithin the tumor on contrasted MRI or CT studies. This loss of central en-hancement occurred in 70% of patients and was typically observed within6 to 12 months of treatment. These changes, however, were reversible.Another change that was observed and that the authors have often seen isa transient increase in the size of the tumor during the first 6 months afterradiosurgery. This change is commonly seen in tumors that then regressto their original size or smaller.
Clinical outcomes following radiosurgery. In the vestibular schwannomapatients treated at the University of Virginia, five had transient changes in

1222 ASTHAGIRI et al
trigeminal sensation and three had facial paresis. One of the patients whohad facial weakness was operated on shortly after radiosurgery and waslost to follow-up. Another patient recovered completely in 6 weeks, andthe third has nearly completely recovered at 10 months. Of the patientswho had useful hearing before GKRS, 58% retained their hearing followingradiosurgery, 42% experienced some degree of deterioration, and 31% lostuseful hearing. Most hearing changes were observed at the 2-year checkup,and additional auditory changes were observed as late as 8 years postradiosurgery.
Fig. 1. Vestibular schwannomas. Of the patients treated primarily with GKRS, a decrease in
tumor size was seen in 81% (78 patients). (A) Pretreatment T1WI with contrast. (B) Post-treat-
ment T1WI with contrast (12 months post-treatment).

1223MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
Previously published prevalence of cranial neuropathies at other centerswere 17% at Karolinska and 29% at Pittsburgh for facial paresis, whichin most cases was transient or mild. The trigeminal nerve was affected ina variety of ways in 33% at Pittsburgh, most commonly a mild hypoesthe-sia. Recent complication rates at these institutions are comparable to thoseat the authors’ center. The authors have not seen an instance of cerebellaredema or hydrocephalus requiring spinal fluid diversion following GKRSfor vestibular schwannomas, but these complications have been reportedelsewhere [111,116].
Summary
The initial management of a patient presenting with radiographic evi-dence of a typically benign extra-axial neoplasm is a complex and evolvingprocess. As we approach an era in which the molecular processes underlyingneoplastic transformation and proliferation become more clearly delineated,new chemotherapeutic agents targeting these processes will broaden our ar-mamentarium with which we can target these tumors. Exciting frontiers,such as treatment of meningiomas with cyclo-oxygenase-2 inhibitors, shouldbe embraced with cautious optimism. Enthusiasm generated by successful invitro and nonprimate experiments in the treatment of meningiomas withantihormonal therapy and hydrosurea has met significant obstacles in thetransition to efficacy in human clinical trials. We are hopeful that inthe near future we may be enlightened with a chemobiologic treatment ad-vance that is comparable to the contributions brought to meningioma andschwannoma management by radiosurgery over the past several decades.
Patients presenting with asymptomatic, small meningiomas may be bestmanaged conservatively with a trial of expectant management and close sur-veillance with sequential MRI. In the treatment of these lesions, conserva-tive management may be undertaken with a period of observation for
Table 6
Outcome of radiosurgery for vestibular schwannomas
Author (year) [Reference]
No. of patients
who had follow-up
imaging studies
Mean
follow-up
(mo)
Tumor
increased
(%)
Tumor
unchanged or
decreased (%)
Noren et al (1993) [116] 209 minimum
of 12
16 84
Flickinger et al (1993) [111] 134 24 11 89
Foote et al (1995) [117] 35 16 0 100
Kwon et al (1998) [112] 63 52 5 95
Prasad et al (2000) [118] 153 51 7 93
Flickinger et al (2001) [113] 190 30 3 97
Bertalanffy et al (2001) [114] 40 36 9 91
Iwai et al (2003) [115] 51 60 4 96

1224 ASTHAGIRI et al
