Curbing Prescription Opiods

of 20
description
Curbing Prescription Opiods
Transcript of Curbing Prescription Opiods
-
Curbing Diversion of Prescription OpioidsNathaniel Katz, MD, MSTufts University School of MedicineAnalgesic ResearchOpioid Prescribing to Adolescents in Dental SettingsNational Institute of Drug AbuseFebruary 23, 2009
-
OutlineDefine and characterize diversionPresent what is known about sources of diverted prescription opioidsSpeculate about role of dentistsDescribe potential solutions
-
1Define and Characterize Diversion
-
Definition of DiversionThe transfer of a controlled substance from a lawful to an unlawful channel of distribution or use.Section 309, Diversion Prevention and ControlUniform Controlled Substances ActNational Conference of Commissioners onUniform State Laws, 1994
means manufacture, possession,delivery or use of a controlled substance by a person or in a manner not specifically authorized by law.Section 3302.(12) of the New York State Public Health Law
-
Diversion ExamplesDiversionSharingSelling, buyingStealingPrescription forgeryDoctor shoppingIllegal internet RxCriminal prescribingNot DiversionUsing your own legitimately prescribed medication to get high(~20% of NMU)
-
2What is Known About Sources of Diverted Prescription Opioids
-
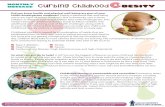
Source of Pain Relievers by Past Year Users Aged 12: 2006
Totals may not =100% because of rounding or because suppressed estimates not shownOther includes: Wrote fake prescription, Stole from doctors office/clinic/hospital/pharmacy, & Some other way.68% from docs
-
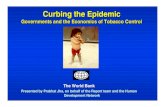
5 Most Common Sources of Misused Prescription Opioids: By Population*For free & bought; Own prescription, 1 doctor, & >1 doctor Stolen, stole from friend/family, theft, & forged prescriptionPercentage
Chart1
63.657.45446Friend/ relative*42
1416.42862Rx from MD37
4.812.58663Dealer60
3.86.31011Stolen/forged Rx15
01.338InternetInternet
NSDUH: gen. population 18-25
NSDUH dependent 18-25
Methadone maint. AATOD
Subst. abuse treatment NAVIPPRO
Methadone maintenance2
Subst. abuse treatment RADARS 21-30
Sheet1
NSDUH: gen. population 18-25NSDUH dependent 18-25Methadone maint. AATODSubst. abuse treatment NAVIPPROMethadone maintenance2Subst. abuse treatment RADARS 21-30
Friend/ relative*63.657.454465442
Rx from MD1416.428622837
Dealer4.812.586638660
Stolen/forged Rx3.86.310111015
Fake Rx383
Internet01.3383
EDTo resize chart data range, drag lower right corner of range.1313
-
Sources of Diverted Dosage UnitsDistribution SystemManufacturersDistributorsPharmaciesHospitals/ClinicsInternetPractitionersNursing HomesHospicesPatientsPrimary DiversionTheft from ManufacturersTheft from DistributorsTheft from PharmaciesTheft from Hospitals/ClinicsIllegal InternetInternatl SmugglingForgeryScript Doc/Pill MillDoctor ShoppingPatient Sells/Gives2007 Total Doses3,251,539706,5582,633,098175,000,000??Tens of millions???Tens of millions??TOTAL1,000,000,000?
