CTEV Non-op Tt
43
CTEV(NONOPERATIVE) CTEV(NONOPERATIVE) PRESENTED BY: DR.SEZO PRESENTED BY: DR.SEZO MODERATORS: DR SHAH ALAM MODERATORS: DR SHAH ALAM DR DR ASHOK ASHOK
-
Upload
drdeepak-gautam -
Category
Documents
-
view
122 -
download
2
Transcript of CTEV Non-op Tt
CTEV(NONOPERATIVE)
PRESENTED BY: DR.SEZO BY: DR. MODERATORS: MODERATORS: DR SHAH ALAM DR ASHOK
INTRODUCTION
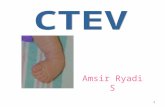
The full blown CTEV present with the heel in equinus, entire hind foot in varus and mid and forefoot adducted and supinated Talipes: Talipes: It is a Latin word derived from talus- ankle, taluspespes- foot Original meaning: A deformity that causes the meaning: patient to work on the ankle Present day meaning is any variety of club-foot clubClub-foot: Club-foot: It is so called because severe untreated Talipes equinovarus has a club-like appearance club-
Incidence
Varies with sex and race 1-2 per thousands births Max in polynesian - 6.81 Min in Chinese and mongoloid -0.39 B/L -40% 40% U/L M:F right affected slightly more 3:1
Familial tendency - 1in 35 Genetic predisposition- identical twin 1in3 (32.5%) predispositionin3 32.
Etiology
Etiology of idiopathic club foot is multifactorial and is modulated significantly by developmental aberration early in limbbud development There is no apparent cause and various theories are proposed these are: are:
Theories of C TEV
Turco s: medial displacement of navicular and calcaneus s: around the talus Brockmans: Brockmans: Congenital atresia of the TN joint McKays: McKays: Three dimensional bony deformity of the subtalas complex Intrauterine: Due to compression by malposition of Intrauterine: foetus in utero Genetic: General population 1:800 Genetic:
In siblings 1: 35 In identical twins 1:3
Germ plasm theory: Primary germ plasm defect theory: in talus with subsequent soft tissue changes Soft tissue theory: Primary soft tissue defect theory: with secondary bony changes Prenatal muscle Imbalance theory pronators and overacting of invertors weak
Secondary clubfoot: - paralytic disorder: polio,spina bifida, myelodysplasia and Freidreichs ataxia -Arthrogryposis multiplex congenita.
PathoanatomyThe pathology in CTEV affects all the bones and joints of the foot with corresponding soft tissue contractors especially of the postero medial structures (A) Contractures in foot are: are: (I) Medially: Medially:
Posterior tibial tendon, the flexor hallucis longus tendon and the flexor digitorum longus tendon are all shortened, occasionally also the abductor hallucis longus The navicular is displaced medially and fixed in scar tissue usually, in some cases against the tibia
Deltoid ligament TN joint capsule Spring ligament Plantar fascia contracture
(ii) Subtalor contractors: contractors:
Bifurcated ligament Interrosseus ligament The talus may be almost subluxed forward out of the mortice of the ankle joint with an inability of the talus be fit back into the mortice contracture of the distal tibio fibular syndesmoses Achilles tendon Talofibular ligament Calcaneofibular ligaments
(iii) Posteriorly: Posteriorly:
(B) Bones: The bones of the foot are smaller than normal Bones:
The neck of the talus is angulated so that the head of the talus faces downwards and medially The calcaneum is small and concave medially
(C) Joints: Joints:
Equinus: Equinus: Deformity occurs primarily at the ankle joint Inversion deformity occurs primarily at the subtalar joint Fore foot adduction deformity occurs at the mid tarsal joints mainly at Talo-navicular jn TaloFore foot cavus: deformity is the result of excessive arching of cavus: the foot at the mid-Tarsal jn. midjn.
Radiographic anatomy
Normal range of roentgenoglaphic angles for comparison to club foot
Talocalcaneal angle
A.P. view 30 to 35 35 D.F. lat view 25 to 50 50
Tibio calcaneal angle
Stress lateral view 10-40 10-40 A.P. view 5 to 15 15
Talus first MT angle
Diagnosis clinical features:
Five classical deformities are seen and in response to this secondary deformities develop Primary deformities
Equinus Varus Cavus Forefoot adduction Internal tibial torsion
Secondary deformities :
Foot size is decrease to 50% 50% Medial border is concave, lateral border is convex Fore foot is plantar flexes upon hint foot Skin is stretched over the dorsum of the foot Callosties over dorsum of foot Stumbling gait Atrophy of muscles in anterior or posterior compartments of the leg
Kawashima and Uhthoff:classify CTEV into extrinsic intrinsic Bony deformity + + Fibrosis _ + flexible rigid conservative surgery
Rigid club foot :forefoot corrected but hint foot remain uncorrected after cons t/t, Relapse club foot :corrected initially, but relapse later Recurrent club foot:type of relapse the cause being muscle imbalance which was over look initially. Resistant :totally resistant to correction
Clinical test
Dorsi flexion test
Screening text
Plumbline test
To detect the tibial torsion
Scratch test
To detect muscle imbalance
Medial scratch test Lateral scratch test
Classification4 most common classification are :
Ponseti and smoley Harrold and walkes Latterall s Dimeglio et al (Mostly accepted system)
The system of dimeglio et al classificationClassificatio n grade I II Type Benign Moderate Score