3 to 12 months before any definitive treatment decision is made [119]. Me-ningiomas presenting in symptomatic patients due to mass effect should gen-erally be resected completely, especially in the subset of patients harboringtumors that are relatively low risk for surgical complication. Meningiomasurgery in the elderly (O65 years old) has been performed with rates of mor-bidity and mortality similar to a control group of younger patients matchedfor tumor size and location [120]. Thus, age should not be a deterrent formicrosurgical treatment. A decision regarding invasive surgical managementversus radiosurgery can be influenced by preinterventional clinical perfor-mance status of the patient. When the mass effect of high-risk types of tu-mors extends beyond local cranial nerve dysfunction, surgical debulkingbecomes an absolute prequel to adjuvant radiosurgical methods, evenwhen a complete resection is not practical. The greatest amount of contro-versy exists in treatment of small (!3 cm) skull-base lesions presenting dueto focal neurologic signs and symptoms solely from cranial nerve dysfunc-tion. Radiosurgery advocates, in support of primary radiosurgical interven-tion, note the efficacy of radiosurgical methods in controlling tumor growthand emphasize the high rates of immediate postoperative morbidity associ-ated with attempted surgical resection of these lesions. Supporters of com-plete surgical resection stress the importance of cure being the ultimategoal, as opposed to control of the disease. They also question the legitimacyof long-term control of tumor growth with radiosurgery, citing the lack oflong-term follow-up. A third approach involves the combination of thesetherapeutic modalities. The benefits from immediate surgical decompressionof the cranial nerves with tumor debulking as a pretreatment adjunct toradiosurgical therapy for residual tumor is suggested as a synergistic, ratherthan mutually exclusive, way to approach the management of these difficultskull-base lesions [121].
The management of small and medium-sized vestibular schwannomasemphasizes the fundamental questions that are brought about in the man-agement of skull-base meningiomas. These lesions arise in the cerebellopon-tine angle where, even at a small size, they may cause profound effects oncranial nerve function. Surgical management of these lesions allows a cure(recurrence-free) in 92% to 100% of patients undergoing a complete resec-tion, with a small rate of major morbidity and mortality [120–126]. The ef-fectiveness of primary radiosurgical management in the control of tumorgrowth is indisputable in most patients. Even a tumor with marginal masseffect that extends beyond local cranial nerve involvement may be managedexclusively with radiosurgery. This management is possible because of thelarge subset of treated tumors that decreases in tumor volume after treat-ment (see Fig. 1). Monitoring trends in management over the last 2 decadeshas shown a precipitous decrease in the number of patients undergoingoperative intervention, commensurate with a proportional increase in thenumber of patients treated with radiosurgical methods. The reasons forthis are multifactorial, the least of which may be any true indication that

1225MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
radiosurgery is a better alternative than microsurgery for treatment of theselesions. The once-patriarchal patient–physician interaction has been re-placed with one of informed patient decision making. Patients are gaininga skeptical understanding of treatment paradigms through use of the Inter-net and health care advertising, and the wave of enthusiasm for minimallyinvasive surgery and noninvasive therapeutic modalities is swelling. This,in conjunction with third-party payors helping formulate health care deliv-ery strategies and protocols has placed the management of vestibularschwannomas at the whim of supply and demand economics, rather thana true shift toward superior outcomes. As with any new therapy that comesto the attention of the medical community, this initial crest in interest willsubside and an equilibrium will be reached that emphasizes the unique ben-efits of microsurgery and radiosurgery in the management of these lesionsand of their respective definitive niches. At this juncture, providing patientsready accessibility to treatment modalities and education regarding the ob-jectives, risks, and success rates of each will help clarify which managementstrategy is most suitable for patients on an individual basis.
References
[1] al-Rodhan NR, Laws ER Jr. Meningioma: a historical study of the tumor and its surgical
management. Neurosurgery 1990;26(5):832–46 [discussion: 846–7].
[2] House W, Luetje C. Acoustic tumors. Baltimore (MD): University Park Press; 1979.
[3] CushingH. Tumors of the nervus acusticus and the syndrome of the cerebellopontine angle.
