Cultural Competency Integrating Differences into Community Services.
42
Cultural Competency Integrating Differences into Community Services
-
Upload
eleanore-holmes -
Category
Documents
-
view
216 -
download
0
Transcript of Cultural Competency Integrating Differences into Community Services.

Cultural Competency
Integrating Differencesinto Community Services

Objectives
Understand Stigma. Understand Culture Competency. Learn Culturally competent care for
people with Mental Health, IDD and Addictions.

Some important definitions
Related to Cultural Competency

StigmaDefinitions from the U. of Chicago PSR Training Manual
“Stigmas are negative attitudes about a group that lead to depriving them ofsome fair opportunities.”

Stereotypesfrom The Asian Health Coalition of Illinois
Stereotypes are exaggerated beliefs or fixed ideas about a person or
group which is held by people and sustained by selective perception and
selective forgetting.

Prejudicefrom The Asian Health Coalition of Illinois
Prejudice is a preconceived idea or negative attitude formed before the facts are known and sustained over generations. A bias without reason,
resisting all evidence…
Discriminationfrom The Asian Health Coalition of Illinois
Discrimination refers to treatment in favor or against a person based on
the group to which that person belongs and not on merit.

People are often stigmatized by:
Mental Illness Intellectual Developmental Disability Physical Disability (including blindness, deafness) Alcoholism /and or Drug Addiction HIV or AIDS, Cancer or other terminal illnesses Criminal behavior Poverty Alternative Lifestyles/sexual orientation Wheelchair bound Gender Obesity

“Different” people are “Stigmatized”
IDD inmates in a sanitorium in Germany

stigmatized groups!All our Consumers belong to

We live in an worldwhich often separates us.
Racism Sexism Ageism Feminism Classism Atheism

Culture from King,et. al
The Office of Special Programs, U.S. Dept. of Education
“The integrated patterns of human behavior that includes thoughts,
communications, actions, customs, beliefs,values, and institutions of racial, ethnic, religious, or social
groups.”

The Bottom Line:People are different, even within
their own culture!
These differences matter when planning and
providing services.

Here at Hill Country MHDDC
Consumers are very diverse in their language and culture.

How Can We Communicate?
Think Language first! Do we need an interpreter? Communicate respectfully. Be sensitive to the consumer and the family. Consider your dress, tone of voice, eye contact,
location, seating arrangement, privacy, etc.

Religion
Religious beliefs shape how the world is viewed. Is illness a punishment? The devil’s work? An
evil spell? Bad karma? For Hispanics, the curandero is a trusted healer. For Lakota Sioux, the ritual Vision Quest,
praying and fasting at a holy site is life changing.
Treatment Issues of Mentally Challenged
People need to have meaningful activity
and purpose in their lives. People need to feel acknowledged and
appreciated. People need safety, structure, and security. Lack of continuity can cause crisis! They may need vocational assistance.
How Do We Best Serve Our Consumers?
Examine own stereotypes.
Build trust.
Use People First language!

How do we best serve our consumers?
Pronounce the person’s name correctly. Get an interpreter, if necessary. Educate yourself from the consumer, his
family, co-workers, etc.
Remember differences do matter!

Cultural Diversity and Health Care
Cultural Competence – Definition
A set of congruent behaviors, practices, attitudes and policies that come together in a system or agency or among professionals, enabling effective work to be done in cross-cultural situations
Cultural Diversity and Health Care
The Cultural Competence Continuum
Where Am I Now?
Where Could I Be?

The Cultural Competence Continuum
Cultural Diversity and Health Care
Cultural Competence Definitions Cultural Destructiveness: forced
assimilation, subjugation, rights and privileges for dominant groups only
Cultural Incapacity: racism, maintain stereotypes, unfair hiring practices
Cultural Blindness: differences ignored, “treat everyone the same”, only meet needs of dominant groups

Cultural Diversity and Health Care
Cultural Competence Definitions Cultural Pre-competence: explore cultural
issues, are committed, assess needs of organization and individuals
Cultural Competence: recognize individual and cultural differences, seek advice from diverse groups, hire culturally unbiased staff
Cultural proficiency: implement changes to improve services based upon cultural needs, do research and teach

Cultural Diversity and Health Care
Acquiring Cultural Competence
Starts with Awareness Grows with Knowledge Enhanced with Specific Skills Polished through Cross-Cultural
Encounters

