Curative early psychosocial interventions: evidence-based! Dr Jonathan I Bisson Clinical Reader in...
23
Curative early psychosocial interventions: evidence-based! Dr Jonathan I Bisson Clinical Reader in Psychiatry Cardiff University
-
Upload
betty-blair -
Category
Documents
-
view
215 -
download
1
Transcript of Curative early psychosocial interventions: evidence-based! Dr Jonathan I Bisson Clinical Reader in...

Curative early psychosocial interventions: evidence-based!
Dr Jonathan I Bisson
Clinical Reader in Psychiatry
Cardiff University

Guideline recommendation 23
• Treatment with trauma-focused cognitive behavioural therapy for those affected who have an acute stress disorder or severe symptoms of post-traumatic stress disorder in the first month after a shocking experience
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Agreed Practice
0-5scale

Wait and Target
• Traumatic stress symptoms within three months– Acute stress disorder– Acute PTSD
• Trauma-focused CBT• Fifteen RCTs
– Individual 4-16 sessions (4 - 17 hours) – Education, relaxation, imaginal exposure, cognitive
restructuring and in vivo exposureRoberts et al, 2008
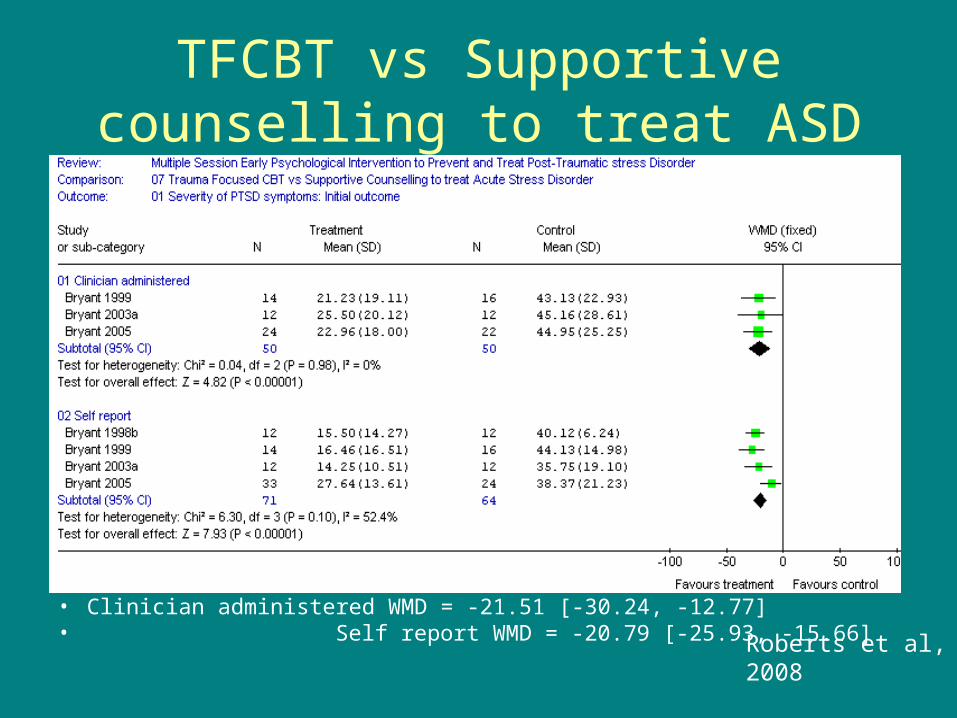
TFCBT vs Supportive counselling to treat ASD
• Clinician administered WMD = -21.51 [-30.24, -12.77]• Self report WMD = -20.79 [-25.93, -15.66] Roberts et al, 2008
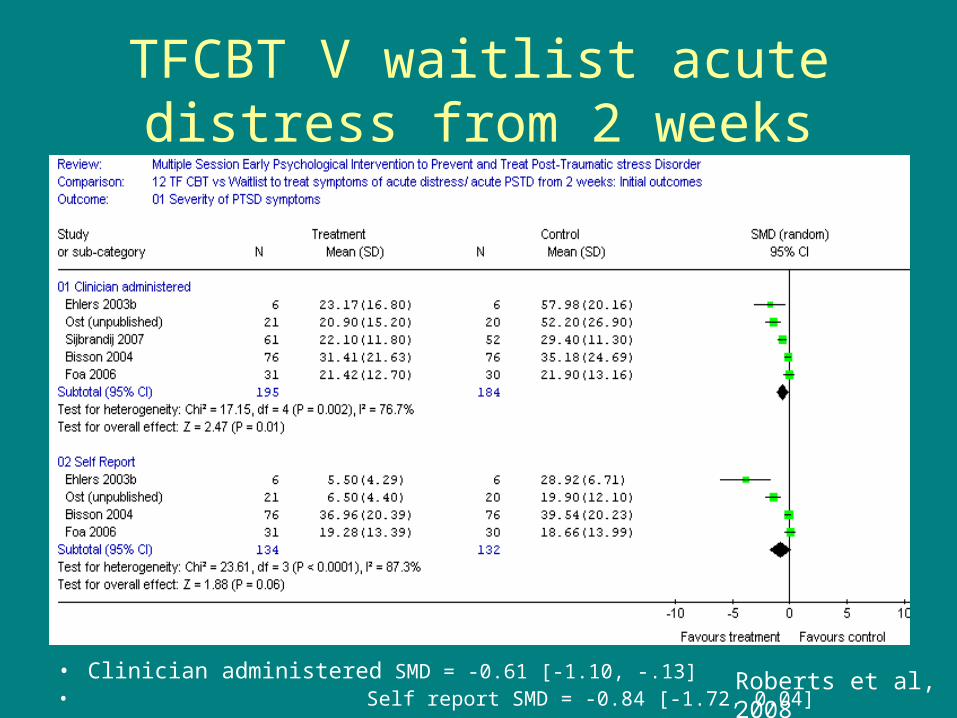
TFCBT V waitlist acute distress from 2 weeks
• Clinician administered SMD = -0.61 [-1.10, -.13]• Self report SMD = -0.84 [-1.72, 0.04]
Roberts et al, 2008