Philadelphia: Saunders; 1917.
[4] Bondy M, Ligon BL. Epidemiology and etiology of intracranial meningiomas: a review.
J Neurooncol 1996;29(3):197–205.
[5] Surawicz TS, McCarthy BJ, Kupelian V, et al. Descriptive epidemiology of primary brain
and CNS tumors: results from the Central Brain Tumor Registry of the United States,
1990–1994. Neuro oncol 1999;1(1):14–25.
[6] Claus EB, Bondy ML, Schildkraut JM, et al. Epidemiology of intracranial meningioma.
Neurosurgery 2005;57(6):1088–95 [discussion: 1088–95].
[7] Central Brain Tumor Registry of the United States. Primary brain tumors in the United
States statistical report (1998–2002 years data collected) 2005–2006.
[8] Central Brain Tumor Registry of the United States. Primary brain tumors in the United
States statistical report (1990–1994 years data collected) 1999.
[9] Flickinger JC, Lunsford LD, Coffey RJ, et al. Radiosurgery of acoustic neurinomas.
Cancer 1991;67(2):345–53.
[10] Harner SG, Laws ER Jr. Clinical findings in patients with acoustic neurinoma. Mayo Clin
Proc 1983;58(11):721–8.
[11] Cushing H. The meningiomas (dural endotheliomas): their source, and favoured seats of
origin. Brain 1922;45:282–316.
[12] Cushing H, Eisenhardt LC. Meningiomas: their classification, regional behavior, life
history and surgical end results. Springfield (IL): Thomas; 1938.
[13] Inskip PD, Mellemkjaer L, Gridley G, et al. Incidence of intracranial tumors follow-
ing hospitalization for head injuries (Denmark). Cancer Causes Control 1998;9(1):
109–16.
[14] Kotzen RM, Swanson RM, Milhorat TH, et al. Post-traumatic meningioma: case report
and historical perspective. J Neurol Neurosurg Psychiatry 1999;66(6):796–8.

1226 ASTHAGIRI et al
[15] Preston-Martin S. Descriptive epidemiology of primary tumors of the brain, cranial nerves
and cranial meninges in Los Angeles County. Neuroepidemiology 1989;8(6):283–95.
[16] Phillips LE,Koepsell TD, vanBelle G, et al. History of head trauma and risk of intracranial
meningioma: population-based case-control study. Neurology 2002;58(12):1849–52.
[17] Annegers JF, Laws ER Jr, Kurland LT, et al. Head trauma and subsequent brain tumors.
Neurosurgery 1979;4(3):203–6.
[18] Wilkins RH, Rengachary SS. Neurosurgery. 2nd edition. New York: McGraw-Hill Health
Professions Division; 1996.
[19] Modan B, Baidatz D, Mart H, et al. Radiation-induced head and neck tumours. Lancet
1974;1(7852):277–9.
[20] Al-Mefty O. Meningiomas. New York: Raven Press; 1991.
[21] Mack EE,Wilson CB.Meningiomas induced by high-dose cranial irradiation. J Neurosurg
1993;79(1):28–31.
[22] Dumanski JP, Rouleau GA, NordenskjoldM, et al. Molecular genetic analysis of chromo-
some 22 in 81 cases of meningioma. Cancer Res 1990;50(18):5863–7.
[23] ZanklH, ZangKD.Cytological and cytogenetical studies on brain tumors. 4. Identification
of the missing G chromosome in human meningiomas as no. 22 by fluorescence technique.
Humangenetik 1972;14(2):167–9.
[24] Mark J, Levan G, Mitelman F. Identification by fluorescence of the G chromosome lost in
human meningomas. Hereditas 1972;71(1):163–8.
[25] Zang KD. Cytological and cytogenetical studies on human meningioma. Cancer Genet
Cytogenet 1982;6(3):249–74.
[26] Drummond KJ, Zhu JJ, Black PM. Meningiomas: updating basic science, management,
and outcome. Neurologist 2004;10(3):113–30.