The Explanatory ModelAuther Klienman, PH.D.
Culturally sensitive approach to asking
inquiring about a health problem
What do you call your problem? What do you think caused your problem? Why do you think it started when it did? What does your sickness do to you? How
does it work? How severe is it? How long do you think you
will have it?(continued next page)

The Explanatory ModelAuther Klienman PH.D.
Culturally sensitive approach to asking about a health problem
What do you fear most about your illness? What are the chief problems your sickness
has caused you? Anyone else with the same problem? What have you done so far to treat your
illness: What treatments do you think you should
receive? What important results do you hope to
receive from the treatment? Who else can help you?
The LEARN ModelBerlin and Fowkes
Listen to the patient’s perception of the problem
Explain your perception of the problem
Acknowledge and discuss differences/similarities
Recommend treatment
Negotiate treatment

Working with Interpreters
Qualifications: Bilingual, bicultural, understands
English medical vocabulary Comfort in the medical setting,
understands significance of the health problem
Preserves confidentiality
Working with Interpreters
Multiple Roles:
Translator of Language
Culture Broker
Patient Advocate: Convey expectations, concerns
Working with Interpreters
Use language to identify the
interpreter as the go-between, not as the person to be blamed, e.g., the interpreter might say, “The doctor has ordered tests and this is what he says”

Working with Interpreters
Translation factors Language: how are new words created?
Navajo: Penicillin = “the strong white medicine shot you get for a cold”
Minimize jargon, e.g., “machine to look at your heart” instead of “EKG”
Nonverbal communication = 60% of all communication
Nodding may indicate politeness, not comprehension
Bilingual interviewing takes at least twice as long as monolingual interviews!
Caretakers’ Responsibilities
Learn and use a few phrases of greeting and introduction in the patient’s native language. This conveys respect and demonstrates your willingness to learn about their culture.
Tell the patient that the interpreter will translate everything that is said, so they must stop after every few sentences.

Caretakers’ Responsibilities
When speaking or listening, watch the patient, not the interpreter. Add your gestures, etc. while the interpreter is translating your message.
Reinforce verbal interaction with visual aids and materials written in the client’s language.
Repeat important information more than once.
(continued on next page)

Caretakers’ Responsibilities
Always give the reason or purpose for a treatment or prescription.
Make sure the patient understands by having them explain it themselves.
Ask the interpreter to repeat exactly what was said.
Personal information may be closely guarded and difficult to obtain.
Patient often request or bring a specific interpreter to the clinic.
(continued on next page)

Caretakers’ Responsibilities
In some cultures it may not be appropriate to suggest making a will for dying patients or patients with terminal illnesses; this is the cultural equivalent of wishing death on a patient.
Avoid saying “you must... Instead teach patients their options and let them decide, e.g., “some people in this situation would...”

Cultural Diversity and Health Care
It is because we are different that each of us is special.

Putsch III RW. Cross-cultural communication: The special case of interpreters in health care. JAMA 1985;254(23):3344-48
Sockalingum adapted from Hayes, Cultural Competence Continuum, 1993 and Terry Cross Cultural Competency Continuum.
References
What is a TTY