TFCBT v waitlist Acute PTSD
• Clinician administered SMD = -1.22 [-1.65, -0.78]• Self report SMD = -1.68 [-2.34, -1.01]
Roberts et al, 2008
Guideline recommendation 24
• The study group recommends that relaxation should be offered only as part of CBT, not as a (nontrauma-focused) intervention on its own
0
0.5
1
1.5
2
2.5
3
Agreed* Practice*
0-5scale

Relaxation
• Partner disagreement• No evidence in first
six weeks• Absence of evidence
is not evidence of no effect
• What if can’t tolerate or access TFCBT?
0
0.5
1
1.5
2
2.5
TFCBT
EMDR
Stress M
an't
Other
Group
CBT
SMD & 95% CIs
Psychological treatment for chronic PTSD versus wait list

The European Network for Traumatic Stress
http://www.tentsproject.eu/

TENTS Delphi Process
• Recognizes the value of experts’ opinion, experience and intuition
• Allows use of limited information when full scientific knowledge is lacking
• 122 experts (106 responded)• Three rounds • After each round anonymous summary provided
with reasons for judgments• Convergence towards “correct” answer aimed for

An Example of 2nd Round Question
1. <<< THERE IS GOOD CONSENSUS REGARDING THIS POINT >>> Every area should have a multi agency psychosocial care planning group. (1=Completely disagree; 9=Completely agree and 5=Neither)
Rate (1st round average= 7.78):
1 (0.9% )
2 (0.9% )
3 (2.8% )
4 (0.0% )
5 (5.7% )
6 (5.7% )
7 (13.2% )
8 (24.5% )
9 (46.2% )
Comment:

0.01.02.03.04.05.06.07.08.09.0
10.0
2 3 4 5 6 7 8 9 10 11 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
0.01.02.03.04.05.06.07.08.09.0
10.0
35 36 37 38 39 40 41 42 43 44 45 46 47 49 50 51 52 53 54 55 56 57 58 59 60 62 63 64 65 66 67 68
0.01.02.03.04.05.06.07.08.09.0
10.0
69 70 71 72 73 74 75 76 78 79 80 81 82 83 84 85 86 87 89 90 91 92 93 94 95 96 97 98 99 100101103
Average Rating of All Questions

TENTS Guidance
• Other treatments should be available for individuals with acute post traumatic stress disorder when TF-CBT is not available or is not tolerated
• Evidence based interventions for individuals with other mental health difficulties should be available

Guideline recommendation 26
• In the event of sleep disorders as a result of the trauma, pharmacotherapy may be considered. For any drug treatment for sleep disorders, depressive disorders or anxiety disorders, the study group refers the reader to the existing guidelines. 3.1
3.2
3.3
3.4
3.5
3.6
3.7
Agreed Practice
0-5scale

Relative Risk of PTSD
0
1
2
3
4
5
6
Hydrocort Propranolol Temazepam
95% CI = 19

Shalev et al (2007)
• Prolonged exposure, cognitive therapy, escitalopram 10-20mg, placebo, wait list (bi-weekly telephone)
• 4220 screened, 1470 +ve, 753 interviewed, 397 invited for Rx, 289 randomised
• 152 agreed to any intervention, 118 to anything but SSRI, 19 SSRI c’ind’d
• 12% SSRI non completers, 26% PE

Shalev et al (2007)
0
10
20
30
40
50
60
70
80
Baseline 4 months
Placebo
Escitalopram
PE
CT
WL
Early Pharmacological Interventions
• No convincing evidence– Propranolol versus placebo (two studies)– Gabapentin versus placebo (one study)– Temazepam versus placebo (one study)– Escitalopram versus placebo (one study)
• Limited evidence of benefit– Hydrocortisone versus placebo (one study)

Guideline recommendation 27
• The study group recommends that the employer should offer counselling (to be carried out by a relief worker or trained volunteer) if a shocking event takes place at work. 0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Agreed Practice
0-5scale

Boscarino et al (2006)
• 1121 employed adults after 9/11• Telephone interviews at 1 and 2 years• 7% reported receipt of employer-sponsored,
worksite crisis interventions (? timing) by mental health professionals (non worksite excluded)
• 1-3 sessions associated with positive outcomes, 4+ sessions excluded
• Sessions ranged from psychoeducation to anxiety management, 80% said they were positive

Employer counselling
• Partner agreement
• No evidence in first six weeks
• Absence of evidence is not evidence of no effect
• ? recommendation not based on evidence
• ? need to provide basic support and identify employees who require evidence based intervention

Guideline recommendation 28
• The study group recommends treatment with trauma-focused cognitive behavioural therapy (CBT) for children, more than 7 years of age, with severe symptoms of acute post-traumatic stress and/or an acute stress disorder in the first month after a shocking event.
• Lacks evidence, consistent with NICE
Research Recommendations
• 25. Further studies into the effectiveness of EMDR as a curative early intervention in the first six weeks after stressful life events.
• 29. Further studies into the effectiveness of EMDR as an early curative intervention in children.
• 30. Further studies into pharmacological interventions in children.