[27] PerryA, CaiDX, Scheithauer BW, et al.Merlin, DAL-1, and progesterone receptor expres-
sion in clinicopathologic subsets of meningioma: a correlative immunohistochemical study
of 175 cases. J Neuropathol Exp Neurol 2000;59(10):872–9.
[28] Evans JJ, Jeun SS, Lee JH, et al. Molecular alterations in the neurofibromatosis type 2 gene
and its protein rarely occurring in meningothelial meningiomas. J Neurosurg 2001;94(1):
111–7.
[29] Pravdenkova S,Al-MeftyO, Sawyer J, et al. Progesterone and estrogen receptors: opposing
prognostic indicators in meningiomas. J Neurosurg 2006;105(2):163–73.
[30] Grunberg SM, Rankin C, Townsend J, et al. Phase III double-blind randomized placebo-
controlled study of mifepristone (RU) for the treatment of unresectable meningioma.
Presented at the American Society of Clinical Oncology. San Francisco (CA), May 12–
15, 2001.
[31] Grunberg SM,WeissMH, Spitz IM, et al. Treatment of unresectablemeningiomaswith the
antiprogesterone agent mifepristone. J Neurosurg 1991;74(6):861–6.
[32] Rouleau GA, Wertelecki W, Haines JL, et al. Genetic linkage of bilateral acoustic neuro-
fibromatosis to a DNA marker on chromosome 22. Nature 1987;329(6136):246–8.
[33] Trofatter JA,MacCollinMM, Rutter JL, et al. A novel moesin-, ezrin-, radixin-like gene is
a candidate for the neurofibromatosis 2 tumor suppressor. Cell 1993;75(4):791–800.
[34] Rouleau GA, Merel P, Lutchman M, et al. Alteration in a new gene encoding a putative
membrane-organizing protein causes neuro-fibromatosis type 2. Nature 1993;363(6429):
515–21.
[35] IrvingRM,MoffatDA,HardyDG, et al. SomaticNF2 genemutations in familial and non-
familial vestibular schwannoma. Hum Mol Genet 1994;3(2):347–50.
[36] Welling DB, Guida M, Goll F, et al. Mutational spectrum in the neurofibromatosis type 2
gene in sporadic and familial schwannomas. Hum Genet 1996;98(2):189–93.
[37] Jacoby LB,MacCollinM, Louis DN, et al. Exon scanning for mutation of the NF2 gene in
schwannomas. Hum Mol Genet 1994;3(3):413–9.
[38] Zucman-Rossi J, Legoix P, Der Sarkissian H, et al. NF2 gene in neurofibromatosis type 2
patients. Hum Mol Genet 1998;7(13):2095–101.

1227MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
[39] BuetowMP,BuetowPC, Smirniotopoulos JG. Typical, atypical, andmisleading features in
meningioma. Radiographics 1991;11(6):1087–106.
[40] Schmidek HH. Meningiomas and their surgical management. Philadelphia: Saunders;
1991.
[41] Kaye AH, Laws ER. Brain tumors: an encyclopedic approach. 2nd edition. Edinburgh
(UK): Churchill Livingstone; 2001.
[42] Black P. Meningiomas. In: Bernstein M, Berger MS, editors. Neuro-oncology: the essen-
tials. New York: Thieme Medical Publishers; 2000. p. xv, 508.
[43] Fick J, Wilson CB, Fuller G. Intracranial extra-axial tumors: meningiomas. In: Levin VA,
editor. Cancer in the nervous system. New York: Churchill Livingstone; 1996. p. 384–90.
[44] NiiroM, YatsushiroK, NakamuraK, et al. Natural history of elderly patients with asymp-
tomatic meningiomas. J Neurol Neurosurg Psychiatry 2000;68(1):25–8.