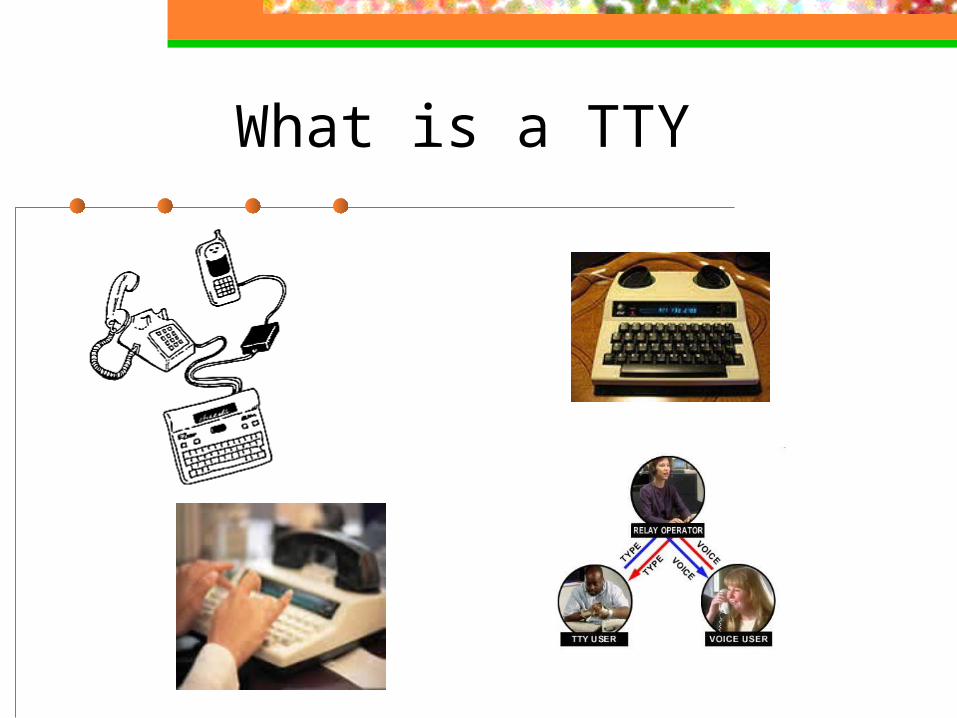
TTY = Text Telephone
Also sometimes called a TDD or Telecommunication Device for the Deaf. A TTY is a special device that lets people who
are deaf, hard of hearing, or speech impaired use the telephone to communicate by typing back and forth instead of talking and listening.
A TTY is required at both ends of the conversation to communicate.

TTY Use
To use a TTY, you set the telephone Handset on to special acoustic cups built into the TTY. Then type the message you want to send on the TTY’S keyboard. As you type, the message is sent over the phone line just like your voice would be sent over the
phone line if you talked. You can read the other person’s response on the TTY’S
text display.
Telecommunications Relay Service
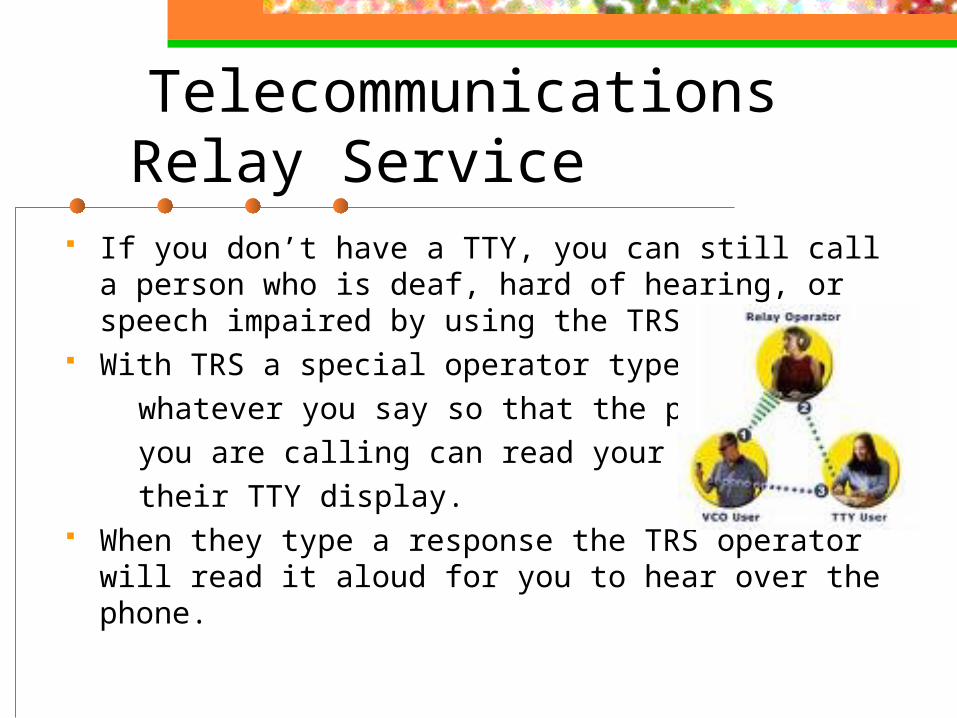
If you don’t have a TTY, you can still call a person who is deaf, hard of hearing, or speech impaired by using the TRS.
With TRS a special operator types whatever you say so that the person you are calling can read your words on their TTY display. When they type a response the TRS operator
will read it aloud for you to hear over the phone.