-
Criminal Prescribing: 1 caseThe board investigator presented evidence that Brown was the single leading prescriber of OxyContin in the entire state, with his prescriptions accounting for 288,859 of the 922,985 OxyContin tablets sold through pharmacies in 2004.For a 30-month period, Brown was the state's second largest prescriber of OxyContin
-
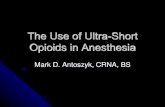
Schedule II Opioid Rx Dispensed to Individuals Showing Questionable Activity**Questionable activity = obtained Schedule II opioid prescriptions from 4 pharmacies & 4 physicians during the specified yr0123456969899000102030405Fiscal yrEstimated percentage63,000 scripts973.5 million doses
-
Quantifying Diversion: Research AgendaClean up NSDUH data:Break down non-medical use dataHow many dosage units ingestedHow many dosage units acquired through different sources*Update drug picture cardsClean up DEA Form 106 DatabaseCompile Internet diversion dataCompile criminal prescribing data; validate algorithms for identifying criminal prescribingCompile doctor shopping data; validate algorithms for identifying inappropriate doctor shopping
-
3Speculate About the Role of Dentists in Prescription Opioid Diversion
-
*Top Specialties Prescribing Immediate-Release Opioids, 1998 vs. 2002(WITH Hydrocodone & Oxycodone Combination Products)19982002Source: IMS Health, National Prescription Audit PlusTM, Year 1998 to 2002, Excluding Long-Term Care & Mail Order Channels, Data Extracted August 2003. Dentists likely prescribe about a billion doses per year of opioids, mostly immediate-release combination products
-
Speculations About Role of Dentists in Prescription Opioid DiversionDentists prescribe large volumes of drugs most commonly abused by adolescents and othersThe extent to which opioids are prescribed in greater quantities than necessary is unknown but probably considerableAnecdotal evidence suggests that adolescents use opioids non-medically that they or family members obtain from dentistsDentists rarely screen for opioid abuse risk factors or doctor shopping, monitor pts, educate them on risks of controlled substances or med storage/disposal, etc.It is not clear how well dentists understand the basic pharmacotherapy of pain and the appropriate role of opioids
-
4Potential Solutions
-
FDA, Opioids, and REMSFDAAA September 2007
RISK EVALUATION AND MITIGATION STRATEGIES (REMS) REQUIREMENTSTitle IX, Subtitle A, Section 901 of the Food and Drug Administration Amendments Act of 2007 (FDAAA) amends the Federal Food, Drug, and Cosmetic Act (FDCA) to authorize FDA to require the submission of a REMS for an approved drug if FDA becomes aware of new safety information and determines that such a strategy is necessary to ensure that the benefits of the drug outweigh the risks (section 505-1(a)). This provision took effect on March 25, 2008.
-
Switch-Based Retail SolutionPrescriberPatientExplains Med GuideREMS registryPatient training-enrollmentRetail PharmacyPrescription broughtEnrollment verifiedPrescription filledDataClientFDAWeb-based trainingSwitch company(ies)Closed Distribution
-
Solutions
Good morning and thank you for the invitation to speak at this important meeting.Although I am not a dentist, and there is little known about the specific role of dentists in the huge problem of prescription opioid diversion,Ill attempt to provide a general background on diversion, and do my best to submit to you some thoughts about how this might be relevantTo the dental community.Ill present my thoughts in the following order.I recently presided over a 2-day meeting at Tufts University on prescription opioid diversionYou would be amazed how complex it is to agree on a definition of diversion.For the purpose of todays conversation I will point out to you the definition in the Controlled Substances Act,Which is the act that is the raison detre of the DEA.Here are some examples of diversion, all of which involve transfer of the substance from licit to illicit channels.READ.[CLICK]Note that a great deal of prescription opioid abuse occurs when people who obtain medications from prescriptions for pain use their medications non-medically.This is not considered diversion.Based on NSDUH data this is the case for about 20% of non-medical users.The take-home message is that although my talk is focused on diversion, diversion is only part of the prescription opioid abuse problem.Many of you are familiar with these widely disseminated data from NSDUH.The popular interpretation is that the majority of diversion is from friends and family.Another important take-home message is that most people get their medications either directly or indirectly from doctors.The survey doesnt differentiate types of doctors, so I have no idea how much of this is from dentists.Another important message is that these data represent people, mostly amateurs, not dosage units.If you want to understand diversion, you need to understand this slide, painful as it might be.The leftmost columns represent the NSDUH data you just saw.The remaining bars indicate the sources of diversion endorsed by progressively more addicted individuals.In these populations, who presumably move many more dosage units than the NSDUH population,Sources such as dealers, theft and forgery, doctor shopping, and Internet loom much larger.It is a critical national priority to figure out how big the various sources of diversion are.In this complicated slide I have put in what we know about the magnitude, in terms of doses, of different sources.Bottom line: we dont know much.I recently completed a study that suggests that the total number of dosage units ingested non-medically in the US is 0.5-2 BB/yr.Supply chain losses seem very small; otherwise not a lot is known.
Ive picked a couple of examples to highlight a bit further.The magnitude of criminal prescribing is unknown, but if you read the newspaper and add up the number of doses involved,Its potentially a huge amount.Doctor shopping is another problem of unknown magnitude.In Massachusetts.While there is little data to support any specific cutoff for doctor shopping,I have been involved in a recent study that validated a specific cutoff using PMP data from 800,000 patients in Maine.If we want to quantify the magnitude of sources of diversion in the US, here is what we need to do.*