[45] Go RS, Taylor BV, Kimmel DW. The natural history of asymptomatic meningiomas in
Olmsted County, Minnesota. Neurology 1998;51(6):1718–20.
[46] Pollack IF, Sekhar LN, Jannetta PJ, et al. Neurilemomas of the trigeminal nerve. J Neuro-
surg 1989;70(5):737–45.
[47] Tan LC, Bordi L, Symon L, et al. Jugular foramen neuromas: a review of 14 cases. Surg
Neurol 1990;34(4):205–11.
[48] SamiiM,BabuRP, TatagibaM, et al. Surgical treatment of jugular foramen schwannomas.
J Neurosurg 1995;82(6):924–32.
[49] Symon L, Cheesman AD, Kawauchi M, et al. Neuromas of the facial nerve: a report of 12
cases. Br J Neurosurg 1993;7(1):13–22.
[50] McCormick PC, Bello JA, Post KD. Trigeminal schwannoma. Surgical series of 14 cases
with review of the literature. J Neurosurg 1988;69(6):850–60.
[51] Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J Neurol
Neurosurg Psychiatry 1957;20(1):22–39.
[52] Melamed S, Sahar A, Beller AJ. The recurrence of intracranial meningiomas. Neurochirur-
gia (Stuttg) 1979;22(2):47–51.
[53] Adegbite AB, KhanMI, PaineKW, et al. The recurrence of intracranial meningiomas after
surgical treatment. J Neurosurg 1983;58(1):51–6.
[54] Boker DK, Meurer H, Gullotta F. Recurring intracranial meningiomas. Evaluation of
some factors predisposing for tumor recurrence. J Neurosurg Sci 1985;29(1):11–7.
[55] de la Monte SM, Flickinger J, Linggood RM. Histopathologic features predicting recur-
rence of meningiomas following subtotal resection. Am J Surg Pathol 1986;10(12):836–43.
[56] Marks SM, Whitwell HL, Lye RH. Recurrence of meningiomas after operation. Surg
Neurol 1986;25(5):436–40.
[57] Black PM, Loeffler JS. Cancer of the nervous system. 2nd edition. Philadelphia: Lippincott
Williams & Wilkins; 2005.
[58] Jaaskelainen J. Seemingly complete removal of histologically benign intracranial meningi-
oma: late recurrence rate and factors predicting recurrence in 657 patients. A multivariate
analysis. Surg Neurol 1986;26(5):461–9.
[59] JanM, Bazeze V, Saudeau D, et al. [Outcome of intracranial meningioma in adults. Retro-
spective study of a medicosurgical series of 161 meningiomas]. Neurochirurgie 1986;32(2):
129–34 [in French].
[60] Ojemann RG. Skull-base surgery: a perspective. J Neurosurg 1992;76(4):569–70.
[61] Pertuiset B, Farah S, Clayes L, et al. Operability of intracranial meningiomas. Personal
series of 353 cases. Acta Neurochir (Wien) 1985;76(1–2):2–11.
[62] Kallio M, Sankila R, Hakulinen T, et al. Factors affecting operative and excess long-term
mortality in 935 patients with intracranial meningioma. Neurosurgery 1992;31(1):2–12.
[63] Manelfe C, Lasjaunias P, Ruscalleda J. Preoperative embolization of intracranial meningi-
omas. AJNR Am J Neuroradiol 1986;7(5):963–72.
[64] Olivecrona H. The meningiomas. In: Olivecrona H, Tonnis W, editors. Handbuch der
neurochirugie. Berlin: Springer-Verlag; 1967. p. 1–191.

1228 ASTHAGIRI et al
[65] Morimura T, Takeuchi J, Maeda Y, et al. Preoperative embolization of meningiomas: its
efficacy and histopathological findings. Noshuyo Byori 1994;11(2):123–9.
[66] Bonnal J, ThibautA, Brotchi J, et al. Invadingmeningiomas of the sphenoid ridge. JNeuro-
surg 1980;53(5):587–99.
[67] Ojemann RG. Meningiomas of the basal parapituitary region: technical considerations.
Clin Neurosurg 1980;27:233–62.
[68] Jaaskelainen J, Ohman J, Kotilainen P, et al. In: Black P, KayeAH, editors. Operative neu-
rosurgery. Sphenoidal wing meningiomasdouter and middle, vol. 1. London: Harcourt;
2000. p. 587–604.
[69] DeMonte F, Smith HK, al-Mefty O. Outcome of aggressive removal of cavernous sinus
meningiomas. J Neurosurg 1994;81(2):245–51.
[70] Al-MeftyO, Smith RR. Surgery of tumors invading the cavernous sinus. SurgNeurol 1988;
30(5):370–81.
[71] Maruyama K, Shin M, Kurita H, et al. Proposed treatment strategy for cavernous sinus
meningiomas: a prospective study. Neurosurgery 2004;55(5):1068–75.
[72] Zentner J, Meyer B, Vieweg U, et al. Petroclival meningiomas: is radical resection always
the best option? J Neurol Neurosurg Psychiatry 1997;62(4):341–5.
[73] Ballance CA. Some points in the surgery of the brain and its membranes. London:Macmil-
lan; 1907.
[74] DandyWE. An operation for the total removal of cerebellopontine (acoustic) tumors. Surg
Gynecol Obstet 1925;41:129–48.
[75] Yamakami I, Uchino Y, Kobayashi E, et al. Conservative management, gamma-knife
radiosurgery, and microsurgery for acoustic neurinomas: a systematic review of outcome
and risk of three therapeutic options. Neurol Res 2003;25(7):682–90.
[76] House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg
1985;93(2):146–7.
[77] Haines SJ, Levine SC. Intracanalicular acoustic neuroma: early surgery for preservation of
hearing. J Neurosurg 1993;79(4):515–20.
[78] Nadol JB Jr, ChiongCM,OjemannRG, et al. Preservation of hearing and facial nerve func-
tion in resection of acoustic neuroma. Laryngoscope 1992;102(10):1153–8.
[79] Samii M, Matthies C, Tatagiba M. Intracanalicular acoustic neurinomas. Neurosurgery
1991;29(2):189–98 [discussion: 198–9].
[80] Morrison AW, King TT. Experiences with a translabyrinthine-transtentorial approach to
the cerebellopontine angle. Technical note. J Neurosurg 1973;38(3):382–90.
[81] DiTullio MV Jr, Malkasian D, Rand RW. A critical comparison of neurosurgical and
otolaryngological approaches to acoustic neuromas. J Neurosurg 1978;48(1):1–12.
[82] Ojemann RG. Management of acoustic neuromas (vestibular schwannomas). [Honored
guest presentation]. Clin Neurosurg 1993;40:498–535.
[83] EbersoldMJ,Harner SG, Beatty CW, et al. Current results of the retrosigmoid approach to
acoustic neurinoma. J Neurosurg 1992;76(6):901–9.
[84] Sekhar LN, Gormley WB, Wright DC. The best treatment for vestibular schwannoma
(acoustic neuroma): microsurgery or radiosurgery? Am J Otol 1996;17(4):676–82 [discus-
sion: 683–9].
[85] Whittaker CK, Luetje CM. Vestibular schwannomas. J Neurosurg 1992;76(6):
897–900.
[86] Shelton C, Brackmann DE, House WF, et al. Middle fossa acoustic tumor surgery: results
in 106 cases. Laryngoscope 1989;99(4):405–8.
[87] Gardner G, Robertson JH. Hearing preservation in unilateral acoustic neuroma surgery.
Ann Otol Rhinol Laryngol 1988;97(1):55–66.
[88] Baldwin DL, King TT, Morrison AW. Hearing conservation in acoustic neuroma surgery
via the posterior fossa. J Laryngol Otol 1990;104(6):463–7.
[89] Fischer G, Fischer C, Remond J. Hearing preservation in acoustic neurinoma surgery.
J Neurosurg 1992;76(6):910–7.

1229MANAGEMENT OF MENINGIOMAS AND SCHWANNOMAS
[90] Flickinger JC, Kondziolka D, Maitz AH, et al. Gamma knife radiosurgery of imaging-
diagnosed intracranial meningioma. Int J Radiat Oncol Biol Phys 2003;56(3):801–6.
[91] Nicolato A, Foroni R, Alessandrini F, et al. Radiosurgical treatment of cavernous sinus
meningiomas: experience with 122 treated patients. Neurosurgery 2002;51(5):1153–9 [dis-
cussion: 1159–61].
[92] Roche PH, Pellet W, Fuentes S, et al. Gamma knife radiosurgical management of petro-
clival meningiomas results and indications. Acta Neurochir (Wien) 2003;145(10):883–8
[discussion: 888].
[93] Roche PH, Regis J, Dufour H, et al. Gamma knife radiosurgery in the management of
cavernous sinus meningiomas. J Neurosurg 2000;93(Suppl 3):68–73.
[94] Liscak R, SimonovaG, Vymazal J, et al. Gamma knife radiosurgery of meningiomas in the
cavernous sinus region. Acta Neurochir (Wien) 1999;141(5):473–80.
[95] Kondziolka D, Lunsford LD, Coffey RJ, et al. Stereotactic radiosurgery of meningiomas.
J Neurosurg 1991;74(4):552–9.
[96] Steiner L, Lindquist C, SteinerM.Meningiomas and gamma knife surgery. In: Al-MeftyO,
editor. Meningiomas. New York: Raven Press; 1991. p. 263–72.
[97] KondziolkaD, Lunsford LD, CoffeyRJ, et al. Gammaknife radiosurgery ofmeningiomas.
Stereotact Funct Neurosurg 1991;57(1–2):11–21.
[98] Pendl G, Schrottner O, Eustacchio S, et al. Stereotactic radiosurgery of skull base menin-
giomas. Minim Invasive Neurosurg 1997;40(3):87–90.
[99] Lee JY, Niranjan A, McInerney J, et al. Stereotactic radiosurgery providing long-term
tumor control of cavernous sinus meningiomas. J Neurosurg 2002;97(1):65–72.
[100] Liscak R, Kollova A, Vladyka V, et al. Gamma knife radiosurgery of skull base meningi-
omas. Acta Neurochir Suppl 2004;91:65–74.
[101] Pollock BE. Stereotactic radiosurgery for intracranial meningiomas: indications and
results. Neurosurg Focus 2003;14(5):1–7.
[102] Kondziolka D, Nathoo N, Flickinger JC, et al. Long-term results after radiosurgery for
benign intracranial tumors. Neurosurgery 2003;53(4):815–21 [discussion: 821–2].
[103] Kreil W, Luggin J, Fuchs I, et al. Long term experience of gamma knife radiosurgery for
benign skull base meningiomas. J Neurol Neurosurg Psychiatry 2005;76(10):1425–30.
[104] Pollock BE, Stafford SL, Utter A, et al. Stereotactic radiosurgery provides equivalent
tumor control to SimpsonGrade 1 resection for patients with small- tomedium-sizemenin-
giomas. Int J Radiat Oncol Biol Phys 2003;55(4):1000–5.
[105] Harris AE, Lee JY, Omalu B, et al. The effect of radiosurgery during management of
aggressive meningiomas. Surg Neurol 2003;60(4):298–305 [discussion: 305].
[106] Malik I, Rowe JG,Walton L, et al. The use of stereotactic radiosurgery in the management
of meningiomas. Br J Neurosurg 2005;19(1):13–20.
[107] Ojemann SG, Sneed PK, Larson DA, et al. Radiosurgery for malignant meningioma:
results in 22 patients. J Neurosurg 2000;93(Suppl 3):62–7.
[108] Stafford SL, Pollock BE, Foote RL, et al. Meningioma radiosurgery: tumor control, out-
comes, and complications among 190 consecutive patients. Neurosurgery 2001;49(5):
1029–37 [discussion: 1037–8].
[109] Jensen AW, Brown PD, Pollock BE, et al. Gamma knife radiosurgery of radiation-induced
intracranial tumors: local control, outcomes, and complications. Int J Radiat Oncol Biol
Phys 2005;62(1):32–7.
[110] Pollock BE, Stafford SL. Results of stereotactic radiosurgery for patients with imaging
defined cavernous sinus meningiomas. Int J Radiat Oncol Biol Phys 2005;62(5):1427–31.
[111] Flickinger JC, Lunsford LD, Linskey ME, et al. Gamma knife radiosurgery for acoustic
tumors: multivariate analysis of four year results. Radiother Oncol 1993;27(2):91–8.
[112] KwonY,Kim JH, Lee DJ, et al. Gamma knife treatment of acoustic neurinoma. Stereotact
Funct Neurosurg 1998;70(Suppl 1):57–64.
[113] Flickinger JC, Kondziolka D, Niranjan A, et al. Results of acoustic neuroma radiosurgery:
an analysis of 5 years’ experience using current methods. J Neurosurg 2001;94(1):1–6.

1230 ASTHAGIRI et al
[114] Bertalanffy A, Dietrich W, Aichholzer M, et al. Gamma knife radiosurgery of acoustic
neurinomas. Acta Neurochir (Wien) 2001;143(7):689–95.
[115] Iwai Y, Yamanaka K, Shiotani M, et al. Radiosurgery for acoustic neuromas: results of
low-dose treatment. Neurosurgery 2003;53(2):282–7 [discussion: 287–8].
[116] NorenG,GreitzD,HirschA, et al. Gammaknife surgery in acoustic tumours.ActaNeuro-
chir Suppl (Wien) 1993;58:104–7.
[117] Foote RL, Coffey RJ, Swanson JW, et al. Stereotactic radiosurgery using the gamma knife
for acoustic neuromas. Int J Radiat Oncol Biol Phys 1995;32(4):1153–60.
[118] Prasad D, Steiner M, Steiner L. Gamma surgery for vestibular schwannoma. J Neurosurg
2000;92(5):745–59.
[119] Black PM. Meningiomas. Neurosurgery 1993;32(4):643–57.
[120] Black P, Kathiresan S, Chung W. Meningioma surgery in the elderly: a case-control study
assessing morbidity and mortality. Acta Neurochir (Wien) 1998;140(10):1013–6 [discus-
sion: 1016–7].
[121] Couldwell WT, Kan P, Liu JK, et al. Decompression of cavernous sinus meningioma for
preservation and improvement of cranial nerve function. Technical note. J Neurosurg
2006;105(1):148–52.
[122] Pollock BE, Lunsford LD, Noren G. Vestibular schwannomamanagement in the next cen-
tury: a radiosurgical perspective. Neurosurgery 1998;43(3):475–81 [discussion: 481–3].
[123] GormleyWB, Sekhar LN,Wright DC, et al. Acoustic neuromas: results of current surgical
management. Neurosurgery 1997;41(1):50–8 [discussion: 58–60].
[124] Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas):
surgical management and results with an emphasis on complications and how to avoid
them. Neurosurgery 1997;40(1):11–21 [discussion: 21–3].
[125] Sampath P, HollidayMJ, BremH, et al. Facial nerve injury in acoustic neuroma (vestibular
schwannoma) surgery: etiology and prevention. J Neurosurg 1997;87(1):60–6.
[126] Wiegand DA, Ojemann RG, Fickel V. Surgical treatment of acoustic neuroma (vestibular
schwannoma) in the United States: report from the Acoustic Neuroma Registry. Laryngo-
scope 1996;106(1 Pt 1):58–66.